Research Letter
Prenatal diagnosis of microvillus inclusion disease
Chih-Ping Chen
a,b,c,d,e,f,*
, Yi-Ning Su
g, Schu-Rern Chern
b,
Pei-Chen Wu
a, Wayseen Wang
b,haDepartment of Obstetrics and Gynecology, Mackay Memorial Hospital, Taipei, Taiwan bDepartment of Medical Research, Mackay Memorial Hospital, Taipei, Taiwan
cDepartment of Biotechnology, Asia University, Taichung, Taiwan
dSchool of Chinese Medicine, College of Chinese Medicine, China Medical University, Taichung, Taiwan eInstitute of Clinical and Community Health Nursing, National Yang-Ming University, Taipei, Taiwan fDepartment of Obstetrics and Gynecology, School of Medicine, National Yang-Ming University, Taipei, Taiwan
g
Department of Medical Genetics, National Taiwan University Hospital, Taipei, Taiwan
h
Department of Bioengineering, Tatung University, Taipei, Taiwan Accepted 13 June 2011
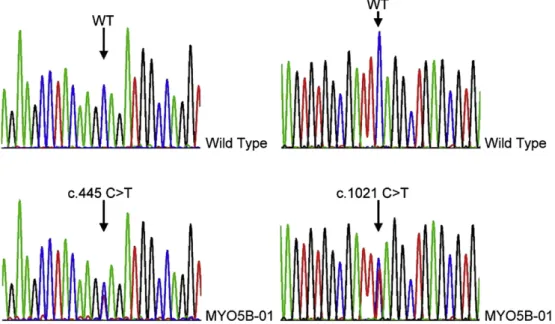
A 23-year-old, gravida 3, para 1, woman underwent amniocentesis at 20 weeks of gestation because of a previous child affected with microvillus inclusion disease (MVID). The child died of intractable diarrhea, sepsis, malnutrition, and multiple organ failure at the age of 6 months. Mutation analysis of the family revealed a c.445C>T nonsense mutation in Exon 4 of the MYO5B gene in the affected child and the father and a c.1021C>T nonsense mutation in Exon 9 of the MYO5B gene in the child and the mother[1]. During this pregnancy, routine sonographic findings were normal. There was neither intestinal dilation nor polyhydramnios. The pregnancy was uneventful and did not have antepartum hemorrhage. Amniocentesis revealed a karyotype of 46,XX. The level of amniotic fluid a-fetoprotein (AFAFP) at 20 weeks of gestation was 67,420 ng/ mL (7.69 multiples of the median). Molecular analysis of the MYO5B gene using both uncultured and cultured amniocytes revealed compound heterozygous nonsense mutations in the MYO5B gene. The mutation of c.445C>T or CAG>TAG predicts a p.Q149X, and the mutation of c.1021C>T or CAG>TAG predicts a p.Q341X in the affected fetus (Fig. 1). The maternal serum AFP level at 23 weeks of gestation was not elevated. The parent elected to terminate the pregnancy, and a 634-g affected fetus was delivered at 23 weeks of gestation. The fetus did not have structural abnormalities. The placenta was grossly normal. Postnatal analysis of the fetal tissues confirmed the prenatal diagnosis.
MVID (OMIM 251850) is an autosomal recessive disorder of intestinal epithelial cells and is characterized by intractable life-threatening watery diarrhea during infancy. MVID is caused by mutations in the MYO5B gene (OMIM 606540)[2]. MYO5B encodes myosin Vb or the unconventional class V dimeric nonfilamentous myosin that regulates membrane traf-ficking along the recycling pathway in polarized epithelial cells
[2,3]. Loss-of-function mutations of the MYO5B gene that
cause disruption of epithelial cell polarity are a major cause of
MVID[2,4,5]. MYO5B mutations have been shown to correlate
with an aberrant subcellular distribution of the myosin Vb protein and apical recycling endosomes[6]. The present case had compound heterozygous nonsense mutations in the MYO5B gene causing early truncation of MYO5B and the loss of its function.
