Can Chlorhexidine Mouthwash Twice a Day Ameliorate Cyclosporine-induced Gingival Overgrowth? Translational possibilities
Running title: Chlorhexidine for CsA-induced Gingival Overgrowth
Ching-Hwa Gau1, BS, MS; Hsiao-Pei Tu2, BS, MS, PhD;Yu-Tang Chin3, BS, MS;Rebecca Y.A. Chen, BDS 4 Martin Ming-Jen Fu5, BDS, MS; Earl Fu6,*,BDS, DSc
1Lecturer, Department of Nursing, Kang-Ning Junior College of Medical Care and Management, Taipei, Taiwan, ROC
2Assistant Professor, Department of Dental Hygiene, China Medical University, Taichung, Taiwan, ROC
3Candidate of Doctor Philosophy, Graduate Institute of Life Sciences, National Defense Medical Center, Taipei, Taiwan, ROC
4Resident, Department of Orthodontics and Pediatric Dentistry, School of Dentistry, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, ROC
5Resident, Division of Periodontology, Department of Oral Medicine, Infection and Immunity, Harvard School of Dental Medicine, Boston, MA, USA
6Professor, Department of Periodontology, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan, ROC
School of Dentistry, National Defense Medical Center, PO Box 90048-507, Taipei, Taiwan Tel: 886-2-87927150; Fax: 886-2-87927145; Email: [email protected]
Acknowledgement
This study was supported by Kang-Ning Junior College of Medical Care and Management, Taipei, Taiwan and the Chen-Han Foundation for Education.
ABSTRACT
Background/Purpose: Gingival overgrowth can be induced by treatment with
cyclosporine-A (Cscyclosporine-A), an immunosuppressant often used following organ transplantation. cyclosporine-A pre-existing rat model designed to mimic CsA-induced gingival overgrowth in humans was used to test the effectiveness of frequent application of a chlorhexidine anti-plaque solution in reducing the overgrowth.
Methods: Four groups of rats were fed CsA and received chlorhexidine mouthwash twice a
day, every day, every other day, or not all. A fifth negative control group received only mineral oil. Overgrowth was determined by measuring changes in gingival probing depth and keratinized gingival width on molars. Gingival histological examination was performed.
Results: Rats treated with mouthwash twice daily exhibited decreased probing depths and
gingival widths without statistical significance. Histological examination revealed that CsA treatment caused gingival enlargement, whereas chlorhexidine treatment twice a day diminished the enlargement.
Conclusions: These findings suggest that chlorhexidine mouthwash used twice daily may
reduce the severity of CsA-induced gingival overgrowth. Further research is warranted to determine the optimal dose and treatment regimen.
INTRODUCTION
The use of immunosuppressive drugs such as cyclosporine-A (CsA) is a major factor in the dramatic increase in allograft survival and successful management of certain autoimmune diseases.1, 2 However, gingival overgrowth is a troublesome complication of chronic CsA usage as well as that of other drugs, namely calcium channel blockers (e.g., nifedipine)3, 4 and phenytoin.5, 6 Because of their immunosuppressed state, patients receiving CsA are prone to various infections, including oral candidiasis and mucositis.7-9 Gingival overgrowth can also become disfiguring and affect mastication and speech. The prevalence of gingival overgrowth averages around 30%, with reported rates ranging 10-85%, largely due to diverse risk factors including bacterial plaque formation, age, cyclosporine dosage, use of calcium channel blockers, and genetic predisposition.10
Cyclosporine is a hydrophobic neutral polypeptide comprising 11 amino acids; it is produced by the fungus Tolypocladium inflatum gams.11, 12 It acts to suppress immune-modulated T lymphocytes and is then biotransformed in the liver into metabolic products excreted in feces or eliminated by the kidneys. Studies have long shown the association between gingival alterations and CsA therapy.13, 14 The severity of gingival overgrowth stemming from chronic use of CsA is further influenced by bacterial plaque and local irritants.9, 15 Studies have also shown increased expression of specific cytokines, especially transforming growth factor-beta (TGF-β), in drug-induced gingival overgrowth. This
suggests that TGF-β, an inflammatory mediator that regulates cell proliferation and differentiation, plays a role in enlarging the extracellular matrix in hyperplastic gingival tissue.10 However, the precise underlying mechanism(s) are undetermined.
