Developing an Analytic Framework of Health Information Exchange : A Case Study
of Regional Health Information Organization in U.S.
張 音
a,b, 楊澤泉
c*In Chang ab PhD., Tzer-Chyun Yang c* PhD.
a
Department of Medical Informatics, National Cheng Kung University Medical College and Hospital,Taiwan
bBiotechnology Office, Science and Technology Group, Executive Yuan, Taipei, Taiwan
cDepartment of Business Administration, National Cheng Kung University, Tainan, Taiwan
*通訊作者
:
楊澤泉
,
[email protected]
摘要 可互通電子病歷最近在台灣開始受到重視,這需要一個 可互通的基礎建設來支持,以協助臨床專業人員在做臨 床或處置決策時,可即時取得重要的健康照護資訊。美 國在國家健康資訊基礎建設計畫下,為建置國家級健康 資訊交換網路,規劃以「區域健康資訊組織」為基石, 來落實區域級電子健康資訊網路的互通,以加速社區中 電子病歷系統的使用。由於美國較早發展國家健康資訊 基礎建設,以及台灣尚未具有建置可永續經營健康資訊 交換系統的實作經驗,因此本文目的係提供美國建置健 康資訊交換系統的實作經驗,以供政府單位及相關機構 參考。本研究發展一個健康資訊交換的分析架構,並選 取一個「區域健康資訊組織」進行個案分析。台灣在建 立可互通健康資訊基礎建設方面尚屬啟始階段,但在有 關「區域健康資訊組織」的角色、治理,和永續經營等 議題上仍應加以重視,俾利日後能發展出可永續經營的 商業模式。本研究所發展的分析架構,未來可進一步廣 泛應用在台灣的個案分析上。藉由對「區域健康資訊組 織」的特性,以及對可互通健康資訊基礎建設的宏觀及 微觀層次議題的更多暸解,將有助我們發展可行的健康 資訊交換政策,加速台灣電子病歷的使用。 關鍵字:健康資訊交換、區域健康資訊組織、電子病歷 AbstractAttention to the use of interoperable electronic medical records is intensifying rapidly in Taiwan. This will require
an interoperable infrastructure to help clinicians get access to critical health care information when their clinical or treatment decisions are being made. To implement such a national health information exchange network of NHII in U.S., regional health information organizations (RHIOs) are envisioned as a building block for interconnecting electronic health information networks at the regional level and accelerating the adoption of EMRs in communities. Due to the earlier development of NIII in U.S and the lack of real-world implementation of a sustainable HIE system in Taiwan, the aim of this study is to obtain experiences of a sustainable HIE case from U.S.. A case study of RHIO was performed based on an analytic framework developed in our study. Although building an interoperable HIE infrastructure in Taiwan remains in its infancy, the issues regarding the role, governance, and sustainability of RHIOs should be addressed in order to develop a sustainable business model. The analytic framework of HIE developed in our study can also be widely used to furthermore analyze Taiwan’s RHIO cases. With an understanding of these RHIO’s characteristics, macro-level and micro-level issues of interoperable health information infrastructure, we can develop enabling HIE policies to facilitate the use of EMR in Taiwan.
Health Information Organization (RHIO), Electronic Medical Record (EMR)
1. Introduction
Information technology has significant potential to meet the diverse needs of patients and providers in a health care environment burdened by rising costs, inefficiency, and poor quality of care [1, 2]. Over the past decade, significant initiatives, such as electronic medical record (EMR) and healthcare information exchange (HIE) systems, have been proposed to prompt the adoption of healthcare information technology (HIT) [3, 4].
To transform the delivery of health care, the U.S. government has established a 10-year plan in 2004 by building a new national healthcare information infrastructure (NHII), including EMR and a new network to link medical records nationwide. Many developed countries, such as Canada, UK and Australia, have also devoted considerable time and resources to building their NHII and encouraging EMR adoption in recent years [5, 6]. Attention to the use of interoperable electronic medical records is intensifying rapidly in Taiwan recently, with the Department of Health (DOH) calling for widespread adoption of EMRs within the next five years [7, 8, 9]. Not many studies have been performed so far to understand the challenges of implementing HIE and EMR exchange [2, 10]. Due to the earlier development of NIII in U.S and the lack of real-world implementation of a sustainable HIE system in Taiwan, the aim of this study is to obtain experiences of a sustainable HIE case from U.S.. A case study of RHIO was performed based on an analytic framework developed in our study. The results of our study, we expect, will be very beneficial for the government in setting HIE strategies and policies.
