Chronic Rhinosinusitis and the Risk of Nasopharyngeal Cancer in a
Taiwanese Health Study
Yung-An Tsou MD, MS1,2, Jern-Chen Lin MS3, Chin-Jaan Tai MD1, Tung-Chou Tsai
PhD2, Chuan-Mu Chen PhD2,4, Ming-Hsui Tsai MD1
1Department of Otolaryngology Head and Neck Surgery, School of Medicine, China
Medical University Hospital, Taichung 404, Taiwan
2The Department of Life Sciences, Agricultural Biotechnology Center, National
Chung Hsing University, Taichung 402, Taiwan
3The China Medical University Biostatistics Center, Taichung 404, Taiwan 4Rong Hsing Research Center for Translational Medicine, National Chung Hsing
University, Taichung 402, Taiwan
Please send correspondence to Yung-An Tsou, MD, MS ([email protected]), address: Yuh-Der Road, No. 2, Taichung, Taiwan Level of Evidence: 4.
The authors have no funding, financial relationships, or conflicts of interest to disclose. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
ABSTRACT
Background: Although epidemiologic and laboratory studies report that chronic
inflammatory conditions contribute to the pathogenesis of cancer, it remains controversial whether chronic rhinosinusitis results in nasopharyngeal carcinoma (NPC).
Methods: Retrospective Cohort in NHI Taiwan database. This study prospectively
examined whether chronic rhinosinusitis or nasal polyposis is associated with nasopharyngeal cancer risk in the Taiwan National Health Insurance (NHI), a population-based cohort of 231,490 Taiwan Chinese individuals with a mean age of 32 years, recruited between 2000 and 2006.
We collected information from Longitudinal Health Insurance Database (LHID).
Each subject completed an interview including questions about medical conditions, and the NPC occurrence and survival status were determined by linkage to population-based NHI registries in Taiwan. And each NPC and chronic rhinosinusitis subject had completed a clearly interview on medical condition to confirm their diagnosis.
Results: After adjustment for age, sex, hypertension, diabetes mellitus (DM), allergic
rhinitis (AR), otitis media (OM) and coronary artery disease (CAD), individuals with rhinosinusitis were found to have a 3.55-fold increased risk of developing NPC 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
compared to individuals without rhinosinusitis (HR=3.55, 95% CI=2.22-5.69). The same results were also observed when the study subjects were analyzed without comorbidities.
Conclusions: Adult patients with rhinosinusitis should be followed up with regard to
the nasopharynx for at least 3 years, particularly repeat sinusitis patients.
Keywords: rhinosinusitis, nasopharyngeal carcinoma, risk factor, allergic rhinitis,
nasal polyposis, comorbidity, Taiwan database 1 2 3 4 5 6 7 8 9
INTRODUCTION
Sinusitis is a common disease and a common problem in ENT OPD (out-patient-department), and the overall burden from sinusitis and the various types of antibiotics and medical spending related to this disease are increasing, with approximately 10 billion dollars spent in the US every year. Sinusitis is caused by a viral, bacterial and fungus infection; prolonged viral or bacterial sinusitis often leads to a chronic sinusitis condition that should be treated with antibiotics3. However, the failure of antibiotic
treatment often necessitates surgical treatment, such as functional endoscopic sinus surgery, to cure the disease3. Sinusitis often extends to the nasopharyngeal area and
causes otitis media and nasopharyngitis4. Some agents of viral sinusitis, such as
Epstein–Barr virus (EBV), are even considered a cause of nasopharyngeal cancer development.
Nasopharyngeal cancer (NPC) arises in the nasopharynx, with an anatomic position near the posterior nasal chamber; chronic sinusitis causes a posterior mucopus drip that irritates the nasopharynx, causing chronic inflammation of the nasopharynx. However, it remains unclear whether adult sinusitis is a predictor of subsequent NPC and whether sinusitis patients should receive subsequent regular nasopharyngoscopy examinations as a high-risk group.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
NPC is rare in Caucasians, Japanese, and Koreans but is common in the inhabitants of southern China, Hong Kong, and Taiwan. In 2008, the Taiwan Department of Health reported an NPC incidence of 9.99 cases per 100,000 men and 3.47 cases per 100,000 women. NPC ranks ninth among cancer-related deaths for men and 14th for women in Taiwan. The Taiwan National Health Insurance (NHI) program was initiated in 1996, and 97% of hospitals and clinics are under contract with the system, covering almost 99% of the population in Taiwan. Thus, by examining NHI patient records, we were able to investigate the hypothesis that adult sinusitis is associated with an increased risk for the subsequent development of NPC using a nationwide, population-based cohort study.
1 2 3 4 5 6 7 8 9 10 11
MATERIAL AND METHODS
Data source
Since 1996, the Taiwan government has organized a nation-wide single-payer health insurance program, The Taiwan National Health Insurance program, which involved more than 99% of the 23 million Taiwan citizens in 1998. The National Health Insurance Research Database (NHIRD) consists of the historical reimbursement claim data from the health insurance, and The National Health Research Institute (NHRI) manages and maintains the database.
