血液透析病人睡眠品質及影響因素探討; Quality of Sleep and the Affecting Factors in ESRD Patients with Hemodialysis in Taiwan
84
0
0
全文
(2) 誌謝 生活中總是有很多意外,進中國醫藥大學醫管所是意外,半年後 發現右眼白內障需手術治療是意外,手術後發現雙眼視差一千多度須 左眼戴隱形眼鏡再戴眼鏡才可以和右眼看更是意外,無法只戴眼鏡看 書是最大的意外,但是意志力加上努力讓我畢業就不是意外。我終於 可以畢業了! 能畢業要感謝很多人,首先是我太太--麗卿的體諒,半夜擾人清 夢的電腦吵雜聲音是我的錯,清晨上網查資料也是我的錯,對的是我 可以畢業了。謝謝尚翰及尚恩的幫忙,在我將會記工作帶回家時,挺 身 key 資料並對帳,在我電腦有問題時及時幫我修電腦!星期日的工作 吵得大家無法補眠,跟你們說聲抱歉! 特別要感謝的是指導教授蔡文正老師,自己臨床上雖努力了十幾 年,也參與了幾次的研究,但總是有不明所以的缺憾,在研究設計上 的不足,老師給了我最佳的啟示。在整體架構及時間管理應用上更是 無懈可擊,對於老師嚴謹的研究精神,更是令人佩服。感謝亞洲大學 的楊志良院長,他是我國健康保險的先驅,也是醫管的前輩,在上課 中言簡義賅,在口試中給我諸多良議。另外要感謝彰基劉青山主任, 在百忙中指導,在統計的建議與見解。采娟老師的不吝指導,榕浚學 長排解我對統計問題的疑惑,鼎力相助建檔及分析,謝謝! 同學的相扶相持,更是讓我走過憂黯的最佳助力,嘉欣是最佳見 證,娟娟、珮琳、佳怡、懿君、冠馨、美倫、禺彤、顒秀、宏茂大哥、 敏耀大哥、子凱、元德、啟淑、憲忠、盈森、冠華、睿圻、佳樺、劭 雯、玉資、寶玲、素茹、依霙、靖婷,醫管所 21 屆的同學,謝謝您們! 要感謝的人很多,潔宜的幫忙收案與連絡,大為的電腦維修加持, 佳特公司的馮姐、靜子及清泉醫院透析室的各位夥伴,參與此次研究 的透析中心夥伴,謝謝您們! 冠璋 i. 謹誌 2006/6/8.
(3) 摘要 目的:評估台灣血液透析病人,其睡眠品質不良的發生率,了 解腿部不寧及憂鬱對睡眠品質的影響,分析睡眠品質良好與不好的 病人,其基本特質、臨床因素等的差異。 方法:以台灣血液透析病人為母群體,以 63 個透析中心,經系 統性隨機選擇 348 個血液透析病人,以匹茲堡睡眠品質量表測量睡 眠品質為依變項,以國際腿部不寧量表測量腿部不寧徵候群症狀嚴 重度,貝克憂鬱量表測量憂鬱嚴重度。以病人特質、合併疾病、臨 床因素、憂鬱、腿部不寧徵候群症狀為變項。使用複迴歸探討影響 睡眠品質相關因素。 結果:透析病人抱怨睡眠品質不良的發生率為 66%。調整其它 變項後,以複迴歸分析,發現睡眠品質不良與年齡、家庭收入、使 用助眠藥物、腿部不寧的嚴重度、憂鬱有顯著關聯性(P<0.05) ,其 中憂鬱症狀愈嚴重的病人,睡眠品質愈差。 結論: 睡眠品質不良是血液透析病人常見的問題,腿部不寧、 憂鬱會降低血液透析病人睡眠品質,早期發現腿部不寧徵候群及憂 鬱,早期診斷及治療是未來血液透析醫療應努力的方向及課題。. 關鍵字:睡眠品質、血液透析、憂鬱、腿部不寧. ii.
(4) Abstract Objectives: The aim of this study was to determine the prevalence of poor quality of sleep (QOS) and the affecting factors in patients on maintenance hemodialysis in Taiwan. Methods: This study population was 44,121 HD patients in Taiwan. A total of 348 hemodialysis patients by systematic random selection in 63 hemodialysis units were enrolled in the cross-sectional study. We used Pittsburgh Sleep Quality Index (PSQI) to measure the quality of sleep (QOS) as dependent variable. The Beck Depression Inventory (BDI)-II Chinese version was used to rate the severity of depressive symptoms. We used International Restless Legs Syndrome Rating Scale (IRLS) to illustrate the severity of restless legs syndrome (RLS). The demographics, co-morbidity, hemodialysis (HD) mode, clinical parameters, the severity of depressive symptoms, and the severity of RLS are independent variables. We analyzed the categorical variables by the chi-square test or the Fisher exact test and continuous variables by student’s t-test. We use multiple linear regression analysis to estimate the relationship between the QOS and independent variables. Results: The prevalence of sleep complaints in Taiwanese HD patients was 66%. Subjects characterized by poor QOS were significantly more likely to be female, lower education status, without work, sleep medicine, RLS, and depression (all p<0.05). QOS was significantly associated with age, family income, sleep medicine, RLS, and depression by multiple linear regression after controlling for the other variables (all p<0.05). Conclusions: Age, less family income, usage of sleep medicine, RLS symptom, and depression are independently associated with poor QOS in HD patients. To find out depression and RLS of HD patients as early as possible is important.. Keywords: quality of sleep, hemodialysis, depression, restless legs syndrome. iii.
(5) Tables of Contents Chapter 1 Introduction .............................................................................1 Session 1 Background ......................................................................1 Session 2 Statements of Problems....................................................1 Session 3 Research Objectives.........................................................3 Chapter 2 Literature Review ....................................................................4 Session 1 Uremia and Dialysis.........................................................4 Session 2 Outcome of ESRD Therapy ...........................................10 Session 3 Quality of Sleep (QOS)..................................................14 Session 4 Summary of Literature Review......................................22 Chapter 3 Research Methods .................................................................23 Session 1 Research Structure .........................................................23 Session 2 Study Hypothesis ...........................................................23 Session 3 Sample and Data Sources ..............................................25 Session 4 Instruments.....................................................................26 Session 5 Measurement..................................................................27 Session 6 Analytical Methods ........................................................35 Chapter 4 Results ...................................................................................37 Session 1 Descriptive Analyses......................................................37 Session 2 Bivariate Analyses .........................................................41 Session 3 Multiple Linear Regression ...........................................43 Chapter 5 Discussion..............................................................................44 Chapter 6 Conclusion and Recommendations .......................................51 Chapter 7 Research Limitations .............................................................52 Reference................................................................................................70 iv.
(6) List of Tables Table 3-1. Operational Definitions of Variables ....................................27 Table 2-1. Manifestations of the Uremic Syndrome ..............................53 Table 2-2. Potentially Toxic Compounds That Accumulate in Renal Failure ...................................................................................55 Table 2-3. The Karnofsky score in ESRD Patients in Taiwan. ..............56 Table 4-1. Characteristics of the Subjects ..............................................57 Table 4-2. Characteristics of the HD subjects........................................59 Table 4-3. Comparison of Good Sleepers and Poor Sleepers ................62 Table 4-4. Multiple Linear Regression Models with PSQI score on HD patients. .................................................................................66. List of Figures Figure 2-1. Factors potentially contributing to sleep disturbances in dialysis patients. ...................................................................20 Figure 3-1 Research Structure................................................................24 Figure 5-1.The mean scores in the seven components of the PSQI in our HD patients, Canadian HD patients [15], Taiwanese elder [76], and US healthy subject as normal control [66]. ..........68 Figure 5-2. The mean score in the seven components of all HD subjects, ‘poor sleepers’, and ‘good sleepers’. ...................................69. v.
(7) Chapter 1 Introduction Session 1 Background End-stage renal disease (ESRD) is one of the most important health problems in Taiwan. The major leading causes of ESRD in Taiwan are diabetic mellitus (DM), chronic glomerulonephritis (CGN) and hypertension (HT) [1]. Diabetic nephropathy is getting more and more proportion in new cases of treated ESRD from 2001(37.7%), 2002(39.7%), to 2003(42.2%) in our country [2]. As same as United States, according to the United States Renal Data System (USRDS), the proportion of DM in new cases of treated ESRD was approximately 44% in 2002 [3]. The overall crude annual prevalence rate of maintaining dialysis for ESRD was 400 per million populations in our country in 2003 [2]. In 2003, nephritis, nephrotic syndrome and nephrosis ranked eighth in the leading cause of death in Taiwan area [4]. By the end of March in 2005, there were 46,512 patients with ESRD on dialysis in this country and over 93.4% under hemodialysis (HD) therapy [5]. In 2003, the total direct expenditures for dialysis patients from Bureau of National Health Insurance (BNHI) was over NT$ 21 billions, and it is the most usage of expenditures in single disease from BNHI [6].. Session 2 Statements of Problems According to the increase of prevalence and cost of treatment in ESRD, the physicians and researchers put emphasis on improving clinical outcomes, such as issue of hospitalization, morbidity and mortality. The National Kidney Foundation-Kidney Disease Outcome Quality Initiative (NKF-K/DOQI) sets. 1.
