Incidence of and Mortality from Type I Diabetes in Taiwan From 1999
Through 2010: A Nationwide
Cohort Study
Wei-Hung Lin1,2*, Ming-Cheng Wang2,3*, Wei-Ming Wang4, Deng-Chi Yang2, Chen-Fuh Lam5, Jun-Neng Roan1,6, Chung-Yi Li7,8
1Institute of Clinical Medicine, National Cheng-Kung University Hospital, National
Cheng Kung University College of Medicine, Tainan, TAIWAN.
2Division of Nephrology, Department of Internal Medicine, National Cheng Kung
University Hospital, College of Medicine, National Cheng Kung University, Tainan, TAIWAN.
3Institute of Clinical Pharmacy and Pharmaceutical Sciences, College of Medicine,
National Cheng Kung University, Tainan, TAIWAN.
4Biostatistics Consulting Center, National Cheng Kung University Hospital, College
of Medicine, National Cheng Kung University, Tainan, TAIWAN.
5Department of Anesthesiology National Cheng Kung University Medical College
Tainan, TAIWAN.
6Division of Cardiovascular Surgery, Department of Surgery, National Cheng Kung
University Hospital and College of Medicine, National Cheng Kung University 7Department and Graduate Institute of Public Health, College of Medicine, National
Taichung, TAIWAN.
*These authors contribute equally to this work.
Requests for reprints should be addressed to: Chung-Yi Li, PhD (corresponding author)
Department and Graduate Institute of Public Health College of Medicine, National Cheng Kung University #1, University Rd., Tainan 701, Taiwan
TEL: 886-6-2353535 ext. 5862 FAX: 886-6-2359033
E-mail: cyli99@mail.ncku.edu.tw
Funding: This study was supported by a grant from the National Scientific Council (grant number: NSC101-2314-B-006-076 -MY3). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Authorship: All authors had access to the data and played a role in writing this manuscript.
Acknowledgments: Data from the National Health Insurance Research Database was provided by the Taiwan Bureau of National Health Insurance, Department of Health. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Type of manuscript: Research article
Key words: Epidemiology, Incidence, Population-based, Type 1 diabetes, standardized mortality ratio
Abstract
Objective: To evaluate the secular trend in incidence of and mortality from Type 1
diabetes mellitus (T1DM) in Taiwan, 1999-2010.
Methods: All 7,225 incident cases of T1DM were retrospectively retrieved from
Taiwan’s National Health Insurance Research Database from 1999 to 2010. Trend of bi-annual age- and sex-specific incidence rates of T1DM was calculated and tested with Poisson regression model. Standardized mortality ratios (SMRs) were calculated, using age-, sex-, and calendar years-specific mortality rates of the general population as the reference, to estimate the relative mortality risk of T1DM.
Results: The number of male and female T1DM was 3,471 (48%) and 3,754 (52%),
respectively. The annual number of incident T1DM increased from 543 in 1999 to 737 in 2010. The overall bi-annual incidence rate rose from 1999-00 to 2003-04 and mildly declined thereafter rose to 2009-10, with an insignificant trend (P = 0.489) over the study period. . Regardless of gender, the higher age-specific incidence rate was noted in the younger groups (<30 years) and highest at <15 years. The incidence rates in younger groups were constantly higher in female population than in male one. The SMR from all causes was significantly increased at 3.00 (95% Confidence Interval (CI) 2.83–3.16) in patients with T1DM. The sex-specific SMR was 2.66 (95% CI 2.46–2.85) and 3.58 (95% CI 3.28–3.87) for male and female patients,
respectively. For both sexes, the age-specific SMR peaked at 15-29 years.
Conclusions: Among T1DM patients in Taiwan, there were significant increasing
trends in males and female aged <15 years. We also noted a significantly increased overall and sex-specific SMR from all causes in patients with TIDM which suggests a need for improvements in treatment and care of patients with T1DM.
Introduction
Type 1 diabetes mellitus (T1DM) has been reported to increase the risk of death [1, 2], mainly resulting from hyperglycemia, which is linked to a number of acute (e.g., diabetic ketoacidosis) and chronic (e.g., diabetic nephropathy and
cardiovascular disease) complications [3]. Although treatment for T1DM improved evidently during the 1980s and 1990s with the advent of blood glucose
self-monitoring, hemoglobin A1c testing, and use of angiotensin-converting-enzyme inhibitors/angiotensin II receptor blocker [4-6], T1DM complications still frequently lead to premature mortality [7]. Recent reports from Western Europe have shown a 3 to 4-fold higher long-term mortality rate (≧15 years follow-up) in T1DM, as
compared to the general population [1, 8]. In the U.S., for example, the mortality rate of T1DM ranges from 5 to 7 times that of the general population [2, 7], and such increased risk of mortality was particularly notable for women and African Americans with T1DM. Risk of mortality from T1DM in Asian societies has rarely been reported in the literature.