The present research was constructed by the Longitudinal Health Insurance Database (LHID), a subset of the NHIRD that randomly selected one million people of those insured during 1996-2000. According to an NHRI report, there was no difference in the distribution of age and sex ratio between LHID and NHIRD. To protect the privacy of the insured individuals, the NHRI provided a scrambled and anonymous identification number to connect the personal data, including a registry of beneficiaries and a medical service record prior to releasing the information for research. In addition, this study was approved by the Ethics Review Board of China Medical University (CMU-REC-101-012).
The disease record was based on International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). Cancer diagnoses were recorded from a 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
catastrophic illness registry, and other disease history was collected from outpatient and inpatient files.
Study population
This study consisted of a population-based, retrospective cohort study. The rhinosinusitis case cohort was established from individuals with a first incidence of rhinosinusitis (ICD-9-CM 417 and 473) diagnosed during 2000 to 2006, and the index date was set as the date of diagnosis. The comparison cohort comprised individuals without diagnosed rhinosinusitis in LHID, and randomly frequency matched by age (per 5 years) and sex at a ratio of 1:4. The index dates of the comparison individuals were randomly assigned to months and days within the same year of the index date of the patients in the rhinosinusitis cohort with whom they were matched. The follow-up of two cohorts began within six months of the index date. We excluded individuals who had a cancer (ICD-9-CM 140-208) diagnosis before their follow-up had started. The main outcome of interest in the study was the occurrence of nasopharyngeal cancer (NPC, ICD-9-CM 147). Follow-up was terminated when the individual withdrew from the insurance plan or developed NPC, or on December 31, 2010. we just collected them with confirming the rhinitis code (acute or chronic rhinitis) co-list for 3 months time period or patients underwent sinus surgery in OPD or sinus surgery 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
in admission database. Therefore, we consider them the chronic rhinosinusitis condition.
Comorbidities were also considered as a confounding factor in the study. The comorbidities were defined as a disease recorded in the inpatient and outpatient files prior to index date and included hypertension (ICD-9-CM 401-405), diabetes mellitus (DM, ICD-9-CM 250), otitis media (OM, ICD-9-CM 381.0-381.4 and 382), allergic rhinitis (AR, ICD-9-CM 477), and coronary artery disease (CAD, ICD-9-CM 410-414).
Statistical analysis
To compare the compositions of the comparison and rhinosinusitis cohorts, the continuous variable of age is presented as the mean and standard deviation (SD), and the category variables, including sex and comorbidities, are provided as the number and proportion. The t-test for continuous variables and the chi-square test for category variables were used to evaluate the difference between the two cohorts. The cumulative incidence of developing NPC was calculated as the sum of all newly diagnosed NPC events divided by the total sum of follow-up years (per 10,000 person-years). The cumulative incidence curves of NPC development were measured by the Kaplan-Meier method.
The hazard ratios (HRs) and 95% confidence intervals (CIs) were estimated by a 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
multivariable Cox proportional hazard regression model to compare the risk of developing NPC between the rhinosinusitis and comparison cohorts. We considered the risk of NPC among patients with different types of rhinosinusitis. According to the type of rhinosinusitis observed in follow-up, we separated the condition into 3 sub-cohorts: chronic sinusitis only (ICD-9-CM 473), nasal polyps only (ICD-9-CM 471), and both types. We also considered the association between rhinosinusitis severity and NPC risk. We calculated the average number of visits for rhinosinusitis as the total number of rhinosinusitis visits in follow-up divided by the follow-up years and separated the results into 3 sub-cohorts: <1 time per year, 1-2 times per year, and ≧2 times per year. The demographic-specific and comorbidity-specific HR were estimated as the individuals with rhinosinusitis compared to the individuals without rhinosinusitis under different stratifications of demographic and comorbidity factors. Lastly, to validate the association between rhinosinusitis occurrence and NPC risk, we performed a sensitivity analysis to measure the risk of developing NPC with different follow-up durations
SAS 9.3 software (SAS Institute, Cary, NC, USA) was used to manage and analyze the data. The significance level was set at less than 0.05 for the two-side testing of the p-values. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
RESULTS
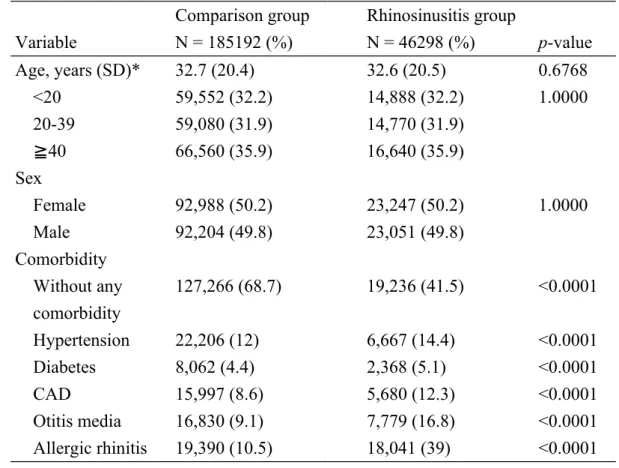
This study ultimately included cohorts of 46,298 rhinosinusitis cases and 185,192 comparison subjects with the same mean age (32 years) and sex ratios (50.2% female) (Table 1). The individuals with rhinosinusitis exhibited higher comorbidity proportions than the individuals without rhinosinusitis (p < 0.0001).
