210 J Formos Med Assoc | 2006 • Vol 105 • No 3 J. Hung, et al
Background: Smoking cessation programs are critical to the safety and health of workers. Exhaled carbon monoxide (CO) is an effective indicator of smoking in clinics and hospitals. Its application in the community and workplace, however, remains limited. This study assessed whether exhaled CO concentration can be used as an objective indicator of the amount of daily cigarette consumption among smokers in the workplace in Taiwan.
Methods: A total of 150 workers from a chemical manufacturer in Taiwan were included; there were 27 nonsmokers and 123 current smokers. The number of cigarettes smoked daily by each subject was reported, and exhaled CO concentration was measured in each subject using the Micro CO meter (Micro Medical Ltd, Chatham, Kent, UK).
Results: Exhaled CO levels were associated with the number of cigarettes consumed daily, with a correlation coefficient of 0.73 (p < 0.01) and an adjusted R-square (simple linear regression model) of 0.44. The mean exhaled CO level of nonsmokers was 4.2 ppm (95% confidence interval, 3.3–5.1). A reading of > 6 ppm had a sensitivity of 84% and specificity of 85% in detecting workplace smoking.
Conclusion: Exhaled CO level can be used as an objective, noninvasive indicator to determine the smoking status of an individual in the workplace. [J Formos Med Assoc 2006;105(3):210–213]
Key Words: cigarette, exhaled carbon monoxide, smoking cessation, workplace
○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○ ○
Institute of Occupational Medicine and Industrial Hygiene, College of Public Health, National Taiwan University, Taipei, Taiwan.
Received: February 17, 2005 Revised: June 13, 2005 Accepted: August 2, 2005
Despite the fact that smoking is associated, both etiologically and prognostically, with numerous diseases, the prevalence of smoking remains high in Taiwan, with adult smoking prevalence at 45.9% and 6.2% for males and females, re-spectively.1
Consequently, the implementation of effective smoking cessation programs is very im-portant; such programs require a valid and con-venient method of monitoring smoking status to assess program effectiveness. In addition, demon-stration of the immediate and potentially harmful consequence of smoking by using a portable de-vice might increase a smoker’s compliance with the cessation program.2
*Correspondence to: Dr. Chang-Chuan Chan, Room 1447, Institute of Occupational Medicine and Industrial Hygiene, College of Public Health, National Taiwan University, No. 1, Section 1, Jen-Ai Road, Taipei 100, Taiwan. E-mail: ccchan@ha.mc.ntu.edu.tw
Some methods for distinguishing smokers from nonsmokers, such as the measurement of nico-tine, cotinine, or thiocyanate levels in the plasma or urine, are either invasive or time consuming.3 Exhaled carbon monoxide (CO) level is well cor-related with blood carboxyhemoglobin level;4–6
it has also been reported to be highly correlated with smoking status, and measuring exhaled CO level using a portable and noninvasive CO moni-tor has been widely adopted for assessing individ-uals’ smoking status.2,3,7
The Tobacco Hazards Prevention Act was pro-mulgated in Taiwan in 1997, and a series of smok-ing cessation programs were implemented both ORIGINAL ARTICLE
Exhaled Carbon Monoxide Level as an
Indicator of Cigarette Consumption in a
Workplace Cessation Program in Taiwan
Jane Hung, Ching-Hua Lin, Jung-Der Wang, Chang-Chuan Chan*
211
J Formos Med Assoc | 2006 • Vol 105 • No 3
Exhaled CO and smoking
calibrated with a mixture of 50 ppm CO in air. Subjects were asked not to smoke for at least 1 hour before CO measurement. Subjects were instructed to exhale completely, inhale fully, hold their breath for 15 seconds, and then to exhale rapidly into a disposable mouthpiece, from which the reading of CO level can be directly obtained. The measure-ment was performed twice. There was no passive smoking in the workplace, and the mean ambient CO concentration during the study period was 0.4 ppm (as detected in the nearby monitor station).
Statistical analysis
All statistical analyses were conducted using SAS version 8.2 (SAS Institute Inc, Cary, NC, USA). Descriptive summary statistics, Spearman’s cor-relation analyses, and simple linear regression model were used to evaluate the relationship be-tween exhaled CO level and the amount of daily cigarette consumption. The CO concentration giv-ing the optimum sensitivity and specificity was selected as the cut-off point for differentiating smokers from nonsmokers using a two-by-two table.
Results
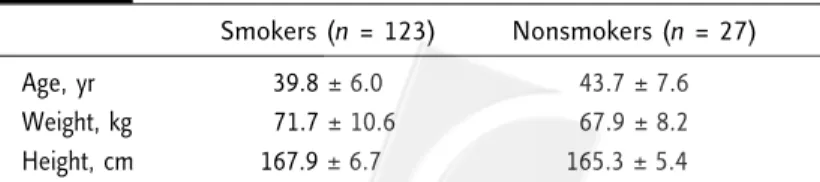
The age, weight, and height of subjects in the smoking and nonsmoking groups are shown in Table 1. All subjects were male. According to their medical records, none of the subjects had any significant respiratory or cardiovascular diseases. The mean amount of daily cigarette consumption (± standard deviation) among the current smok-ers was 14.7 ± 7.5 cigarettes/day. Exhaled CO lev-els were detectable in all subjects. Table 2 shows officially and privately.8,9 Questions regarding
dai-ly cigarette consumption are often asked through-out the course of such programs. However, many smokers deny or under-report their real cigarette consumption, making it impossible to obtain an accurate assessment.