A steady increase in the incidence of T1DM has been reported worldwide [9]. The incidence of this disease varies considerably among countries-e.g., it is lowest in China and Venezuela and highest in Finland and Sardinia [10]. However, long-term
population-based data on T1DM incidence in the ethnic Chinese population is very limited (11, 12). One national survey on whole diabetes found that T1DM was present in less than 1% of the diabetic population and the standardized incidence of T1DM remained constant over the recent 10 years in Taiwan (13). No nationwide research focusing on T1DM mortality in Taiwan has been published. Using a large population-based T1DM cohort in Taiwan diagnosed between 1999 and 2010, we now
investigated the long-term trends of incidence rate of T1DM in all sex and age stratifications after diagnosis and explored the overall as well as the age and sex-specific risk of mortality in patients with T1DM. Data analyzed in this study were derived from Taiwan’s National Health Insurance Research Database (NHIRD) that provides a valid and nation-wide registration system for T1DM.
Patients and methods
Data Sources
The National Health Insurance (NHI) service was launched in Taiwan on 1st March 1995. The coverage rate of the NHI from 2000 to 2007 had increased steadily from 96.1% to 98.6% [14]. The NHIRD, a large-scale computerized database, derived from this system by the Bureau of NHI and maintained by the National Health
Research Institutes (NHRI), is provided to scientists in Taiwan for research purposes. Data in NHIRD that could be used to identify patients or care providers, including medical institutions and physicians, are scrambled before being sent to the National Health Research Institutes for database construction. Data are further scrambled before being released to each researcher. Therefore, individuals cannot be identified from the database.
In Taiwan, the certification of various catastrophic illnesses is subject to evaluation and review by the Bureau of NHI. Patients with catastrophic illness certificates (CICs) are eligible for exemption from insurance premiums and co-payments. Therefore, the CICs data are highly accurate and reliable [14]. The CICs will be terminated once the patients died. Access of this study to the NHIRD has been approved by the Review Committee of the NHRI, and conduct of this study was
approved by the Institutional Review Board of National Cheng Kung University Hospital.
Identification of newly-diagnosed type 1 diabetes mellitus
We searched the Taiwan NHIRD for the T1DM population from 1 January 1999 to 31 December 2010. (as per the International Classification of Diseases, 9th
Revision, Clinical Modification, ICD-9-CM code 250). We considered the first ever registered CICs for T1DM as the newly-diagnosed T1DM patients, and excluded all CICs registered before 1999. T1DM is recognized as a catastrophic illness by the Taiwan NHI. Due to the fact that no co-payment is required for admission,
emergency, or outpatient services, this certification is only applied when detailed and specific clinical data are met, e.g., regular insulin use with a history of diabetic ketoacidosis, a positive glucagon test, or the presence of glutamic-acid-decarboxylase (GAD) antibodies [13]. This CICs registration is a valid and reliable source of data for the T1DM retrieval. Besides, cases of newly-diagnosed T1DM retrieved from the CICs are considered complete [15].
Validation
We validated the ICD-9-CM code for the identification of T1DM by analyzing the chart records for 60 patients who were randomly selected using the study method
from the inpatient claims database in National Cheng Kung University Hospital, a 1143-bed tertiary medical center in southern Taiwan, between 2002 and 2010. The contents of this database were used for reimbursements and similar to those of the NHIRD. T1DM was ascertained by the patients who had 3 or more outpatient diabetes diagnoses with insulin prescriptions, and a history of diabetic ketoacidosis, a positive glucagon test, or the presence of glutamic-acid-decarboxylase (GAD) antibodies [16, 17].
Statistical Analysis
We first calculated the age- and sex-specific proportion of T1DM in Taiwan during the study period with the age stratifications of <15, 15-29, 30-44, 45-59, and 60 years or older. To obtain the reliable estimates of incidence rates, we calculated the age- and sex-specific biannual incidence rates of T1DM over the study period. The bi-annual incident rate of T1DM was calculated by dividing the number of incident T1DM cases by the averaged mid-year population of every two years. To examine the secular trend of T1DM incidence rate across the study period, we treated the calendar year as a continuous variable and testing the statistical significance of regression coefficient derived from the Poisson regression model that simultaneously included age, sex, and calendar year in the multivariable regression model. We also employed
the 2000 WHO standard population as the reference to calculate the age- and sex-standardized incidence rate of overall T1DM bi-annually.