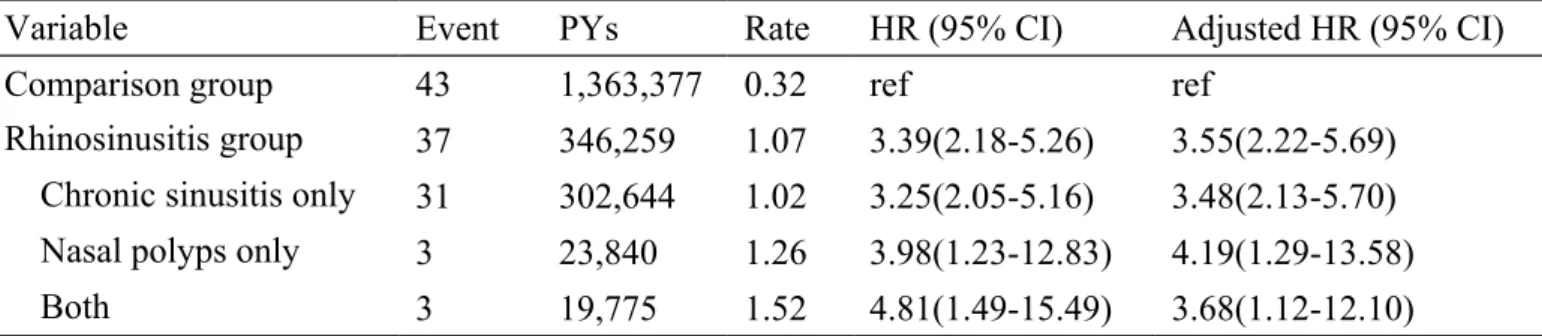
The cumulative incidence of developing NPC in the rhinosinusitis cohort was 1.07 per 10,000 person-years and 0.32 per 10,000 person-years in the without rhinosinusitis cohort (Table 2). After adjustments for age, sex, hypertension, DM, AR, OM, and CAD, the individuals with rhinosinusitis had a 3.55-fold increased risk of developing NPC compared to the individuals without rhinosinusitis (HR=3.55, 95% CI=2.22-5.69). Relative to the without-rhinosinusitis cohort, the individuals with nasal polyps only had a greater increased risk of NPC (HR=4.19, 95% CI=1.29-13.58) than the individuals with chronic sinusitis only (HR=3.48, 95% CI=2.13-5.70) and the individuals with both types of rhinosinusitis (HR=3.68, 95% CI=1.12-12.10).
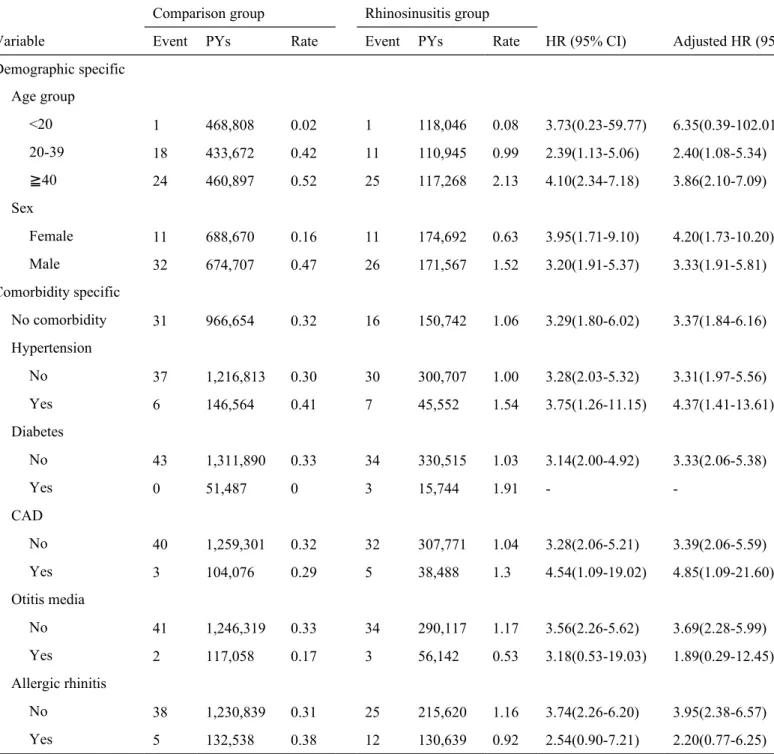
Table 3 demonstrates the demographic-specific and comorbidity-specific incidence
of NPC risk between the rhinosinusitis and comparison cohorts. The risk of developing NPC was not statistically significant between the individuals with and without rhinosinusitis aged <20 years; however, the individuals with rhinosinusitis had a significant increased risk of NPC versus those without rhinosinusitis in the older 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
age groups. Females with rhinosinusitis had a nearly 4-fold increased risk of NPC in comparison to females without rhinosinusitis, whereas males with rhinosinusitis only had a nearly 3-fold increased risk of NPC compared with males without rhinosinusitis. When the study population without any comorbidities was analyzed, those with rhinosinusitis had a 3.37-fold increased risk of NPC compared to the individuals without rhinosinusitis (HR=3.37, 95% CI=1.84-6.16). The individuals with rhinosinusitis also showed a significant association with increased NPC risk compared to the individuals without rhinosinusitis when the study subjects without each comorbiditiy.