(8) guidelines to care the patients under dialysis, such as, guidelines for cardiovascular disease, anemia, HD adequacy, vascular access, and nutrition [7]. These guidelines achieved the substantial improvement in the qualities and outcomes of medical care for ESRD patients. The data of USRDS revealed that the first year death rates for dialysis patients was declined from about 35-38% to 25.7% from 1983 through 1993 [8]. Many data analysis from the USRDS and studies reported the lower hospitalization, morbidity and mortality after medical interventions [8, 9, 10, 11]. The dialysis dosage, usage of synthetic membranes and erythropoietin played important roles in decrease of mortality. After the clinical outcomes improved, the clinical and research settings have paid more attention to the quality of life in patients treated with dialysis. Quality of sleep (QOS) is one of the most important indicators of quality of life because its important impact on healthy condition [12, 13, 14]. To gain more complete knowledge of QOS and the affecting factors in HD patients is absolutely imperative if our efforts are going to ameliorate the health outcome. The incidence of subjective sleep disturbance has been demonstrated over 50% to 80% in ESRD patients surveyed by many studies [12, 13, 14, 15]. Sleep apnea syndrome (SAS), periodic limb movement disorder (PLMD), and restless legs syndrome (RLS) had also been documented higher prevalent rate than the general population [16, 17, 18]. There is little report about QOS in these groups in Taiwan. Hui et al. reported the prevalence rate of subjective sleep complaints is 52% in peritoneal dialysis (PD) patients in Taipei [13]. They found that 18 (52%) of a sample size of 34 patients who completed the survey described sleep complaints. Another study by Tsay et al. reported that the QOS in HD patients after acupoints massage was improved [19]. These patients were all limited in north Taiwan. To our knowledge, there is no large-scale survey about QOS in ESRD patients treated with 2.
(9) maintenance HD in Taiwan. However, fewer studies discuss QOS and the affecting factors in ESRD patients treated with maintenance HD in our country.. Session 3 Research Objectives 1. Describe demographics, co-morbidity, clinical parameters, depression level, restless legs syndrome in HD patients. Using the descriptive analysis, this study wants to determine the demographics, co-morbidity, and clinical data of enrolled HD patients. 2. Assess the level of depression symptom, restless legs syndrome, and QOS in HD patients. Using the Beck Depression Inventory II of Chinese version, the International Restless Legs Syndrome rating scale, and the Pittsburgh Sleep Quality Index, this study measures the level of depression symptom, restless legs syndrome, and QOS in samples from HD facilities participating in this study. 3. Determine the statistic differences between poor and good quality of sleep in patients under this study with demographics, co-morbidity, clinical parameters, depression levels, restless legs syndrome scale. Using multiple linear regression analysis, this study aims to determine the factors associated with the poor QOS in HD patients.. 3.
(10) Chapter 2 Literature Review Session 1 Uremia and Dialysis 1. Renal Function The major functions of the kidney can be briefly classified as follows: 1. To excrete the metabolic end products and solutes. The kidneys are the major organ to excrete the protein products, the urea, creatinine, etc. As we know, most drugs are excreted in unchanged form by kidney. 2. To adjust the body fluid and electrolytes and keep body component steadily. The secretion and reabsorption of water and electrolyte in different parts of the renal tubules play the central role in this mechanism. 3. To produce hormone and activate hormone. Erythropoietin is produced by renal interstitial cell to stimulate erythrocyte production in bone marrow. Renin is secreted by the juxtaglomerular cells and initiates a sequence reaction in regulation of blood pressure. Active form of vitamin D3 is formed by renal tubule cell and its role is to regulate the calcium and phosphate.. 2. Chronic Kidney Diseases (CKD) In America, there are twenty million adults have CKD, about 1 person in 9 adults [7]. Chronic renal failure is a term that includes a large number of progressive processes of renal destruction. It is characterized by gradual loss of renal function. The major deteriorations of function in chronic renal failure are related to the decrease of glomerular filtration rate and the loss of tubular functions. The result was the accumulation of the waste, such as blood urea nitrogen and creatinine. Furthermore, the impairment of endocrine activity, such as erythropoietin secretion,. 4.
(11) may provide the clinical presentations of chronic renal failure. The statistical data in 2002 from USRDS, diabetes was the first leading cause of new ESRD patients, followed by hypertension, glomerulonephritis and cystic kidney [8]. But in Taiwan, the first leading cause of new ESRD cases was still glomerulonephritis (44%), followed by diabetes (25.2%), hypertension (6.7%), and chronic interstitial nephritis (3.4%) in 2001 [20]. After 2002, the situation was changed. Glomerulonephritis replaced by diabetes, the proportion of diabetes in new ESRD cases was from 39.7% (2002) to 42.2% (2003). Diabetes plays more important role in the new ESRD cases in our country [2]. NKF-K/DOQI guidelines defined that CKD should be established based on follow conditions: 1. The presences of kidney damage greater than or equal to three months was based on structure or functional abnormalities or markers of kidney damage. 2. The level of kidney function or glomerular filtration rate (GFR) < 60 mL/min/1.73 m2 was persisted for greater than or equal to three months. The stages of CKD are expression of functional abnormality by the level of GFR, with lower stage representing higher GFR levels, as follows [7]: Stage 1. Individual has kidney damage with normal or increase GFR. GFR is greater than or equal to 90 mL/min/1.73 m2. Stage 2. Individual has kidney damage with mild decrease GFR. GFR is between 60 to 89 mL/min/1.73 m2. Stage 3. Individual has kidney damage with moderate decrease GFR. GFR is between 30 to 59 mL/min/1.73 m2. Stage 4. Individual has kidney damage with severe decrease GFR. GFR is between 15 to 29 mL/min/1.73 m2. Stage 5. Individual has kidney damage with marked decrease GFR. GFR is less than 15 mL/min/1.73 m2. 5.
(12) All the patients with kidney damage greater than or equal to three months must be detective and intervened as early as possible to prevent renal function progressively going down to ESRD. Generally speaking, renal replacement therapy is expected when individual with chronic kidney disease in stage 4 or 5 even if many medical efforts have been done. Clinically, chronic kidney disease often appears without any symptom and sign until renal damage is widely enough to 80-90% loss of nephrons.. 3. ESRD and Uremia ESRD is an administrative term definite almost whole failure of kidneys’ function to do their job in the body. It commonly occurs when the GFR is less than 10 mL/min/1.73 m2 with or without symptom and sign. In this condition, renal replacement therapy or kidney transplant is necessary due to the accumulation of waste and metabolic poisoning products in the body at the point of renal function. Uremia is a clinical term that means “urine in the blood”. It does not demonstrate the uremic syndrome entirely accurate but it presents progressive accumulation of toxic products from dietary and endogenous derivations. Chronic kidney failure is often in symptom-free condition until the serum creatinine increases over 6-10 mg/dl. Abnormalities of laboratory finding appear long before any symptoms presented. Significant symptoms and physical manifestations appear lately in the course. The native kidneys have greatly reserved function but also because the residual nephrons have a noteworthy capacity to compensate the loss of other nephrons. The first symptoms may be influenza-like presentation, general malaise, fatigue, headache, and inability to concentrate. Loss of appetite, altered taste sensation with body weight loss may occur early in gastrointestinal symptom. The skin pigmentation increased after sunlight exposure. Extracellular volume 6.
(13) expansion resulted in severe lower leg edema, pleural effusion, and ascites [21]. The major symptoms and signs of uremia are related to three aspects of function: diminished excretion of water and electrolytes; declined excretion of the metabolic end products and solutes (also called uremic toxins); reduced renal hormone synthesis. The stage 4 or 5 of chronic kidney diseases always progress, the uremic syndrome can be predicted but the first appearance is usually nonspecific. Important manifestations of the uremic syndrome are listed in Table 2-1 [21]. Restrictive diet with low protein content is the most important prescription to patient with uremic syndrome that rejects dialysis. It is known for improving the symptoms such as anorexia, nausea, vomiting, lethargy, and somnolence. Early studies provide evidence of that protein derivatives are major factors related to uremic syndrome [22]. In uremic patients, many substances accumulated in the body that could be potentially toxic compounds are listed in Table 2-2 [21]. The cumulative effect of uremic toxins leads into multiple organs dysfunction. As syndrome depicted in Table 2-1, the initiation of renal replacement therapy is need for the debilitating health of patient. In Taiwan, ESRD patients need to apply the uremic major illness card (UMIC) from Bureau of National Health Insurance (BNHI) for initiation and maintenance dialysis if the payment from BNHI [23]. The absolute criteria to apply the UMIC are 24 hours creatinine clearance rate (CCR) is less than 5 ml/minute or plasma creatinine is greater than 8 mg/dl. Individual with ESRD, however, the 24 hours CCR is less than 15 ml/minute or plasma creatinine is greater than 6 mg/dl with following symptoms- heart failure or pulmonary edema, pericarditis, bleeding tendency, neurological abnormalities, hyperkalemia, severe metabolic acidosis, intractable nausea and vomiting, cachexia, and severe azotemia (blood urea nitrogen greater than 100 mg/dl) can also apply the UMIC to maintain dialysis. 7.
(14) 4. Hemodialysis The term “Dialysis” was first described by Thomas Graham (1805-1869), he made a loop dialyzer membrane and found that process of the some crystalloids pass through the semipermeable membrane and colloids cannot pass through the membrane. He can be called the father of modern dialysis [24]. In 1945, Willem Kolff performed the first clinically successful hemodialysis in a patient with renal failure on comatose stage in Netherlands [24]. The hemodialysis is performed through diffusion and ultrafiltration which needs a semipermeable membrane with solute-discriminatory to separate the blood from dialysate. Small solutes, such as urea and electrolytes, pass easily through the membrane. It is more difficult for larger solutes to pass through the membrane than small solutes. The hemodialytic machine is used to generate negative hydraulic pressure on the dialysate side to drive ultrafiltration. Therefore, the major elements of hemodialysis are 1) artificial kidney or dialyzer; 2) machine to drive ultrafiltration and pump the dialysate and patient’s blood through the dialyzer; 3) the dialysate, that is the liquid with adjusted chemical composition used for solute clearance. The dialysate and patient’s blood are pumped along the dialyzer in contrary direction at flow rate of 500 and 200 to 400 mL/min. The flow rate is chose by physician’s decision under consideration of patient’s status and the major factors affecting the effectiveness of the hemodialysis. There are so many kinds of commercial artificial kidney- such as modified biologic materials or synthetic materials- used in renal replacement therapy. The major consideration in choice of dialyzer is made by its ability to clear the toxin particles and its potential for water removal. Its biocompatibility after contacting the blood and the static volume are also the consideration in decision-making. Another weight in the physician’s mind is the reprocessing probability and cost. In general, most dialyzers used in Taiwan are synthetic membranes because of more 8.