2. Literature review
NHII can be defined as: “a comprehensive knowledge-based network of interoperable systems of
clinical, public health, and personal health information that is intended to improve decision making by making health information available when and where it is needed” [6]. The new vision of NHII in U.S. is to realize the consumer-centric and information-rich care through the use HIT [5].
Interconnecting clinicians, one of major goals in NHII, will allow information to be portable and to move with consumers from one point of care to another. This will require an interoperable infrastructure to help clinicians get access to critical health care information when their clinical or treatment decisions are being made. To implement such a national health information exchange network in NHII, regional health information organizations (RHIOs) are envisioned as a building block for interconnecting electronic health information networks at the regional level and accelerating the adoption of EMRs in communities [6].
Broadly, HIE is likely to consist of many networks that are capable of communicating and exchanging information with each other. Some networks will be geographically defined (so-called regional health information organizations, or RHIOs); others will be defined by affinity groups of various kinds – networks of cancer research center, collaborating businesses, or distributed enterprises.
Internally, these networks may take a variety of approaches to governance, data standards, data management, financing, and privacy policies [10, 11]. A RHIO also can be defined as a multi-stakeholder organization that enables the secure exchange and use of patient health information among clinicians and caregivers to improve the delivery, efficiency, quality, and safety of patient care [12].
The ultimate goal of HIE system is interconnecting electronic health information networks and linking patient
data across multiple healthcare settings; transform how healthcare data is delivered, positively affecting patient safety while reducing medical errors and healthcare costs [5]. However, HIE is not an entirely new concept. The Community Health Information Networks (CHINs) of the 1990s in U.S. were an early attempt to create interoperability at the local level [13, 14]. Unfortunately, by 2000 nearly all of them failed. The concept of streamlining health information to support health care was an intellectually supported “concept”, but not fully conceptualized at the implementation level [15]. The reasons they failed include lack of financing, inadequate buy-in and conflicting missions, lack of trust, the need for centralized databases and desire for control, data ownership issues, and the high cost of network technology [12, 16].
3. Materials and Methods
In this study, we used a range of methods to gather materials of a RHIO case, including the literature review, expert interview, and case study. A systematic literature review was initially performed to develop an analytic framework for the HIE case study. Next, a case study design was used to perform an analysis of one specific HIE case in U.S..
We focused our efforts initially on analyzing published sources for HIE cases, where these were lacking, turned to experts to fill critical gaps. An expert interview was convened in U.S. to advise us throughout this study. We also interviewed two other experts, including hospital information systems executives working with various facets of interoperability and directors of regional data-sharing initiatives in U.S.
The primary case was collected based on the published literatures [1, 16] and recommended by the experts in an expert interview. The case selected is a regional HIE in U.S., called “Simplifying Healthcare Among Regional
Entities (MA-SHARE)”, which is one of successful regional HIEs designed for electronic medical record exchange in NHII.
4. Developing an analytic framework of HIE
An analytic framework for HIE in our study was developed based on these key measures which were solicited from the prevailing HIE research result [16, 17, 18] and confirmed through discussions in an expert interview. The analytic framework developed by our study includes several key measures as follows.