We selected age- and sex-matched control subjects by identifying from the national database with the age distribution of standard population and yearly mortality
counting (i.e., population of Taiwan since 1999 to 2010) collected from Department of Statistics, Ministry of the Interior, Executive Yuan, Taiwan. Compared to the all-causes mortality rates of the general population of the same age and sex, we also calculated the age, sex, and calendar year standardized mortality ratio (SMR) of patients with T1DM. The 95% confidence intervals (CIs) of SMR were estimated using the Poisson distribution. The analyses were performed using SAS software (SAS Institute Inc., Cary, NC, USA). A P-value below 0.05 was considered statistically significant.
Results
Proportion and incidence of type 1 diabetes mellitus
Figure 1 shows the age and sex specific proportions of newly-diagnosed T1DM in Taiwan from 1999 to 2010. A total of 7,225 T1DM patients were identified from the CICs between 1999 and 2010 including 3,471 males and 3,754 females. The number of newly-diagnosed T1DM was increased from 1,133 in 1999-00 to 1,276 in 2009-10, and the number of female patients was generally greater than that of male patients. The majority of T1DM were diagnosed at ages of 30 years or less in both males and females. The age and sex-specific proportions of T1DM were generally constant over the study period. In male patients, the younger group (i.e., <30 years) accounted for about 60% of the patients, while the corresponding figure for female patients was even higher at 70%.
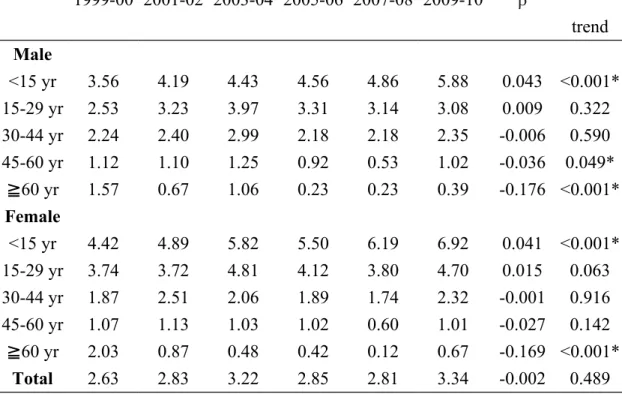
Table 1 shows the bi-annual overall as well as age- and sex-specific incidence rates of T1DM throughout 1999 to 2010. The standardized bi-annual overall incidence rate rose from 1999-00 (2.63 per 100,000) to 2003-04 (3.22 per 100,000) and then mildly declined thereafter rose to 2009-10 (3.34 per 100,000). Over the study period, the β value was -0.002 with an insignificant secular trend (P = 0.489). Regardless of gender, the highest age-specific incidence rate was noted in the younger group (<30
years) and especially highest at <15 years. Additionally, the incidence rate was constantly higher in females than in males in subjects aged <30 years during 1999 to 2010 (Figure 2). For both subjects, the mostly notable increase in incidence rate was noted for ages <15 yr in male (β = 0.043) and female (β = 0.041), respectively. . Those aged 45-60 yr (β = -0.036) and ≧60 yr (β = -0.176) in male subjects and those aged ≧60 yr (β = -0.169) in female subjects showed the greater decreases.
Mortality of type 1 diabetes mellitus
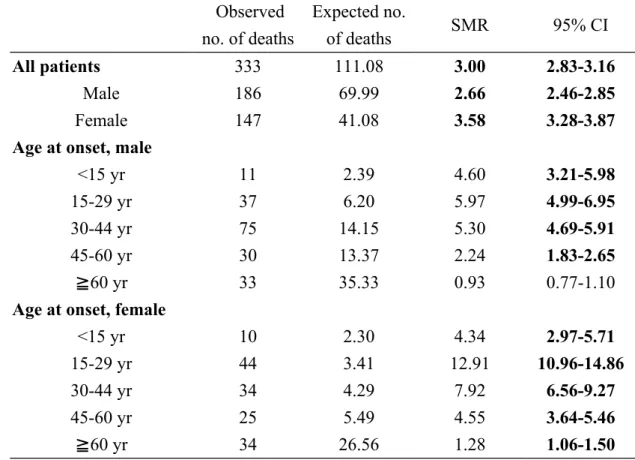
The all causes SMR in patients with T1DM was significantly increased at 3.00 (95% CI, 2.83–3.16). The sex-specific SMR for men and women was also
significantly increased at 2.66 (95% CI 2.46–2.85) and 3.58 (95% CI 3.28–3.87)
(Table 2). Among the age stratifications, the SMR peaked when age at onset was 15-29 years for both male (5.97, 95% CI 4.99-6.95) and female (12.91, 95% CI 10.96-14.86) subjects. The SMR was significantly increased at all age stratifications in females, but age at onset <60 years in male subjects.