(15) biocompatibility. The solute concentration gradients started the diffusion process across the dialyzer by dialysate compositions. It is important to keep dialysate sodium concentrations similar to serum to prevent sodium imbalance and hemolysis. The dialysate potassium concentration is often kept in 0-4 meq/Liter since most of the ESRD patient impaired the ability to secrete potassium. The other components are glucose, bicarbonate, calcium, magnesium, and chloride. All of the elements are formulated commercially in powder or liquid form. The liquid dialysate with fixed formulation can be used immediately after opened. A reconstituted dialysate is supplied by powdered concentrate that is diluted with purified water processed by reverse osmosis device, ion exchange, water softener, carbon adsorption and filters. The blood and dialysate are pumped by dialysis machine to create negative pressure in dialysate side between dialyzer. The dialysis machine needs to mix liquid dialysate with purified water to appropriate composition, to keep adequate dialysate temperature, to maintain blood and dialysate flow for ultrafiltration, and to monitor air bubbles in blood and blood leakage in dialysate. It is important to keep alertly monitoring above parameters during dialysis session to prevent lethal event. The therapies of ESRD are dialysis and kidney transplantation. The patients should be fully informed of the services available to them, including PD, HD, and transplantation. In Taiwan, most of patients (93.4%) selected HD and received dialysis in facility of hospitals or clinics [5]. Long-term vascular access for HD is ordinarily established by arteriovenous (AV) fistula creation in the upper extremities after patient’s selection of HD. AV fistula needs 4-8 weeks to mature (wall thickened and lumen dilatation by blood flow). After AV fistula punctured with two needles and connected with blood tube to the dialyzer and dialysis machine, dialysis is starting. The blood exposes to the extracorporeal circuit and 9.
(16) needs anticoagulant to prevent the clotting mechanism.. Session 2 Outcome of ESRD Therapy The outcome of therapy is the major concerning decision in selection of a treatment by patient and his or her physician. There are many studies in ESRD patients which are around the outcome of therapy; such as to improve the survival rate, decrease the hospitalization rate, ameliorate the quality of life, return to work or social activity or schooling (9,10,16,18). There are many subjects to evaluate the outcome of ESRD therapy; such as mortality, morbidity, quality of life and rehabilitation.. 1. Mortality The number of deaths in a year as a percentage of the mean of the number of ESRD patients at the beginning and end of the year is the crude mortality rate. It is not a good method for matching patients in different treatment due to individual variant, financial condition, social supports, and not all patients have died under analytic time. Kaplan-Meier (K-M) estimation is the most commonly used method to depict survival curves in ESRD patients [16, 25]. Time sequence in beginning of follow–up is depicted on the horizontal axis, and the percentage or probability of patients alive at a definite time is depicted on the vertical axis. Mortality is one of the most important and most commonly used methods to describe outcome for ESRD patients. USRDS points out that the adjusted one-year mortality rate of patients in United State is reduced gradually from 35-40% in 1985 to 22-25% in 2002 [26]. In 2001, there are 1019 (3%) patients on maintenance HD over 15 years, 10.2% patients between 10-15 years, and 24.6% patients between 5-10 years in 10.
(17) Taiwan [20]. The most important factors affecting mortality rate are age, race, cause of ESRD, pre-existing cardiac disease, gender, anemia, dialysis adequacy, co-morbidity [8,26]. The risk factors of mortality are smoking, neoplasm, malnutrition, and low serum albumin [8,26]. The leading causes of death in dialysis patients in Taiwan are cardiopulmonary system diseases (24.3%), and followed by infectious diseases (14.9%), neoplasm (4.6%), central nervous system diseases (4.5%), and gastrointestinal diseases (4.5%) [20]. Another complex method of survival analysis uses a multiple regression model, the most known of which is the Cox proportional hazards regression model. It is used to estimate the effects on mortality rate of different factors simultaneously or patients in different group [27] .. 2. Hospitalization Hospitalization is one of the representatives of the healthy condition for ESRD patient. It is difficult to compare between countries because many factors such as culture, geographic differences, health insurance status, and political rules. It can be accumulated. in. hospitalization. rate. such. as. Point-prevalent. sample. or. Period-prevalent sample over a year period, numbers of admissions, and length of hospital stay per year. A large-scale study in five European countries participating in the Dialysis Outcomes and Practice Pattern Study (DOPPS) reported that hospitalization rate was 0.99 per patient year and the mean length of hospital stay was 11 days. The major causes of hospitalization were cardiovascular-related diseases, vascular access-related diseases, infectious diseases, gastrointestinal diseases, and liver-related diseases [28]. Hospitalization data is reported annually in the USRDS, including times of 11.
(18) admissions and hospital days per year. Statistic data of hospitalization can be used to compare in diabetics and non-diabetics patients, HD and CAPD patients, and cause of ESRD and with treatment modality. In all age groups, the hospitalization rates for diabetics are higher than those for non-diabetics. The most common discharge diagnoses are cardiovascular diseases, infectious diseases, and gastrointestinal diseases [26].. 3. Rehabilitation Rehabilitation is a surrogate of the fundamental base of social life and ability to return to work or school. It has always been of concern in ESRD patients for going back to normal life as early as possible. The need of active patient participation is important to return functional activity. Psychologic support by family and friend can partially motivate the sense of controlling themselves health and desire of social activity. The rehabilitation of ESRD patients in Taiwan is household (23%), full time job (10.5%), part time job (6.7%), school (0.5%), unemployed (3.4%), self-care but need help (13.6%), and bed-ridden (11.5%) [20].. 4. Quality of Life (QOL) The World Health Organization (WHO) put forward a definition of quality of life (QOL) in 1993. It is defined as “ An individual’s perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns” [29]. In other word, QOL describes how well people feel about their life in many aspects as following: physical, psychological, social, and economic. In ESRD patients on dialysis therapy, better survival rate were ascribed to aggressive medical care, new technology, and social supports [30,31]. Now, the goal 12.
(19) of health care is not only to prolong the life or to ameliorate disease but also in improving the QOL. Therefore, QOL is the important indicator of the evaluation of therapy and health care. QOL can be measured from many aspects with subjective indicators in field such as physical function, energy, psychological function, social activity, life satisfaction, sexual function, happiness, and individual values. Objective assessments of QOL contain functional ability, employment status, and health status. For example, the ways to quantify a person’s ability to perform the test in observed variables such as muscle strength, speed of contraction and balance are good examinations in functional ability. The indicator which often used to estimate the functional ability of the ESRD patients is Karnofsky index. In Taiwan, the HD quality analysis in ESRD patients revealed that the Karnofsky score in most of patients are shown in Table 2-3 [20]. Employment is evaluated by employed or not under the condition of patient’s perception of himself or herself assessment with having ability to work. Another objective measure is the established generic Sickness Impact Profile to assess health status of disability related with chronic illness [32]. It can be used to check a person’s ability to do daily work, such as shopping, housework, and to evaluate the change in memory and judgment behavior. There are many subjective measures includes medical outcome study such as the World Health Organization Quality of life. (WHOQOL) assessment instrument,. Short Form-36 (SF-36) health survey, and the Kidney Disease Quality of life (KDQOL) instrument [29,33,34]. A total randomly selected sample size with 17236 HD patients in a cross-national prospective, observational study used KDQOL in 7 countries (USA, Japan, France, Germany, Italy, Spain, and the United Kingdom) revealed that QOL were highly related to risk of death and hospitalization in HD 13.
(20) patients under adjustment of demographic and co-morbid factors [35]. This large-scale study revealed that QOL was affected by socioeconomic factors (income, education, occupational status, and living status), treatment modal, laboratory factors, and co-morbidity factors. The living status, sleep especially affects QOL in ESRD patient on maintaining HD.. Session 3 Quality of Sleep (QOS) To maintain healthy circadian rhythm of sleep and waking is an important element of life cycle. It is very common to complaint sleep problems from ESRD patients. In clinical setting, a lot of burdens were borne by sleep disturbance in ESRD patients. There is a battery of reports about sleep disturbances in HD patients. A very high prevalence of subjective sleep complaints has been reported by over 50-80% of patients surveyed [12, 13, 14, 15, 16, 17, 19]. ESRD directly affected QOS, and therefore impacted the QOL [15]. Performing a more complete comprehending the sleep problems occurred by HD patients is important if developing better health outcomes is the object.. 1. Sleep Disturbances in Dialysis Patients Sleep problems are always existence from general population to ESRD patients. Daly and Hassall reported one of the earliest studies about sleep problem in 34 HD patients in 1970 [36]. It was noted that patients slept less on nights following dialysis. Total sleep time is apparently deceased and poor recovery of physical energy. Strub et al in their analysis illustrated that 63% of a sample of 22 HD patients reported subjective sleep disturbance represented by diminished sleep efficiency, portioned sleep, and more time lying awake in bed [37]. This was one of the earliest studies reported the prevalence of sleep complaints in HD patients. They 14.
(21) found that there was no difference in age, personality, or medications between subjects with sleep symptoms and those without. The limits of this study were small sample size and without controlling variables that affect sleep quality. In 1992, Holly et al. assessed the prevalence of 48 HD patients, 22 peritoneal dialysis (PD) patients, and 41 control subjects [12]. Fifty-two percent of HD, 50% of PD and 12% of control subjects reported sleeping problems. Caffeine intake and worry were associated with sleep disturbance. The same authors reported that jerking legs (28%), trouble falling asleep (67%), early morning waking (72%), nighttime waking (80%), and restless legs (83%) were the major complaints by HD patients [38]. The prevalence of self-reported sleep complaints was equal in HD and PD patients in this study. Walker et al. [14] described the extent, severity, and types of subjective sleep disturbance with a sleep questionnaire in a 64 HD patients units. Fifty-four patients completed the survey and 83% of subjects had sleep-wake complaints. The most common complaints included daytime sleepiness (66.7%), daily naps (59.2%), restless leg syndrome (RLS) (57.4%), disturbed sleep (51.8%), and use of sleeping medication (46.3%). Twenty-eight patients reported disturbed sleep characterized by delayed sleep onset, frequent awakening, RLS causing disturbed sleep, or generalized restlessness during the night. Their data revealed that RLS had an association with levels of urea and creatinine. Another complaint was often claimed to clinical team by HD patients. Which was daily sleepiness. In 1994, a study reported trouble sleeping and daily sleepiness were highly ranked in the KDQOL bothersome symptoms in HD patients from 9 different outpatient dialysis center located in California [34]. Winkelman et al. [39] designed a study to investigate the incidence of RLS in HD patients and to identify associated factors in 1996. They studied 204 HD patients with questionnaire about symptoms of RLS, sleep habits, pruritus, and 15.