(1) Significant drivers: 7 items developed by eHi [17] were used to assess significant drivers of RHIOs. These items include: improving quality of healthcare, improving patient safety, inefficiencies experienced by providers, rising health-care costs, availability of grant funding, increased attention on HIT, public health surveillance needs
(2) Development stage: 7 stages developed by eHi [17] were used to evaluate the development stage of RHIOs. These stages include: stage 1(recognition of the need for health information exchange among multiple stakeholders in your state, region or community), stage 2 (getting organized; defining shared vision, goals, and objectives; identifying funding sources, setting up legal and governance structures), stage 3 (transferring vision, goals and objectives to tactics and business plan; defining your needs and requirements; securing funding), stage 4 (well under way with implementation – technical, financial and legal), stage 5 (fully operational health information organization; transmitting data that is being used by healthcare stakeholders), stage 6 (fully operational health information organization; transmitting data that is being used by healthcare stakeholders and have a sustainable business model), stage 7 (demonstration of expansion of organization
to encompass a broader coalition of stakeholders than present in the initial operational model).
(3) Core organizational roles and functions: two organizational roles and three distinct organizational functions developed by FORE [16] were used to assess the roles and functions of RHIOs. These items include: the role of governance (functions for convening and educating), and the role of technical operations (for operating and managing).
(4) HIE activities and services: 5 items developed by Labkoff & Yasoff [18] were used to assess HIE activities and services of RHIOs. These items include: patient care, public health, clinical research, quality improvement, and health care operations
(5) Funding and financial model: two types of financial modes developed by FORE [16] were used to assess financial sustainability of RHIOs. These items include: initial funding and sources of revenue. Using above key measures in this analytic framework, a summary of description and analysis of our case study will be listed in the next section.
5. Result - An analysis of a RHIO case
The RHIO in Massachusetts, called “Simplifying Healthcare Among Regional Entities” (MA-SHARE), is geographically based on the majority of healthcare in the state in the Boston metro area. Massachusetts (MA) includes three large integrated delivery networks (CareGroup, Partners and Caritas) cover approximately 6,35 million residents. The Massachusetts Health Data Consortium (MHDC) was founded in 1978 as a nonprofit coalition by the public and private health care organization of the Commonwealth to develop a system for collecting, organizing, and disseminating data on all hospital care in the state.
MA-SHARE serves as the de-factor RHIO for Massachusetts. It is a regional collaborative initiative
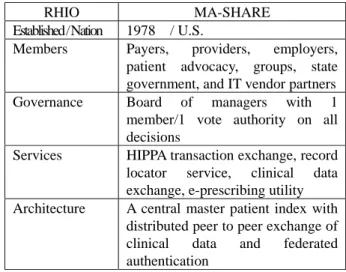
operated by the MHDC which seeks to promote the inter-organizational exchange of healthcare data using information technology, standards and administrative simplification, in order to make accurate clinical health information available wherever needed in an efficient, cost-effective and safe manner. A summary of characteristics of MA-SHARE is listed in Table 1.
Table 1. A summary of characteristics of MA-SHARE
RHIO MA-SHARE Established / Nation 1978 / U.S.
Members Payers, providers, employers, patient advocacy, groups, state government, and IT vendor partners Governance Board of managers with 1
member/1 vote authority on all decisions
Services HIPPA transaction exchange, record locator service, clinical data exchange, e-prescribing utility
Architecture A central master patient index with distributed peer to peer exchange of clinical data and federated authentication
5.1 Significant drivers
MA-SHARE demonstrates that it can serve as a mechanism to address an array of technical, legal, and policy issues to serve regional health policy interests. The most significant drivers were “improving quality of healthcare”, “improving patient safety”, and “public health surveillance needs”. Table 2 provides a list of significant drivers for HIE development of MA-SHARE.
Table 2. Significant drivers for HIE development
Significant drivers RHIO (MA-SHARE)
Improving quality of healthcare Improving patient safety
Inefficiencies experienced by providers
Rising health-care costs Availability of grant funding Increased attention on HIT Public health surveillance needs
5.2 Development stage
stage 6, which is a “fully operational health information organization; transmitting data that is being used by healthcare stakeholders and have a sustainable business model”. Our study indicated that health information exchange initiatives are continuing to mature in U.S. according to the result of eHI survey of U.S. 130 regional HIE initiatives [17]. Among these, 32 organizations reported that they were “fully operational” in stage 5, 6, and 7.
5.3 Core organizational roles and functions
The governance structure of MA-SHARE is a combination of efforts from several entities that comprise a virtual state-level RHIO. Close communication and coordination is achieved due to the fact that many of the same people are on the Boards of these four organizations. MHDC serves as a convener, lobbying and policy organization.
