功能性鼻竇內視鏡手術對於中重度慢性鼻炎及鼻竇炎的角色:以病人感受評分、內視鏡及電腦斷層來評估; The Role of Functional Endoscopic Sinus Surgery in Moderate-to-Severe Chronic Rhinosinusitis: Evaluation by Patient Perception Score, Endoscopy and CT Scan
59
0
0
全文
(2) Abstract Objectives Chronic Rhinosinusitis (CRS) is a common upper airway respiratory disease in Taiwan. Although it is clear from a popular standpoint that CRS makes a negative influence on patient’s quality of life, the level of personal influence may vary widely from individual to individual. For patient’s perception, symptom severity can easily be classified as none, mild, moderate and severe. Medical treatment is reasonable to treat patients with mild symptoms of CRS. For patients with severe symptoms of CRS, or CRS due to nasal polyp, sinonasal tumor, fungal infection or identified sinonasal anatomic variations, surgical intervention is indicated if they have been refractory to medical treatment. FESS has been the main stream of surgical methods to treat CRS for about 20 years. Few literatures offered adequate discussions focusing on the role of FESS for patients with perceived moderate-to-severe symptoms of CRS. The aim of this study was to investigate the role of FESS in moderate-to-severe chronic rhinosinusitis by using subjective symptom score and objective endoscopy and CT scan. Materials and Methods We used Visual Analogue Score (VAS) Questionnaire to evaluate CRS symptoms status. Symptoms include nasal obstruction, rhinorrhea / postnasal drip, headache, facial pain and olfactory disturbance and overall discomfort. Each symptom was scored on a scale from 0 to 10 which 0 presented no symptom and 10 presented the most severe symptom. According to the VAS questionnaire, patients with equal to or over 8 scales in at least two symptom items and overall discomfort scales also equal to or over 8 scales were included into our I.
(3) study. They were regarded as having moderate-to-severe symptoms of CRS. Patients with nasal polyp, sinonasal tumor, fungal sinusitis or sinonasal anatomic variations were excluded. Analysis of prospectively collected data was performed. These patients filled the VAS Questionnaire in the initial visit. Diagnostic nasal endoscopy was performed and given a score from 0 to 20 according to the scoring system proposed by Lund and Kennedy. Sinus CT scan were assessed and given a score from 0 to 24 according to the Lund-Mackay staging system. Functional endoscopic sinus surgery (FESS) was suggested if patient was refractory to maximal medical treatment. Patients who have undergone FESS filled VAS Questionnaire and were assessed with nasal endoscopy at least 6 months postoperatively. Those without FESS due to personal reasons also filled VAS Questionnaire and were assessed with nasal endoscope at least 6 months after initial visit. Results Thirty two patients were included in this study. There were 22 males and 10 females. The mean patient age was 38.2 years (range, 18-56 years). Mean follow-up period was 11.8 months (range, 7-19 months). Thirteen patients were allergen positive proved by specific IgE antibody in serum. Eighteen patients underwent FESS. After statistical analysis, the endoscopic findings correlate with the subjective symptom severity (p <0.05). Moreover, there was excellent correlation between the endoscope score and CT score (p <0.001). In contrast, there was no significant correlation between VAS score and CT score (p >0.05). There was also no statistically significant difference in VAS score and CT score between atopic and non-atopic group in the pre-treatment period (p >0.05). There was no statistically significant difference between surgical and II.
(4) non-surgical group in the three parameters in the pre-treatment period (p >0.05). However, the VAS score, endoscopy score had more marked reduction in surgical group than non-surgical group in the post-treatment period (p <0.05). Conclusions This study demonstrated that findings on the CT scan do not correlate with the severity of nasal symptoms. Although atopy constitute is an important factor, there was no significant difference between atopic and non-atopic CRS patients on VAS symptom score and CT score in the pre-treatment period. The VAS score, endoscopy score had significantly marked reduction in surgical group than non-surgical group. For patients with moderate-to-severe symptoms of CRS, if they have been refractory to adequate medical treatment, FESS is an effective treatment method. Keywards: chronic rhinosinusitis, patient perception, functional endoscopic sinus surgery (FESS). III.
(5) 摘. 研究目的. 要. 慢性鼻炎及鼻竇炎是台灣常見的上呼吸道疾病。雖然從一. 般大眾的觀點而言,慢性鼻炎及鼻竇炎對於病人的生活品質有著負面 的影響,但影響程度卻在病人之間有很大的不同,病人感受症狀的嚴 重程度也有很大的變異,可簡略分為沒有症狀、症狀輕微、症狀中等 以及症狀嚴重四個層級。症狀輕微者,以內科治療是一合理的治療方 式。症狀嚴重者或是慢性鼻炎及鼻竇炎歸因於鼻息肉、鼻腔鼻竇腫 瘤、黴菌感染或是鼻腔鼻竇解剖構造異常,若內科治療無效,手術治 療確實有其必要。功能性鼻竇內視鏡手術已成為治療慢性鼻炎及鼻竇 炎手術方法中的主流。然而,對於症狀為中重程度者,功能性鼻竇內 視鏡手術的角色為何?很少有文獻針對病人本身主觀認知其慢性鼻 炎及鼻竇炎症狀為中重度的族群來分析其預後。本研究目的就是先摒 除鼻息肉、鼻腔鼻竇腫瘤、黴菌感染或是鼻腔鼻竇解剖構造異常的情 況之下,針對病人自身感受有中重度的慢性鼻炎及鼻竇炎症狀的族 群,以病人感受評分、內視鏡及電腦斷層攝影來評估功能性鼻竇內視 鏡手術的角色。 研究方法. 我們使用視覺類比評分問卷來評估慢性鼻炎及鼻竇炎症. 狀的嚴重程度。所評估的症狀包括鼻塞、流鼻水/鼻水倒流、頭痛、. IV.
(6) 臉痛及嗅覺損失等五種及整體的不舒適程度。每一症狀評分範圍為零 分到十分,零分為沒有症狀,十分為症狀最嚴重。我們選取慢性鼻炎 及鼻竇炎症狀為至少有兩項或兩項以上的症狀,其症狀評分大於或等 於八分,而且其整體的不舒適程度也必須大於或等於八分的患者視為 中重程度患者。前瞻性地蒐集患有中重度慢性鼻炎及鼻竇炎症狀的成 年人的資料,並予以分析。這些病患在初診時填寫視覺類比評分問 卷,並接受診斷性的鼻內視鏡檢查,依照 Lund and Kennedy 提出的 內視鏡評分系統給予 0 至 20 分的評分。病患亦接受鼻竇電腦斷層檢 查,並依照 Lund-Mackay 評分系統給予 0 至 24 分的評分。若病患對 於足夠的內科治療無效,則建議病患接受功能性鼻竇內視鏡手術。有 接受功能性鼻竇內視鏡手術的病患在至少 6 個月之後再次填寫視覺 類比評分問卷,並接受鼻內視鏡檢查。因個人因素未接受功能性鼻竇 內視鏡手術的病患,亦在距離初診至少 6 個月之後再次填寫視覺類比 評分問卷,並接受鼻內視鏡檢查。 研究結果. 共有三十二位病患列入本研究,其中有 22 位男性,10 位. 女性。平均年齡 38.2 歲(範圍為 18 至 56 歲) ,平均追蹤時間為 11.8 個月(範圍為 7 至 19 個月) 。13 位病人經由血清特殊免疫球蛋白 E 檢查,證實具有過敏體質。有 18 位病人接受功能性鼻竇內視鏡手術。 經由統計分析,視覺類比症狀評分與電腦斷層評分二者之間並無相關. V.