(22) adherence to dialysis therapy. The study used 129 patients with heart disease as control group. ESRD patients received laboratory tests and sensory nerve amplitudes recorded. Twenty percent of the HD patients and 6 % of the control subjects reported moderate to severe RLS. Sleep onset with delay and reduction of total sleep time in HD patients compared to control group. RLS were correlated with sleep measures and pruritus. Sleep complaints included nocturnal awakening, sleep onset latency, total sleep time diminished, use of sleep medications, and nocturnal leg movement. They found increased mortality in patients with RLS at a 2.5-year follow-up. Benz et al. conducted a study to investigate predictors of mortality with reviewed the medical record in twenty-nine ESRD patients who had previously undergone polysomnography (PSG) between 1990 and 1993 [16]. They examine the associated between periodic limb movements (PLMS) in sleep and mortality in ESRD. Post 48 months follow-up, the patients with a PLMS index less than 20 had high mortality than patients with a PLMS index of 20 or greater. After controlling for the other risk factors, such as, urea reduction rate, albumin level, and hematocrit, comparing patients having greater PLMS index with patients having less PLMS index in survival rate still reached statistical significance. This study reported the potentially new predictors of mortality in ESRD patients with sleep disorders. Sakami et al examined insomnia and the affecting effect on immune functions in 578 Japanese men without any toxic exposure [40]. The study found the prevalence of insomnia in 9.2% Japanese men. The insomniac men without any medical disorders had significantly lower interferon-gamma and ratio of interferon-gamma to interleukin –4 than non-insomniac men. A significantly lower interferon-gamma to interleukin-4 ratio was detected in men with insufficient sleep or difficulty initiating sleep. They conclude that the immune system could be negatively affected 16.
(23) by sleep quality in insomnia. In 2005, Erten et al. reported the similar finding that lower interleukin-6 and tumor necrosis factor-alpha was got in obstructive sleep apnea patients in maintenance HD with sleep complaints [41] Olson et al. reported a study with questionnaire in 441 subjects age 34 to 69 years old from a community to measure the association between sleep-disordered breathing (SDB) in 1995 [42]. The hypertension, coronary artery disease, and occlusive vascular disease diagnosed by physician. They found that the prevalence of hypertension, coronary artery disease, and occlusive vascular disease were significantly increased in the subjects with SDB. Hanly and Pierratos found the mean serum creatinine was lower and higher mean serum bicarbonate in patients with nocturnal HD 8 hours during six or seven nights a week than same patients on conventional HD for 4 hours on each of three days per week [43]. There was significantly reduction in sleep apnea-hypopnea index from polysomnography study compared nocturnal HD with conventional HD. In 2001, the Framingham Heart Study matched the age, sex, and body mass index from subjects with polysomnography survey. Ninety subjects with SDB defined as a respiratory disturbance index (RDI) score > 90 percentile were compared with 90 low-RDI subjects [44]. Right ventricular wall thickness was significantly increased in subjects with SDB. Zoccali et al. [45] found sleep apnea inducing nocturnal hypoxemia, after that they recorded cardiovascular events during follow-up. They excluded patients on regular HD with primary sleep apnea, pulmonary diseases, and illness causing sleep apnea. The study found that the risk of cardiovascular increased 33 % in 1 % decrease in average nocturnal oxygen saturation. In Italy, Sabbatini et al. organized a study that aimed to investigate sleep disturbances in 694 HD patients in 21 different HD units in Naples and its neighborhood with a specific questionnaire in 2002 [46]. In this study, the 17.
(24) prevalence of the HD patients with sleep disturbances was 86%. There was a significantly higher sleep disturbance in HD patients on dialysis greater than 12 months than patients on dialysis less than 12 months. The patients dialyzed in the morning were in higher risk of insomnia than patients dialyzed in the afternoon. There was a significant difference in parathyroid hormone, pre-dialysis plasma values of creatinine and urea in the insomnia group compared with control group. Mucsi et al. designed a cross-sectional study to assess the prevalence of sleep problems and examined their effect on quality of life in Hungary [47]. Their data revealed that 65% of the patients had at least one sleep disorder. The first sleep complaint was insomnia in 49% of patients. The prevalence of patients with sleep apnea syndrome was 32%. The prevalence of patients with RLS was 15 %. They concluded that sleep disorders was correlated to illness intrusiveness, a significant factor of health-related quality of life. Another cross-sectional study reported by Mucsi et al. in 2005 [17], the aim of the study was to investigate the relationship of RLS, insomnia and specific insomnia symptoms with health-related QOL in 333 HD patients. The prevalence of RLS was 14%. There were higher co-morbidity in patients with than without RLS. RLS was associated with impaired overall QOS and poorer QOL. Parker et al. designed a study with objective polysomnography measures to compare chronic kidney disease (CKD) patients with estimated GFR of 14.5 ml/min and HD patients with Kt/V > 1.2 (equivalent to GFR of 10-15 ml/min) [48]. They reported that the total sleep time and sleep efficiency were both reduced in chronic kidney disease patients without dialysis and HD patients in 2005. More wake after sleep onset, much periodic limb movement, longer sleep latency, lower efficiency in sleep, and less sleep time were also found in comparing HD group to CKD group. After matching the metabolic data in both groups, they suggested that the sleep problems of both groups might have different etiologies. The etiologies of 18.
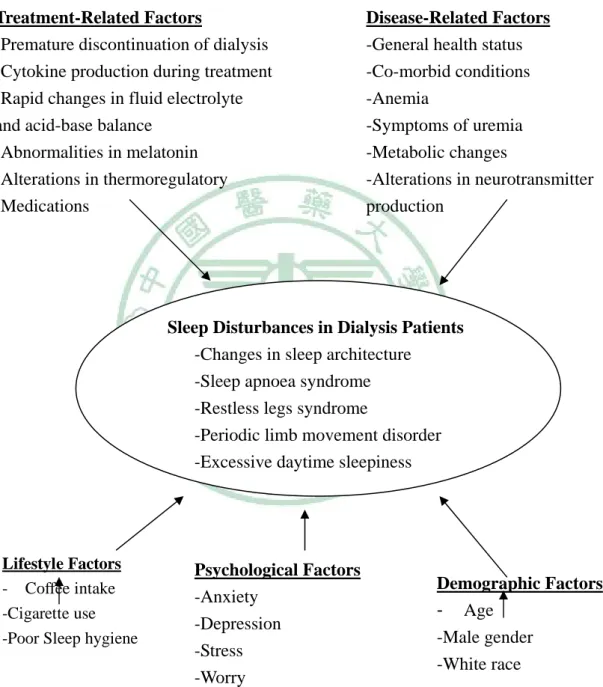
(25) sleep disturbances in CKD patients might be due to functional and psychological factors. The sleep disturbances in HD patients might be due to intrinsic sleep disruption (arousals, apnoeas and limb movements). Merlino et al. conducted a study to assess the prevalence of sleep disorders using a self-administered questionnaire in 883 ESRD patients in Italy [49]. The record included the demographic, lifestyle, clinical and laboratory data. The percentage of insomnia, RLS, sleep apnea syndrome, nightmares and excessive daytime sleepiness were 69.1%, 18.4%, 23.6%, 13.3% and 11.8%. The data revealed 80% of patients with at least one sleep disorder. The risk factors were older age, excessive alcohol intake, smoking, polyneuropathy and dialysis in the morning.. 2. The factors influence sleep disturbance in HD patients The etiologies of sleep disturbance in ESRD patients on maintaining HD are often multiple factors. Parker summarized the relevant factors to influence sleep disturbance in HD patients, such as disease-related factors, psychological factors, treatment-related factors, lifestyle factors, and demographic factors. (Figure 2-1) [50]. QOS in ESRD patients is an important issue confirmed by clinicians and researchers. QOS in ESRD patients includes the quantitative and qualitative aspects of sleep, it is rather subjective and variable between individuals. However, the QOS consists many of components. It is difficult to define and measure objectively due to complex aspects. Furthermore, QOS assessed outcome may be changing by subjective perceiving in quality. Finally, sleep quality measuring is influenced by study’s architectural design. There are a lot of evidences link diseases and sleep disorder [12, 51, 52, 53], such as cardiovascular disease, rheumatoid arthritis, fibromyalgia, asthma, chronic obstructive pulmonary disease, hyperparathyrodism, and gastroesophageal reflux. 19.
(26) The hypertension, coronary artery disease, claudication, and stroke are significantly correlated sleep disturbance in HD patients [42]. Uremic patients with hyperparathyrodism or pruritus complaint sleep problem [12, 39, 46].. Treatment-Related Factors -Premature discontinuation of dialysis -Cytokine production during treatment -Rapid changes in fluid electrolyte and acid-base balance -Abnormalities in melatonin -Alterations in thermoregulatory -Medications. Disease-Related Factors -General health status -Co-morbid conditions -Anemia -Symptoms of uremia -Metabolic changes -Alterations in neurotransmitter production. Sleep Disturbances in Dialysis Patients -Changes in sleep architecture -Sleep apnoea syndrome -Restless legs syndrome -Periodic limb movement disorder -Excessive daytime sleepiness. Lifestyle Factors - Coffee intake -Cigarette use -Poor Sleep hygiene. Psychological Factors -Anxiety -Depression -Stress -Worry. Demographic Factors - Age -Male gender -White race. Figure 2-1. Factors potentially contributing to sleep disturbances in dialysis patients. Source: Parker KP. Sleep disturbances in dialysis patients. Sleep Med Rev. 2003; 7(2):131-43. 20.