Table 3 shows the SMR of T1DM according to the duration since diagnosis of T1DM. Among the age stratifications after T1DM onset, the SMR were significantly increased at all following time for both gender after T1DM diagnosis. The SMR for male was increased from 1.78 (95% CI 1.35-4.63) in the first year to 2.84 (95% CI
2.57-3.52) for the period of <5 yr then mildly declined to 2.66 (95% CI 2.46-2.85) for the period of <12 yr. The SMR for female was highest from 5.00 (95% CI 4.02-9.09) then declined to 3.58 (95% CI 3.28-3.87) for the period of <12 yr.
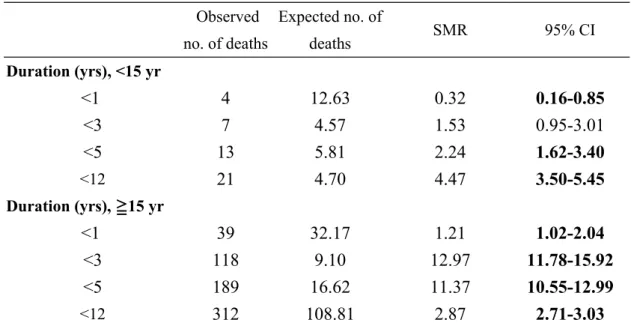
To know if the SMR is different if the diagnosis of T1DM is in childhood or in adulthood, we further divided the results in the Table 3 according to the age at onset (Table 4). Among the group of <15yr, the SMR gradually rose from 0.32 (95% CI 0.16-0.85) in the first year to 4.47 (95% CI 3.50-5.45) for the period of <12 yr. Among the group of ≧15yr, the SMR rose from 1.21 (95% CI 1.02-2.04) in the first year to 12.97 (95% CI 11.78-15.92) for the period of <3 yr then declined to 2.87 (95% CI 2.71-3.03) for the period of <12 yr.
Validation and Sensitivity Analyses
Among the randomly selected 60 patients coded with T1DM, 59 were confirmed by chart review, yielding a positive predictive value of 98.3%. Additionally, T1DM was listed in the principal diagnosis in 100.0% of the patients (data not shown in the table).
Discussion
This is the largest population-based T1DM cohort study with at least 12 years of follow-up in Taiwan. We noted that the incidence rate of T1DM was higher in
women, especially in the younger group (age at onset <30 years) and was highest when age at onset <15 years both in both sexes. Additionally, the all causes SMR was significantly increased in female patients of all age stratifications. The age-specific SMR was peaking when age at onset was 15-29 years for both sexes. Moreover, the significantly increased SMR was also noted for both gender in the variable following time especially highest for female after disease diagnosis less than one year. From our study we also found that the trend of SMR is different if the diagnosis of T1DM is in childhood (<15yr) or in adulthood (≧15yr).
It has been well-documented that the incidence of T1DM is higher among
Caucasoid populations than among Mongoloids and Blacks. The distribution of ethnic diversity shows the importance of the differential genetic susceptibility among
populations. Within ethnic groups, however, there are also geographical differences in incidence largely explained by the admixture between racial groups and possible environmental exposures [18]. The incidence of T1DM possibly has been
from undiagnosed diabetes. Compared with the Chinese population study in Shanghai [19, 20], our group may provide more reliable and updated estimates of incidence and mortality rates in patients with ethnic Chinese T1DM patients due to certain
methodological strengths including a much larger and representative study cohort. A steady increase in the incidence of T1DM has been reported worldwide [9]. From our study, we found an upward trend in the incidence of T1DM in younger age-groups (<15 yr), which is similar to the findings of other countries, buts a downward trend in older age-groups (≧60 yr). There are several possible reasons that may explain the downward trend among old ages in our study. Free health check-ups have been available for adults aged 40 years or older since 1995 in Taiwan. A diagnostic
protocol for diabetes was also proposed using fasting plasma glucose and hemoglobin A1c levels as criteria. The American Diabetes Association also lowered the fasting plasma glucose level (i.e.,126 mg/dL) in determining diabetes in 1997. Since we enrolled the study patients registered in 1999 and thereafter, therefore, the elderly T1D registered in earlier years might include some patients who had delayed diagnosis.
