EARLY EXPERIENCE OF STEREOTACTIC BODY RADIOTHERAPY IN
PATIENTS WITH PRIMARY AND METASTATIC LUNG TUMORS
SBRT for Primary and Metastatic Lung Tumors
Hsin-Lun Lee1 Jo-Ting Tsai1,5 Shang-Wen Chen7 Jia-Wei Lin2 Wilson Tiu Lao3 Kum-Min Wang4 Chiu-Ping Chen1 Jeng-Fong Chiu6 Tao-Sang Chung1,5
Department of Radiation Oncology1, Neurosurgery2, Radiology3, Thoracic Surgery4, Taipei Medical University-Wan Fang Hospital
Department of Radiation Oncology, Taipei Medical University-Shuang Ho Hospital5 Department of Radiation Oncology, Taipei Medical University Hospital6
Department of Radiation Oncology, China Medical University Hospital7
李欣倫1 蔡若婷1,5 陳尚文7 林家瑋2 留偉順3 王孔民4 陳秋萍1 邱仲峰6 鍾道生1,5 台北醫學大學市立萬芳醫院 放射腫瘤科1 神經外科2 放射診斷科3 胸腔外科4 台北醫學大學署立雙和醫院 放射腫瘤科5 台北醫學大學附設醫院 放射腫瘤科6 中國醫藥大學附設醫院 放射腫瘤科7
Corresponding Author: Tao-Sang Chung
Address: No.111, Section 3, Hsin Long Road, Wen Shan District, Taipei 116, Taiwan
Tel: 02-29307930 ~ 1360
EARLY EXPERIENCE OF STEREOTACTIC BODY RADIOTHERAPY IN
PATIENTS WITH PRIMARY AND METASTATIC LUNG TUMORS
Purpose
︰
︰
︰
︰
To investigate the clinical outcomes of patients with primary and metastatic lung tumors treated by CyberKnife® (CK) stereotactic body radiotherapy (SBRT).Methods
:
:
:
:
Between November 2005 and June 2008, we treated 19 patients with SBRT at Taipei Medical University-Wan Fang Hospital. The SBRT was delivered by CK tumortracking system. Tumor response and treatment-related toxicity were evaluated by follow-up
image study. Treatment-related toxicities were scored by Common Terminology Criteria for
Adverse Events version 3.0. In this study, we reviewed their medical records retrospectively.
Results
:
:
:
:
We treated 47 lung tumors in 19 patients using CK SBRT. Eleven tumors in 8 patients were primary lung cancer, and 36 tumors in 11 patients were metastatic lung cancer.The locations of 9 tumors were central, whereas the others were peripheral. The tumor
volumes were ranged from 1.1 to 110.5 ml (median, 9.5 ml). The radiation doses were
ranged from 22 to 60 Gy, given in 2 to 4 fractions. The prescribed doses were normalized at
76% to 85% of the planned isodose. With a median follow-up interval of 12 months, we
observed that grade 2 radiation pneumonitis (RP) occurred in 3 patients (1 central; 2
peripheral), whereas we found that grade 3 RP occurred in 2 patients with central lesions.
According to the univariate analysis, female (p = 0.038) and central lesion (p = 0.042) were
two predictive factors to the occurrence of grade > 2 RP. One grade 4 tracheal complication
(tracheoesophageal fistula) and one grade 5 bronchial complication (bronchial necrosis) were
observed in two patients who had centrally located recurrent tumors and had been previous
treated with external beam radiotherapy. Four of the evaluable patients (16 patients) had
responded completely (25%), seven exhibited partial response to treatment (43.8%), and two
1-year overall survival (OS) was 63%, and the 1-year local progression-free survival (PFS)
was 84.2%. The 1-year local PFS was 87.5% for primary lung cancer and 81.8% for
metastatic lung cancer (p = 0.87). The 1-year local PFS for central and peripheral lesions was
80% and 85.7%, respectively (p = 0.63).
Conclusion
:
:
:
:
Our study showed that SBRT using the CK system was effective for treating primary and metastatic lung tumors, providing better local control and shorter treatmentcourse compared with those treated with conventional fractionated radiotherapy. Our study
also showed two predicting factors for RP. Finally, using SBRT to treat centrally located
tumor or re-irradiate recurrent tumor require additional caution due to higher risk of having
complication. Thus, we suggest that more studies are needed in the future to confirm those
findings in this study.
Key words:CyberKnife®, Stereotactic body radiotherapy, Lung tumor, Radiation pneumonitis
INTRODUCTION
Stereotactic body radiotherapy (SBRT) has been used to deal with tumors outside of
the central nervous system for more than 10 years. Due to recent advances in imaging and
radiotherapy technique, dose escalation for improving therapeutic gain has become feasible.
Several clinical studies have been reported to have the efficacy of SBRT in treating primary
or metastatic lung tumors, and promising local control rates of 80% or greater [12, 23, 26, 35,
38, 40].
The major concern is the tolerance of treatment-related normal tissue toxicities from
prescription of a large fraction size. Less standard dose-volume constraints for organs at risk
(OARs) in SBRT have been studied compared with those in conventional radiotherapy. When
using SBRT in treating lung tumors, a new strategy of dose constraints needs to be
investigated. Furthermore, care must be taken particularly when treating central lesions (i.e.
tumors close to trachea or carina) [7].