(7) 性(p >0.05)。視覺類比症狀評分與電腦斷層評分在過敏體質的病患 與非過敏體質的病患之間,並無統計學上的顯著差別(p >0.05)。也 就是說有過敏體質者未必有較嚴重的慢性鼻炎及鼻竇炎症狀,也未必 有較嚴重的電腦斷層評分。假設不考慮是否有無過敏體質,比較手術 組與非手術組在治療前的電腦斷層評分、治療前後的視覺類比症狀評 分與內視鏡評分,發現治療前的三種評分在手術組與非手術組之間並 無統計學上的顯著差別(p >0.05)。然而手術組在治療後的視覺類比 症狀評分與內視鏡評分明顯低於非手術組(p <0.05)。除此之外,若 將過敏體質的因素列入考慮,手術組亦有較佳的治療預後。 研究結論. 本研究顯示電腦斷層上的發現與病患主觀認知的症狀嚴. 重程度,二者之間並無相關性。雖然過敏是一個重要的因素,但本研 究發現過敏體質者未必有較嚴重的慢性鼻炎及鼻竇炎症狀,也未必有 較嚴重的電腦斷層評分。治療後的視覺類比症狀評分與內視鏡評分, 手術組明顯低於非手術組。所以對於具有中重程度的慢性鼻炎及鼻竇 炎症狀的病患而言,假設內科治療無效,功能性鼻竇內視鏡手術是一 個有效的治療方式。 關鍵字. 慢性鼻炎及鼻竇炎,病人感受性,功能性鼻竇內視鏡手術. VI.
(8) Acknowledgement Chronic Rhinosinusitis (CRS) makes a negative influence on patients’ quality of life. For patients’ perception, symptom severity can easily be classified as none, mild, moderate and severe. Medical treatment is adequate to treat patients with mild symptoms of CRS. For patients with severe symptoms of CRS, or CRS due to nasal polyp, sinonasal tumor, fungal infection or identified sinonasal anatomic variations, surgical intervention is indicated and helpful if they have been refractory to medical treatment. Functional endoscopic sinus surgery has been the main stream of surgical methods to treat CRS for about 20 years. Because few literatures offered adequate discussions focusing on the role of FESS in patients with perceived moderate-to-severe symptoms of CRS, the goal of my study is to discuss the role of FESS for this patient population. I have to give my best appreciations to Professor Weng-Cheng Chang, Dr. Yuan-Kai Cheng and Dr. Weng-Cheng Chen. Professor Weng-Cheng Chang provided me the directions and many substantial help in this study. Dr. Yuan-Kai Cheng and Dr. Weng-Cheng Chen offered their abundant clinical experiences to me. Finally, I will give my heartfelt thanks to my family because their encouragement supported me to complete this study.. Yu-Chien Chang July, 2007. VII.
(9) Abbreviation CRS: chronic rhinosinusitis AAO-HNS: American Academy of Otolaryngology – Head and Neck Surgery AAOA: American Academy of Otolaryngologic Allergy ARS: American Rhinologic Society OMC: ostiomeatal complex CT: computed tomography FESS: functional endoscopic sinus surgery VAS: Visual Analogue Score MAST: multiple allergens simultaneous test HTN: hypertension DM: Diabetic Mellitus SNOT-20: 20-item Sinonasal Outcome Test CCS: Chronic Sinusitis Survey RSDI: Rhinosinusitis Disability Index. VIII.
(10) Table of Contents Abstract . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . I Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VII Abbreviation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. VIII Text . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1 Objectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8. Materials and Methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10 Study population . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Symptom severity evaluation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 Endoscopy score . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 CT score . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 Statistical analysis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 14. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 Patient characteristics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 Subjective and objective testing in pre-treatment and post-treatment period . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 Correlation analysis among the subjective and objective testing . . . . . . . . . . . . 17 Comparison of outcome for atopic and non-atopic patients . . . . . . . . . . . . . . . . 18 Comparison of outcome for surgically treated and non-surgically treated patients . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 Comparison of outcome, considering both factors of atopy and surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19. Discussion. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 Conclusions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29 References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30 Appendix. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40. IX.
(11) 目. 錄. 摘要. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . I 致謝. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. VII 縮寫. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . VIII 正文. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 前言. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 1 研究目的 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8. 材料及方法. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. 10 研究族群. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 症狀嚴重度評估. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10 內視鏡分數 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 電腦斷層攝影分數 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12 統計方法 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14. 研究結果. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 . . 病人資料 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 治療前後的主觀及客觀檢驗 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16 主觀及客觀檢驗的相關性分析 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17 過敏及非過敏病人的預後比較 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 手術及非手術病人的預後比較 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18 同時考慮過敏及手術兩種因素的預後比較 . . . . . . . . . . . . . . . . . . . . 19. 討論. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .20 結論. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29 參考文獻. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30 附件. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .40. X.
(12) Introduction Anatomy and Physiology of the Sinuses There are four pairs of paranasal sinuses at the nose. They consist of the frontal, ethmoidal, maxillary, and sphenoidal sinuses. Each sinus is lined with a mucous membrane that is continuous with the mucosa of the nasal cavity through an ostium.1 The maxillary and ethmoid sinuses are present at birth, whereas the sphenoid and frontal sinuses appear by the second to third years of life. Complete sinus development generally occurs by the 18th year of life. The frontal sinus varies greatly in size and shape. Some adults may demonstrate a rudimentary frontal sinus or may lack pneumatization of the frontal bone. The nasofrontal duct drains into the frontoethmoidal recess located in the middle meatus. The ethmoidal sinus is the most developed sinus at birth. The ethmoidal sinus is separated from the orbit by a very thin layer of bone, the lamina papyracea; therefore, infections can readily penetrate the thin bone, leading rapidly to orbital complications. The anterior and middle ethmoid cells drain into the middle meatus, whereas the posterior cells drain into the superior meatus.. 1.
(13) The maxillary sinus is generally present at birth. The ostium drains through the membranous middle meatus. The sphenoid sinus begins to develop by the second or third year of life and generally is completely pneumatized by the 17th or 18th year of life. The sphenoid sinus drains into the sphenoethmoidal recess. Under normal anatomic and physiologic conditions, the sinuses are filled with air; however, variations in anatomic structure or changes in mucous membrane function predispose a person to sinus disease. An area that appears particularly prone to obstruction is the ostiomeatal complex (OMC). This narrow channel, the infundibulum, drains the frontal, anterior ethmoid, and maxillary sinuses. Ostiomeatal complex is typically the first site to be involved in inflammatory rhinosinusitis. Mucosal swelling and obstruction in this critical area can result in significant disturbances in the physiology of the sinus, which can lead to the development of significant disease and resultant symptoms.. 2.
(14) Overview of Chronic Rhinosinusitis Chronic rhinosinusitis (CRS) is one of the most frequent chronic illnesses encountered in otolaryngology clinics in Taiwan. Annual expenditures on prescription medications for CRS rose year by year. In addition to the economic impact of this disease, CRS has a significant influence on patients' quality of life and interfere with their overall sense of well-being.2. Definitions Although conventionally called sinusitis, it often is preceded by rhinitis and rarely occurs without concurrent rhinitis. The term ‘‘rhinosinusitis’’ now is used more widely. Rhinosinusitis may be defined clinically as a condition manifested by an inflammatory response involving the mucous membranes of the nasal cavity and paranasal sinuses.3, 4 The most common inflammation of the paranasal sinuses and the nose is the common cold. Task Force on Rhinosinusitis concluded that there were five different classifications of adult rhinosinusitis.3 (1)Acute sinusitis is sudden in onset and lasts up to four weeks. (2)Subacute sinusitis represents a continuum of the natural progression of. 3.
(15) acute sinusitis, which lasts for a period of four to 12 weeks. (3)Recurrent acute sinusitis is defied by symptoms and physical findings consistent with acute rhinosinusitis, with these symptoms and findings worsening after 5 days or persisting>10 days. Furthermore, ≧4 episodes occur per year and each episode lasts 7 to 10 days or more. Between episodes, symptoms are absent without concurrent antibiotic therapy. (4)Chronic sinusitis is defined as inflammation of the mucosa of the nose and paranasal sinuses lasting for at least 12 consecutive weeks. (5)Acute exacerbation of chrinic rhinosinusitis is a sudden worsening of the baseline chronic rhinosinusitis with either worsing or new symptoms.. Pathophysiology The development of rhinosinusitis depends on a variety of environmental and host factors.5 Environmental factors may include infection (viral, bacterial, and fungal), trauma, noxious chemicals, pollutants, iatrogenic medications, surgery and trauma. Host factors may include genetic causes,6, 7 mucociliary dysfunction, allergic or immune conditions, anatomic abnormalities, systemic disease, or tumors.. 4.