Smoking cessation programs are especially im-portant in the workplace, particularly in chemical manufacturing, due to the additional safety con-cerns. Smoking behavior in the workplace is often subjected to additional restrictions compared to that in the community, usually for safety reasons. Workers tend to smoke less during working hours than during other activities. This might affect the exhaled CO level measured in the workplace.
The objective of this study was to evaluate the feasibility of using exhaled CO monitoring to as-sess the smoking status among workers in a chem-ical manufacturing plant, as part of a workplace smoking cessation program.
Methods
In 2003, a smoking cessation program was con-ducted in a chemical manufacturing plant employ-ing 300 workers in Taiwan. A total of 150 workers were recruited to participate in the program. Among them, 27 were nonsmokers and the other 123 were current smokers. A nonsmoker was defined as an individual who had not smoked for at least 1 year before the study, and a smoker was defined as an individual who had smoked regular-ly in the past 1 year. Worksite smoking prohibi-tion at the chemical manufacturing plant had been a company policy enforced since 1997, and workers were only allowed to smoke in designated smoking areas outside of buildings. All subjects were informed of the purpose of the study, and they were reassured that the results would be kept confidential to encourage accurate reporting of smoking history. They were asked about their medical and smoking histories. Exhaled CO level was measured in parts per million (ppm) using a Micro CO meter (Micro Medical Ltd, Chatham, Kent, UK). Prior to the study, the CO meter was
Table 1. Age, body weight and height of subjects*
Smokers (n = 123) Nonsmokers (n = 27)
Age, yr 39.8 ± 6.0 43.7 ± 7.6
Weight, kg 071.7 ± 10.6 67.9 ± 8.2
Height, cm 167.9 ± 6.70 165.3 ± 5.40
*All subjects were male, and none had any significant respiratory or cardiovascular diseases. Data presented as mean ± standard deviation.
212 J Formos Med Assoc | 2006 • Vol 105 • No 3 J. Hung, et al
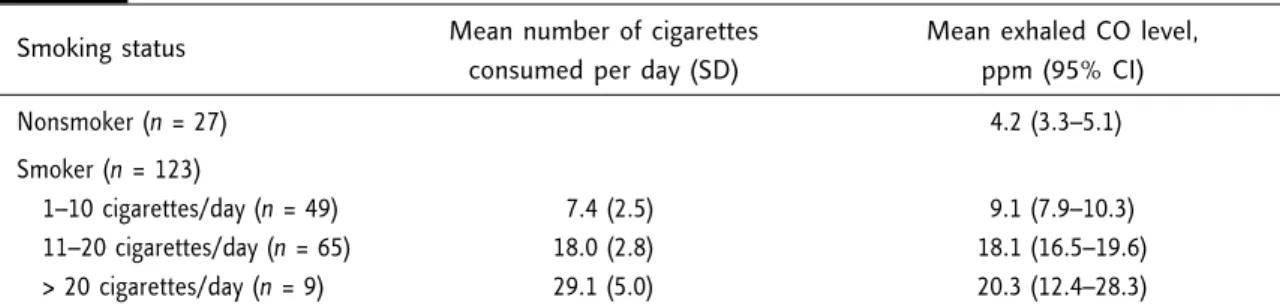
the mean exhaled CO levels of the subjects with different smoking status. The mean exhaled CO level of nonsmokers was 4.2 ppm (95% confi-dence interval, 3.3–5.1). A CO reading > 6 ppm suggested that the individual might be a smoker with a sensitivity and specificity of 84% and 85%, respectively. There was a significant positive cor-relation between exhaled CO level and the self-reported amount of daily cigarette consumption (r = 0.73, p < 0.01, Spearman’s test). The regres-sion coefficient in the simple regresregres-sion model was 0.70 (F value = 97.1, p < 0.01, adjusted R-square = 0.44) (Figure).
Discussion
Although many factors might affect exhaled CO level, the most likely cause of high levels of
CO exposure is smoking.2 The time period between the last cigarette smoked and CO measurement is an important consideration in individual smok-ing status accordsmok-ing to the exhaled CO level. This might explain why the mean exhaled CO level of those consuming 1–10 cigarettes a day was signi-ficantly lower than the mean exhaled CO level of those consuming > 10 cigarettes a day in this study. In contrast, there was no significant differ-ence in mean exhaled CO levels between individ-uals consuming 11–20 cigarettes a day and those consuming > 20 cigarettes a day (Table 2). Those consuming more cigarettes tend to visit the smok-ing areas and smoke dursmok-ing worksmok-ing hours, which explains their higher exhaled CO levels measured in the workplace. However, because of the limita-tion of time, individuals who generally smoke > 20 cigarettes a day might not easily smoke more than those who smoke 11–20 cigarettes a day dur-ing workdur-ing hours.