This retrospective analysis was conducted to investigate the clinical outcome in
patients with lung tumors treated with SBRT.
METHODS
Patient Eligibility
We reviewed the medical records retrospectively between November 1, 2005 and June
30, 2008 for lung cancer patients who received SBRT. We found that 47 lung tumors in 19
patients treated by CyberKnife® (CK, Accuray Inc., Sunnyvale, California, USA) at Taipei Medical University-Wan Fang Hospital. All cases were discussed by the multi-disciplinary
thoracic oncology team.
In this study, the selection criteria for CK treatment included: (1) pathological
refusal for surgery, (3) performance status being equal or smaller than 2 according to Eastern
Cooperative Oncology Group (ECOG) scale, and (4) favorable pulmonary function with
forced expiratory volume in the first second (FEV1) being greater than 70% or breath-holding
time being more than 10 seconds.
Stereotactic Treatment
The CK stereotactic radiosurgery system is a frameless, image-guided robotic
radiosurgery device which has a 6-MeV linear accelerator mounted on a robotic arm to
deliver wide-ranged radiation beams at six degrees of freedom. CK is equipped with a
real-time imaging tracking system to track for patient movement with sub-millimeter spatial
accuracy and can compensate tumor movement.
Before the SBRT, we implanted three or more gold markers (fiducials, 5 mm in length
and 0.8 mm in thickness) in the peripheral of the tumors through computed tomography
(CT)-guided percutaneous needle approach performed by experienced interventional radiologists
except in patients unsuitable for the procedure. The exclusion criteria for the fiducial implant
included: (1) contraindication to anesthetic agents, (2) having bleeding tendency, and (3)
tumor’s proximity to major vessels. Unenhanced CT was performed after the procedure to
evaluate markers location and immediate complications. We monitored patients without
complications with chest radiograph in the coming morning and then being discharged from
hospital, whereas patients with complications received further appropriate treatment in the
hospital.
We did CT simulation at least seven days after markers implantation to allow the
resolution of tissue inflammation and markers migration. Patients underwent a spiral
treatment-planning CT scan using an individualized immobilization device in the treatment
gross primary tumor and the whole thoracic cavity. All critical thoracic structures and the
lungs were contoured. Lung tumors seen in lung windows on enhanced CT were delineated as
gross tumor volumes (GTV). A 0.5 to 1 cm margin was expanded to form the planning tumor
volumes (PTV). The dose schemes and dose constraints (Table 1) were adapted based on
clinical studies results [22, 33]. The conformity index (CI) was determined from the ratio of
the prescription isodose volume (VRx) and the target volume (VPTV): CI = VRx / VPTV. The homogeneity index (HI) was determined by dividing the maximal dose (DmaxPTV) by the prescription dose to the PTV (DRxPTV): HI = DmaxPTV / DRxPTV. The centrally located tumor was defined as their proximal margin within 2 cm from trachea or main bronchus on CT scan.
The Synchrony® Respiratory Tracking System (RTS) was a subsystem of the CyberKnife® robotic treatment device to irradiate extracranial tumors that move due to respiration. In the beginning of treatment, two orthogonal X-ray images were taken at
different phases of the motion cycle. By registering these images with two digital
reconstruction radiography images from the planning CT, the absolute position of the target
relative to the fiducial markers was determined (Figure 1A). Three red light-emitting diodes
(LED) were attached on the surface of the patient's anterior chest region with maximum
respiratory motion. The camera array was continuously recorded the positions of the LED
markers as a function of time. Immediately before the treatment delivery, we created an
adaptive correlation model between the internal fiducial markers positions imaged by the
X-ray targeting system and the external LED as continuously imaged by the camera arX-ray
(Figure 1B). The RTS estimated the tumor positions by correlating the external LED motion
and implanted fiducial locations. By using the Synchrony® RTS, the tumor motion could be real-time validated and updated during treatment [8, 21].
For eight patients with unsuitable condition for the implanted procedure, we did SBRT
with the X-sight® Spine Tracking System, which used the neighboring spine structures to set up the global position of the target [15, 20].
Toxicity scoring and follow up
The primary endpoints were to analyze the local control and the treatment-related
toxicities. We did follow-up evaluations for treatment response with history taking, physical
examination and chest imaging every 3 months for the first year, every 6 months for the
second year, and annually thereafter, or any time point when being recorded to have related
pulmonary symptoms. Positron emission tomography (PET) scan was performed in selected
patients whose clinical radiological findings were indefinite. Treatment-related acute and late
toxicities were scored according to the Common Terminology Criteria for Adverse Events
version 3.0 [34]. We evaluated tumor response with CT study basing on the Response
Evaluation Criteria in Solid Tumors (RECIST) criteria [30].
Statistical analysis
The follow-up interval was defined as the duration between SBRT completion and the
last follow-up. For patients with multiple tumors concurrently irradiated by SBRT,
progression of any treated tumors was recorded as local failure. We used the Kaplan-Meier
method to calculate the local control and survival rates. The chi-square test and independent
t-test were applied to analyze the factors associated with grade 2 or greater radiation
pneumonitis.