(16) CRS with nasal polyps and CRS without nasal polyps represent different disease entities. Polzehi et al.8 found histopathological differences in ethmoidal mucosa between CRS with nasal polyps and CRS without nasal polyps.. Subjective Findings According to the diagnostic criteria approved by the American Academy of Otolaryngology – Head and Neck Surgery (AAO-HNS), the American Academy of Otolaryngologic Allergy (AAOA), and the American Rhinologic Society (ARS), the signs and symptoms reported by patients comprise the cornerstone of CRS criteria3 and are divided into major and minor factors (Table I).. Physical Examination A nasal endoscope is ideal for evaluating the entire nasal cavity and the region of the middle turbinate. Mucopurulent secretion seen discharging from the middle meatus is strongly supportive of the diagnosis of rhinosinusitis. Inflamed mucosa or discolored mucus within the nasal cavity is consistent with chronic rhinosinusitis.. 5.
(17) Imaging Studies Patients with suspected chronic sinusitis that do not improve with medical therapy should be further investigated by imaging studies. Sinus radiographs have traditionally been used to screen such patients; however, they often miss obstructing pathology in the ostiomeatal complex region of the ethmoid sinus. Plain sinus x-rays have largely been replaced by the computed tomography (CT) scan. For most patients with chronic rhinosinusitis, a standard sinus CT scan is the radiographic study of choice as it can define the extent and location of disease, particularly within the OMC region.9,. 10. Furthermore, CT is. suggested to confirm and stage the disease and to evaluate the anatomy for those who may require surgery.11. Diagnosis The diagnosis of acute rhinosinusitis is usually not difficult; however, the diagnosis of chronic rhinosinusitis may be more challenging. Family. practitioners,. pediatricians,. pediatric. allergists,. and. otorhinolaryngologists have become increasingly aware of the possibility of rhinosinusitis. With the development of computed tomography (CT) scan and improvement in nasal endoscopy, the understanding and diagnosis of chronic rhinosinusitis have been significantly improved.. 6.
(18) According to the consensus established through the Task Force on Rhinosinusitis on August 17, 1996, the diagnosis of chronic sinusitis requires the presence of two major factors or one major and two minor factors for at least 12 consecutive weeks duration. In addition, concurrent signs of sinonasal inflammation must be present on physical or radiological examination.3. Medical Therapy The goal of medical therapy for chronic sinusitis is to promote sinus drainage and eradicate the offending pathogens. Medical treatment includes antibiotics, mucolytics, decongestants, corticosteroid, allergen avoidance, irritant avoidance (such as smoke, pollution, and occupational irritants) and nasal douching.12. Surgical Therapy The introduction of endoscopic sinus surgery by Messerklinger since the late 1970s thoroughly changed the way otolaryngologists treat sinusitis.13, 14 The goal of functional endoscopic sinus surgery (FESS) is to restore physiologic sinus ventilation and drainage, which allows for the gradual resolution of mucosal disease. All surgical manipulations are performed. 7.
(19) with endoscopes passed through the nostrils, so no external incisions are necessary. Under direct endoscopic visualization, the OMC is opened and the natural sinus ostia are enlarged. Fluid trapped within the sinuses can also be evacuated and cultured.15 Minor complications of endoscopic sinus surgery include bleeding, infection, and adhesion formation leading to sinus reobstruction. Major complications are rare and include orbital injury, intracranial injury, or CSF leak.16. Objectives of this study Chronic Rhinosinusitis (CRS) is a common upper airway respiratory disease in Taiwan. Although it is clear from a popular standpoint that CRS make a negative influence on patients’ quality of life, the level of personal influence may vary widely from individual to individual. There is variation of severity of presenting symptoms. Some patients only felt mild uncomfortable. However, some patients suffered from severe symptoms. For patient’s perception, symptom severity can easily be classified as none, mild, moderate and severe. Medical treatment is reasonable to treat patients with mild symptoms of CRS. For patients with severe symptoms of CRS, surgical intervention is indicated. 8.
(20) if they have been refractory to medical treatment. If CRS is due to nasal polyp, sinonasal tumor, fungal infection or identified sinonasal anatomic variations such as pneumatization of the middle turbinate (Concha bullosa) or severe deviated nasal septum, surgical intervention is also indicated. FESS has been the main stream of surgical methods to treat CRS for about 20 years. FESS is the major subject of discussion in our study. After excluding the condition of nasal polyp, sinonasal tumor, fungal sinusitis or sinonasal anatomic variations, however, what is the role of FESS in CRS with perceived moderate-to-severe symptoms? There were prior researches have studied the outcome of surgically treated patients of CRS.17-22 However, few literatures offered adequate discussions focusing on role of FESS for patients with perceived moderate-to-severe symptoms of CRS. The aim of this study was 1) to evaluate the correlation between subjective perception of symptom severity and objective assessment of disease severity. 2) to evaluate if atopic constitute affect the subjective and objective disease severity 3) to investigate. the. role. of. FESS. in. Rhinosinusitis.. 9. moderate-to-severe. Chronic.
(21) Materials and Methods Study Population This study was conducted in the Otolaryngology Clinics at China Medical University Hospital, Taichung and Chang Gung Memorial Hospital, Chiayi. Between September 2004 and November 2006, patients diagnosed as CRS and met our definition of perceived moderate-to-severe symptoms mentioned below were enrolled into our surgery.. Criteria of Chronic Rhinosinusitis Patients were required to have two or more major factors or one major and at least two minor factors for CRS with clinical symptoms for more than 12 consecutive weeks.3. Symptom Severity Evaluation We use Visual Analogue Score (VAS) Questionnaire (Table II and Table III) to evaluate CRS symptoms status as the primary outcome measure.23 Symptoms include nasal obstruction, rhinorrhea / postnasal drip, headache, facial pain and olfactory disturbance and overall discomfort. Each symptom was scored on a scale from 0 to 10 where 0. 10.
(22) presented no symptom and 10 presented the greatest severity of symptom. A numeric score between 0 and 10 is also given to overall discomfort (“how bad the patient feels”).. Selection of Patients with Perceived Moderate-to-Severe Symptoms of CRS According to the VAS questionnaire, patients with equal to or over 8 scales in at least two symptom items and overall discomfort scales also equal to or over 8 scales were included into our study. They were regarded as having moderate-to-severe symptoms of CRS.. Exclusion Criteria Patients with immunodeficiency, fungal sinusitis, nasal polyp, sinonasal tumor, sinonasal anatomic variations such as pneumatization of the middle turbinate (Concha bullosa) or severe deviated nasal septum were excluded. Patients who have experienced any prior sinonasal surgery were also excluded from our study.. 11.
(23) Data Collection Analysis of prospectively collected data in adult (18 years or older) patients with moderate-to-severe perceived symptoms of CRS for more than 12 weeks was performed. These patients filled the VAS Questionnaire in the initial visit. Patients’ history and medical records were reviewed to collect information such as age, sex, medical comorbidity, atopy status, duration of symptoms of CRS, current medication and history of nasal surgery. Nasal endoscopy and sinus CT scan were performed to collect baseline information.. Endoscopy Score Diagnostic nasal endoscopy was performed and given a score from 0 to 20 according to the scoring system proposed by Lund and Kennedy.23 (Table IV). CT Score Sinus CT film were assessed and given a score from 0 to 24 according to the Lund-Mackay scoring system for chronic. 12.
(24) rhinosinusitis.24 (Table V) Lund-Mackay staging system has excellent interrater and intrarater agreement.25. Allergen Testing Patients underwent allergen testing by checking specific IgE antibody in serum, Pharmacia CAP test or multiple allergens simultaneous test (MAST) was used.. Therapy of Chronic Rhinosinusitis with Severe Symptoms Medical Therapy Medical Therapy including mucolytics, antibiotics, intranasal steroid sprays and nasal irrigations was prescribed first for these patients of CRS.. Functional Endoscopic Sinus Surgery (FESS) FESS was suggested if patient was refractory to adequate medical treatment. Patients who did not want to receive surgery due to personal. 13.
(25) reasons or were medically unsuitable for surgery continued medical therapy.. Data Collection after 6 Months Later Patients who have undergone FESS completed VAS Questionnaire and were assessed with nasal endoscopy at least 6 months postoperatively. Those without FESS also completed VAS Questionnaire and were assessed with nasal endoscopy at least 6 months after initial visit.. Statistical Analysis All statistical analysis for this study was performed using SPSS version 13.0 statistical software (SPSS Inc, Chicago, III). P Value < 0.05 was considered significant and all the tests were two-tailed. Pearson correlation coefficient was used to test association between pretreatment VAS score, endoscope score and CT score. Student’s t-test was used to compare the VAS score, endoscopy score and CT score between atopy and non-atopy group in the pretreatment period. Student’s t-test was used to compare the outcome (difference in VAS score, endoscopy score between pre-treatment and. 14.