(27) The most frequent psychological problems affecting sleep disturbances include depression, anxiety, stress, and worry in general population. Worry was found to associate reported sleep disturbances in patients under dialysis[12]. In 2002, Williams et al reported a large-population study (The Kidney Outcomes Prediction and Evaluation Study, KOPE) to identify the correlation between sleep disturbances and psychosocial problems [54]. There was significantly associated in higher levels of depressive symptom with sleep disturbance. HD patients with greater levels of anxiety had poor sleep behavior than HD patients without. Especially, the patients have been in trouble falling asleep and feeling tired in the morning. The similar relationship between anxiety, worry, and sleep disorders was reported in Hong Kong Chinese patients [55]. A study from Japan reported that the anxiety and emotion-oriented coping stress were significantly associated with restless leg syndrome in ESRD patients [56]. In 2005, Wuerth et al. reported that the estimated prevalence of depression in ESRD patients was 20-30% [57]. They surveyed 380 PD patients for depression with BDI. There was 49% of patients who had a BDI score of 11 or greater than 11. Eighteen percent of the patients received pharmacologic therapy and BDI score improved from mean 17.4 to 8.4 point. Soldatos et al. reported that cigarette smoking contributed difficult falling asleep and increasing total time awake in 1980 [58]. The similar effect was reported in ESRD patients [12, 49]. Holley et al. and Walker et al. reported that caffeine drinking was associated with sleep problem [12, 14]. The other lifestyle factors influenced sleep disturbances was alcohol consumption [49]. The report from Hong Kong did not revealed the similar effect of alcohol and caffeine drinking in Chinese ESRD patients in continuous ambulatory peritoneal dialysis [55]. In human being, aging is a nature process and the length of sleep gradually decreased. There were reports that aging was the risk factors to sleep problems in 21.
(28) ESRD patients [14, 49, 59], but one report indicated no relation between age and sleep disturbances [12]. Male adult was associated with more sleep disturbances in ESRD patients [14, 60], even in pediatric dialysis patients [61]. More sleep complaints in white race had also been reported [59]. The clinical parameters influencing sleep disturbances in ESRD patients include blood urea nitrogen (BUN), creatinine [16, 46, 62], anemia [63], hypertriglyceridemia [13], hypercalcemia [64], and high serum phosphate [60]. The other independent risk factor for sleep disorders was dialysis shift in the morning [49, 65].. Session 4 Summary of Literature Review The literature review revealed that the QOS was highly related to the health of patients. The physician and researchers must to do not only improving survival rate and clinical outcome but also enhancing the quality of life and quality of sleep in ESRD patients. A better estimate of the prevalence of sleep disturbances in the generalized Taiwanese HD population is lacking because most of the reports about QOS studying in Taiwanese HD patients were localized in north Taiwan. To investigate the factors affecting the QOS in Taiwanese HD are important to in clinical and researchers.. 22.
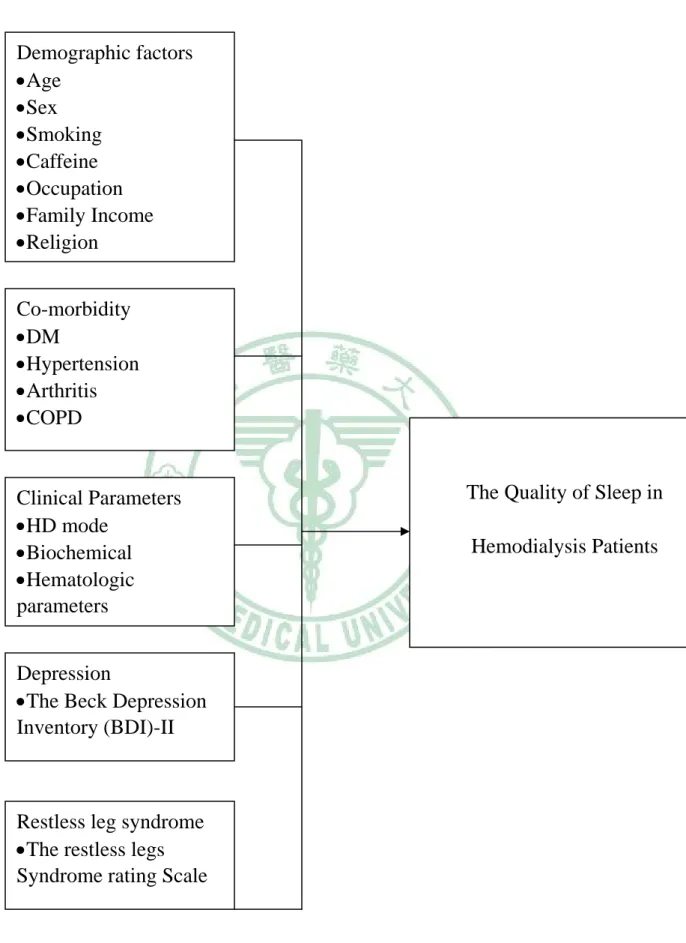
(29) Chapter 3 Research Methods Session 1 Research Structure The structure of this study was summarized in Figure 3-1. This study aims to explore that the relevant factors such as, demographic factors, co-morbidity factors, clinical factors, depression, and the RLS would influence the QOS in ESRD patients treated with HD in Taiwan.. Session 2 Study Hypothesis To our knowledge, the major factors might be potentially influencing to quality of sleep in ESRD patients, such as, aging, gender, smoking, coffee intake, anemia, co-morbidity, depression, anxiety, stress, HD mode, and RLS. Our study hypothesis was building on the bases of literatures review above. To examine the distributions in patient’s characteristic, co-morbidity, HD mode, clinical parameters, depression, RLS, and QOS in ESRD patients in Taiwan, we analyze the data that will be collected. Our hypotheses are as following: 1) Patients with severe depression symptom will have poorer QOS. 2) Patients with less RLS symptom will have better QOS. 3) There are some differences in patients’ characteristic, co-morbidity, and HD mode between ESRD patients with poor and good QOS.. 23.
(30) Demographic factors •Age •Sex •Smoking •Caffeine •Occupation •Family Income •Religion Co-morbidity •DM •Hypertension •Arthritis •COPD. The Quality of Sleep in. Clinical Parameters •HD mode •Biochemical •Hematologic parameters. Hemodialysis Patients. Depression •The Beck Depression Inventory (BDI)-II. Restless leg syndrome •The restless legs Syndrome rating Scale. Figure 3-1 Research Structure. 24.
(31) Session 3 Sample and Data Sources The HD patients in Taiwan were the study population. The data used for the analysis were from sixty-three outpatients dialysis units located in Taiwan. The geographic representative samples of dialysis facilities were recruited after telephone communication. There were 17 facilities in Taipei Branch of Bureau of National Health Insurance (BNHI), 9 facilities in Northern Region Branch of BNHI, 20 facilities in Central Region Branch of BNHI, 8 facilities in Southern Region Branch of BNHI, and 9 facilities in Kao-Ping Branch of BNHI. Within each participating HD units, the patients were ranked from 1 to N before selected and one subject was randomly selected in number from one to ten by researcher without giving care, the next patient would be increase by ten, for example, ranked 5, 15, 25, and so forth. Patients with bed-ridden and poor communicated were excluded. The questionnaires were explained to each participant and informed consent was obtained (proved by the Ethical Committee of the Ching-Chyuan hospital, under monitoring by the Institutional Review Board). The patient’s right to stop participating any time was reserved. If patient, such as, ranked five refused to join this study, patient ranked four then six replaced, and so on. This cross-sectional study included data from 63 facilities (total facilities in Taiwan =449) with total random selected sample size of 374 patients (total patients number in Taiwan = 44,121). The average number in each participated facility was 6 patients. All patients had received HD for more than 3 months before enrolled in this study. The data regarding QOS, demographic factors, co-morbidity factors, HD mode, clinical parameters, depression, and the RLS were collected from Dec 2005 to Feb 2006. The Beck Depression Inventory-II (BDI-II, Chinese version), The International Restless Leg Syndrome rating scale (IRLS), and the Pittsburgh Sleep 25.