MA-SHARE is a wholly owned subsidiary of MHDC. MHDC appoints the MA-SHARE Board members. MA-SHARE serves as the grid for clinical operability for the state and provides community utility services that support secure clinical data exchange with a Resource Locator Service (RLS).
MA-SHARE’s characteristics of operations and technology are described as below [16, 20]:
(1). Technical model: MA-SHARE hosts the record locator service and creates all the clinical exchange gateway software that resides at each provider site and enables peer to peer data exchange. Quality data warehouse is centralized, but is deidentified.
(2). Hardware and software: All hardware is currently owned by stakeholders and is housed at their locations. MA-SHARE is deploying shared hardware for selected central functions in 2006. A computer company provides development services and integrates commercial products.
(3). Standards: MA-SHARE does not plan to do any mapping or coding of labs, but rather to have the data providers map them at the local level.
(4). Training and support: Provide training to trainers. (5). Intellectual property: MA-SHARE believes in open
source for all its software, and plans to release all as open source.
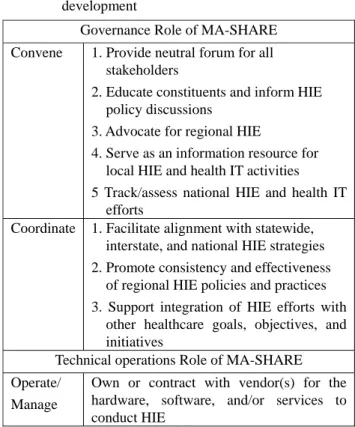
Table 3 provides a list of Organizational roles and functions for HIE development in MA-SHARE.
Table 3. Organizational roles and functions for HI E development
Governance Role of MA-SHARE Convene 1. Provide neutral forum for all
stakeholders
2. Educate constituents and inform HIE policy discussions
3. Advocate for regional HIE
4. Serve as an information resource for local HIE and health IT activities 5 Track/assess national HIE and health IT
efforts
Coordinate 1. Facilitate alignment with statewide, interstate, and national HIE strategies 2. Promote consistency and effectiveness
of regional HIE policies and practices 3. Support integration of HIE efforts with
other healthcare goals, objectives, and initiatives
Technical operations Role of MA-SHARE Operate/
Manage
Own or contract with vendor(s) for the hardware, software, and/or services to conduct HIE
5.4 HIE activities and services
There are several community utilities implemented to best serve the needs of the MA state as follows: (1). ePrescribing: Statewide ePrescribing gateway infrastructure connecting SureScripts, RxHub, payers and providers deployed in May 2006. (2). Clinical data exchange: MA-SHARE went live with lab, allergies, problem lists, and medication history by the end of 2006. (3). Medication history: eRx Gateway was developed to
do provider identifier mapping and went live in May 2006. (4). Public heath: Several local hospitals participate in the CDC’s BioSense project and transmit Emergency department chief complaint data to CDC every 15 minutes. Since 2003, Boston based emergency departments provide demographic and discharge data to the state department of health.