The present case is the first report of prenatal molecular diagnosis of MVID. The present case did not present poly-hydramnios and bowel dilation in the second trimester. Ruem-mele et al[7]suggested that in cases of MVID, the pregnancy is uneventful, and there is no polyhydramnios. However, Kennea et al[8]and Chen et al[1]reported polyhydramnios and bowel dilation associated with MVID in the third trimester. The peculiar aspect of this presentation is elevated AFAFP in the second trimester, which has not been previously described in pregnancy with MVID. Elevated AFAFP can be associated with fetal anomalies such as ventral wall defects, esophageal atresia, fetal teratoma, cloacal extrophy, and epidermolysis bullosa as well as placental abruption and hemorrhage. Because there were no other uteroplacental and fetal factors of elevated AFAFP in this case, we speculate that the AFAFP elevation may possibly be caused by in utero body fluid leakage into the amniotic fluid through fetal enteropathy.
* Corresponding author. Department of Obstetrics and Gynecology, Mackay Memorial Hospital, 92, Section 2, Chung-Shan North Road, Taipei, Taiwan.
E-mail address:[email protected](C.-P. Chen).
Available online at www.sciencedirect.com
Taiwanese Journal of Obstetrics & Gynecology 50 (2011) 399e400
www.tjog-online.com
1028-4559/$ - see front matter CopyrightÓ 2011, Taiwan Association of Obstetrics & Gynecology. Published by Elsevier Taiwan LLC. All rights reserved. doi:10.1016/j.tjog.2011.06.001
Acknowledgments
This work was supported by research grants NSC-97-2314-B-195-006-MY3 and NSC-99-2628-B-195-001-MY3 from the National Science Council and MMH-E-100-04 from Mackay Memorial Hospital, Taipei, Taiwan.
References
[1] Chen C-P, Chiang M-C, Wang T-H, Hsueh C, Chang S-D, Tsai F-J, et al. Microvillus inclusion disease: prenatal ultrasound findings, molecular diagnosis and genetic counseling of congenital diarrhea. Taiwan J Obstet Gynecol 2010;49:487e94.
[2] Mu¨ller T, Hess MW, Schiefermeier N, Pfaller K, Ebner HL, Heinz-Erian P, et al. MYO5B mutations cause microvillus inclusion disease and disrupt epithelial cell polarity. Nat Genet 2008;40:1163e5.
[3] Rodriguez OC, Cheney RE. Human myosin-Vc is a novel class V myosin expressed in epithelial cells. J Cell Sci 2002;115:991e1004.
[4] Erickson RP, Larson-Thome K, Valenzuela RK, Whitaker SE, Shub MD. Navajo microvillous inclusion disease is due to a mutation in MYO5B. Am J Med Genet 2008;146A:3117e9.
[5] Ruemmele FM, Mu¨ller T, Schiefermeier N, Ebner HL, Lechner S, Pfaller K, et al. Loss-of-function of MYO5B is the main cause of microvillus inclusion disease: 15 novel mutations and a CaCo-2 RNAi cell model. Hum Mutat 2010;31:544e51.
[6] Szperl AM, Golachowska MR, Bruinenberg M, Prekeris R, Thunnissen AM, Karrenbeld A, et al. Functional characterization of mutations in the myosin Vb gene associated with microvillus inclusion disease. J Pediatr Gastroenterol Nutr 2011;52:307e13.
[7] Ruemmele FM, Schmitz J, Goulet O. Microvillous inclusion disease (microvillous atrophy). Orphanet J Rare Dis 2006;1:22.
[8] Kennea N, Norbury R, Anderson G, Tekay A. Congenital microvillous inclusion disease presenting as antenatal bowel obstruction. Ultrasound Obstet Gynecol 2001;17:172e4.
Fig. 1. Compound heterozygous nonsense mutation of c.445C>T, p.Q149X in Exon 4 and c.1021C>T, p.Q341X in Eexon 9 of the MYO5B gene in the fetus. MYO5B-01¼ fetus; WT ¼wild type as control.