(26) post-treatment period) between atopy group and non-atopy group. General Linear Model, repeated measures was used to compare the outcome if considering both the two factors of atopy and surgery.. 15.
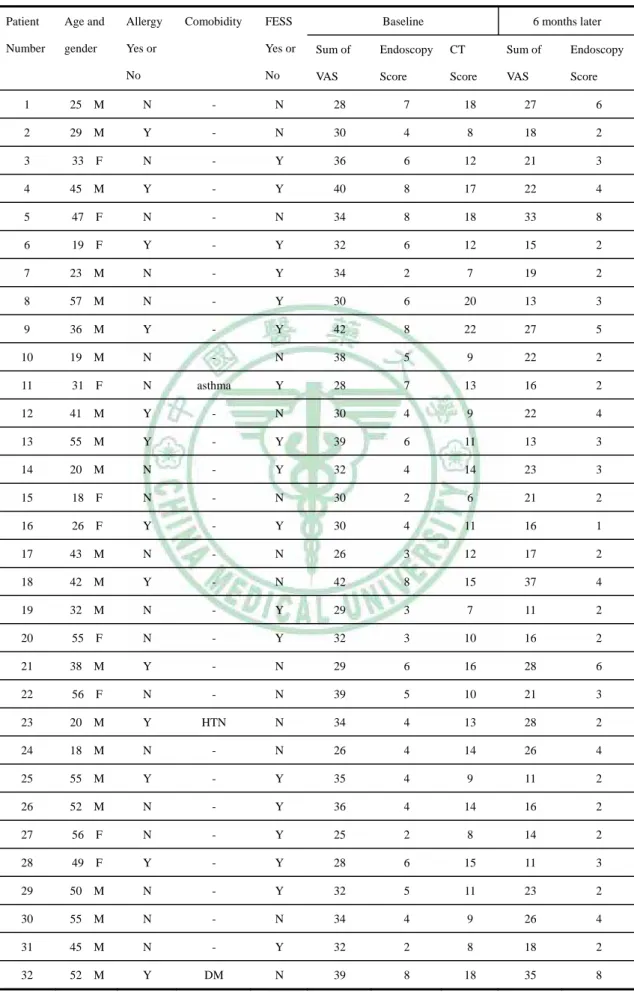
(27) Results Patient Characteristics Between September 2004 and November 2006, thirty two patients with complete pre-treatment VAS Questionnaire, nasal endoscopy, sinus CT film and post-treatment VAS Questionnaire, nasal endoscopic examination were included in this study. Table VI lists the pre-treatment and post-treatment data of patients in this study. Twenty two patients were male and 10 were female. The mean patient age was 38.2 years (range, 18-56 years). Mean follow-up period was 11.8 months (range, 7-19 months). There was one patient with hypertension (HTN), one patient with Diabetic Mellitus (DM) and another patient with asthma and all received medical treatment. Thirteen patients were allergen positive proved by specific IgE in serum; 19 patients were negative of atopy. Eighteen patients underwent FESS without major complications; sixteen patients received non-surgery therapy (Table VII).. Subjective and Objective Testing in Pre-treatment and Post-treatment Period The data in the pre-treatment period and post-treatment period (6. 16.
(28) months later) was demonstrated in Table VIII. The pre-treatment leading severe mean symptom scores were nasal obstruction (9.03 ± 1), followed by rhinorrhea, headache, facial pain and olfactory disturbance.. Correlation Analysis among the Subjective and Objective Testing The association between pre-treatment VAS score, endoscope score and CT score was analyzed with Pearson correlation coefficients which were showed in Table IX. The correlation coefficient between VAS score and endoscopy score was 0.491 (p <0.05, statistically significant). The correlation coefficient between endoscopy score and CT score was 0.8 (p <0.001, statistically significant). In contrast, there was no significant correlation between VAS score and CT score (p >0.05). That is, the objective CT score could not predict the subjective symptom severity, at least based on our study results.. The correlation of net change between VAS score and endoscopy score 6 months later was showed in Table X. The correlation coefficient. 17.
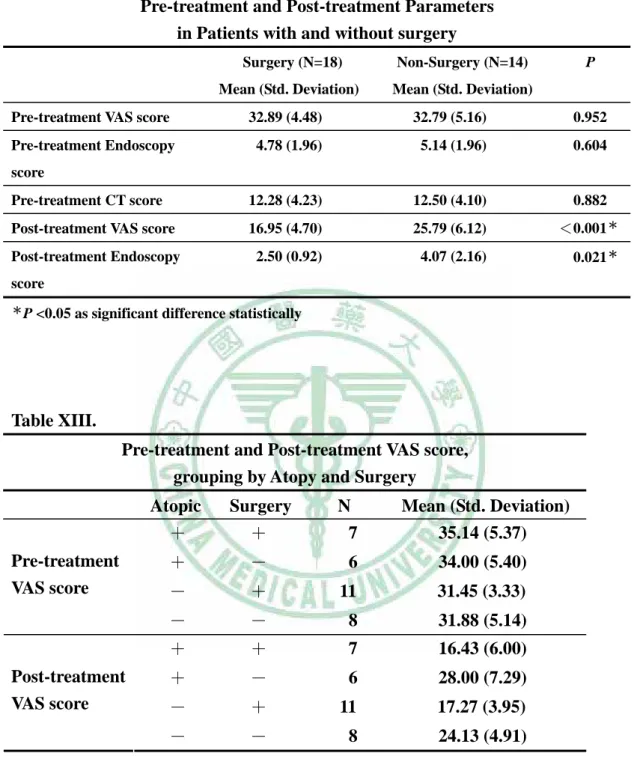
(29) of net change between VAS score and endoscopy score was 0.453 (p <0.05, statistically significant).. Comparison of Outcome for Atopic and Non-Atopic Patients The pretreatment VAS symptom score, endoscopy score, CT score in atopic group and non-atopic group were demonstrated in Table XI. There was no statistically significant difference in VAS score and CT score between atopic and non-atopic group in the pretreatment period (two sample t test, p >0.05). That is, atopic constitute could not predict higher VAS score and CT score in this study. However, the atopic group had significantly higher endoscope score than non-atopic group (two sample t test, p <0.05).. Comparison of Outcome for Surgically Treated and Non-Surgically Treated Patients The pre and post-treatment VAS symptom score, endoscopy score, CT score in surgical group and non-surgical group were demonstrated in Table XII. We compared the pre-treatment VAS symptom score,. 18.
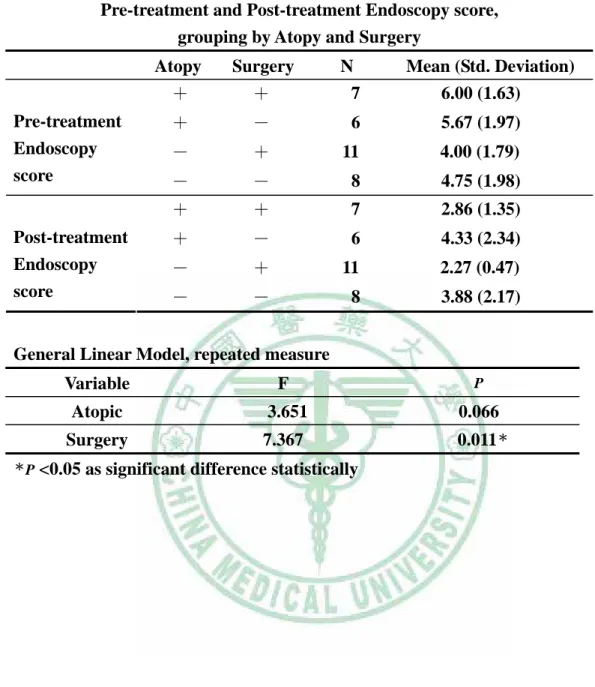
(30) endoscopy score, CT score and post-treatment VAS symptom score, endoscopy score in surgical group and non-surgical group. There was no statistically significant difference between surgical and non-surgical group in the three parameters in the pre-treatment period (p >0.05). However, the VAS score, endoscopy score had more marked reduction in surgical group than non-surgical group in the post-treatment period (p <0.05).. Comparison of Outcome, Considering Both Factors of Atopy and Surgery On the other hand, supposing to consider the atopy status, the surgical group also had more reduction in symptom score and endoscopy score (General Linear Model, repeated measure) (Table XIII, XIV).. 19.