We computed the data with the Software Package for Social Sciences (SPSS Inc.,
Chicago, Illinois, USA) version 13.0 for statistical analysis. The differences between groups
RESULTS
Patient and treatment characteristics
Forty-seven lung tumors in 19 patients were treated by CK SBRT. Eleven tumors in 8
patients were primary lung cancer (stage IIB: 2, IIIA: 1, IV: 5), and 36 tumors in 11 patients
were metastatic lung cancer. The location of 9 tumors was central, whereas that of the other
38 tumors was peripheral. Table 2 lists the patient characteristics.
The median tumor volume was 9.5 ml (range, 1.1 ml to 110.5 ml). The radiation
doses ranged from 22 to 60 Gy, given in 2 to 4 fractions. Most patients were treated with 36
to 45 Gy in 3 fractions, whereas dose was modified for small peripheral lesions (48 to 60 Gy
in 3 fractions) and centrally located tumors (22 to 45 Gy in 2 to 4 fractions). The prescribed
doses were normalized at 76% to 85% of the planned isodose.For patients with multiple
tumors, lesions were treated concurrently in 1 or 2 SBRT courses in two weeks interval.
Complications and toxicities
Among the 11 patients who received fiducials implantation, two of them developed
grade 2 pneumothorax. The pneumothorax recovered either spontaneously or after chest tube
insertion within 10 days after the implant. The incidence of implant-related pneumothorax
was 18%.
The median follow-up period for patients was 12 months. Grade 2 radiation
pneumonitis (RP) was observed in 3 patients (1 central; 2 peripheral), whereas grade 3 RP
occurred in 2 patients with central lesions. The median time of the pneumonitis occurrence
was 4 months after the SBRT. According to the univariate analysis, female (p = 0.038) and
central lesion (p = 0.042) were two predictive factors to the occurrence of grade > 2 RP
and one had bronchial necrosis (grade 5 bronchial complication). These two adverse events
were observed at 5 months after their SBRT, and the treated tumors were categorized as
centrally located tumors. Furthermore, both patients had received more than 50 Gy of thoracic
external beam irradiation about 6 months before their SBRT and they had SBRT to relieve
symptoms caused by the recurrent lung tumors. Table 4 summarizes the patients with grade 2
or greater toxicities.
Local control and survival
Three patients died within two months after SBRT, and they were excluded from the
assessment of local control. Among these three patients, two suffered from hepatocellular
carcinoma and they both died of intracranial tumor bleeding. The other one died of
inter-current sepsis. Among the evaluable 16 patients, three patients had tumor progression after
SBRT, eleven were recorded as response to treatment (4 complete response, 7 partial response)
and 2 patients had stable disease. The overall local control rate to SBRT was 81.3%
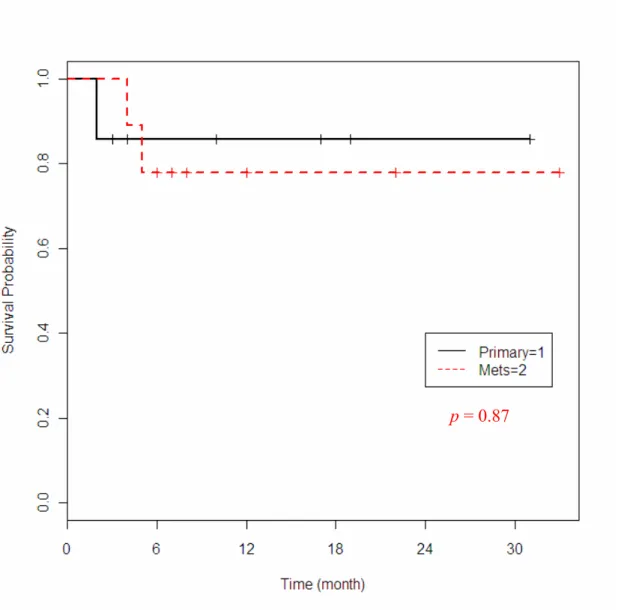
The 1-year overall survival (OS) was 63%, and the 1-year local progression-free
survival (PFS) was 84.2% (Figure 2). According to the tumor origin, the 1-year local PFS
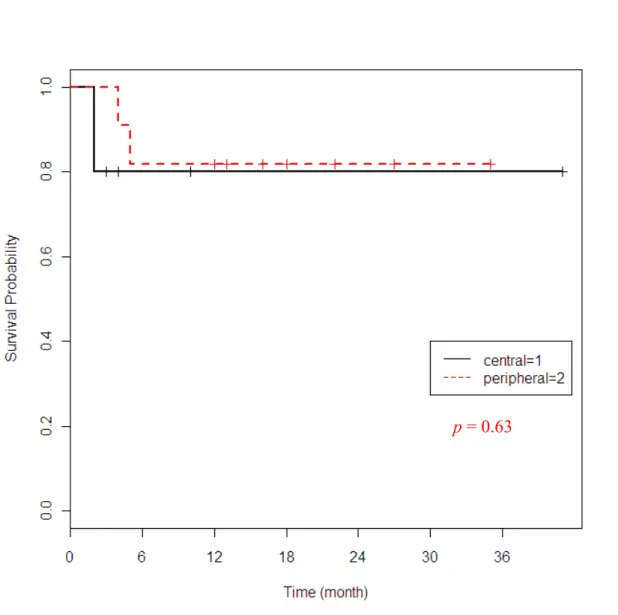
was 87.5% for primary lung cancer and 81.8% for metastatic lung cancer (p = 0.87). The
1-year local PFS for central and peripheral lesions was 80% and 85.7%, respectively (p = 0.63).