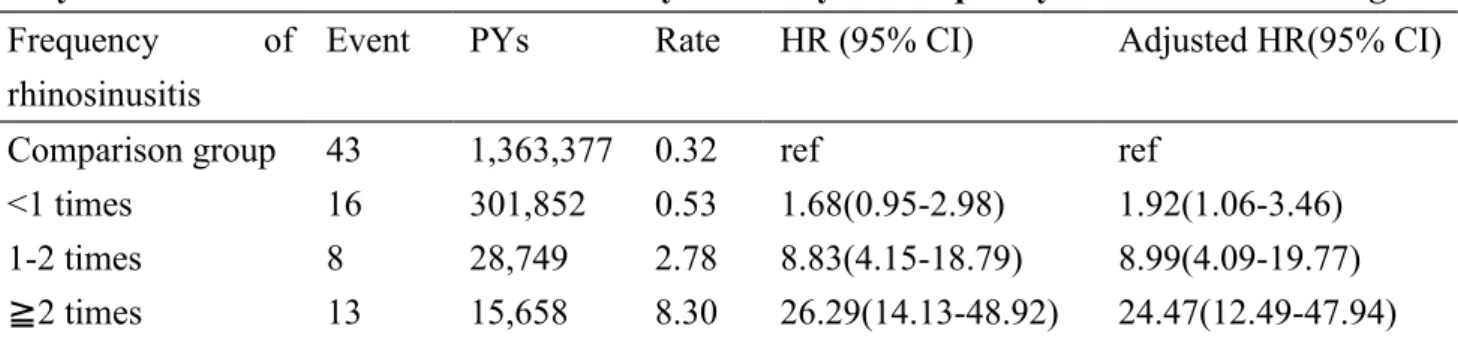
Relative to those without rhinosinusitis, the individuals with lower and median levels of average rhinosinusitis showed a significant association with an increased risk of NPC (HR=1.92 and 8.99, respectively) (Table 4). The individuals with the highest number of rhinosinusitis visits exhibited a dramatically increased risk of NPC compared to those without rhinosinusitis (HR=24.47, 95% CI=12.49-47.94). The results also revealed a significant trend of increasing risk of NPC with an enhanced average frequency of rhinosinusitis visits (p for trend < 0.0001).
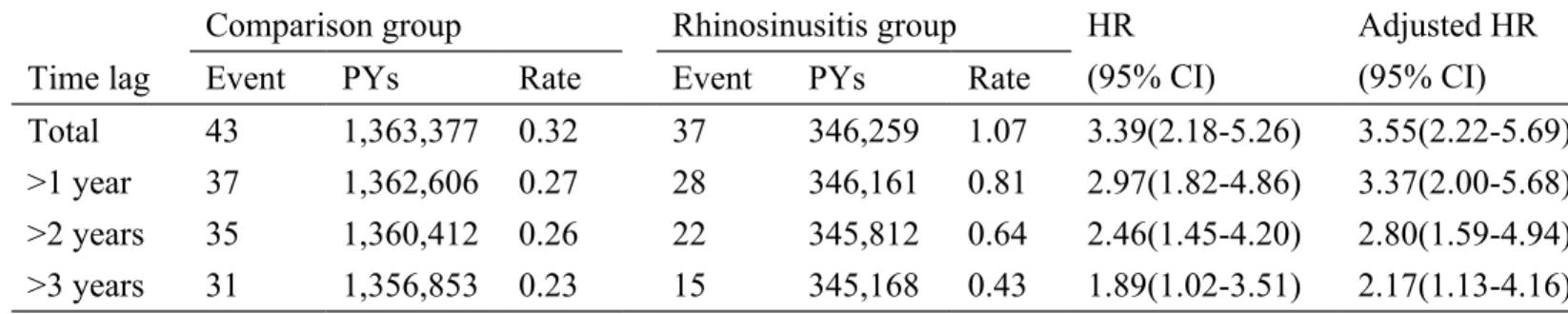
Finally, we used a sensitivity analysis to interpret the association between rhinosinusitis occurrence and the risk of developing NPC in a study population with different follow-up durations (Table 5). The rhinosinusitis cohort showed a 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
significantly increased risk of developing NPC compared to those without rhinosinusitis, even though the study population had at least 3 years of follow-up duration.