Chlorhexidine is a antimicrobial agent commonly used in oral rinse solutions to control plaque formation and prevent the occurrence of gingivitis.16 Administered in rinse form it has few reported serious side effects, although teeth and tongue discoloration may occur.16
Chlorhexidine binds to different surfaces in the mouth (teeth and mucosa) and to the dental pellicle and saliva. After a single rinse with chlorhexidine, the saliva has been shown to exhibit antibacterial activity for up to five hours, whereas persistence at the oral surfaces has been demonstrated to suppress salivary bacterial counts for over 12 hours.17, 18 One study showed that oral hygiene improved via topical chlorhexidine application plus adherence to a ventilator weaning protocol can reduce both the incidence of ventilator-associated pneumonia and the duration of mechanical ventilation in surgical ICU patients.19 An observational study at five acute care hospitals further showed that implementing an oral cleansing protocol improved the care of patients receiving mechanical ventilation.20
Gingival overgrowth makes effective oral hygiene more important, especially in critically ill transplant patients. Unfortunately, not enough is known about the effect of frequent use of oral antiseptic solutions on the severity of CsA-induced gingival overgrowth. Although the clinical focus is on reducing the inflammatory process in gingival tissues,21 no
evidence-based study has described the potential benefits of frequent mouthwash application (twice daily) for reducing gingival overgrowth associated with CsA treatment. The purpose of this study, therefore, was to evaluate the effectiveness of frequent application of
chlorhexidine mouthwash on the severity of CsA-induced gingival overgrowth using a previously established rat model. The findings of this study may ultimately help patients who have gingival-overgrowth associated with CsA treatment.
METHODS
A total of 50 male Sprague Dawley rats (six weeks old) were randomly assigned to five groups of 10 rats. For reference, a six-week-old rat would be considered an adolescent in terms of human development. Four groups were fed CsA (Sandimmun, Sandoz, Basel, Switzerland) and received chlorhexidine mouthwash twice a day (2/D), every day (1/D), or every other day (0.5/D); the fourth group received no mouthwash (0/D). The mouthwash solution contained 0.15% chlorhexidine (in humans the typical dose administered ranges 0.1-0.2%) (16, 22-24). We chose to administer CsA via the oral route, as this is the most common route of administration in humans. A fifth group of 10 rats served as a negative control group and received only mineral oil (the solvent for CsA administration) and no CsA or
mouthwash. Male rats were used as previous studies have found males to be more susceptible to CsA-induced gingival overgrowth.25, 26
and 30 mg/kg body weight per day in five other rats. The CsA doses were chosen in order to maximize immunosuppression, while minimizing toxicity.27 CsA is typically administered in humans in a dose of 5-20 mg/kg.28, 29 CsA was administered by gastric feeding for four weeks as in our previous studies, this duration of treatment was found to significantly induce
gingival overgrowth.30, 31 The chlorhexidine mouthwash was applied topically on the buccal surfaces of the teeth and mucosa around the left mandibular molars using small cotton pellets soaked in 0.15% chlorhexidine solution (Parmoson®, Panion & BF Biotech Inc., Tao-Yuan, Taiwan), as previously described.32 At the end of week 4, the rats were sacrificed using an approved humane method (exposure to 95% CO2 and 5% O2). Immediately afterwards the gingival probing depth at the distobuccal site of the left mandibular first molars and the width of keratinized gingiva at the mesiobuccal, midbuccal, and distobuccal sites of the molars were measured using a stereomicroscope (Olympus®-Szh, Olympus, Tokyo, Japan) (Figures 1 and 2). The measurement method used was a modification of that described by Morisaki et al..3 which involves measuring the width, height and area of the central papilla under a stereomicroscope; the area of central papilla is self-determined as its width times its height. The method has also been successfully used to measure gingival overgrowth in humans.33 The mandibular specimens around the mandibular molars, including the soft tissue and tooth, were fixed in 4% paraformaldehyde and prepared for histopathological examination. Samples were decalcified in 5% hydrochloric acid, and 4 mm-thick serial sections were cut in a
buccolingual direction throughout the entire distal root of the first molar. Hematoxylin and eosin staining was performed. The midsections of the root (exposing the root canal) were selected for histological examination as previously described.34
The institutional Animal Care and Use committee approved this study.