(31) Discussion There has been a trend to evaluate the outcome of chronic rhinosinusitis with subjective symptom rating and objective measures (such as endoscope and CT scan).26-32 Although CT scan is widely accepted as an accurate diagnostic tool for CRS,11 the present study demonstrated that findings on the CT scan do not correlate with the severity of nasal symptoms. Other studies26,. 33-38. have found no. correlation between subjective quality-of-life questionnaire or sinonasal symptom scores and objective staging scores based on CT scan. The result may reflect the limitation that CT findings could not predict the symptom severity of CRS. Wabnitz et al.32 concluded that there was no significant correlation between the 20-item Sinonasal Outcome Test (SNOT-20) questionnaire and the Lund-Mackay CT score and between the Chronic Sinusitis Survey (CCS) and the Lund-Mackay CT score in his study. However, a weak but statistically significant correlation was found between the sum of five sinonasal VAS symptoms and the Lund-Mackay CT score. However, Kenny and colleagues39 disclosed that the severity of selected sinus symptoms correlated with the severity of CT imaging evidence for rhinosinusitis.. 20.
(32) The good correlation of net change between VAS score and endoscopy score was showed in our present study. This finding is similar to the study of Giger et al.19. They found that subjective symptom responses correlated quite well with objective endoscopic assessment of the post-operative sinonasal cavity. Nasal endoscopy displayed the detailed condition of sinonasal cavity such as edema, discharge and obstruction of ostium which may result in sinonasal symptoms. One explanation for no correlation between VAS sores and CT score is that single sinus lesion could give rise to severe symptoms such as headache and rhinorrhea. On the other hand, multiple sinus lesions might only cause mild symptoms. It should be realized that the subjective measures and objective measures essentially examine independent aspects of disease. Therefore, there may be no correlation between these measures. A potential limitation of this study is that the scores of symptom severity were obtained from patient-reported data. It is possible that patients overrated or underrated their symptom severity. However, the endoscope findings correlate with the subjective symptom severity. There was excellent correlation between the endoscope score and CT score.. 21.
(33) These two objective measures for chronic rhinosinusitis correlated with each other in this study. The little or lack of correlation between VAS symptom score and CT score does not suggest that one or both these measure are unhelpful. The VAS offers a reproducible and quantifiable evaluation of patient’s rhinosinusitis-specific symptoms, which is a better means of assessing symptom intensity. CT scan provides critical information about sinus anatomy and the extent of disease, both is critical in treatment planning.40, 41. It is important to integrate subjective assessment with objective. measure to realize the severity of CRS and to determine appropriate therapy. Except the Visual Analogue Symptom Score, we may use questionnaire for quality of life, such as Sino-Nasal Outcome Test 20 (SNOT-20) questionnaire. It is because data from SNOT-20 questionnaire could define clearly the burden of CRS in the study population. Besides, the Rhinosinusitis Disability Index (RSDI), Chronic Sinusitis Survey (CSS) could also offer more detailed information about impact for rhinosinusitis related quality of life. Certainly, patients of CRS expect not only symptomatic but also quality-of-life improvements.. 22.
(34) In our study, atopic CRS patients have significantly higher endoscopy score than non-atopic CRS patients. But there was no significant difference between atopic and non-atopic CRS patients on VAS symptom score and CT score in the pre-treatment period. The inconsistent result may be due to small sample size in the present study. Besides,. all. patients. included. in. our. study. have. perceived. moderate-to-severe symptoms. Therefore, the impact of atopy constitute affecting the VAS symptom score and CT score might be weakened in the present study. Savolainen found that 25% to 58% of individuals with sinusitis have allergic rhinitis.42 In addition, elevated levels of serum total IgE is a risk factor for the presence of severe chronic rhinosinusitis.43 The normal sinus physiology can be altered by allergic inflammation. The most commonly proposed mechanism is ostial obstruction. Allergic mucosal edema causes ostial obstruction that interferes with drainage and ventilation from the sinuses, promoting mucus accumulation, and decreased oxygenation within the sinuses. These changes result in impaired ciliary movement, retained secretions, and bacterial growth.44 Berrettini et al.45 reported computed tomography sinus abnormalities in. 23.
(35) 67.5% of perennial allergic rhinitis patients compared with 33.4% of controls. Nasal allergen challenges in sensitive individuals produce radiographic changes of the maxillary sinuses, including edema and opacification.46 Nasal allergen challenges produce significant increase in levels of eosinophils, eosinophil cationic protein, histamine, and albumin in the nose and maxillary sinus.47 If we consider both factors of surgery and atopy status, Table XIII and Table XIV revealed surgery (FESS) had statistically significant improvement in VAS score and endoscopic findings in the post-treatment period (6 months after baseline data) but atopy constitute did not show significant difference. This does not mean atopy constitute is not a predictor factor for outcome of CRS. Six months of follow-up period is not adequate to make conclusion. In fact, atopy affects the long term outcome. The VAS score, endoscopy score had more marked reduction in surgical group than non-surgical group in the present study. Functional endoscopic sinus surgery (FESS) played a beneficial role in treatment of patients with perceived moderate-to-severe symptoms of CRS. Bradley and Kountakis28 reported on 113 adult patients with 1 year of clinical. 24.
(36) follow-up after functional endoscopic sinus surgery (FESS). They found that a significant reduction in SNOT-20 symptom scores was achieved after FESS as early as 3 symptoms post-surgery. Overall composite symptoms were improved 3, 6 and 12 months after surgery. In a 3 years of follow-up study of 77 patients with CRS without polyposis, Giger et al.19 found 92% of patients showed a marked improvement in symptoms after FESS. The data in the literatures18, 20-22, 48-52 clearly support the use of FESS in patients with CRS who have been refractory to medical treatment. Some studies have dealt with special populations under FESS. For example, elderly patients may not be immediately considered as surgical candidates for CRS because of their old age and possible associated medical comorbidities making them higher risk for surgery. As revealed by Colclasure et al.53, patients over 60 years of age still obtained substantial symptomatic improvement after FESS. Batra et al.54 retrospectively reviewed 17 patients who underwent FESS with concomitant diagnosis of nasal polyps and steroid-dependent asthma. Patients experienced substantial improvements in the post-operative. 25.
(37) forced expiratory volume at 1 second. Twelve of the 17 patients (70.6%) experienced a reduction in systemic steroid use after surgery. For patients’ perception, symptom severity can easily be classified as none, mild, moderate and severe. It may not give rise to medical attention if the symptoms of CRS are none or mild. Medical treatment is reasonable to treat patients with mild symptoms of CRS in the initial stage. For patients with severe symptoms of CRS, surgical intervention is indicated if they have been refractory to medical treatment. If CRS is due to nasal polyp, sinonasal tumor, fungal infection or identified sinonasal anatomic variations such as Concha bullosa or severe deviated nasal septum, surgical intervention is indicated and is helpful. CRS with nasal polyp is also a common disease but it is distinct from CRS without nasal polyps in histopathogenesis.8 The presence of nasal polyps has a significant negative impact on patients with CRS. Patients with nasal polyps have more severe symptoms with less improvement after surgical intervention, higher CT scores at presentation, and a significantly higher need for revision surgery.55-58 As for patients with perceived moderate-to-severe symptoms of CRS but without condition of nasal polyp, sinonasal tumor, fungal. 26.
(38) sinusitis or sinonasal anatomic variations, few literatures offered adequate discussions focusing this issue. Our present study concluded that FESS played a beneficial role for patients with perceived moderate-to-severe symptoms.. Limitations There are some limitations in this study. First of all, as mentioned above,. the. scores. of. symptom. severity. were. obtained. from. patient-reported data. It is possible that patients overrated or underrated their symptom severity. Potential biases in the patient-reported data should be kept in mind when analyzing these data. A second limitation of this study is lack of long-term follow-up. For the moment, the shortest and longest follow-up period is only 7 months and 19 months respectively. The follow-up time point of complete questionnaire and nasal endoscopy examination is only at 6 months after surgical or non-surgical treatment. Long-term outcomes with similar measures are needed. We should keep following up these patients and add the time point of complete questionnaire and endoscope examination whenever they returned to the clinic every 6 months.. 27.