1 2 3 4
DISCUSSION
Sinusitis is an inflammatory disease of the sinus mucosa that frequently occurs during upper airway infection (URI) or viral or bacterial URI infection. Patients with long-term sinusitis may develop comorbidities of otitis media with effusion and adjacent chronic nasopharyngitis. The sustained inflammatory condition also leads to systemic comorbidities as acute myocardial infarction10. Some types of viral sinusitis, such as
EBV sinusitis, are also correlated with nasopharyngeal cancer development.
Nasopharyngeal cancer also occurs in patients with EBV nasopharyngeal infection of the upper airway, and EBV infection is related to NPC occurrence6. Indeed, the
EBV titer can be used as a prognostic factor and marker of recurrence in the follow-up of NPC patients11. Thus, sinonasal EBV infection involving the nasal sinus, nose, and
nasopharynx could suggest pre-cancerization in certain genetic varied NPC patients and presented as chronic rhinosinusitis. In addition, innate immunological problems, such as PLUNC (palate, lung and nasal epithelium clone) deficiency, also lead to NPC; the PLUNC protein is a secretory protein that has antimicrobial and anti-cancer capacities14. It has been reported that patients with NPC have nearly untraceable
PLUNC expression in their nasopharynx and sinus mucosa15, and a recent study also
showed that the expression of antimicrobial PLUNC protein in nasal polyp tissues from patients with chronic rhinosinusitis was reduced. However, the link between 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
PLUNC expression level in certain chronic rhinosinusitis and occurrence of nasopharyngeal cancer should be proved by further studies in the future.
Although adult sinusitis is common, the diagnosis of NPC in sinusitis patients may have an anatomical correlation. Nonetheless, evidence for an association between adult sinusitis and subsequent NPC is primarily derived from small-scale case series studies with a diverse range of results. Although a study conducted in the USA and published in NEJM (1976) suggested that sinusitis is a predictor of NPC19, there is no
study yet showing this, and we are the first to identify a correlation between sinusitis and NPC in a large nationwide cohort survey.
During the 3-year follow-up period, the incidence rate of NPC showed an approximately 2.17-fold greater risk, compared to the participants with no history of sinusitis. This finding supports our hypothesis that the risk of NPC is increased following a diagnosis of sinusitis in adults. Furthermore, there was a significantly higher hazard rate of NPC during the first three years of sinusitis follow up. Such evidence also supports regular medical examinations of adult sinusitis patients for the early detection of NPC during the 3 years following a sinusitis diagnosis. However, such conclusions may be limited to adult sinusitis patients in Taiwan. With the exception of the possible explanations of EBV sinusitis, poorer innate immunity, and inflammation causing cancer development, the underlying mechanisms of subsequent 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
NPC in patients with adult sinusitis remain unclear. Another mechanism is nasal airway mechanical obliteration inducing chronic hypoxia, as environmental hypoxia induces hypoxia-induced factor (HIF), which is correlated to epithelial cancer development. Thus, it is possible that sinusitis is a risk factor for NPC. However, the significantly increased risk of NPC that was observed among the sinusitis cohort even at 3 years after the initial diagnosis in our study (adjusted HR = 2.17; 95% CI, 1.13– 4.16) may indicate a multifactorial etiology. These data imply that sinusitis patients should be followed to check the nasopharynx, at least during the first 3 years.
Apart from EBV related chronic rhinosinusitis, PLUNC, and HIF, the pathogenicity related to sinusitis and NPC occurrence still needs to be studied. Although we speculate that adult sinusitis may share a common etiology with NPC by nasopharyngeal epithelium is exposed to environmental factors, including bacteria, fungi, viruses, and carcinogenic pollutants. Inflammation and/or infection in the sinus mucosa can extend to the nasopharynx through the common nasal conduit, which may contribute to the development of both sinusitis and NPC. And besides, chronic infection and inflammation have gained prominence as potentially important factors for tumor development recently, and are regarded as the seventh hallmark of cancer22, with up to 20% of cancer cases linked to chronic inflammation2324.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Studies have revealed that the chronic infection or inflammation of paranasal sinus, nose, throat, and lower respiratory tract may double the risk of NPC, suggesting that persistent inflammation and infection of the upper airway mucosa may render the nasopharyngeal mucosa more susceptible to carcinogenesis.