Statistical Analysis
Data are presented as mean ± standard deviation. The width of the keratinized gingiva were compared between groups by mixed model analysis, taking into consideration the repeated measures effect. Multiple comparisons for different CsA dosages and mouth washing frequencies were determined using Bonferroni’s method.. All statistical analyses were performed using SAS 9.0 statistical software (SAS Institute, Inc., Cary, NC). Differences were considered significant when p < 0.05.
RESULTS
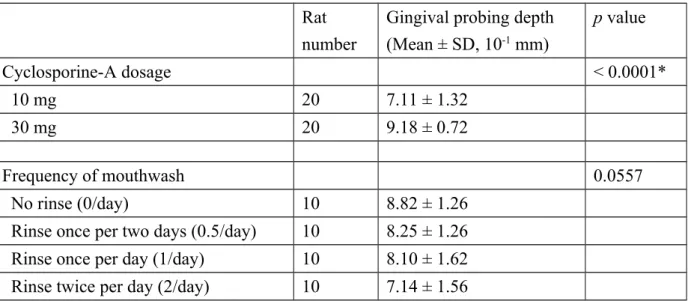
At the molar sites, significantly greater probing depths were found in rats treated with 30 mg/kg CsA than in rats treated with 10 mg/kg CsA (Table 1). Probing depth did not differ significantly according to the frequency of mouthwash application (p = 0.0557).
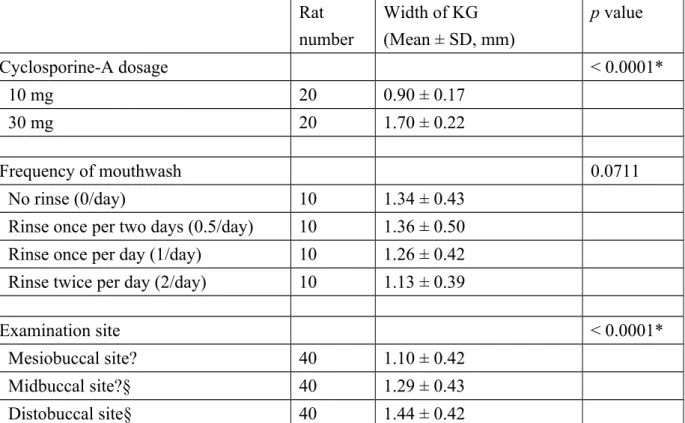
Although the mean width of the keratinized gingiva was significantly greater in rats treated with 30 mg/kg CsA than that in rats treated with 10 mg/kg CsA (p < 0.001),widths did
not differ significantly according to frequency of mouthwash application (p = 0.0711) (Table 2). Microscopy confirmed the presence of enlarged gingival tissue at the molar region of CsA-treated rats. Prominent overgrowth was clearly apparent in rats treated with the higher dose (30 mg/kg), while enlargement appeared less prominent in rats treated with mouthwash (especially twice daily, Figure 3).
DISCUSSION
CsA is one of the most significant and frequently used immunosuppressive drugs
administered following organ transplantation. Is also used to treat other diseases, including type 1 diabetes mellitus,35, 36 Behcet's disease,37, 38 psoriasis39, 40 and other skin disorders, and autoimmune diseases (e.g., rheumatoid arthritis, systemic lupus erythematosus). Its
usefulness is offset to a certain degree by its side effects, which may include nephrotoxicity, hepatotoxicity, hypertrichosis, and gingival enlargement.5, 6 Further to this, CsA has been shown to interact with several drugs commonly taken by immunosuppressed patients. For instance, nifedipine, taken to treat hypertension, when combined with CsA exacerbates gingival overgrowth.3, 4
Various methods have been used to assess changes in gingival contours in patients with gingival overgrowth. The simplest classification uses an ordinal scale to describe the severity as mild, moderate, or severe; however, there are no clearly described thresholds between the categories.41, 42 Another ordinal scale classifies the severity of overgrowth according to the
amount of tooth surface covered by the gingiva. These ordinal scales are similar, although the actual definition of each category differs between reports.15, 43, 44 A number of authors have measured periodontal probing depth to assess gingival overgrowth, although this method measures three-dimensional overgrowth only in the vertical plane.33, 45 Another investigation has shown that photographic scoring of gingival overgrowth is suitable for large-scale
population studies as it provides a continuous scale of gingival changes that can be compared statistically.46 In the present study, we measured gingival probing depth and keratinized gingival width around the molar region to assess overgrowth in rats.