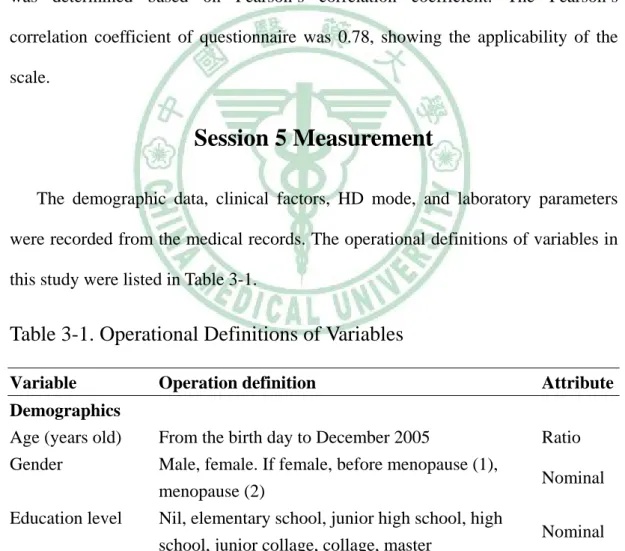
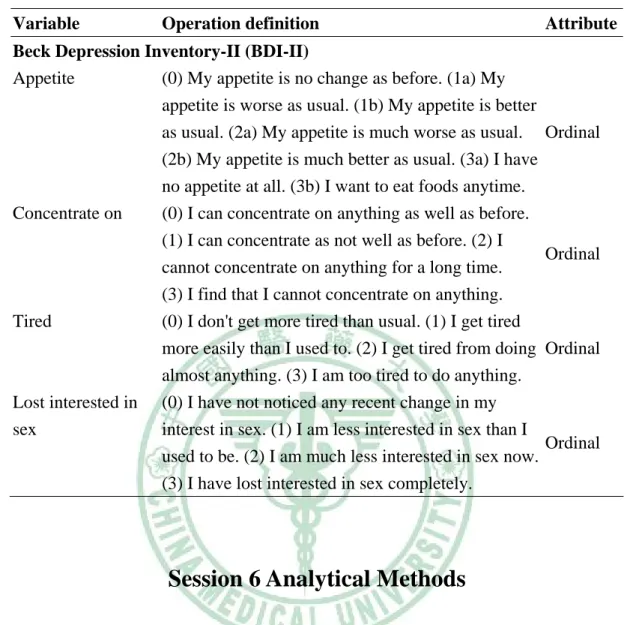
(32) Quality Index (PSQI) were collected using questionnaires translated to Chinese language and completed separately face-to-face by the HD unit nurse with training.. Session 4 Instruments The PSQI is a standard self-administered questionnaire used to evaluate QOS [66]. This questionnaire has been widely used in measuring the QOS of dialysis and transplantation therapy in ESRD patients [15, 19, 67, 68] and chronic renal disease [69]. The questionnaire was previously translated into Chinese to assess the quality of sleep in Taiwan [13, 70] and Hong Kong [71]. The PSQI contains seven components with nineteen questions. The components are subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, use of sleep medications, and daytime dysfunction. Every component is scored from 0 to 3 and the total score yielded between 0 and 21, the lower scores displaying higher quality of sleep. The PSQI has been usefully separated ‘good sleeper’ and ‘poor sleeper’ in literature [13, 15, 66, 70, 71]. The cutting point of total scores greater than 5 indicates that a person is a ‘poor sleeper’. The Beck Depression Inventory (BDI) is a self-rated questionnaire, has been used to assess patients for depression over forty-five years [72] and to investigate the depression symptom in ESRD patients [73]. The BDI-II was translated to Chinese by Chinese Behavioral Science Corporation and assesses the presence and severity of depression. It is a reliable and validated instrument of depression, existing high correlation with diagnostic criteria [74]. It has 21 items and scored from 0 to 3 then yielding global score of 0 to 63. A patient with BDI scores of 14 to19 indicates mild degree of depression, 20 to 28, a moderate degree, and 29 or greater, a severe degree of depression. 26.
(33) The International Restless Legs Syndrome rating scale (IRLS), ten-question scale measuring the severity of RLS, a patient-scaled tool has high levels of internal consistency and reliability [17, 75]. All the questions are rated in the range 0 to 4 (0=absence of a problem, 4=very severe problem), the global scores range between 0 and 40 (0=absence of a problem, 1 to 10=mild problem, 11 to 20=moderate problem, 21 to 30=severe problem, and 31 to 40=very severe problem). Test-retest reliability of the diagnosis was done in two weeks after data collected in 26 randomized patients from three facilities. The relationship between test and retest was determined based on Pearson’s correlation coefficient. The Pearson’s correlation coefficient of questionnaire was 0.78, showing the applicability of the scale.. Session 5 Measurement The demographic data, clinical factors, HD mode, and laboratory parameters were recorded from the medical records. The operational definitions of variables in this study were listed in Table 3-1.. Table 3-1. Operational Definitions of Variables Variable Demographics Age (years old) Gender Education level Marital status Occupation Family income (thousand). Operation definition. Attribute. From the birth day to December 2005 Male, female. If female, before menopause (1), menopause (2) Nil, elementary school, junior high school, high school, junior collage, collage, master Single, married, separated, widow/widower, divorced None, part-time, day-time, night-time (1)≦30, 30<(2)≦60, 60<(3)≦90, 90<(4)≦120, 120<(5)≦150, 150<(6). Ratio. 27. Nominal Nominal Nominal Nominal Ordinal.
(34) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. Attribute. Yes, No (1)≦0.5, 0.5<(2)≦1, 1<(3)≦2, (4)>2. Nominal Ordinal. Yes, No (1)≦1, 1<(2)≦2, 2<(3)≦3, (4)>3. Nominal. Demographics Smoking Yes (pack) Caffeine Yes (cup) Religion. None, Taoism, Buddhism, Christian, Catholic, Muslim. Ordinal Nominal. Hemodialysis and co-morbidity Causes of ESRD. Diabetes mellitus (DM), Hypertension (HT), Nominal Chronic glomerulonephritis (CGN), Systemic lupus erythematous (SLE), polycystic kidney disease (PKD). Co-morbidity. DM, HT, angina pectoris, heart failure (HF), myocardial infarction, cerebral vascular accident Nominal (CVA), chronic obstructive pulmonary disease (COPD), liver cirrhosis, chronic hepatitis, peripheral vascular disease, neoplasm, head injury, psychiatry disease. Time on dialysis (years). From the day of first time HD to December 2005. Ratio. Hemodialysis (HD) HD in the Morning, afternoon, or at night shift mode. Nominal. HD times/per week HD times per week, 1,2,3, >3. Ordinal. HD duration hours/per session. Ordinal. HD≦3, 3< HD≦3.5, 3.5< HD≦4, 4< HD. Clinical parameters and laboratory data Serum albumin (g/dl). Pre-HD serum albumin value on December 2005. Blood urea nitrogen Pre-HD serum BUN value on December 2005 (BUN) mg/dl Creatinine (Cr). Ratio Ratio. Pre-HD serum creatinine value on December 2005 Ratio. Urea reduction rate The percentage of (Pre-HD serum BUN minus (%) Post-HD BUN)/ Pre-HD serum BUN. 28. Ratio.
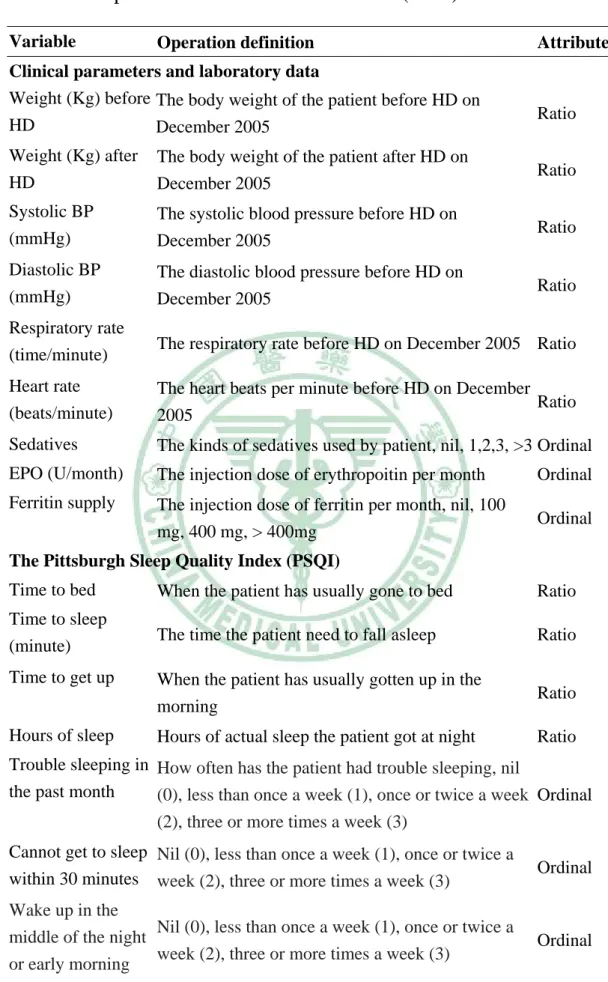
(35) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. Attribute. Clinical parameters and laboratory data Kt/V (Daugirdas) The Daugirdas method Kt/V = -ln(R-0.008*t) + (4-3.5* R) * UF/W, R=post-HD BUN/Pre-HD BUN, t = HD duration (hours), UF= ultrafiltration Ratio volume (Liter), W= Post-HD body weight (Kg), on December 2005 Uric acid (mg/dl). Pre-HD serum uric acid value on December 2005. Total cholesterol (mg/dl) T-CHO. Pre-HD serum cholesterol value on December 2005 Ratio. Ratio. Triglyceride (TG) Pre-HD serum triglyceride value on December (mg/dl) 2005. Ratio. Na meq/L. Pre-HD serum sodium value on December 2005. Ratio. Ca * P. Pre-HD serum calcium value multiplier serum phosphate on December 2005. Ratio. Ferritin (ng/ml). Pre-HD serum Ferritin value on December 2005. Ratio. K (meq/L). Pre-HD serum potassium value on December 2005 Ratio. iPTH (pg/ml). Pre-HD serum intact parathyroid hormone value on Ratio December 2005. Iron (ug/dl). Pre-HD serum iron value on December 2005. Ratio. Ca (mg/dl). Pre-HD serum calcium value on December 2005. Ratio. GOT (IU/L). Pre-HD serum GOT value on December 2005. Ratio. Total iron binding capacity (TIBC) Pre-HD serum TIBC value on December 2005 Ratio (ug/dl) P (mg/dl) Pre-HD serum phosphate value on December 2005 Ratio GPT (IU/L). Pre-HD serum GPT value on December 2005. Ratio. Red Blood Cell (*106). Pre-HD red blood cell on December 2005. Ratio. Hemoglobin (g/dl) Pre-HD hemoglobin value on December 2005. Ratio. Hct (%). Ratio. Pre-HD Hct value on December 2005. 29.