Moreover, bacterial growth could catalyze the reduction of nitrates to nitrites in the nasopharyngeal mucosa to form carcinogenic N-nitroso compounds29, which also
increase NPC risk30. Regardless, further mechanism studies of sinusitis and NPC are
warranted. Adult sinusitis and subsequent NPC are correlated in our nationwide population-based dataset, strengthening the statistical power through the large sample size. Moreover, the participants recruited from a wide range of demographic characteristics allowed us to perform stratified analyses according to age, sex, occupation, and urbanization level. However, there are some limitations to our findings. First, the dataset did not include information regarding health-related factors, such as smoking, diet, and family history of NPC. Therefore, we were unable to adjust for the relevant effects of such factors on the NPC risk. Second, we could not obtain the status of Epstein–Barr virus infection and its serologic markers, which are proven predictors of NPC6, as not all the participants were evaluated for viral titer during the
our study period. Thus, any association between Epstein–Barr virus infection with adult sinusitis and NPC could not be proven in our study. And even after we had 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19
collect the chronic rhinosinusitis condition in patients with rhinitis persisted for over 3 months or underwent sinus surgery finally proved by database survey, we still could not totally exclude the acute rhinitis condition. In addition, most of patients had this condition (CRS code) for over 3 times within one year, and we just use the mean to present the disease frequency. Therefore, most of them are considered chronic rhinosinusitis condition. However, we still could not totally exclude patients with repeated acute rhinitis in our study. However, this study could give us a trend of correlation to chronic rhinosinusitis and the occurrence of nasopharyngeal carcinoma.
CONCLUSION
The risk of developing NPC in Taiwanese adults was found to be approximately 3.55
times higher in those who had previously been diagnosed with sinusitis than in control participants. Thus, physicians should be aware of the statistical link to NPC when assessing sinusitis in adults. Based on the results of our study, we recommend follow-up examinations for at least 3 years. Further studies on the associations between sinusitis and NPC in other countries are warranted, particularly in areas in with a high incidence of NPC. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
ACKNOWLEDGMENTS
The study was supported in part by the study projects of National Science Council 101-2314-B-039-013-MY3, and Taiwan Department of Health Cancer Research Center for Excellence (DOH101-TD-C-111-005), and the China Medical University Hospital (Grant No. 1MS1, DMR-103-025). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. 1 2 3 4 5 6
REFERENCES
1. Anzai Y, Jarvik JG, Sullivan SD, et al. The cost-effectiveness of the management of acute sinusitis. Am J Rhinol 2007; 21:444-451.
2. Halawi AM, Smith SS, and Chandra RK. Chronic rhinosinusitis: epidemiology and cost. Allergy Asthma Proc 2013; 34:328-334.
3. Fokkens WJ, Lund VJ, Mullol J, et al. EPOS 2012: European position paper on rhinosinusitis and nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 2012; 50:1-12.
4. Rawlings BA, Higgins TS, and Han JK. Bacterial pathogens in the nasopharynx, nasal cavity, and osteomeatal complex during wellness and viral infection. Am J Rhinol Allergy 2013; 27:39-42.
5. Hulse KE, Norton JE, Suh L, et al. Chronic rhinosinusitis with nasal polyps is characterized by B-cell inflammation and EBV-induced protein 2 expression. J Allergy Clin Immunol 2013; 131:1075-1083, 1083 e1071-1077.
6. Chien YC, Chen JY, Liu MY, et al. Serologic markers of Epstein-Barr virus infection and nasopharyngeal carcinoma in Taiwanese men. N Engl J Med 2001; 345:1877-1882.
7. Grief SN. Upper respiratory infections. Prim Care 2013; 40:757-770. 8. Linder JA, Singer DE, and Stafford RS. Association between antibiotic
prescribing and visit duration in adults with upper respiratory tract infections. Clin Ther 2003; 25:2419-2430.
9. Elwany S, El-Dine AN, El-Medany A, et al. Relationship between bacteriology of the adenoid core and middle meatus in children with sinusitis. J Laryngol Otol 2011; 125:279-281.
10. Wang PC, Lin HC, and Kang JH. Chronic rhinosinusitis confers an increased risk of acute myocardial infarction. Am J Rhinol Allergy 2013; 27:e178-182.
11. Lin JC, Wang WY, Chen KY, et al. Quantification of plasma Epstein-Barr virus DNA in patients with advanced nasopharyngeal carcinoma. N Engl J Med 2004; 350:2461-2470.
12. Sheen TS, Ko JY, Chang YL, et al. Nasopharyngeal swab and PCR for the screening of nasopharyngeal carcinoma in the endemic area: a good supplement to the serologic screening. Head Neck 1998; 20:732-738. 13. Zhang Y, Wang C, Zhao Y, et al. Some polymorphisms in Epstein-Barr
virus-induced gene 3 modify the risk for chronic rhinosinusitis. Am J 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37
14. Bingle L, and Bingle CD. Distribution of human PLUNC/BPI fold-containing (BPIF) proteins. Biochem Soc Trans 2011; 39:1023-1027. 15. He Y, Zhou G, Zhai Y, et al. Association of PLUNC gene polymorphisms
with susceptibility to nasopharyngeal carcinoma in a Chinese population. J Med Genet 2005; 42:172-176.