We must acknowledge the influence of other risk factors in gingival changes, especially the presence of plaque. Dental bacterial plaque is considered a significant local risk factor for CsA-induced gingival overgrowth.9, 15 In animal studies, overgrowth was exacerbated when dental plaque was retained, but reduced by a single application of chlorhexidine.34 In this study we did not measure plaque because of the small size of rats and because previous studies show that caries score, sulcular temperature and pH of the gingiva were more often observed in rat models.47,48 Human studies, however, rely more on plaque scores. In humans, adequate plaque control improves the gingival condition but cannot completely prevent overgrowth.7 A review study based on literature identified using the online databases MEDLINE and PUB MED suggested that intervention was necessary to prevent or arrest drug-induced gingival overgrowth and that, whenever possible, a management strategy
should be adopted to avoid surgical treatment; however, the study also suggested that surgical treatment is often the most reliable option.49 In the present study, we found that mouthwash reduced, but did not completely prevent, gingival enlargement. Given that previous reports have suggested that plaque-associated gingival inflammation is a contributing factor to the development of CsA-induced overgrowth,50 it is possible that chlorhexidine may have reduced gingival overgrowth via an anti-inflammatory mechanism. It has been demonstrated that expression of proinflammatory cytokines such as interleukin-1b, tumor necrosis factor-a, and interleukin-6 are altered in CsA-induced gingival overgrowth.51,52 Further research is needed to assess potential changes in the levels of inflammatory mediators in this model of chlorhexidine treatment for CsA-induced gingival overgrowth. In addition, recent guidelines include the process of mouth care in the context of care bundles for preventing ventilator-associated pneumonia and catheter-ventilator-associated bloodstream infections in ICUs.53
Gingival overgrowth can be prevented by intensive plaque-control practices, including meticulous brushing, although critically ill patients receiving CsA may not be the ideal candidates for such intensive procedures. A simple chemical method to control plaque by rinsing or topical application may be a more suitable choice for nurses caring for critical patients. Most current oral care protocols involve a combination of chlorhexidine or normal saline mouth rinses and mechanical cleaning.54 Chlorhexidine mouthwash is considered the gold standard,24 with concentrations of 0.2- 0.12% shown to be effective in preventing plaque
accumulation.55 However, the antiplaque efficacy of 0.2% chlorhexidine mouthwash was found to be unaffected by subsequent tooth brushing with a dentifrice.56 In the present study, we found that CsA-induced gingival overgrowth in rats was not reduced following treatment with chlorhexidine. This lack of a significant finding can be attributed to the small sample size in each group and/or to insufficient duration of treatment (i.e., >four-weeks may be efficacious). We might also consider that the concentration of chlorhexidine administered was too low (higher doses may be more effective) and/or the CsA dose was too high. Overgrowth decreased with increased frequency of application. We recognize that a longer study period may be needed to demonstrate an observable significant effect; nevertheless, these study results suggest that chlorhexidine oral rinse twice a day may help limit severe gingival overgrowth.
In the present study, we tested whether or not potential maintenance activity from a single chlorhexidine rinse could provide lasting improvements in the overgrowth. We found that twice daily application of chlorhexidine reduced the overgrowth, although not
significantly so. Even meticulous plaque control cannot completely prevent gingival
overgrowth in patients receiving CsA.49,57 Nevertheless, findings from a recent study suggest that plaque-induced inflammation may modulate drug-gingival tissue interaction,58 supporting the hypothesis that strict plaque control could play a pivotal role in managing transplant patients who exhibit CsA-induced gingival overgrowth. The extent of drug-induced gingival
growth and its recurrence rate can be reduced by non-surgical techniques even though scalpel gingivectomy remains the treatment of choice.49 Our findings indicate that increased
frequency of chlorhexidine application may facilitate better condition management in humans. This possibility deserves further study.