Studies of patients with T1DM have shown relative mortality peaking in young adults. For example, both the Pittsburgh and Denmark studies showed that relative mortality was highest in the 30–39 ages [21, 22]. The New Zealand and UK studies
showed that the highest relative mortality occurred in the 0–29 age group [23, 24]. Our study also revealed a higher relative risk of mortality noted in the younger (age at onset < 45 years) group and the highest when age at onset was 15-29 years, which was compatible with findings of the previous studies [21-24]. The higher relative risk of death for T1DM patients diagnosed during adolescence and young adults may reflect that these patients are essentially out of their parents’ control at the time of diagnosis, increasing the risk of diabetic ketoacidosis (DKA) or poor overall diabetes management [25]. Besides, the severity of T1DM itself would be different across age groups; that is, patients who have severe conditions or rapidly progressive T1DM could be detected in younger age and subsequently have a higher mortality risk.
Many studies have shown that there are no gender differences in mortality associated with T1DM, either in terms of death rates or relative risk of mortality [26-28]. In contrast, the risk of mortality relative to the New Zealand general population was higher at all ages in female T1DM than in males except in the 40–49 age group at onset, and the largest difference was noted in the 0–29 age group at onset [23]. Results from the British Diabetic Association Cohort Study also showed a higher mortality in diabetic females than in males at all ages at onset compared to the general population [24]. Finland was the country with the world’s highest incidence of T1DM and had many related researches [10, 29]. In a population based nationwide cohort
study conducted in Japan and Finland, women had a higher relative mortality in both country but men had a higher absolute mortality in the Finnish cohort. These previous findings suggested a greater effect of T1DM on mortality in female population than in males [10, 29].These previous findings are generally further supported by our study findings, showing a significantly higher SMR among female patients. One possible explanation for a higher SMR in female T1DM patients may be related to our previous findings that although the overall incidence of DKA linearly decreased between 1997 and 2005 in Taiwan, significantly sharp rising trends were still
observed in female diabetic patients aged < 35 years [30]. It has been reported that, to have a better body image, girls with diabetes often omit insulin injections to avoid
weight gain [31]. Rodin et al also reported that young female patients with T1DM
tend to have a relatively high prevalence of eating disorders, which might contribute to impaired metabolic control, and consequently result in hyperglycemia and DKA
[32]. More aggressive diabetic care programsaimed at young female patients should
be considered to reduce this emergency and possibly fatal diabetic complications.
Since women usually have lower absolute rates of mortality than men at these ages in Taiwan, clinicians must be acutely aware of this differential and be aggressive in diabetes management.
the importance of renal disease, including persistent microalbuminuria, as a marker of mortality risk and suggested that T1DM patients without renal disease achieve long-term survival comparable to the general population [33]. Taiwan was a country with a very high prevalence of end stage renal disease (ESRD) and diabetes was the leading cause [34]. Whether or to what extent the ESRD may have explained the increased risk of mortality from Taiwanese T1DM population warrants further investigations.
For males, the SMR gradually increased with the increasing duration of T1DM. But for females, the highest SMR was noted during the first year, and decreased after 5 years. Patients with T1DM have been found to experience various acute and chronic complications. DKA has been reported to be the leading cause of early mortality in T1DM, which may occur long before the peak incidence of chronic complications of diabetes [8, 35-37]. The EURODIAB mortality study reported that as many as 35% of the deaths in children diagnosed after 1989 were due to acute complications with DKA [35]. Although the etiology is not fully clear, it is found that the incidence of T1DM is relative low, but the frequency of DKA in T1DM is very high (65%) in Taiwan [38, 39]. A previous Taiwanese study [30] reported a significant rising trend of DKA incidence in female diabetic patients aged <15 years between 1997 and 2005, but such rising trend was not observed in male patients of the same age, which may largely contribute to our finding that a high SMR in the first years of T1DM diagnosis
in females, especially in the first year. It is therefore suggested that more aggressive diabetic cares aiming at young female patients are warranted. Physicians should also be more alert of the increased risk of death, especially from DKA, in children or younger adults diagnosed with T1DM.
The strengths of this work included its nationwide population-based cohort design, relative long duration of follow-up (up to 12 years), and the large number of incident cases of T1DM, which allowed us to calculate the incidence and mortality according to various sex and age stratifications. In addition, the study used the registration system of catastrophic diseases in Taiwan, which provides a good validation of disease diagnosis. Besides, based on the universal coverage system, all T1DM patients were enrolled in the study and a nationally representative sample can be assumed in our study. Findings from our study may provide the updated
information on T1DM incidence and mortality in Asian populations. Despite the above strengths, certain limitations involved in our study should be noticed. First, the claim data do not cover laboratory data and clinical details specific to T1DM, which made it impossible to determine the severity of T1DM. Second, there is no
information on the underlying cause of death in the NHI claims, thus, we were unable to estimate the cause-specific risk of mortality in T1DM.