Jarvis et al studied 211 hospital outpatients and reported that the optimal cut-off to differenti-ate a smoker from a nonsmoker was 8 ppm, with a sensitivity and specificity of 90% and 89%, respectively.3 Wald et al studied 11,249 men aged 35–64 years attending a medical center for health screening examination and also reported that a cut-off of 1.5% COHb in the blood (which corre-sponds to an exhaled CO level of approximate-ly 8 ppm) differentiated a smoker from a non-smoker with a sensitivity of 86% and specificity of 96.6%.5 In other studies using exhaled CO monitors, a CO level of 10 ppm was used as the cut-off.10,11 However, our results suggest that such a high cut-off level might reduce the sensitivity of CO monitoring, as a better diagnostic value
Figure. Correlation between exhaled carbon monoxide (CO) levels and the number
of cigarettes consumed daily in 123 current smokers. The dashed lines indicate the 95% confidence interval, and the dotted lines indicate the 95% prediction interval.
Table 2. Mean exhaled carbon monoxide (CO) level of subjects with different smoking status
Smoking status Mean number of cigarettes Mean exhaled CO level,
consumed per day (SD) ppm (95% CI)
Nonsmoker (n = 27) 4.2 (3.3–5.1)0 Smoker (n = 123) 1–10 cigarettes/day (n = 49) 07.4 (2.5) 9.1 (7.9–10.3) 11–20 cigarettes/day (n = 65) 18.0 (2.8) 18.1 (16.5–19.6) > 20 cigarettes/day (n = 9) 29.1 (5.0) 20.3 (12.4–28.3) 50 40 30 20 10 0 –10 Exhaled CO level (ppm) 0 10 20 30 40 50 Number of cigarettes consumed daily
CO = 4.43 + 0.70 × number of cigarettes consumed daily r = 0.73, p < 0.01
213
J Formos Med Assoc | 2006 • Vol 105 • No 3
Exhaled CO and smoking
was obtained at a CO cut-off of 6 ppm, in accord-ance with the work of Middleton and Morice, who also showed that a cut-off level of exhaled CO of 6 ppm detected 94% of smokers and 96% of nonsmokers in a respiratory outpatient clinic.2 Because smoking behavior in the workplace is dif-ferent from that in the community, we did mis-classify smokers as nonsmokers. Consequently, the sensitivity of the best cut-off point to differen-tiate smokers from nonsmokers in this study was only 84%.
In conclusion, this study supports a good correlation between exhaled CO level and daily cigarette consumption in the workplace in Taiwan. The exhaled CO monitor can be used to monitor smoking status, and can be combined with a smok-ing cessation program for health promotion. A reading of > 6 ppm is a good cut-off point that strongly indicates that an individual is a current smoker.
Acknowledgments
We would like to thank all of the participants for their invaluable support of this study. This study could not have been completed without their time and cooperation.
References
1. Bureau of Health Promotion, Department of Health. Taiwan
Tobacco Control Annual Report, 2005. [In Chinese]
2. Middleton ET, Morice AH. Breath carbon monoxide as an indication of smoking habit. Chest 2000;117:758–63. 3. Jarvis MJ, Tunstall-Pedoe H, Feyerabend C, et al. Comparison
of tests used to distinguish smokers from nonsmokers. Am
J Public Health 1987;77:1435–8.
4. Peterson JE. Postexposure relationship of carbon monoxide in blood and expired air. Arch Environ Health 1970;21: 172–3.
5. Wald NJ, Idle M, Boreham J, et al. Carbon monoxide in breath in relation to smoking and carboxyhaemoglobin levels. Thorax 1981;36:366–9.
6. Jarvis MJ, Belcher M, Vesey C, et al. Low cost carbon mon-oxide monitors in smoking assessment. Thorax 1986;41: 886–7.
7. Deveci SE, Deveci F, Acik Y, et al. The measurement of ex-haled carbon monoxide in healthy smokers and non-smokers.
Respir Med 2004;98:551–6.
8. Bureau of Health Promotion, Department of Health. Clinical
Practice Guidelines for Treating Smokers in Taiwan, 2002.
[In Chinese] Available from: http://health99.doh.gov.tw/ quit/re01-001.doc
9. Liou YM, Ko YL. The role of primary clinicians in preventing smoking. Formosa J Med 1998;2:91–6. [In Chinese] 10. Tonnesen P, Norregaard J, Mikkelsen K, et al. A
double-blind trial of a nicotine inhaler for smoking cessation. JAMA 1993;269:1268–71.
11. Jorenby DE, Smith SS, Fiore MC, et al. Varying nicotine patch dose and type of smoking cessation counseling.