Our study is similar to that reported by Pilatti and Sampaio.59 These investigators assessed CsA-induced gingival overgrowth in rats treated with 0.12% chlorhexidine once daily for 14 to 21 days and found that gingival overgrowth was significantly inhibited. In contrast, we found that twice-daily topical administration of 0.15% chlorhexidine over 28 days did not significantly reduce CsA-induced gingival overgrowth (although a definite trend was observed). The between study disparity may be related to differences in the method of CsA administration. In our study, CsA was administered by gastric feeding, while Pilatti and Sampaio gave CsA via the subcutaneous route.597 It is possible that the severity of gingival overgrowth may have been greater in our study and hence the treatment less effective. Our findings suggest that 28 days of chlorhexidine treatment (at least at the dose, route of administration and frequency of application described herein) may not be sufficient to significantly retardCsA-induced gingival overgrowth.
In conclusion, we found that CsA-induced gingival overgrowth in rats was not reduced significantly following treatment with chlorhexidine, although reduced overgrowth was observed with increased frequency of application. Twice-daily application of mouthwash
with chlorhexidine reduced gingival overgrowth in the gingiva around rat posterior molars. Compared to other treatments such as surgical intervention, chlorhexidine mouthwash remains a low cost, easily applied and modestly effective method of reducing gingival overgrowth. Further study is required to determine whether chlorhexidine mouthwash can provide reliable maintenance therapy when used as routine daily oral hygiene for patients receiving CsA or whether a specific concentration and frequency of chlorhexidine can better ameliorate gingival overgrowth.
Limitations
The results of this study are limited by our use of a short-term animal model to gather preliminary data; for results to be more credible and clinically applicable, a patient-based study is required. However, the limitation of a potential human study may be the nature of the patient population; most patients are organ transplant recipients and are seriously ill,
requiring concerted nursing attention that may not easily include focused oral care. In designing future studies, we will consider a longer study period, reduced CsA dosage, use of a higher concentration of chlorhexidine and increased frequency (more than twice daily) of application. Because statistical significance was not reached in the main study findings, it may be useful to repeat the present study with a larger sample in each group to further clarify the effects of different chlorhexidine concentrations and CsA dosages on gingival
overgrowth.
Conflict of interest
REFERENCES
1. Armstrong VW and Oellerich M. New developments in the immunosuppressive drug monitoring of cyclosporine, tacrolimus, and azathioprine. Clin Biochem 2001;34: 9.16. 2. Kramer NC, Peters TG, Rohr MS, et al. Beneficial effect of cyclosporine on renal transplantation. A multicenter long-term study. Transplantation 1990;49: 343.8.
3. Morisaki I, Fukui N, Fujimori Y, et al. Effects of combined oral treatments with cyclosporine A and nifedipine or diltiazem on drug-induced gingival overgrowth in rats. J
Periodontol 2000;71: 438.43.
4. O'Valle F, Mesa F, Aneiros J, et al. Gingival overgrowth induced by nifedipine and cyclosporin A. Clinical and morphometric study with image analysis. J Clin Periodontol 1995;22: 591.7.
5. Kato T, Okahashi N, Ohno T, et al. Effect of phenytoin on collagen accumulation by human gingival fibroblasts exposed to TNF-alpha in vitro. Oral Dis 2006;12: 156.62.
6. Soga Y, Nishimura F, Ohtsuka Y, et al. CYP2C polymorphisms, phenytoin metabolism and gingival overgrowth in epileptic subjects. Life Sci 2004;74: 827.34.
7. Bolwell B, Sobecks R, Pohlman B, et al. A prospective randomized trial comparing cyclosporine and short course methotrexate with cyclosporine and mycophenolate mofetil for GVHD prophylaxis in myeloablative allogeneic bone marrow transplantation. Bone Marrow
Transplant 2004;34: 621.5.
transplantation patients: an outcome-based analysis. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2003;96: 154.63.
9. Lucas VS and Roberts GJ. Oro-dental health in children with chronic renal failure and after renal transplantation: a clinical review. Pediatr Nephrol 2005;20: 1388.94.
10. Condé SA, Aarestrup FM, Vieira BJ, et al. Roxithromycin reduces cyclosporine-induced gingival hyperplasia in renal transplant patients. Transplant Proc 2008;40: 1435.8.