Conclusions
In summary, the incidence rate of T1DM was highest in the young-aged group (age at onset < 15 years) in both women and men in Taiwan, and the difference in incidence rate between sexes was also greatest in this young group.We also noted an excess mortality in Taiwan’s T1DM patient population of both sexes, and of many age stratifications. Targeted strategies aimed at reducing mortality among individuals with T1DM must be considered from both clinical and health policy perspectives.
Financial & conflict of interest disclosure
No other benefits from commercial sources, or any other financial interests that any of the authors may have, gave rise to any potential conflict of interest or the appearance of a conflict of interest with regard to this work.
This work was supported by the 'Department of Internal Medicine, National Cheng Kung University Hospital' to achieve access to the NHIRD database.
Author Contributions
Conceived and designed the experiments: WHL MCW WMW LHC CYL. Analyzed the data: WHL WMW CYL. Contributed reagents/materials/analysis tools: WHL MCW DCY CFL JNR CYL. Wrote the paper: WHL MCW CYL.
References
1. Asao K, Sarti C, Forsen T, Hyttinen V, Nishimura R, et al. (2003) Long-term mortality in nationwide cohorts of childhood-onset type 1 diabetes in Japan and Finland. Diabetes Care 26: 2037-42.
2. Nishimura R, LaPorte RE, Dorman JS, Tajima N, Becker D, et al. (2001) Mortality trends in type 1 diabetes. The Allegheny County (Pennsylvania) Registry 1965-1999. Diabetes Care 24: 823-7.
3. Shankar A, Klein R, Klein BE, Moss SE. (2007) Association between glycosylated hemoglobin level and cardiovascular and all-cause mortality in type 1 diabetes. Am J Epidemiol 166(4): 393-402.
4. Goldstein DE, Walker B, Rawlings SS, Hess RL, England JD, et al. (1980) Hemoglobin A1c levels in children and adolescents with diabetes mellitus. Diabetes Care 3: 503-7.
5. Ziegler R, Heidtmann B, Hilgard D, Hofer S, Rosenbauer J, Holl R. (2011)
Frequency of SMBG correlates with HbA1c and acute complications in children and adolescents with type 1 diabetes. Pediatr Diabetes 12: 11–7.
6. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. (1993) The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. The Collaborative Study Group. N Engl J Med 329: 1456-62.
7. Secrest AM, Becker DJ, Kelsey SF, LaPorte RE, Orchard TJ. (2010) All-cause mortality trends in a large population-based cohort with long-standing childhood-onset type 1 diabetes: the Allegheny County type 1 diabetes registry. Diabetes Care 33: 2573-9.
8. Skrivarhaug T, Bangstad HJ, Stene LC, Sandvik L, Hanssen KF, et al. (2006) Long-term mortality in a nationwide cohort of childhood-onset type 1 diabetic patients in Norway. Diabetologia 49: 298-305.
9. Onkamo P, Vaananen S, Karvonen M, Tuomilehto J. (1999) Worldwide increase in incidence of Type I diabetes--the analysis of the data on published incidence trends. Diabetologia 42: 1395-403.
10. The DIAMOND Project Group. (2006) Incidence and trends of childhood Type 1 diabetes worldwide 1990-1999. Diabetic Medicine 23: 857-66.
11. Wei JN, Sung FC, Lin CC, Lin RS, Chiang CC, et al. (2003) National surveillance for type 2 diabetes mellitus in Taiwanese children. JAMA 290: 1345-50.
12. Wei JN, Li HY, Chang CH, Sung FC, Li CY, et al. (2006) Birth weight and type 1 diabetes among schoolchildren in Taiwan--A population-based case-controlled study. Diabetes Res Clin Pract 74: 309-15.
13. Jiang YD, Chang CH, Tai TY, Chen JF, Chuang LM. (2012) Incidence and prevalence rates of diabetes mellitus in Taiwan: analysis of the 2000-2009 Nationwide Health Insurance database. J Formos Med Assoc 111: 599-604.
14. Chiu YM, Lai CH. (2010) Nationwide population-based epidemiologic study of systemic lupus erythematosus in Taiwan. Lupus 19: 1250-5.
15. Chen HF, Chen P, Li CY. (2011) Risk of malignant neoplasm of the pancreas in relation to diabetes: a population-based study in Taiwan. Diabetes Care 34: 1177-9. 16. American Diabetes Association (2004) Diagnosis and classification of diabetes mellitus. Diabetes Care 27 Suppl 1: S5-S10.
17. Lawrence JM, Black MH, Zhang JL, Slezak JM, Takhar HS, et al. (2013)
Validation of Pediatric Diabetes Case Identification Approaches for Diagnosed Cases by Using Information in the Electronic Health Records of a Large Integrated Managed Health Care Organization. Am J Epidemiol.