Figures 3 and 4 depict the local PFS curves according to tumor origin and location. One
patient with solitary lung metastasis showed progression free over 1 year was illustrated in
Figure 5.
DISCUSSION
Although surgical resection continues to be the standard of care for patients with lung
surgery is not feasible or is medically contraindicated. SBRT, which is allowed for a highly
precise irradiation is originally developed from stereotactic radiosurgery in the 1970s. Since,
it has been used more and more in extracranial indications [36]. In the first study of SBRT for
lung, reported in 1995 by Blomgren et al., the investigators enrolled 15 patients treated with
total doses of 20 to 40 Gy, given in 1 to 3 fractions [3]. The study result has shown
progression-free in all lesions after a median follow-up of 8 months.
Many innovative radiotherapy techniques, such as respiratory gating for tumor motion
control, the image-guided radiation therapy, and robotic radiosurgery have been emerged
recently. CK is one of the developments and has been proven to provide sub-millimeter
accuracy in SBRT using an intra-fractional tumor tracking with its robot arm [9, 21]. Despites
the potential risk of pneumothorax, bleeding, or the possibility of migration [18, 39], the
fiducials were implanted to improve SBRT delivery accuracy in many patients. Our data
showed lower incidence (18%) of pneumothorax when compared with other reports (25% to
30%) [27, 39], and no other implant-related toxicity was recorded after a two-year maximum
follow-up. This might be attributed to the routine pretreatment multi-disciplinary team
discussion and the skillful implant technique of our interventional radiologist.
With advanced imaging and radiotherapy technique, previous studies showed the
feasibility of radiation dose escalation in unresectable non-small cell lung cancer (NSCLC)
[14], and the local control rates seem to be improved further [2, 6, 40]. Wulf et al. reported a
one-year local control rate of 76 % using three to four fractions of 7 to 10 Gy to treat primary
and metastatic lung lesions [37]. In Japan series using SBRT treating stage I NSCLC, Onishi
et al. reported an overall response rate (complete response and partial response) of 84.8 % in
245 patients and favorable local control and survival with BED > 100 Gy [26]. Nagata et al.
fractions [23]. Currently, the use of SBRT in treating metastatic lung tumors is increasingly
popular with variable schemes of radiation dose [12, 17, 25].
Despites that many patients had multiple lung tumors or extra-pulmonary metastases
in our cohort, the local PFS curve for metastatic lung tumors was excellent and was nearly
equivalent to primary NSCLC (Figure 3). From our study, the local control rates for primary
and metastatic tumors approached 80% and this result is comparable with other SBRT reports
[5, 10, 29, 32]. Except that three patients experienced early death during follow-up, cancer
progression outside the irradiated field was still the main cause of mortality. Seven patients
died of extra-pulmonary disease progression, 1 treatment-related bronchial necrosis, and 2
local failure. The other 6 patients were alive (1 local progression, and 5 local progression free)
when they were seen at the last follow-up. In our study, many recruited patients were having
metastatic condition and using SBRT was intended to be palliative rather than curative. Thus,
to select suitable patients for SBRT is important to magnify the clinical benefits and optimize
the treatment outcome. Considering the factors affecting local control in SBRT for lung
tumors, there was a trend that primary or peripherally located lung tumor had a better local
control, but the difference was not significantly different in our study. Nonetheless,
comparing our data directly with the published results for local failure was difficult due to
various treatment schemes, including single dose irradiation [11, 13], single dose combined
with conventional fractionated radiotherapy [24], and hypofractionated irradiation [4].
Generally, the acute toxicity rate of stereotactic irradiation is relatively low. Therefore,
SBRT could be used for outpatients. Rib pain and skin itching were two observed acute side
effects in SBRT for lung tumors, and they were usually recovered within a few days [40].
Thus, the major concern was the risk of developing radiation pneumonitis (RP). Our result
showed that CK SBRT for central lesions were associated with severe complications, which
patients had higher rate of RP because they had smaller lung volume and smaller FEV1,
which could result in having greaterrisk of lung injury in the equivalent radiation field [28].
Our data showed similar results regarding the risk factors for predicting grade 2 or greater RP
(Table 3). But we did not have pretreatment pulmonary function data for every patient. In
addition, Morgan and Breit proposed that hypersensitivity reaction has been increased in lung
tissues of female patients because more autoimmune factors like lymphocytosis exist in
women than those in men [19]. Further investigation is required to elucidate the gender
difference in RP. Finally, two patients with re-irradiated central lesions experienced severe
toxicities (one grade 4 tracheal and one grade 5 bronchial complications), even with lower
SBRT treatment doses (28 Gy and 26 Gy, respectively). Therefore, using SBRT to re-irradiate
recurrent centrally located tumor requires additional caution to minimize the treatment-related
toxicities.