11. Petcher TJ, Weber H and Rüegger A. Crystal and molecular structure of an iodo-derivative of the cyclic undecapeptide cyclosporin A. Helv Chim Acta 1976;59: 1480.9. 12. von Wartburg A and Traber R. Chemistry of the natural cyclosporin metabolites. Prog
Allergy 1986;38: 28.45.
13. Calne RY, Rolles K, White DJ, et al. Cyclosporin A initially as the only immunosuppressant in 34 recipients of cadaveric organs: 32 kidneys, 2 pancreases, and 2 livers. Lancet 1979;2: 1033.6.
14. Starzl TE, Weil R 3rd, Iwatsuki S, et al. The use of cyclosporin A and prednisone in cadaver kidney transplantation. Surg Gynecol Obstet 1980;151: 17.26.
15. Pernu HE, Pernu LM, Huttunen KR, et al. Gingival overgrowth among renal transplant recipients related to immunosuppressive medication and possible local background factors. J
Periodontol 1992;63: 548.53.
16. Munro CL and Grap MJ. Oral health and care in the intensive care unit: state of the science. Am J Crit Care 2004;13: 25.33.
17. Jones CG. Chlorhexidine: is it still the gold standard? Periodontol 1997;2000 15: 55.62. 18. Roberts WR and Addy M. Comparison of the in vivo and in vitro antibacterial properties of antiseptic mouthrinses containing chlorhexidine, alexidine, cetyl pyridinium chloride and hexetidine. Relevance to mode of action. J Clin Periodontol 1981;8: 295.310.
19. Genuit T, Bochicchio G, Napolitano LM, et al. Prophylactic chlorhexidine oral rinse decreases ventilator-associated pneumonia in surgical ICU patients. Surg Infect (Larchmt) 2001;2: 5.18.
20. Cutler CJ and Davis N. Improving oral care in patients receiving mechanical ventilation.
Am J Crit Care 2005;14: 389.94.
21. Somacarrera ML, Lucas M, Scully C, et al. Effectiveness of periodontal treatments on cyclosporine-induced gingival overgrowth in transplant patients. Br Dent J 1997;183: 89.94. 22. Bopp M, Darby M, Loftin KC, et al. Effects of daily oral care with 0.12% chlorhexidine gluconate and a standard oral care protocol on the development of nosocomial pneumonia in intubated patients: a pilot study. J Dent Hyg 2006;80: 9.
23. Munro CL, Grap MJ, Jones DJ, et al. Chlorhexidine, toothbrushing, and preventing ventilator-associated pneumonia in critically ill adults. Am J Crit Care 2009;18: 428.37. 24. O'Reilly M. Oral care of the critically ill: a review of the literature and guidelines for practice. Aust Crit Care 2003;16: 101.10.
25. Nishikawa S, Nagata T, Morisaki I, et al. Pathogenesis of drug-induced gingival overgrowth. A review of studies in the rat model. J Periodontol 1996;67: 463.71.
26. Sooriyamoorthy M, Gower DB and Eley BM. Androgen metabolism in gingival hyperplasia induced by nifedipine and cyclosporin. J Periodontal Res 1990;25: 25.30.
27. Fu E, Nieh S, Chang HL, et al. Dose-dependent gingival overgrowth induced by cyclosporin in rats. J Periodontol 1995;66: 594.8.
28. King GN, Fullinfaw R, Higgins TJ, et al. Gingival hyperplasia in renal allograft recipients receiving cyclosporin-A and calcium antagonists. J Clin Periodontol 1993;20: 286.93.
29. Rateitschak-Plüss EM, Hefti A, Lörtscher R, et al. Initial observation that cyclosporin-A induces gingival enlargement in man. J Clin Periodontol 1983;10: 237.46.
30. Gau CH, Chou TC, Chiu HC, et al. Effect of cyclosporin A on the expression of inducible nitric oxide synthase in the gingiva of rats. J Periodontol 2005;76: 2260.6.
31. Gau CH, Hsieh YD, Shen EC, et al. Healing following tooth extraction in cyclosporine-fed rats. Int J Oral Maxillofac Surg 2005;34: 782.8.
32. Caufield PW, Navia JM, Rogers AM, et al.Effect of topically-applied solutions of iodine, sodium fluoride, or chlorhexidine on oral bacteria and caries in rats. J Dent Res 1981;60: 927.32.