16. Seshadri S, Lin DC, Rosati M, et al. Reduced expression of antimicrobial PLUNC proteins in nasal polyp tissues of patients with chronic rhinosinusitis. Allergy 2012; 67:920-928.
17. Tsou YA, Peng MT, Wu YF, et al. Decreased PLUNC expression in nasal polyps is associated with multibacterial colonization in chronic rhinosinusitis patients. Eur Arch Otorhinolaryngol 2013.
18. Ghafouri B, Irander K, Lindbom J, et al. Comparative proteomics of nasal fluid in seasonal allergic rhinitis. J Proteome Res 2006; 5:330-338.
19. Henderson BE, Louie E, SooHoo Jing J, et al. Risk factors associated with nasopharyngeal carcinoma. N Engl J Med 1976; 295:1101-1106.
20. Shi D, Guo W, Chen W, et al. Nicotine promotes proliferation of human nasopharyngeal carcinoma cells by regulating alpha7AChR, ERK, HIF-1alpha and VEGF/PEDF signaling. PLoS One 2012; 7:e43898.
21. Wakisaka N, Kondo S, Yoshizaki T, et al. Epstein-Barr virus latent membrane protein 1 induces synthesis of hypoxia-inducible factor 1 alpha. Mol Cell Biol 2004; 24:5223-5234.
22. Mantovani A. Cancer: Inflaming metastasis. Nature 2009; 457:36-37. 23. Coussens LM, and Werb Z. Inflammation and cancer. Nature 2002;
420:860-867.
24. Grivennikov SI, Greten FR, and Karin M. Immunity, inflammation, and cancer. Cell 2010; 140:883-899.
25. Chang ET, and Adami HO. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol Biomarkers Prev 2006; 15:1765-1777.
26. Yu MC, Garabrant DH, Huang TB, et al. Occupational and other non-dietary risk factors for nasopharyngeal carcinoma in Guangzhou, China. Int J Cancer 1990; 45:1033-1039.
27. Yuan JM, Wang XL, Xiang YB, et al. Non-dietary risk factors for nasopharyngeal carcinoma in Shanghai, China. Int J Cancer 2000; 85:364-369.
28. Zhu K, Levine RS, Brann EA, et al. Case-control study evaluating the homogeneity and heterogeneity of risk factors between sinonasal and nasopharyngeal cancers. Int J Cancer 2002; 99:119-123.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38
29. Bartsch H, Ohshima H, Pignatelli B, et al. Endogenously formed N-nitroso compounds and nitrosating agents in human cancer etiology. Pharmacogenetics 1992; 2:272-277.
30. Mirvish SS. Role of N-nitroso compounds (NOC) and N-nitrosation in etiology of gastric, esophageal, nasopharyngeal and bladder cancer and contribution to cancer of known exposures to NOC. Cancer Lett 1995; 93:17-48. 1 2 3 4 5 6 7 8 9
Table 1. Baseline demographic status and comorbidity between the comparison and rhinosinusitis groups
Variable Comparison group N = 185192 (%) Rhinosinusitis group N = 46298 (%) p-value Age, years (SD)* 32.7 (20.4) 32.6 (20.5) 0.6768 <20 59,552 (32.2) 14,888 (32.2) 1.0000 20-39 59,080 (31.9) 14,770 (31.9) ≧40 66,560 (35.9) 16,640 (35.9) Sex Female 92,988 (50.2) 23,247 (50.2) 1.0000 Male 92,204 (49.8) 23,051 (49.8) Comorbidity Without any comorbidity 127,266 (68.7) 19,236 (41.5) <0.0001 Hypertension 22,206 (12) 6,667 (14.4) <0.0001 Diabetes 8,062 (4.4) 2,368 (5.1) <0.0001 CAD 15,997 (8.6) 5,680 (12.3) <0.0001 Otitis media 16,830 (9.1) 7,779 (16.8) <0.0001 Allergic rhinitis 19,390 (10.5) 18,041 (39) <0.0001 *t-test 1 2 3 4
Table 2. Incidence of nasopharyngeal cancer and the multivariate Cox proportional hazards regression analysis-measured hazard ratio for the study cohort
Variable Event PYs Rate HR (95% CI) Adjusted HR (95% CI)
Comparison group 43 1,363,377 0.32 ref ref
Rhinosinusitis group 37 346,259 1.07 3.39(2.18-5.26) 3.55(2.22-5.69)