18. Karvonen M, Tuomilehto J, Libman I, LaPorte R. (1993) A review of the recent epidemiological data on the worldwide incidence of type 1 (insulin-dependent) diabetes mellitus. World Health Organization DIAMOND Project Group. Diabetologia 36: 883-92.
19. Fu H, Shen SX, Chen ZW, Wang JJ, Ye TT, et al. (1994) Shanghai, China, has the lowest confirmed incidence of childhood diabetes in the world. Diabetes Care 17: 1206-8.
20. Shen SX, Wang HB, Chen ZW, Shen YE, Fu H, et al. (1996) The incidence of insulin-dependent diabetes mellitus in urban districts of Shanghai (1989-1993). J Pediatr Endocrinol Metab 9: 469-73.
21. Chen F, Florkowski CM, Dever M, Beaven DW. (2004) Death Certification and New Zealand Health Information Service (NZHIS) statistics for diabetes mellitus: an under-recognised health problem. Diabetes Res Clin Pract 63: 113-8.
22. DERI Mortality Study Group (1991) Sex differences in the mortality associated with insulin-dependent diabetes mellitus in four countries. The Diabetes
Epidemiology Research International (DERI) Study. Am J Epidemiol 133: 577-84. 23. Dawson SI, Willis J, Florkowski CM, Scott RS. (2008) All-cause mortality in insulin-treated diabetic patients: a 20-year follow-up. Diabetes Res Clin Pract 80: e6-9.
24. Laing SP, Swerdlow AJ, Slater SD, Botha JL, Burden AC, et al. (1999) The British Diabetic Association Cohort Study, I: all-cause mortality in patients with insulin-treated diabetes mellitus. Diabetic Medicine 16: 459-65.
25. Burnet DL, Cooper AJ, Drum ML, Lipton RB. (2007) Risk factors for mortality in a diverse cohort of patients with childhood-onset diabetes in Chicago. Diabetes Care 30: 2559-63.
26. Deckert T, Poulsen JE, Larsen M. (1978) Prognosis of diabetics with diabetes onset before the age of thirty-one. I. Survival, causes of death, and complications. Diabetologia 14: 363-70.
27. Riley MD, McCarty DJ, Couper DJ, Humphrey AR, Dwyer T, et al. (1995) The 1984 Tasmanian insulin treated diabetes mellitus prevalence cohort: an eight and a
half year mortality follow-up investigation. Diabetes Res Clin Pract 29: 27-35. 28. Borch-Johnsen K, Kreiner S, Deckert T. (1986) Mortality of type 1 (insulin-dependent) diabetes mellitus in Denmark: a study of relative mortality in 2930 Danish type 1 diabetic patients diagnosed from 1933 to 1972. Diabetologia 29: 767-72. 29. Harjutsalo V, Sjoberg L, Tuomilehto J. (2008) Time trends in the incidence of type 1 diabetes in Finnish children: a cohort study. Lancet 371: 1777-82.
30. Liu CC, Chen KR, Chen HF, Huang HL, Ko MC, et al. (2010) Trends in hospitalization for diabetic ketoacidosis in diabetic patients in Taiwan: analysis of national claims data, 1997-2005. J Formos Med Assoc 109: 725-34.
31. Meltzer LJ, Johnson SB, Prine JM, Banks RA, Desrosiers PM, et al. (2001) Disordered eating, body mass, and glycemic control in adolescents with type 1 diabetes. Diabetes Care 24: 678-82.
32. Rodin GM, Daneman D. (1992) Eating disorders and IDDM. A problematic association. Diabetes Care 15: 1402-12.
33. Orchard TJ, Secrest AM, Miller RG, Costacou T. (2010) In the absence of renal disease, 20 year mortality risk in type 1 diabetes is comparable to that of the general population: a report from the Pittsburgh Epidemiology of Diabetes Complications Study. Diabetologia 53: 2312-9.
34. U.S. Renal Data System (2012) Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States: National Institutes of
Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD.
35. Patterson CC, Dahlquist G, Harjutsalo V, Joner G, Feltbower RG, et al. (2007) Early mortality in EURODIAB population-based cohorts of type 1 diabetes diagnosed in childhood since 1989. Diabetologia 50: 2439-42.
36. Laing SP, Jones ME, Swerdlow AJ, Burden AC, Gatling W. (2005) Psychosocial and socioeconomic risk factors for premature death in young people with type 1 diabetes. Diabetes Care 28: 1618-23.
37. Laing SP, Swerdlow AJ, Slater SD, Botha JL, Burden AC, et al. (1999) The British Diabetic Association Cohort Study, II: cause-specific mortality in patients with insulin-treated diabetes mellitus. Diabetic Medicine 16: 466-71.