33. Somacarrera ML, Hernández G, Acero J, et al. Localization of gingival overgrowth in heart transplant patients undergoing cyclosporin therapy. J Periodontol 1994;65: 666.70. 34. Fu E, Nieh S and Wikesjö UM. The effect of plaque retention on cyclosporine-induced gingival overgrowth in rats. J Periodontol 1997;68: 92.8.
35. Assan R, Blanchet F, Feutren G, et al. Normal renal function 8 to 13 years after cyclosporin A therapy in 285 diabetic patients. Diabetes Metab Res Rev 2002;18: 464.72. 36. Singh N and Palmer JP. Therapeutic targets for the prevention of type 1 diabetes mellitus. Curr Drug Targets Immune Endocr Metabol Disord 2005;5: 227.36.
37. Kaklamani VG and Kaklamanis PG. Treatment of Behcet's disease--an update. Semin
Arthritis Rheum 2001;30: 299.312.
38. Marshall SE. Behçet's disease. Best Pract Res Clin Rheumatol 2004;18: 291.311.
39. Ortiz A and Yamauchi PS. A treatment strategy for psoriasis: transitioning from systemic therapy to biologic agents. Skinmed 2006;5: 285.8.
40. Pereira TM, Vieira AP, Fernandes JC, et al. Cyclosporin A treatment in severe childhood psoriasis. J Eur Acad Dermatol Venereol 2006;20: 651.6.
41. Klar LA. Gingival hyperplasia during dilantin-therapy; a survey of 312 patients. J Public
Health Dent 1973;33: 180.5.
42. Spira M. Diphenylhydatoin sodium hyperplasia: hydrocortisone acetate as an adjunct in its treatment. J Oral Surg (Chic) 1955;13: 280.7.
43. Bäckman N, Holm AK, Hänström L, et al. Folate treatment of diphenylhydantoin-induced gingival hyperplasia. Scand J Dent Res 1989;97: 222.32.
44. Pan WL, Chan CP, Huang CC, et al. Cyclosporine-induced gingival overgrowth.
Transplant Proc 1992;24: 1393.4.
renal transplant children. Scand J Dent Res 1993;101: 282.6.
46. Ellis JS, Seymour RA, Robertson P, et al. Photographic scoring of gingival overgrowth.
J Clin Periodontol 2001;28: 81.5.
47. Yu D, Pearson SK, Bowen WH, et al. Caries inhibition efficacy of an antiplaque/antigingivitis dentifrice. Am J Dent 2000;13:14C.17C.
48. Firestone AR, Navia JM. In vivo measurements of culcal plque pH after topical applications of sorbitol and sucrose in rats fed sorbitol or sucrose. J Dent Res 1986;65:1020.23.
49. Mavrogiannis M, Ellis JS, Thomason JM, et al. The management of drug-induced gingival overgrowth. J Clin Periodontol 2006;33: 434.9.
50. Fu E, Hsieh YD, Shen EC, et al. Cyclosporin-induced gingival overgrowth at the newly formed edentulous ridge in rats: a morphological and histometric evaluation. J Periodontol 2001;72: 889.94.
51. Irwin CR, Myrillas TT, Traynor P, et al. The role of soluble interleukin (IL)-6 receptor in mediating the effects of IL-6 on matrix metalloproteinase-1 and tissue inhibitor of metalloproteinase-1 expression by gingival fibroblasts. J Periodontol 2002;73: 741.7.
52. Myrillas TT, Linden GJ, Marley JJ, et al. Cyclosporin A regulates interleukin-1beta and interleukin-6 expression in gingiva: implications for gingival overgrowth. J Periodontol 1999;70: 294.300.
hospital? Curr Opin Infect Dis 2009;22: 364.9.
54. Chandu A, Stulner C, Bridgeman AM, et al. Maintenance of mouth hygiene in patients with oral cancer in the immediate post-operative period. Aust Dent J 2002;47: 170.3.
55. Keijser JA, Verkade H, Timmerman MF, et al. Comparison of 2 commercially available chlorhexidine mouthrinses. J Periodontol 2003;74: 214.8.
56. Van Strydonck DA, Demoor P, Timmerman MF, et al. The anti-plaque efficacy of a chlorhexidine mouthrinse used in combination with toothbrushing with dentifrice. J Clin
Periodontol 2004;31: 691.5.