(39) Thirdly, although there were 32 patients enrolled into this study, some patients were not included because of lost of follow-up. Some patients disinclined to spend time returning to clinics because they felt much improved for symptoms of CRS. However, some patients felt no improved for symptoms of CRS and looked for other clinics.. 28.
(40) Conclusions This study demonstrated that findings on the CT scan do not correlate with the severity of nasal symptoms. Although atopy constitute is an important factor, there was no significant difference between atopic and non-atopic CRS patients on VAS symptom score and CT score in the pre-treatment period in the present study. We need more sample size to prove atopy affect the disease severity in perception and CT findings. The VAS score, endoscopy score had more marked reduction in surgical group than non-surgical group. For patients with moderate-to-severe symptoms of CRS, if they have been refractory to adequate medical treatment, functional endoscopic sinus surgery (FESS) is an effective treatment method.. Suggestions The amount of study subjects and the follow-up period are not adequate in the present study. In the future, more study subjects and long-term follow-ups are needed.. 29.
(41) References 1. Bailey BJ. Head and Neck Surgery-Otolaryngology. Lippincott Williams & Wilkins; 2001:321-327.. 2. Gliklich RE, Metson R. The health impact of chronic sinusitis in patients seeking otolaryngologic care. Otolaryngol Head Neck Surg. 1995;113:104-109.. 3. Lanza DC, Kennedy DW. Adult rhinosinusitis defined. Otolaryngol Head Neck Surg. 1997;117:S1-7.. 4. Pawankar R, Nonaka M, Yamagishi S, Yagi T. Pathophysiologic mechanisms of chronic rhinosinusitis. Immunol Allergy Clin North Am. 2004;24:75-85.. 5. Benninger MS, Ferguson BJ, Hadley JA, et al. Adult chronic rhinosinusitis: Definitions, diagnosis, epidemiology, and pathophysiology. Otolaryngol Head Neck Surg. 2003;129:S1-32.. 6. Rhyoo C, Sanders SP, Leopold DA, Proud D. Sinus mucosal IL-8 gene expression in chronic rhinosinusitis. J Allergy Clin Immunol. 1999;103:395-400.. 30.
(42) 7. Cheng YK, Lin CD, Chang WC, et al. Increased prevalence of interleukin-1 receptor antagonist gene polymorphism in patients with chronic rhinosinusitis. Arch Otolaryngol Head Neck Surg. 2006;132:285-290.. 8. Polzehl D, Moeller P, Riechelmann H, Perner S. Distinct features of chronic rhinosinusitis with and without nasal polyps. Allergy. 2006;61:1275-1279.. 9. Zinreich SJ. Imaging of chronic sinusitis in adults: X-ray, computed tomography, and magnetic resonance imaging. J Allergy Clin Immunol. 1992;90:445-451.. 10. Aalokken TM, Hagtvedt T, Dalen I, Kolbenstvedt A. Conventional sinus radiography compared with CT in the diagnosis of acute sinusitis. Dentomaxillofac Radiol. 2003;32:60-62.. 11. Bhattacharyya N, Fried MP. The accuracy of computed tomography in the diagnosis of chronic rhinosinusitis. Laryngoscope. 2003;113:125-129.. 12. Scadding GK. Medical management of chronic rhinosinusitis.. 31.
(43) Immunol Allergy Clin North Am. 2004;24:103-118.. 13. Messerklinger W. Endoscopy technique of the middle nasal meatus (author's transl). Arch Otorhinolaryngol. 1978;221:297-305.. 14. Messerklinger W. Background and evolution of endoscopic sinus surgery. Ear Nose Throat J. 1994;73:449-450.. 15. Witterick IJ, Kolenda J. Surgical management of chronic rhinosinusitis. Immunol Allergy Clin North Am. 2004;24:119-134.. 16. Hopkins C, Browne JP, Slack R, et al. Complications of surgery for nasal polyposis and chronic rhinosinusitis: The results of a national audit in england and wales. Laryngoscope. 2006;116:1494-1499.. 17. Damm M, Quante G, Jungehuelsing M, Stennert E. Impact of functional endoscopic sinus surgery on symptoms and quality of life in chronic rhinosinusitis. Laryngoscope. 2002;112:310-315.. 18. Bhattacharyya N. Symptom outcomes after endoscopic sinus surgery for chronic rhinosinusitis. Arch Otolaryngol Head Neck Surg. 2004;130:329-333.. 19. Giger R, Dulguerov P, Quinodoz D, et al. Chronic panrhinosinusitis 32.
(44) without nasal polyps: Long-term outcome after functional endoscopic sinus surgery. Otolaryngol Head Neck Surg. 2004;131:534-541.. 20. Iro H, Mayr S, Wallisch C, Schick B, Wigand ME. Endoscopic sinus surgery: Its subjective medium-term outcome in chronic rhinosinusitis. Rhinology. 2004;42:200-206.. 21. Khalid AN, Quraishi SA, Kennedy DW. Long-term quality of life measures after functional endoscopic sinus surgery. Am J Rhinol. 2004;18:131-136.. 22. Poetker DM, Smith TL. Adult chronic rhinosinusitis: Surgical outcomes and the role of endoscopic sinus surgery. Curr Opin Otolaryngol Head Neck Surg. 2007;15:6-9.. 23. Lund VJ, Kennedy DW. Quantification for staging sinusitis. The staging and therapy group. Ann Otol Rhinol Laryngol Suppl. 1995;167:17-21.. 24. Lund VJ, Mackay IS. Staging in rhinosinusitus. Rhinology. 1993;31:183-184.. 25. Oluwole M, Russell N, Tan L, Gardiner Q, White P. A comparison of. 33.
(45) computerized tomographic staging systems in chronic sinusitis. Clin Otolaryngol Allied Sci. 1996;21:91-95.. 26. Smith TL, Rhee JS, Loehrl TA, Burzynski ML, Laud PW, Nattinger AB. Objective testing and quality-of-life evaluation in surgical candidates with chronic rhinosinusitis. Am J Rhinol. 2003;17:351-356.. 27. Bhattacharyya N. A comparison of symptom scores and radiographic staging systems in chronic rhinosinusitis. Am J Rhinol. 2005;19:175-179.. 28. Bradley DT, Kountakis SE. Correlation between computed tomography scores and symptomatic improvement after endoscopic sinus surgery. Laryngoscope. 2005;115:466-469.. 29. McMains KC, Kountakis SE. Revision functional endoscopic sinus surgery: Objective and subjective surgical outcomes. Am J Rhinol. 2005;19:344-347.. 30. Smith TL, Mendolia-Loffredo S, Loehrl TA, Sparapani R, Laud PW, Nattinger AB. Predictive factors and outcomes in endoscopic sinus. 34.
(46) surgery for chronic rhinosinusitis. Laryngoscope. 2005;115:2199-2205.. 31. Stewart MG, Smith TL. Objective versus subjective outcomes assessment in rhinology. Am J Rhinol. 2005;19:529-535.. 32. Wabnitz DA, Nair S, Wormald PJ. Correlation between preoperative symptom scores, quality-of-life questionnaires, and staging with computed tomography in patients with chronic rhinosinusitis. Am J Rhinol. 2005;19:91-96.. 33. Bhattacharyya T, Piccirillo J, Wippold FJ,2nd. Relationship between patient-based descriptions of sinusitis and paranasal sinus computed tomographic findings. Arch Otolaryngol Head Neck Surg. 1997;123:1189-1192.. 34. Stewart MG, Sicard MW, Piccirillo JF, Diaz-Marchan PJ. Severity staging in chronic sinusitis: Are CT scan findings related to patient symptoms? Am J Rhinol. 1999;13:161-167.. 35. Krouse JH. Computed tomography stage, allergy testing, and quality of life in patients with sinusitis. Otolaryngol Head Neck Surg.. 35.