(36) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. Clinical parameters and laboratory data Weight (Kg) before The body weight of the patient before HD on HD December 2005. Attribute. Ratio. Weight (Kg) after HD. The body weight of the patient after HD on December 2005. Ratio. Systolic BP (mmHg). The systolic blood pressure before HD on December 2005. Ratio. Diastolic BP (mmHg). The diastolic blood pressure before HD on December 2005. Ratio. Respiratory rate (time/minute). The respiratory rate before HD on December 2005 Ratio. Heart rate (beats/minute). The heart beats per minute before HD on December Ratio 2005. Sedatives. The kinds of sedatives used by patient, nil, 1,2,3, >3 Ordinal. EPO (U/month). The injection dose of erythropoitin per month. Ordinal. Ferritin supply. The injection dose of ferritin per month, nil, 100 mg, 400 mg, > 400mg. Ordinal. The Pittsburgh Sleep Quality Index (PSQI) Time to bed. When the patient has usually gone to bed. Ratio. Time to sleep (minute). The time the patient need to fall asleep. Ratio. Time to get up. When the patient has usually gotten up in the morning. Ratio. Hours of sleep. Hours of actual sleep the patient got at night. Ratio. Trouble sleeping in How often has the patient had trouble sleeping, nil the past month (0), less than once a week (1), once or twice a week Ordinal (2), three or more times a week (3) Cannot get to sleep Nil (0), less than once a week (1), once or twice a within 30 minutes week (2), three or more times a week (3). Ordinal. Wake up in the Nil (0), less than once a week (1), once or twice a middle of the night week (2), three or more times a week (3) or early morning. Ordinal. 30.
(37) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. Attribute. Have to get up to use the bathroom. Nil (0), less than once a week (1), once or twice a week (2), three or more times a week (3). Ordinal. The Pittsburgh Sleep Quality Index (PSQI) Cannot breathe comfortably. Nil (0), less than once a week (1), once or twice a week (2), three or more times a week (3). Ordinal. Cough or snore loudly. Nil (0), less than once a week (1), once or twice a week (2), three or more times a week (3). Ordinal. Feel too cold. Nil (0), less than once a week (1), once or twice a week (2), three or more times a week (3) Feel too hot Nil (0), less than once a week (1), once or twice a week (2), three or more times a week (3) Have bad dreams Nil (0), less than once a week (1), once or twice a week (2), three or more times a week (3) Have pain Nil (0), less than once a week (1), once or twice a week (2), three or more times a week (3) Taken medicine for Nil (0), less than once a week (1), once or twice a sleep week (2), three or more times a week (3) Trouble staying awake while Nil (0), less than once a week (1), once or twice a engaging in social week (2), three or more times a week (3) activity Problems for patient to keep up Nil (0), less than once a week (1), once or twice a enthusiasm to get week (2), three or more times a week (3) things done Patient rate his or Very good (0), fairly good (1), fairly bad (2), very her sleep quality bad (3) overall. Ordinal Ordinal Ordinal Ordinal Ordinal. Ordinal. Ordinal. Ordinal. International Restless Legs Syndrome rating scale (IRLS) RLS discomfort in (4) Very severe, (3) Severe, (2) Moderate, (1) Mild patient’s legs or Ordinal (0) None arms RLS symptoms (4) Very severe, (3) Severe, (2) Moderate, (1) Mild Ordinal need to move (0) None 31.
(38) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. International Restless Legs Syndrome rating scale (IRLS) Relief from moving (4) Very severe, (3) Severe, (2) Moderate, (1) Mild around (0) None Sleep disturbance (4) Very severe, (3) Severe, (2) Moderate, (1) Mild by RLS symptoms (0) None Tiredness, (4) Very severe, (3) Severe, (2) Moderate, (1) Mild sleepiness by RLS (0) None symptoms Overall your RLS (4) Very severe, (3) Severe, (2) Moderate, (1) Mild severity as a whole (0) None RLS symptoms (4) Very severe (This means 6 to 7 days a week.), frequency (3) Severe (This means 4 to 5 days a week.), (2) Moderate (This means 2 to 3 days a week.), (1) Mild (This means 1 day a week or less.), (0) None RLS symptoms on (4) Very severe (This means 8 hours per 24 hour an severe average day or more.), (3) Severe (This means 3 to 8 hours day per 24 hour day.), (2) Moderate (This means 1 to 3 hours per 24 hour day.), (1) Mild (This means less than 1 hour per 24 hour day.), (0) None The impact of RLS (4) Very severe, (3) Severe, (2) Moderate, (1) Mild symptoms on ability to carry out (0) None daily life RLS symptoms on (4) Very severe, (3) Severe, (2) Moderate, (1) Mild, mood (0) None. Attribute. Ordinal. Ordinal. Ordinal. Ordinal. Ordinal. Ordinal. Ordinal. Ordinal. Beck Depression Inventory-II (BDI-II) Sad (0) I do not feel sad.(1) I feel sad. (2) I am sad all the time and I can't snap out of it. (3) I am so sad or Ordinal unhappy that I can't stand it. Discouraged (0) I am not particularly discouraged about the future. (1) I feel discouraged about the future. (2) I feel I have nothing to look forward to. (3) I feel that Ordinal the future is hopeless and that things cannot improve. 32.
(39) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. Attribute. Beck Depression Inventory-II (BDI-II) Failure experience. (0) I do not feel like a failure. (1) I feel I have failed more than the average person. (2)As I look back on Ordinal my life, all I can see is a lot of failure. (3) I feel I am a complete failure as a person.. Dissatisfied. (0) I get as much satisfaction out of things as I used to. (1) I don't enjoy things the way I used to. (2) I don't get any real satisfaction out of anything. Ordinal. anymore. (3) I am dissatisfied with everything the way I used to. Guilty. (0) I don't feel particularly guilty. (1) I feel guilty a good part of the time. (2) I feel quite guilty most of the time. (3) I feel guilty all of the time.. Ordinal. Punished. (0) I don't feel I am being punished. (1) I feel I may be punished. (2) I expect to be punished. (3) I feel I Ordinal m being punished.. Hate. (0) I don't feel disappointed in myself. (1) I am disappointed in myself. (2) I am disgusted with myself. (3) I hate myself. Ordinal. Blame. (0) I don't feel I am any worse than anybody else. (1) I am critical of myself for my weaknesses or mistakes. (2) I blame myself all the time for my Ordinal faults. (3) I blame myself for everything bad that happens.. Suicide. (0) I don't have any thoughts of killing myself. (1) I have thoughts of killing myself, but I would not Ordinal carry them out. (2) I would like to kill myself. (3) I would kill myself if I had the chance.. Cry. (0) I don't cry any more than usual. (1) I cry more now than I used to. (2) I cry all the time now. (3) I used to be able to cry, but now I can't cry even though I want to.. 33. Ordinal.
(40) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. Attribute. Beck Depression Inventory-II (BDI-II) Irritated (0) I am no more irritated by things than I ever am. (1) I am slightly more irritated now than usual. (2) I Ordinal am quite annoyed or irritated a good deal of the time. (3) I feel irritated all the time now. Lost interest (0) I have not lost interest in other people. (1) I am less interested in other people than I used to be. (2) I Ordinal have lost most of my interest in other people. (3) I have lost all of my interest in other people. Make decision (0) I make decisions about as well as I ever could. (1) I put off making decisions more than I used to. (2) I have greater difficulty in making decisions Ordinal than before. (3) I can't make decisions at all anymore. Valueless (0) I don't feel that I am valueless. (1) I am worried that I am more valueless than before. (2) I feel that Ordinal am more valueless than another people. (3) I believe that I am completely valueless. Lost energy (0) I can work about as well as before. (1) It takes an extra effort to get started at doing something. (2) Ordinal I have to push myself very hard to do anything. (3) I can't do any work at all. Sleep habit change (0) I can sleep as well as usual. (1a) I can sleep a little more as I used to. (1b) I can sleep a little less as I used to. (2a) I can sleep more as I used to. (2b) I Ordinal can sleep less as I used to. (3a) I almost sleep all day long. (3b) I wake up s1-2 hours earlier than I used to and cannot get back to sleep. Angry (0) I don't get more angry than usual. (1) I get a little bit angry more easily than I used to. (2) I get Ordinal angry more easily than I used to. (3) I get more angry anytime.. 34.
(41) Table 3-1. Operational definitions of variables (cont’) Variable. Operation definition. Beck Depression Inventory-II (BDI-II) Appetite (0) My appetite is no change as before. (1a) My appetite is worse as usual. (1b) My appetite is better as usual. (2a) My appetite is much worse as usual. (2b) My appetite is much better as usual. (3a) I have no appetite at all. (3b) I want to eat foods anytime. Concentrate on (0) I can concentrate on anything as well as before. (1) I can concentrate as not well as before. (2) I cannot concentrate on anything for a long time. (3) I find that I cannot concentrate on anything. Tired (0) I don't get more tired than usual. (1) I get tired more easily than I used to. (2) I get tired from doing almost anything. (3) I am too tired to do anything. Lost interested in (0) I have not noticed any recent change in my sex interest in sex. (1) I am less interested in sex than I used to be. (2) I am much less interested in sex now. (3) I have lost interested in sex completely.. Attribute. Ordinal. Ordinal. Ordinal. Ordinal. Session 6 Analytical Methods The descriptive statistics was used for demographic variables, co-morbidity, HD mode, laboratory data values and blood parameters in this study. The percentage, mean and standard deviation (SD) were used to describe the operational definition of variables. The categorical variables compared between the ‘good sleeper’ and ‘poorer sleeper’ were analyzed by the chi-square test or the Fisher exact test, as appropriate. Continuous variables were analyzed with student’s t-test. We used multiple linear regression analysis to investigate the significant factors affecting the global PSQI scores. Independent variables entered into the models including all variables that were significantly different in bivariate analysis, or clinical relevant. 35.
(42) reviewed from literature. We used stepwise methods to build the multiple regression models. A two-tailed P value < 0.05 was considered statistical significance. A standard statistical package SAS software (version 8.01) was used to perform all calculations in this study.. 36.