Chronic sinusitis only 31 302,644 1.02 3.25(2.05-5.16) 3.48(2.13-5.70)
Nasal polyps only 3 23,840 1.26 3.98(1.23-12.83) 4.19(1.29-13.58)
Both 3 19,775 1.52 4.81(1.49-15.49) 3.68(1.12-12.10)
Model adjusted for age, sex, hypertension, diabetes CAD, otitis media and allergic rhinitis PYs: person-years; Rate: incidence rate, per 10,000 person-years
1 2 3 4 5 6 7 8 9 10
Table 3. Incidence of nasopharyngeal cancer and multivariate Cox proportional hazards regression analysis measured hazard ratio for study cohort in age, sex and other comorbidities
Comparison group Rhinosinusitis group
Variable Event PYs Rate Event PYs Rate HR (95% CI) Adjusted HR (95% CI)
Demographic specific Age group <20 1 468,808 0.02 1 118,046 0.08 3.73(0.23-59.77) 6.35(0.39-102.01) 20-39 18 433,672 0.42 11 110,945 0.99 2.39(1.13-5.06) 2.40(1.08-5.34) ≧40 24 460,897 0.52 25 117,268 2.13 4.10(2.34-7.18) 3.86(2.10-7.09) Sex Female 11 688,670 0.16 11 174,692 0.63 3.95(1.71-9.10) 4.20(1.73-10.20) Male 32 674,707 0.47 26 171,567 1.52 3.20(1.91-5.37) 3.33(1.91-5.81) Comorbidity specific No comorbidity 31 966,654 0.32 16 150,742 1.06 3.29(1.80-6.02) 3.37(1.84-6.16) Hypertension No 37 1,216,813 0.30 30 300,707 1.00 3.28(2.03-5.32) 3.31(1.97-5.56) Yes 6 146,564 0.41 7 45,552 1.54 3.75(1.26-11.15) 4.37(1.41-13.61) Diabetes No 43 1,311,890 0.33 34 330,515 1.03 3.14(2.00-4.92) 3.33(2.06-5.38) Yes 0 51,487 0 3 15,744 1.91 - -CAD No 40 1,259,301 0.32 32 307,771 1.04 3.28(2.06-5.21) 3.39(2.06-5.59) Yes 3 104,076 0.29 5 38,488 1.3 4.54(1.09-19.02) 4.85(1.09-21.60) Otitis media No 41 1,246,319 0.33 34 290,117 1.17 3.56(2.26-5.62) 3.69(2.28-5.99) Yes 2 117,058 0.17 3 56,142 0.53 3.18(0.53-19.03) 1.89(0.29-12.45) Allergic rhinitis No 38 1,230,839 0.31 25 215,620 1.16 3.74(2.26-6.20) 3.95(2.38-6.57) Yes 5 132,538 0.38 12 130,639 0.92 2.54(0.90-7.21) 2.20(0.77-6.25)
PYs: person-years; Rate: incidence rate, per 10,000 person-years
Model adjusted for age, sex, hypertension, diabetes CAD, otitis media and allergic rhinitis
1 2
3 4 5
Table 4. Incidence of nasopharyngeal cancer and the multivariate Cox proportional hazards regression analysis-measured hazard ratio for the study cohort by the frequency of rhinosinusitis diagnosis
Frequency of
rhinosinusitis
Event PYs Rate HR (95% CI) Adjusted HR(95% CI)
Comparison group 43 1,363,377 0.32 ref ref
<1 times 16 301,852 0.53 1.68(0.95-2.98) 1.92(1.06-3.46)
1-2 times 8 28,749 2.78 8.83(4.15-18.79) 8.99(4.09-19.77)
≧2 times 13 15,658 8.30 26.29(14.13-48.92) 24.47(12.49-47.94)
PYs: person-years; Rate: incidence rate, per 10,000 person-years
Model adjusted for age, sex, hypertension, diabetes CAD, otitis media and allergic rhinitis p-value for trend < 0.0001
1 2 3 4 5 6
Table 5. Cox proportional hazards model-estimated nasopharyngeal cancer incidence in the study cohorts by follow-up year and the hazard ratio of NPC for the study cohorts
Comparison group Rhinosinusitis group HR
(95% CI)
Adjusted HR (95% CI)
Time lag Event PYs Rate Event PYs Rate
Total 43 1,363,377 0.32 37 346,259 1.07 3.39(2.18-5.26) 3.55(2.22-5.69)
>1 year 37 1,362,606 0.27 28 346,161 0.81 2.97(1.82-4.86) 3.37(2.00-5.68)
>2 years 35 1,360,412 0.26 22 345,812 0.64 2.46(1.45-4.20) 2.80(1.59-4.94)
>3 years 31 1,356,853 0.23 15 345,168 0.43 1.89(1.02-3.51) 2.17(1.13-4.16)
PYs: person-years; Rate: incidence rate, per 10,000 person-years
Model adjusted for age, sex, hypertension, diabetes CAD, otitis media and allergic rhinitis.
1 2 3 4 5 6