(47) 2000;123:389-392.. 36. Arango P, Kountakis SE. Significance of computed tomography pathology in chronic rhinosinusitis. Laryngoscope. 2001;111:1779-1782.. 37. Bhattacharyya N. Radiographic stage fails to predict symptom outcomes after endoscopic sinus surgery for chronic rhinosinusitis. Laryngoscope. 2006;116:18-22.. 38. Bhattacharyya N. Clinical and symptom criteria for the accurate diagnosis of chronic rhinosinusitis. Laryngoscope. 2006;116:1-22.. 39. Kenny TJ, Duncavage J, Bracikowski J, Yildirim A, Murray JJ, Tanner SB. Prospective analysis of sinus symptoms and correlation with paranasal computed tomography scan. Otolaryngol Head Neck Surg. 2001;125:40-43.. 40. Branstetter IV BF, Weissman JL. Role of MR and CT in the paranasal sinuses. Otolaryngol Clin North Am. 2005;38:1279-1299.. 41. Reider JM, Nashelsky J, Neher J. Clinical inquiries. do imaging studies aid diagnosis of acute sinusitis? J Fam Pract.. 36.
(48) 2003;52:565-567.. 42. Savolainen S. Allergy in patients with acute maxillary sinusitis. Allergy. 1989;44:116-122.. 43. Newman LJ, Platts-Mills TA, Phillips CD, Hazen KC, Gross CW. Chronic sinusitis. relationship of computed tomographic findings to allergy, asthma, and eosinophilia. JAMA. 1994;271:363-367.. 44. Krause HF. Allergy and chronic rhinosinusitis. Otolaryngol Head Neck Surg. 2003;128:14-16.. 45. Berrettini S, Carabelli A, Sellari-Franceschini S, et al. Perennial allergic rhinitis and chronic sinusitis: Correlation with rhinologic risk factors. Allergy. 1999;54:242-248.. 46. Pelikan Z, Pelikan-Filipek M. Role of nasal allergy in chronic maxillary sinusitis--diagnostic value of nasal challenge with allergen. J Allergy Clin Immunol. 1990;86:484-491.. 47. Baroody F, deTineo M, Haney L, Clark K, Blair C, Naclerio R. University of chicago, chicago, il. influx of eosinophils into the maxillary sinus after nasal challenge with allergen. J Allergy Clin. 37.
(49) Immunol. 2000;105.. 48. Bhattacharyya N. Clinical outcomes after endoscopic sinus surgery. Curr Opin Allergy Clin Immunol. 2006;6:167-171.. 49. Salhab M, Matai V, Salam MA. The impact of functional endoscopic sinus surgery on health status. Rhinology. 2004;42:98-102.. 50. Durr DG, Desrosiers M. Evidence-based endoscopic sinus surgery. J Otolaryngol. 2003;32:101-106.. 51. Toros SZ, Bolukbasi S, Naiboglu B, et al. Comparative outcomes of endoscopic sinus surgery in patients with chronic sinusitis and nasal polyps. Eur Arch Otorhinolaryngol. 2007.. 52. Kaplan BA, Kountakis SE. Role of nasal endoscopy in patients undergoing endoscopic sinus surgery. Am J Rhinol. 2004;18:161-164.. 53. Colclasure JC, Gross CW, Kountakis SE. Endoscopic sinus surgery in patients older than sixty. Otolaryngol Head Neck Surg. 2004;131:946-949.. 54. Batra PS, Kern RC, Tripathi A, et al. Outcome analysis of endoscopic 38.
(50) sinus surgery in patients with nasal polyps and asthma. Laryngoscope. 2003;113:1703-1706.. 55. Deal RT, Kountakis SE. Significance of nasal polyps in chronic rhinosinusitis: Symptoms and surgical outcomes. Laryngoscope. 2004;114:1932-1935.. 56. Wynn R, Har-El G. Recurrence rates after endoscopic sinus surgery for massive sinus polyposis. Laryngoscope. 2004;114:811-813.. 57. Alobid I, Benitez P, Valero A, et al. The impact of atopy, sinus opacification, and nasal patency on quality of life in patients with severe nasal polyposis. Otolaryngol Head Neck Surg. 2006;134:609-612.. 58. Alobid I, Benitez P, Bernal-Sprekelsen M, et al. Nasal polyposis and its impact on quality of life: Comparison between the effects of medical and surgical treatments. Allergy. 2005;60:452-458.. 39.
(51) Appendix Tables Table I. Symptom factors in the diagnosis of chronic rhinosinusitis (1996 Task Force) Major Factors. Minor Factors. Facial pain / pressure* Facial congestion / fullness Nasal obstruction / blockage Nasal discharge / purulence / discolored postnasal drainage Hyposmia / anosmia Purulence on nasal cavity examination. Headache Fever Halitosis Fatigue Dental pain Cough Ear pain / pressure / fullness. *Facial. pain/pressure alone does not constitute a suggestive history for rhinosinusitis in the absence of another major nasal symptom or sign. Fever in acute sinusitis alone does not constitute a strongly suggestive history for rhinosinusitis in the absence of another major nasal symptom or sign. 40.
(52) Table II.. Visual Analogue Score (VAS) Questionnaire 視覺類比症狀評分問卷 日期:. 姓名:. . 病歷號碼:. 為了讓我們能更瞭解您的鼻炎或鼻竇炎情況,請您自我評估症狀的嚴重程度, 從 0 分到 10 分勾選最符合的分數。 完全沒有症狀:0 分. 症狀最嚴重:10 分. 1、鼻塞 □. □. □. □. 0 1 2 3 2、流鼻涕、鼻涕倒流 □ □ □ □. □. □. □. □. □. □. □. 4. 5. 6. 7. 8. 9. 10. □. □. □. □. □. □. □. 0 3、頭痛. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. □. □. □. □. □. □. □. □. □. □. □. 2. 3. 4. 5. 6. 7. 8. 9. 10. □. □. □. □. □. □. □. □. □. 2. 3. 4. 5. 6. 7. 8. 9. 10. 0 1 4、臉部壓痛 □ □ 0 1 5、嗅覺損失 □. □. □. □. □. □. □. □. □. □. □. 0. 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 6、綜合以上五大症狀,鼻炎或鼻竇炎症狀困擾您的嚴重程度? □ □ □ □ □ □ □ □ □ □ 0. 1. 2. 3. 4. 5. 謝謝您填寫問卷!. 41. 6. 7. 8. 9. □ 10.
(53) Table III. VAS symptom score Symptom (score by visual analogue method). Baseline. 6 months later. Nasal obstruction (1-10) Nasal discharge (1-10) Headache (1-10) Facial pain or pressure (1-10) Olfactory disturbance (1-10) Overall discomfort (1-10) Total points each visit 0: symptom not present; 10: greatest severity Adapted from Lund VJ, Kennedy DW. Quantification for staging sinusitis. Ann Otol Rhinol Laryngol Suppl. 1995;167:17-21. Table IV. Endoscopic appearances score Characteristic. Baseline. 6 months later. Polyp, left (0,1,2) Polyp, right (0,1,2) Edema, left (0,1,2) Edema, right (0,1,2) Discharge, left (0,1,2) Discharge, right (0,1,2) Scarring, left * (0,1,2) Scarring, right * (0,1,2) Crusting, left * (0,1,2) Crusting, right * (0,1,2) Total points Scoring: For polyps: 0 = absence of polyps, 1 = polyps in middle meatus only, 2 = polyps beyond middle meatus. For edema, scarring, and crusting: 0 = absent, 1 = mild, 2 = severe. For discharge: 0 = no discharge, 1 = clear, thin discharge, 2 = thick, purulent discharge. *Postoperative scores to be used for outcome assessment only. Adapted from Lund VJ, Kennedy DW. Quantification for staging sinusitis. Ann Otol Rhinol Laryngol Suppl. 1995;167:17-21 42.
(54) Table V. Lund and Mackay Sinus CT Grading System Sinus system. Left. Right. Maxillary (0,1,2) Anterior ethmoids (0,1,2) Posterior ethmoids (0,1,2) Sphenoid (0,1,2) Frontal (0,1,2) Ostiomeatal complex (0 or 2 only) Total points for each side Scoring: For all sinus systems, except the ostiomeatal complex: 0 = no abnormalities, 1 = partial opacification, 2 = total opacification. For the ostiomeatal complex: 0 = not occluded, 2 = occluded... Adapted from Lund VJ, Kennedy DW. Quantification for staging sinusitis. Ann Otol Rhinol Laryngol Suppl. 1995;167:17-21. 43.