38. Usher-Smith JA, Thompson M, Ercole A, Walter FM. (2012) Variation between countries in the frequency of diabetic ketoacidosis at first presentation of type 1 diabetes in children: a systematic review. Diabetologia 55: 2878-94.
39. Ting WH, Huang CY, Lo FS, Hung CM, Chan CJ, et al. (2007) Clinical and laboratory characteristics of type 1 diabetes in children and adolescents: experience from a medical center. Acta paediatrica Taiwanica 48: 119-24.
Table 1. Bi-annual sex- and age-specific incidence rate (per 100,000 inhabitants) of type 1 diabetes in Taiwan, 1999-2010.
1999-00 2001-02 2003-04 2005-06 2007-08 2009-10 β P for trend Male <15 yr 3.56 4.19 4.43 4.56 4.86 5.88 0.043 <0.001* 15-29 yr 2.53 3.23 3.97 3.31 3.14 3.08 0.009 0.322 30-44 yr 2.24 2.40 2.99 2.18 2.18 2.35 -0.006 0.590 45-60 yr 1.12 1.10 1.25 0.92 0.53 1.02 -0.036 0.049* ≧60 yr 1.57 0.67 1.06 0.23 0.23 0.39 -0.176 <0.001* Female <15 yr 4.42 4.89 5.82 5.50 6.19 6.92 0.041 <0.001* 15-29 yr 3.74 3.72 4.81 4.12 3.80 4.70 0.015 0.063 30-44 yr 1.87 2.51 2.06 1.89 1.74 2.32 -0.001 0.916 45-60 yr 1.07 1.13 1.03 1.02 0.60 1.01 -0.027 0.142 ≧60 yr 2.03 0.87 0.48 0.42 0.12 0.67 -0.169 <0.001* Total 2.63 2.83 3.22 2.85 2.81 3.34 -0.002 0.489
Table 2. Standardized mortality ratio of type 1 diabetes in Taiwan according to sex and age at onset, 1999-2010.
Observed no. of deaths Expected no. of deaths SMR 95% CI All patients 333 111.08 3.00 2.83-3.16 Male 186 69.99 2.66 2.46-2.85 Female 147 41.08 3.58 3.28-3.87
Age at onset, male
<15 yr 11 2.39 4.60 3.21-5.98
15-29 yr 37 6.20 5.97 4.99-6.95
30-44 yr 75 14.15 5.30 4.69-5.91
45-60 yr 30 13.37 2.24 1.83-2.65
≧60 yr 33 35.33 0.93 0.77-1.10
Age at onset, female
<15 yr 10 2.30 4.34 2.97-5.71
15-29 yr 44 3.41 12.91 10.96-14.86
30-44 yr 34 4.29 7.92 6.56-9.27
45-60 yr 25 5.49 4.55 3.64-5.46
≧60 yr 34 26.56 1.28 1.06-1.50
Table 3. Standardized mortality ratio of type 1 diabetes in Taiwan according to duration of disease by gender, 1999-2010.
Observed no. of deaths
Expected no. of
deaths SMR 95% CI
Duration (yrs), male
<1 17 9.53 1.78 1.35-4.63
<3 69 26.02 2.65 2.33-3.69
<5 113 39.76 2.84 2.57-3.52
<12 186 69.99 2.66 2.46-2.85
Duration (yrs), female
<1 26 5.20 5.00 4.02-9.09
<3 56 14.08 3.98 3.45-5.49
<5 89 21.87 4.07 3.64-5.04
<12 147 41.08 3.58 3.28-3.87
Table 4. Standardized mortality ratio of type 1 diabetes in Taiwan according to duration of disease by <15 yr and 15 yr≧ , 1999-2010.
Observed no. of deaths Expected no. of deaths SMR 95% CI Duration (yrs), <15 yr <1 4 12.63 0.32 0.16-0.85 <3 7 4.57 1.53 0.95-3.01 <5 13 5.81 2.24 1.62-3.40 <12 21 4.70 4.47 3.50-5.45 Duration (yrs), ≧15 yr <1 39 32.17 1.21 1.02-2.04 <3 118 9.10 12.97 11.78-15.92 <5 189 16.62 11.37 10.55-12.99 <12 312 108.81 2.87 2.71-3.03
Figure Legends
Figure 1. Age and sex specific proportions of newly-diagnosed type 1 diabetes in Taiwan from 1999 to 2010.
Figure 2. Trend of bi-annual age- and sex-specific incidence rate (per 100,000
inhabitants) of type 1 diabetes in Taiwan, 1999-2010. A. In male patients B. In female patients