As the first SBRT report for lung tumor in Taiwan, our current treatment protocol has
provided a feasible SBRT scheme in lung tumors treatment. But our study has three
limitations. First, the median follow-up duration was short. Second, the sample size was
relatively small. And finally, bias might exist due to the heterogeneity of our patient
population. Further studies are imperative to investigate the treatment variables, including
patient selection criteria, optimal dose and fractionation, treatment planning algorithms,
uncertainty of respiratory motion, and the combination of other treatment modalities.
We are also looking forward to the result of multi-centered prospective phase III
randomized trial which we have participated in. In that protocol, we are comparing CK SBRT
with surgical resection in stage I NSCLC [16].
Our study showed that SBRT using the CK system was effective for treating primary
and metastatic lung tumors, providing better local control and shorter treatment course
compared with those treated with conventional fractionated radiotherapy. Our studyalso
showed two predicting factors for radiation pneumonitis. Finally, using SBRT to treat
centrally located tumor or re-irradiate recurrent tumor require additional caution due to higher
risk of having complication. Thus, we suggest that more studies are needed in the future to
confirm those findings in this study.
ACKNOWLEDGEMENT
Professor Winston W. Shen gave valuable editing comments on the previous versions
REFERENCES
1. Ball D: Stereotactic radiotherapy for nonsmall cell lung cancer. Current Opinion in
Pulmonary Medicine 2008; 14 (4): 297-302.
2. Baumann P, Nyman J, Lax I, et al.: Factors important for efficacy of stereotactic body
radiotherapy of medically inoperable stage I lung cancer. A retrospective analysis of patients
treated in the Nordic countries. Acta Oncologica 2006; 45 (7): 787-795.
3. Blomgren H, Lax I, Naslund I, Svanstrom R: Stereotactic high dose fraction radiation
therapy of extracranial tumors using an accelerator. Clinical experience of the first thirty-one
patients. Acta Oncol 1995; 34 (6): 861-870.
4. Brock J, Ashley S, Bedford J, Nioutsikou E, Partridge M, Brada M: Review of
hypofractionated small volume radiotherapy for early-stage non-small cell lung cancer. Clin
Oncol 2008; 20 (9): 666-676.
5. Brown WT, Wu X, Amendola B, et al.: Treatment of early non-small cell lung cancer,
stage IA, by image-guided robotic stereotactic radioablation-CyberKnife. Cancer J 2007; 13
(2): 87-94.
6. Brown WT, Wu X, Fayad F, et al.: CyberKnife radiosurgery for stage I lung cancer: results
at 36 months. Clinical Lung Cancer 2007; 8 (8): 488-492.
7. Chang JY, Balter PA, Dong L, et al.: Stereotactic body radiation therapy in centrally and
superiorly located stage I or isolated recurrent non-small-cell lung cancer. Int J Radiat Oncol
Biol Phys 2008; 72 (4): 967-971.
8. Chang SD, Main W, Martin DP, Gibbs IC, Heilbrun MP: An analysis of the accuracy of the
CyberKnife: a robotic frameless stereotactic radiosurgical system. Neurosurgery 2003; 52 (1):
140-146; discussion 146-147.
9. Chen CP, Chiu JF, Huang YC, et al.: Acceptance test for Cyberknife unit. Therapeut Radiol
10. Collins BT, Erickson K, Reichner CA, et al.: Radical stereotactic radiosurgery with
real-time tumor motion tracking in the treatment of small peripheral lung tumors. Radiat Oncol
2007; 2 (1): 39.
11. Fritz P, Kraus HJ, Blaschke T, et al.: Stereotactic, high single-dose irradiation of stage I
non-small cell lung cancer (NSCLC) using four-dimensional CT scans for treatment planning.
Lung Cancer 2008; 60 (2): 193-199.
12. Fritz P, Kraus HJ, Muhlnickel W, et al.: Stereotactic, single-dose irradiation of stage I
non-small cell lung cancer and lung metastases. Radiat Oncol 2006; 1: 30.
13. Hara R, Itami J, Kondo T, et al.: Stereotactic single high dose irradiation of lung tumors
under respiratory gating. Radiother Oncol 2002; 63 (2): 159-163.
14. Hayman JA, Martel MK, Ten Haken RK, et al.: Dose escalation in non-small-cell lung
cancer using three-dimensional conformal radiation therapy: update of a phase I trial. J Clin
Oncol 2001; 19 (1): 127-136.
15. Ho AK, Fu D, Cotrutz C, et al.: A study of the accuracy of cyberknife spinal radiosurgery
using skeletal structure tracking. Neurosurgery 2007; 60 (2 Suppl. 1): 147-156; discussion
156.
16. International randomized study to compare CyberKnife stereotactic radiotherapy with
surgical resection in stage I non-small cell lung cancer (STARS). Available on line at:
http://clinicaltrials.gov/ct2/show/NCT00840749. Accessed May 1, 2010.
17. Kavanagh BD, McGarry RC, Timmerman RD: Extracranial radiosurgery (stereotactic
body radiation therapy) for oligometastases. Semin Radiat Oncol 2006; 16 (2): 77-84.