57. Seymour RA and Smith DG. The effect of a plaque control programme on the incidence and severity of cyclosporin-induced gingival changes. J Clin Periodontol 1991;18: 107.10. 58. Aimetti M, Romano F, Marsico A and Navone R. Non-surgical periodontal treatment of cyclosporin A-induced gingival overgrowth: immunohistochemical results. Oral Dis 2008;14: 244.50.
59. Pilatti GL and Sampaio JE. The influence of chlorhexidine on the severity of cyclosporin A-induced gingival overgrowth. J Periodontol 1997;68: 900.4.
Table 1 Effects of cyclosporine-A dosage and frequency of chlorhexidine mouthwash on gingival probing depth at the distobuccal site of the mandibular first molar in rats treated daily with either 10 or 30 mg/kg of cyclosporine-A for four weeks.
Rat number
Gingival probing depth (Mean ± SD, 10-1 mm) p value Cyclosporine-A dosage < 0.0001* 10 mg 20 7.11 ± 1.32 30 mg 20 9.18 ± 0.72 Frequency of mouthwash 0.0557 No rinse (0/day) 10 8.82 ± 1.26
Rinse once per two days (0.5/day) 10 8.25 ± 1.26 Rinse once per day (1/day) 10 8.10 ± 1.62 Rinse twice per day (2/day) 10 7.14 ± 1.56
*Indicates a significant overall difference as determined by repeated measures mixed model analysis.
The mean gingival probing depth was 5.13 ± 1.15 10-1 mm in 10 negative control rats receiving neither cyclosporine-A nor mouthwash.
Table 2 Effects of cyclosporine-A dosage, examination sites, and frequency of chlorhexidine mouthwash on the width of keratinized gingiva (KG) around the mandibular first molar in rats treated daily with either 10 or 30 mg/kg of cyclosporine-A for four weeks.
Rat number Width of KG (Mean ± SD, mm) p value Cyclosporine-A dosage < 0.0001* 10 mg 20 0.90 ± 0.17 30 mg 20 1.70 ± 0.22 Frequency of mouthwash 0.0711 No rinse (0/day) 10 1.34 ± 0.43
Rinse once per two days (0.5/day) 10 1.36 ± 0.50 Rinse once per day (1/day) 10 1.26 ± 0.42 Rinse twice per day (2/day) 10 1.13 ± 0.39
Examination site < 0.0001*
Mesiobuccal site? 40 1.10 ± 0.42
Midbuccal site?§ 40 1.29 ± 0.43
Distobuccal site§ 40 1.44 ± 0.42
* Indicates a significant overall difference as determined by repeated measures mixed model analysis.
? Indicates a significant difference in width of KG between the mesiobuccal and midbuccal sites by Bonferroni post-hoc test with p < 0.0001.
§ Indicates a significant difference in width of KG between the midbuccal and distobuccal sites by Bonferroni post-hoc test with p < 0.0001.
The width of KG was 0.73 ± 0.19 mm in 10 negative control rats receiving neither cyclosporine-A nor mouthwash.
FIGURE LEGENDS
Figure 1. The photograph presents the recording of probing depth measured by inserting a specially designed plastic probe with the white marking at the distobuccal site of the mandibular first molar under a stereomicroscope (original magnification 5).
Figure 2. The photograph indicates the measurement of the keratinized gingival width at the mesial, buccal, and distal sites of the mandibular first molar (original magnification 5) in a control rat. The three black lines indicate the width at the mesial, middle, and distal sites of the molar, respectively, using the tips of three buccal cusps as landmarks. The position arrows point to the coronal levels of gingival crests and the apical levels at the mucogingival line.
Figure 3. Representative histological sections illustrating the morphology of the buccal gingiva of the mandibular first molar in rats treated with CsA (10 or 30 mg/kg for upper and lower images, respectively) and mouthwash. The frequency of mouthwash application was (from left to right) none, every other day, daily, or twice daily for four weeks. A negative control histological section is also shown (E). Prominent overgrowth was evident in buccal gingivae from rats treated with the high dose (30 mg/kg) (a, b, c, and d) when compared to those with the low dose (10mg/kg) (A, B, C, and D). Enlargement appeared less pronounced in rats treated with mouthwash, particularly with twice daily treatment.