(55) Table VI. Data of Patients Comobidity. FESS. Patient. Age and. Allergy. Baseline. 6 months later. Number. gender. Yes or. Yes or. Sum of. Endoscopy. CT. Sum of. Endoscopy. No. No. VAS. Score. Score. VAS. Score. 1. 25 M. N. -. N. 28. 7. 18. 27. 6. 2. 29 M. Y. -. N. 30. 4. 8. 18. 2. 3. 33 F. N. -. Y. 36. 6. 12. 21. 3. 4. 45 M. Y. -. Y. 40. 8. 17. 22. 4. 5. 47 F. N. -. N. 34. 8. 18. 33. 8. 6. 19 F. Y. -. Y. 32. 6. 12. 15. 2. 7. 23 M. N. -. Y. 34. 2. 7. 19. 2. 8. 57 M. N. -. Y. 30. 6. 20. 13. 3. 9. 36 M. Y. -. Y. 42. 8. 22. 27. 5. 10. 19 M. N. -. N. 38. 5. 9. 22. 2. 11. 31 F. N. asthma. Y. 28. 7. 13. 16. 2. 12. 41 M. Y. -. N. 30. 4. 9. 22. 4. 13. 55 M. Y. -. Y. 39. 6. 11. 13. 3. 14. 20 M. N. -. Y. 32. 4. 14. 23. 3. 15. 18 F. N. -. N. 30. 2. 6. 21. 2. 16. 26 F. Y. -. Y. 30. 4. 11. 16. 1. 17. 43 M. N. -. N. 26. 3. 12. 17. 2. 18. 42 M. Y. -. N. 42. 8. 15. 37. 4. 19. 32 M. N. -. Y. 29. 3. 7. 11. 2. 20. 55 F. N. -. Y. 32. 3. 10. 16. 2. 21. 38 M. Y. -. N. 29. 6. 16. 28. 6. 22. 56 F. N. -. N. 39. 5. 10. 21. 3. 23. 20 M. Y. HTN. N. 34. 4. 13. 28. 2. 24. 18 M. N. -. N. 26. 4. 14. 26. 4. 25. 55 M. Y. -. Y. 35. 4. 9. 11. 2. 26. 52 M. N. -. Y. 36. 4. 14. 16. 2. 27. 56 F. N. -. Y. 25. 2. 8. 14. 2. 28. 49 F. Y. -. Y. 28. 6. 15. 11. 3. 29. 50 M. N. -. Y. 32. 5. 11. 23. 2. 30. 55 M. N. -. N. 34. 4. 9. 26. 4. 31. 45 M. N. -. Y. 32. 2. 8. 18. 2. 32. 52 M. Y. DM. N. 39. 8. 18. 35. 8. 44.
(56) Table VII. Gender, atopy status and method of therapy of study population gender number. Table VIII.. Mean and standard deviation of parameters Rhinorrhea. atpoic 13. method of therapy. male 22. Nasal. female 10. atopy status. Headache. obstruction. non-atopic 19. surgery 18. non-surgery 14. Facial. Olfactory. Sum of. Endoscopy. CT. pain. disturbance. VAS. score. score. Pre-. 9.03. 8.81. 6.06. 4.81. 4.13. 32.84. 4.94. 12.38. treatment. (1.00). (1.31). (1.72). (1.63). (1.95). (4.71). (1.93). 4.10). Post-. 5.50. 5.31. 3.81. 3.44. 2.75. 20.81. 3.18. treatment. (2.06). (1.93). (1.55). (1.46). (1.81). (6.90). (1.75). -. 6 months. Table IX. Correlation Analysis for pre-treatment VAS score, Endoscopy score and CT score VAS score VAS score Correlation. Pearson. Endoscope score Correlation. Pearson. CT score Correlation. Pearson. **Correlation. 1. P. P. P. 0.491** 0.004 0.252 0.164. is significant at the 0.01 level. 45. Endoscopy score 0.491** 0.004 1 0.800** <0.001. CT score 0.252 0.164 0.800** <0.001 1.
(57) Table X. Correlation Analysis for net change of VAS score and Endoscopy score in 6 months later VAS score net change VAS score Correlation net change. Pearson. Endoscope score Correlation Net change. Pearson. **Correlation. Endoscopy score net change 0.453** 0.009. 1. P. 0.453** 0.009. P. 1. is significant at the 0.01 level. Table XI. Pre-treatment Parameters in atopic patients and non-atopic patients Atopic (N=13). Non-atopic (N=19). Mean (Std.. Mean (Std. Deviation). P. Deviation) Pre-treatment VAS score. 34.62 (5.19). 31.63 (4.06). Pre-treatment Endoscopy. 5.85 (1.72). 4.32 (1.86). 13.54 (4.10). 11.58 (4.02). 0.078 0.025*. score Pre-treatment CT score *P. <0.05 as significant difference statistically. 46. 0.189.
(58) Table XII. Pre-treatment and Post-treatment Parameters in Patients with and without surgery Surgery (N=18). Non-Surgery (N=14). Mean (Std. Deviation). Mean (Std. Deviation). P. Pre-treatment VAS score. 32.89 (4.48). 32.79 (5.16). 0.952. Pre-treatment Endoscopy. 4.78 (1.96). 5.14 (1.96). 0.604. Pre-treatment CT score. 12.28 (4.23). 12.50 (4.10). 0.882. Post-treatment VAS score. 16.95 (4.70). 25.79 (6.12). <0.001*. Post-treatment Endoscopy. 2.50 (0.92). 4.07 (2.16). 0.021*. score. score *P. <0.05 as significant difference statistically. Table XIII. Pre-treatment and Post-treatment VAS score, grouping by Atopy and Surgery Atopic +. Surgery +. +. -. 6. 34.00 (5.40). -. +. 11. 31.45 (3.33). -. -. 8. 31.88 (5.14). +. +. 7. 16.43 (6.00). Post-treatment. +. -. 6. 28.00 (7.29). VAS score. -. +. 11. 17.27 (3.95). -. -. 8. 24.13 (4.91). Pre-treatment VAS score. N 7. Mean (Std. Deviation) 35.14 (5.37). General Linear Model, repeated measure. *P. Variable. F. P. Atopy. 0.634. 0.433. Surgery. 30.027. < 0.001*. <0.05 as significant difference statistically. 47.
(59) Table XIV. Pre-treatment and Post-treatment Endoscopy score, grouping by Atopy and Surgery. Pre-treatment Endoscopy score. Post-treatment Endoscopy score. Atopy +. Surgery +. N 7. Mean (Std. Deviation) 6.00 (1.63). +. -. 6. 5.67 (1.97). -. +. 11. 4.00 (1.79). -. -. 8. 4.75 (1.98). +. +. 7. 2.86 (1.35). +. -. 6. 4.33 (2.34). -. +. 11. 2.27 (0.47). -. -. 8. 3.88 (2.17). General Linear Model, repeated measure. *P. Variable. F. P. Atopic. 3.651. 0.066. Surgery. 7.367. 0.011*. <0.05 as significant difference statistically. 48.
(60)
數據
+4

相關文件
functional impairment: A systematic literature review." Journal of the American Geriatrics Society 64.1 (2016):
Iwaki et al., “Oral malignant melanoma in Japan,” Oral Surgery, Oral Medicine, Oral Pathology, vol.. Myers, “Melanoma of the head and neck: current concepts in staging, diagnosis,
The results were mainly divided into 4 major groups based on origin of the genetic family: American, Caucasian, East Asian and Pacific, and African and South Asian.. American
A sixty-year-old female patient came to the Department of Oral and Maxillofacial Surgery, Faculty of Dental Medicine, Cairo University, complaining of bilateral swellings in
Introduction: Eagle’s syndrome is a rare condition that refers to chronic recurrent pain in the oropharynx, face, and neck due to elongation of the styloid process or calcification
Surgery was indicated and carried out by using a lateral transcervical approach for complete resection of the gland, which was based on the calculation of the total volume of
Distant Metastases Staging (M0) and Detection of Synchronous
Lemma 3 An American call or a European call on a non-dividend-paying stock is never worth less than its intrinsic value.. • An American call cannot be worth less than its