18. Kazerooni EA, Lim FT, Mikhail A, Martinez FJ: Risk of pneumothorax in CT-guided
transthoracic needle aspiration biopsy of the lung. Radiology 1996; 198 (2): 371-375.
19. Morgan GW, Breit SN: Radiation and the lung: a reevaluation of the mechanisms
20. Muacevic A, Drexler C, Wowra B, et al.: Technical description, phantom accuracy, and
clinical feasibility for single-session lung radiosurgery using robotic image-guided real-time
respiratory tumor tracking. Technol Cancer Res Treat 2007; 6 (4): 321-328.
21. Murphy MJ, Cox RS: The accuracy of dose localization for an image-guided frameless
radiosurgery system. Med Phys 1996; 23 (12): 2043-2049.
22. Nagata Y, Matsuo Y, Takayama K, et al.: Current status of stereotactic body radiotherapy
for lung cancer. Int J Clin Oncol 2007; 12:3-7.
23. Nagata Y, Takayama K, Matsuo Y, et al.: Clinical outcomes of a phase I/II study of 48 Gy
of stereotactic body radiotherapy in 4 fractions for primary lung cancer using a stereotactic
body frame. Int J Radiat Oncol Biol Phys 2005; 63 (5): 1427-1431.
24. Nakagawa K, Aoki Y, Tago M, Terahara A, Ohtomo K: Megavoltage CT-assisted
stereotactic radiosurgery for thoracic tumors: original research in the treatment of thoracic
neoplasms. Int J Radiat Oncol Biol Phys 2000; 48 (2): 449-457.
25. Norihisa Y, Nagata Y, Takayama K, et al.: Stereotactic body radiotherapy for
oligometastatic lung tumors. Int J Radiat Oncol Biol Phys 2008; 72 (2): 398-403.
26. Onishi H, Araki T, Shirato H, et al.: Stereotactic hypofractionated high-dose irradiation
for stage I nonsmall cell lung carcinoma: clinical outcomes in 245 subjects in a Japanese
multiinstitutional study. Cancer 2004; 101 (7): 1623-1631.
27. Prévost JBG, Nuyttens JJ, Hoogeman MS, Pöll JJ, van Dijk LC, Pattynama PMT:
Endovascular coils as lung tumour markers in real-time tumour tracking stereotactic
radiotherapy: preliminary results. Eur Radiol 2008: 1-8.
28. Robnett TJ, Machtay M, Vines EF, McKenna MG, Algazy KM, McKenna WG: Factors
predicting severe radiation pneumonitis in patients receiving definitive chemoradiation for
29. Silvano G: New radiation techniques for treatment of locally advanced non-small cell lung
cancer (NSCLC). Ann Oncol 2006; 17 (Suppl. 2): 34-35.
30. Therasse P, Arbuck SG, Eisenhauer EA, et al.: New guidelines to evaluate the response to
treatment in solid tumors. European Organization for Research and Treatment of Cancer,
National Cancer Institute of the United States, National Cancer Institute of Canada. J Natl
Cancer Inst 2000; 92 (3): 205-216.
31. Timmerman R, McGarry R, Yiannoutsos C, et al.: Excessive toxicity when treating
central tumors in a phase II study of stereotactic body radiation therapy for medically
inoperable early-stage lung cancer. J Clin Oncol 2006; 24 (30): 4833-4839.
32. Timmerman RD, Park C, Kavanagh BD: The North American experience with
stereotactic body radiation therapy in non-small cell lung cancer. J Thorac Oncol 2007; 2 (7
Suppl. 3): 101-112.
33. Timmerman RD, Paulus R, Galvin J, et al.: Toxicity analysis of RTOG 0236 using
stereotactic body radiation therapy to treat medically inoperable early stage lung cancer
patients. Int J Radiat Oncol Biol Phys 2007; 69 (3 Suppl. 1): 86.
34. Trotti A, Colevas AD, Setser A, et al.: CTCAE v3.0: development of a comprehensive
grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 2003; 13 (3):
176-181.
35. Uematsu M, Shioda A, Suda A, et al.: Computed tomography-guided frameless
stereotactic radiotherapy for stage I non-small cell lung cancer: a 5-year experience. Int J
Radiat Oncol Biol Phys 2001; 51 (3): 666-670.
36. Uematsu M, Shioda A, Tahara K, et al.: Focal, high dose, and fractionated modified
stereotactic radiation therapy for lung carcinoma patients: a preliminary experience. Cancer
37. Wulf J, Hadinger U, Oppitz U, Thiele W, Ness-Dourdoumas R, Flentje M: Stereotactic
radiotherapy of targets in the lung and liver. Strahlenther Onkol 2001; 177 (12): 645-655.
38. Wulf J, Haedinger U, Oppitz U, Thiele W, Mueller G, Flentje M: Stereotactic
radiotherapy for primary lung cancer and pulmonary metastases: a noninvasive treatment
approach in medically inoperable patients. Int J Radiat Oncol Biol Phys 2004; 60 (1): 186-196.
39. Yousefi S, Collins BT, Reichner CA, et al.: Complications of thoracic computed
tomography-guided fiducial placement for the purpose of stereotactic body radiation therapy.
Clin Lung Cancer 2007; 8 (4): 252-256.