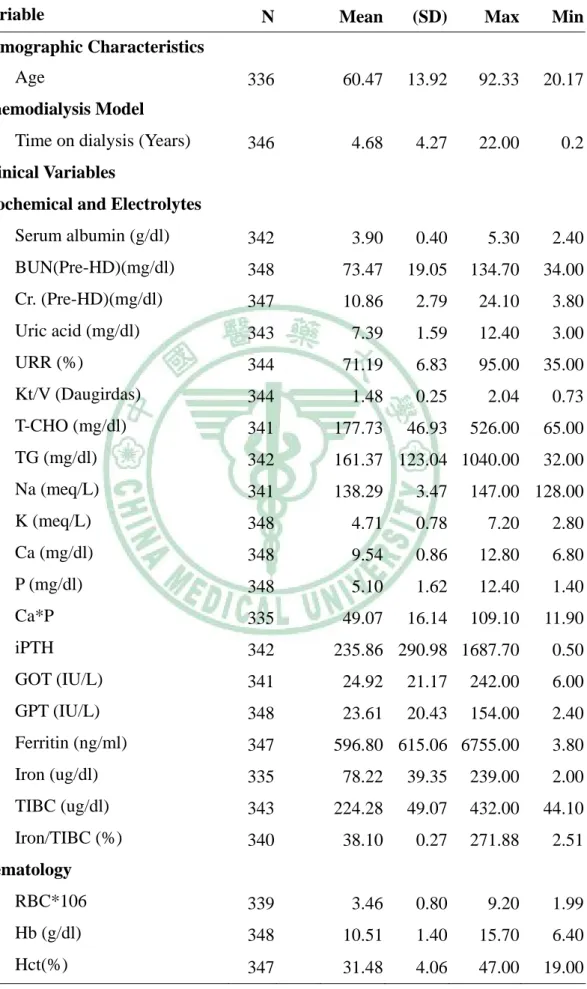
(43) Chapter 4 Results Session 1 Descriptive Analyses z Demographic The demographic characteristics of subjects are shown in Table 4-1 and Table 4-2. There were 348 patients in the final study sample. The response rate was 93.05%. Mean age of population was 60.47 ± 13.92 years (range, 20.17 to 92.33). The proportion of female was 52.3%. Sixty-six patients had never gone to school. The education levels, 124 patients (35.63%) graduated from elementary school, 57 patients (16.38%) graduated from junior high school, 64 patients (18.39%) graduated from high school, and 37 patients (10.64%) graduated from collage or above. The marital status, they were 264 married (76.3%), 36 widow or widower (10.4%), and 14 separated or divorced (4.1%). The proportion of occupational status of subjects without work was 78.9 %, with part-time work was 8.5%, with full daytime work was 11.7%, and with full nighttime work was 0.9%. The family income (NT$ thousand) were less than or equal to 30 (37.46%), between 30 to 60 or equal to 60 (40.25%), between 60 to 90 or equal to 90 (12.07%), between 90 to 120 or equal to 120 (6.5%), and greater to 120 (3.72%). In personal habits, 14.8% of cases were smokers, and 14% of patients had caffeine consumption lifestyle. Similar to Taiwanese religion distribution, most of patients were Buddhist and Taoist (76.3%), none of religion (19.6%), Christian and Catholic (3.5%), and others (0.6%).. z Etiology of ESRD and Co-morbidity The most prevalent end stage renal disease was chronic glomerulonephritis. 37.
(44) (41.95%). The other causes of ESRD were DM (33.6%), hypertension (9.77%), PKD (2.01%), and SLE (1.44%). Other or unknown etiology of ESRD accounted for 11.2% of patients. The co-morbidity was distributed as HT (35.9%), DM (17.9%), chronic hepatitis (10.8%), and HF (4.6%). The proportion of sum of co-morbidity number as following: none was 33.5 %, one was 46 %, two was 16.38 %, and ≧ 3 was 4.6 %... z Clinical Parameters The ESRD patients have been treated on maintenance dialysis for a mean of 4.68 ± 4.27 years (range, 0.2 to 22 years). Forty-four percent of the patients dialyzed in the morning, 42.4% of the patients dialyzed in the afternoon, and 13.8 % of the patients dialyzed at night. Most of HD patients (96.3%) dialyzed 3 times per week. Only 3.7% dialyzed two or four times per week. Most of the each HD session was between 3.5 to 4 hours (73.5%). There were 19% of patients received each HD session greater than 4 hours. The average Pre-HD/Post-HD weight of subjects was 61.1/58.36 Kg. The average ultrafiltration rate per HD session was 2.78 Kg. The average blood pressure (SBP/DBP) before HD was 138.63/77.61 mmHg. The heart rate was between 59 and 102 beats per minute. The respiratory rate ranged from 12 to 22 times per minute.. z Biochemical and Hematologic Parameters The serum albumin level varied from 2.4 g/dl to 5.3 g/dl with mean of 3.9 (±0.4) g/dl. Pre-HD BUN ranged from 34 mg/dl to 134.7 mg/dl with mean of 73.47 (±19.05) mg/dl. Mean and SD of urea reduction rate was 71.19 ± 6.83% and the range from 35% to 95%. The Kt/V (Daugirdas) ranged from 0.73 to 2.04 with average of 1.48. The mean of pre-HD creatinine level was 10.86 ± 2.79 mg/dl (range from 3.8 to 24.1) mg/dl. The serum uric acid had a range of 3-12.4 mg/dl with average of 7.39 mg/dl. Total cholesterol varied from 65 mg/dl to 526 mg/dl 38.
(45) with average of 177.73 ± 46.93 mg/dl. Triglyceride was between 32 mg/dl and 1040 mg/dl with mean of 161.37 ± 123.04 mg/dl. The serum sodium measured from 128 meq/L to 147 meq/L with mean of 138.29 ± 3.47 meq/L. The serum potassium varied from 2.8 meq/L to 7.2 meq/L and mean of 4.71 ± 0.78 meq/L. The mean of total serum calcium was 9.54 ± 0.86 mg/dl and range from 12.8 mg/dl to 6.8 mg/dl. The serum phosphate checked from 1.4 to 12.4 mg/dl and the mean was 5.1 ± 1.62 mg/dl. The calcium phosphate product was between 11.9 and 109.1 with mean of 49.07 ± 16.14. The intact parathyroid hormone varied from 0.5 pg/ml to 1687.7 pg/dl and average of 235.86 ± 290.98 pg/dl. The GOT value was 6 IU/L to 242 IU/L with mean of 24.92 ± 21.17 IU/L. The GPT leveled from 2.4 IU/L to 154 IU/L with mean of 23.61±20.43 IU/L. The serum ferritin ranged from 3.8 ng/ml to 6755ng/ml with mean of 596.8 ± 615.06 ng/ml. The serum iron varied from 2 ug/dl to 239 ug/dl with mean of 78.22 ± 39.35 ug/dl. The TIBC was between 44.1 ug/dl and 432 ug/dl and average of 224.28 ± 49.07 ug/dl. The red blood cells observed 1.99 million per milliliter to 9.2 million per microliter with mean of 3.46±0.8 million per microliter. The hemoglobin measured was 6.4 g/dl to 15.7 g/dl with mean of 10.51 ± 1.4 g/dl. The white blood cells ranged from 2.6 to 20.8 thousand per milliliter and average of 6.54 ± 2.21 thousand per milliliter. The hematocrit checked between 19% and 47% with mean of 31.48 ± 4.06%. There were 48.7 % of patients that had used sleep medications. The percentage of patients used two or more sleep medications were 4.5%. Only three patients had never received the erythropoitin (EPO). The dosage of EPO used for patients and the percentage of patients were less than 10000 (25.95%), 10000 to 18000 (32.65), 18000 to 26000 (26.53%), and greater than 26000 (14%) units per month. There were 17.7% of patients that had received 100 mg ferrous injection per month. Six 39.
(46) percent of patients had received 400 mg ferrous injection per month. Only 3.18% of patients had received more than 400 mg iron supply per month.. z Quality of Sleep The PSQI global score of study patients had a range of 0-21 points with mean of 8.49 ± 4.64 points. For the individual components, each observed ranges were 0-3 points. The subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, use of sleep medications, and daytime dysfunction had mean of 1.34 ± 0.88, 1.79 ± 0.98, 1.03 ± 1.08, 1.03 ± 1.21, 1.36 ± 0.63, 1.14 ± 1.34, and 0.79 ± 0.80.. z RLS and Depression The restless legs syndrome rating scale revealed a range of 0 to 40 points with mean and SD of 14.25 ± 11.48 in HD patients. There were 26.93 % of the ESRD patients on mild severity of RLS symptom. Nine percent of the ESRD patients had moderate symptom of RLS. On severe and very severe symptom, there were 8.05% and 7.43% of the ESRD patients. The total Beck depression inventory (BDI-II) score of 0-13 were 57.47% of the ESRD patients. The mean and SD of the BDI-II scores were 7.05 ± 8.62. There were 14.94 % of subjects with score of 14-19 points in the BDI-II that were considered mild depression. Sixteen percent of cases had BDI-II score of 20-28 points that were regarded as moderate depression, 12.07% of patients greater than 28 points as severe depression.. 40.
數據
+7



相關文件
The IEC endeavours to ensure that the information contained in this presentation is accurate as of the date of its presentation, but the information is provided on an
6 《中論·觀因緣品》,《佛藏要籍選刊》第 9 冊,上海古籍出版社 1994 年版,第 1
The first row shows the eyespot with white inner ring, black middle ring, and yellow outer ring in Bicyclus anynana.. The second row provides the eyespot with black inner ring
identify different types of tourist attractions and examine the factors affecting the development of tourism in these places;.4. recognize factors affecting tourist flows and the
The aim of this theme is to study the factors affecting industrial location using iron and steel industry and information technology industry as examples. Iron and steel industry
To evaluate the clinicopathologic features, prognostic factors, and management of patients in the North Chinese population with head and neck squamous cell carcinoma (HNSCC)
The aim of this study was to investigate, through a prospective clinical study, the prevalence and characteristics of oral lichen planus (OLP) and lichenoid lesions (OLL) in
In this respect, the aim of the present study was to as- sess volumetric as well as morphological surface changes of the orbital cavity in patients treated with both tooth- borne