40. Zimmermann FB, Geinitz H, Schill S, et al.: Stereotactic hypofractionated radiotherapy in
stage I (T1-2 N0 M0) non-small-cell lung cancer (NSCLC). Acta Oncologica 2006; 45 (7):
Table 1. Dose constraints in lung tumor treated with CK
Organ Dose Constraint
Spinal Cord Max < 18Gy (6 Gy/fraction)
Esophagus Max < 27Gy (9 Gy/fraction)
Max < 30Gy (7.5 Gy/fraction)*
Trachea and Ipsilateral Bronchus Max < 30 Gy (10 Gy/fraction)
Ipsilateral Brachial Plexus Max < 24 Gy (8 Gy/fraction)
Heart Max < 10 Gy/fraction
Whole Lung (GTV excluded) V20 < 20%
PTV CI< 1.5, HI < 1.5
Desired isodose >75%
Desired target coverage >95%
Abbreviation: Max = maximum dose; CI = conformity index; HI = homogeneity index
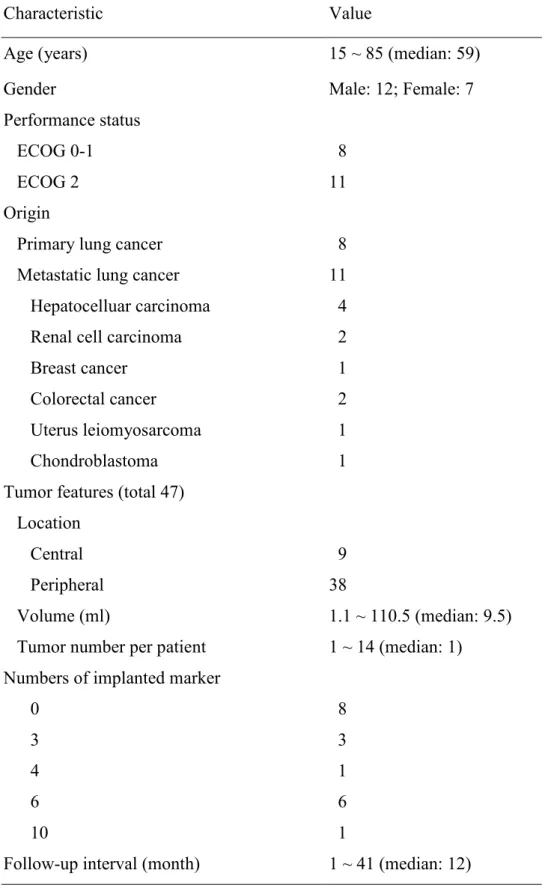
Table 2. Patient characteristics (n=19)
Characteristic Value
Age (years) 15 ~ 85 (median: 59)
Gender Male: 12; Female: 7
Performance status
ECOG 0-1 8
ECOG 2 11
Origin
Primary lung cancer 8
Metastatic lung cancer 11
Hepatocelluar carcinoma 4
Renal cell carcinoma 2
Breast cancer 1
Colorectal cancer 2
Uterus leiomyosarcoma 1
Chondroblastoma 1
Tumor features (total 47) Location
Central 9
Peripheral 38
Volume (ml) 1.1 ~ 110.5 (median: 9.5)
Tumor number per patient 1 ~ 14 (median: 1) Numbers of implanted marker
0 8
3 3
4 1
6 6
10 1
Follow-up interval (month) 1 ~ 41 (median: 12)
Table 3. Univariate analysis of factors related to Grade > 2 radiation pneumonitis after CK treatment Factor N > Gr.2 RP (%) OR 95% CI p-value Chi-square test Gender 1.161 – 185.235 0.038 Male 12 1 (8.33) 1 Female 7 4 (57.14) 14.667 Performance status 0.332 – 21.739 0.603 ECOG 0-1 8 3 (37.50) 2.70 ECOG 2 11 2 (18.18) 1 Origin 0.141 – 8.995 1.000
Primary lung cancer 8 2 (25.00) 1
Metastatic lung cancer 11 3 (27.27) 1.125
Tumor location 1.235 – 66.667 0.042
Central 9 3 (33.33) 9.009
Peripheral 38 2 (5.26) 1
Fiducial marker implant 0.332 – 21.977 0.603
Yes 11 2 (18.18) 1 No 8 3 (37.50) 2.700 Factor p-value Independent t-test Age 0.612 Tumor volume 0.210
Tumor number per patient 0.406
Abbreviation: RP = radiation pneumonitis; OR = odds ratio; CI = confidence interval; ECOG = Eastern Cooperative Oncology Group
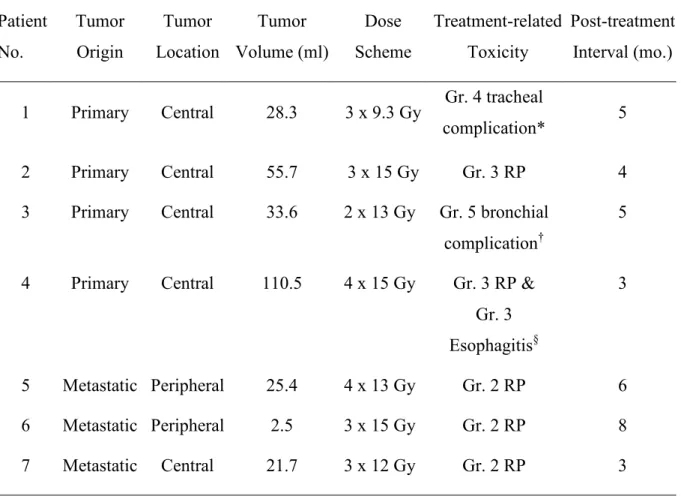
Table 4. Details for patients with symptomatic complications after CK treatment Patient No. Tumor Origin Tumor Location Tumor Volume (ml) Dose Scheme Treatment-related Toxicity Post-treatment Interval (mo.)
1 Primary Central 28.3 3 x 9.3 Gy Gr. 4 tracheal
complication* 5
2 Primary Central 55.7 3 x 15 Gy Gr. 3 RP 4
3 Primary Central 33.6 2 x 13 Gy Gr. 5 bronchial complication†
5
4 Primary Central 110.5 4 x 15 Gy Gr. 3 RP & Gr. 3 Esophagitis§ 3 5 Metastatic Peripheral 25.4 4 x 13 Gy Gr. 2 RP 6 6 Metastatic Peripheral 2.5 3 x 15 Gy Gr. 2 RP 8 7 Metastatic Central 21.7 3 x 12 Gy Gr. 2 RP 3
Abbreviation: RP = radiation pneumonitis
*Tracheoesophageal fistula †
Bronchial necrosis §
Figure 1. The Synchrony® Respiratory Tracking System (RTS) for lung SBRT:
(A) Registration of real time orthogonal X-ray images with digital reconstruction radiography images from the planning CT for fiducial markers tracking
(B) Building the adaptive correlation model for target position tracking and correction during continuous respiratory cycle
Figure 3. Progression free survival curves of patients with (1) primary and (2) metastatic lung tumors treated with CK (n = 19)
Figure 4. Progression free survival curves of patients with (1) centrally and (2) peripherally located lung tumors treated with CK (n = 19)
Figure 5. Serial follow-up CT images of a patient with solitary right lower lobe lung metastasis treated with CK SBRT, 36 Gy /3 fractions to 88% isodose
Before CK Post CK 3 mo. Post CK 6 mo. Post CK 12 mo.
使用立體定位體部放射治療於原發性和轉移性肺腫瘤病患之早期經驗
使用立體定位體部放射治療於原發性和轉移性肺腫瘤病患之早期經驗
使用立體定位體部放射治療於原發性和轉移性肺腫瘤病患之早期經驗
使用立體定位體部放射治療於原發性和轉移性肺腫瘤病患之早期經驗
目的 目的 目的 目的::::探討使用電腦刀立體定位體部放射治療 (SBRT) 於原發性和轉移性肺腫瘤病患之 臨床結果。 方法 方法 方法 方法:回溯性探討自 2005 年 11 月至 2008 年 6 月間於萬芳醫院接受 SBRT 之 19 位病患 的醫療記錄。SBRT 是運用電腦刀之腫瘤追蹤系統來實行治療。治療後腫瘤反應和相關之副作用是以追蹤影像進行評估。治療相關副作用則以 Common Terminology Criteria
for Adverse Events version 3.0 分級來記錄副作用之嚴重程度。
結果 結果 結果 結果::::於接受電腦刀 SBRT 之 19 位肺腫瘤病患(共 47 顆肺腫瘤)中,8 位(11 顆腫 瘤)為原發,11 位(36 顆腫瘤)為轉移。9 顆腫瘤位於中央,其餘位於週邊。腫瘤體 積介於 1.1 至 110.5 毫升(中位數, 9.5 毫升)。放射治療之劑量介於 22 至 60 Gy,歸一 化於 76%至 85%之等劑量曲線,分 2 至 4 次給予。於 12 個月之中位追蹤時間中,共有 3 位病患發生 2 級放射性肺炎,另有 2 位病患發生 3 級放射性肺炎。分析其風險因子, 女性(p = 0.038)和中央型肺腫瘤(p = 0.042)於單變項分析中有統計學上之差異。在 兩位為復發中央型肺腫瘤且先前己接受過肺部體外放射治療之病患中,觀察到氣管食 道瘺管及支氣管壞死之治療相關副作用。於 16 位可供分析局部控制率的病患中,4 位
(25%)為 complete response,7 位(43.8%)為 partial response,2 位(12.5%)為
stable disease,3 位(18.7%)為 progressive disease。病人一年之整體存活率為 63%,
一年之局部無病存活率為 84.2%。比較原發性和轉移性肺癌之一年局部無病存活率
(87.5% vs. 81.8%, p = 0.87),以及中央型和週邊型肺腫瘤之一年局部無病存活率
結論 結論 結論 結論::::於我們的早期經驗中,電腦刀立體定位體部放射治療能有效局部控制原發性和 轉移性肺腫瘤,然而,治療中心型或先前己照射過放射線之復發肺腫瘤時,應特別謹 慎以避免較嚴重之副作用。 關鍵詞 關鍵詞 關鍵詞 關鍵詞::::電腦刀、立體定位體部放射治療、肺腫瘤、放射性肺炎