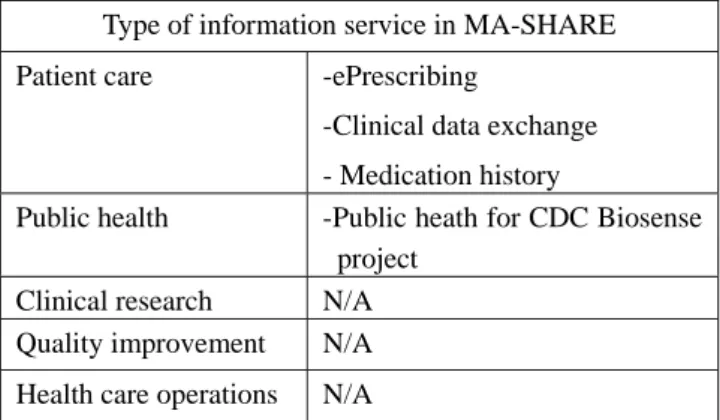
Table 4 HIE activities and services
Type of information service in MA-SHARE Patient care -ePrescribing
-Clinical data exchange - Medication history
Public health -Public heath for CDC Biosense project
Clinical research N/A Quality improvement N/A Health care operations N/A
5.5 Funding and financial model
Initial funding: The various entities in MA have received initial funding from a variety of sources. For example, MA-SHARE received $3.4 MM from grants from stakeholders. It also is a market for the NHII national architecture contract. They have also received eHealth Initiative funding, Markle foundations, and other grants. Sustainability model: MA-SHARE has implemented a subscription fee model for ePrescribing ($50K-$100K per year depending on size) and plans to do the same for clinical data exchange services. They believe that “collaborating to jointly invest in fixed costs to reduce overall costs for all is a more effective model than transaction fees.” Their approach is to create a utility to do several things, and expect that entities will pay membership fee in relation to the value derived from using MA-SHARE services. MA-SHARE plans to begin to receive revenue in 2007 and self-sustaining in 2008.
Table 5. initial funding and source of revenues
Regional HIE MA-SHARE
Source of initial funding
1.Grants from the NHIN architecture contract
2. Grants from stakeholders 3. Grants from eHealth Initiative
funding, Markele foundations, and others.
Source of revenues
1. Grants and contracts from the government
2. Subscription fee
6. Discussion and Conclusion
Due to the lack of real-world implementation of a sustainable HIE system in Taiwan, our study developed an analytic framework of HIE and analyzed a successful case of RHIO in U.S. in order to understand what are those critical factors affecting a RHIO. Through analyzing a RHIO using our framework, we can focus on characteristics of a RHIO, such as organizational structure, time of establishment, members, services, and technical architecture. A further analysis can focus on integrating the macro-level issues of interoperable health information infrastructure and the micro-level issues of HIE case such as significant drivers, the development stage, core organizational roles and functions, HIE activities and services, and funding and financial model. The result of MA-SHARE case has provided precious experiences of implementing a sustainable HIE for us.
Our study reveals that issues around developing a sustainable business model and financing are the most pressing challenges of HIE [16, 17]. One of the primary reasons that health information exchange sustainability has been such a difficult issue for national and local leaders is that the current reimbursement system, which largely rewards both volume and fragmentation, serves as a disincentive for sharing health information across healthcare stakeholders [1, 8, 12]. To achieve the goal of HIE, we suggest that more sustainable, financing issues, technical and policy standards for the exchange of health
information need further exploration [1, 10].
Although building an interoperable HIE infrastructure in Taiwan remains in its infancy, the issues regarding the role, governance, and sustainability of RHIOs should be addressed in order to develop a sustainable business model [16, 18]. An analytic framework of HIE developed in our study can also be widely used to analyze Taiwan’s RHIO cases. With an understanding of these RHIO’s characteristics, macro-level and micro-level issues of interoperable health information infrastructure, we can develop enabling HIE policies to facilitate the use of EMR in Taiwan.
Acknowledgements
We wish to thank Aziz Boxwala, Ph.D., M.D. (Decision Systems Group, Harvard-MIT Division of Health Science and Technology, Brigham and Women’s Hospital, Harvard Medical School) for helpful discussions. This research is supported by National Cheng Kung University Hospital (Project No. NCKUH-9805010) and Taiwan Merit Scholarship for a postdoctoral fellowship from National Science Council, Taiwan. (Grant No.NSC-095-SAF-I- 564-639-TMS)
References
[1] Halamka, J., Overhage, J. M., Ricciardi, L., Rishel, W., Shirky, C., and Diamond, C., “Exchanging health information: Local distribution, national coordination”, Health Affairs, Vol. 24(5), pp. 1170-1179, 2005. [2] Walker, J., Pan, E., Johnston, D., Adler-Milstein, J.,
Bates, D. W., and Middleton, B., “The value of health information exchange and interoperability”, Health Affairs, pp. W5-10 ~ W5-18, 2005.
[3] Institute of Medicine, Committee on Quality of Health Care in America, “The computer-based patient record: an essential technology for health care”. Washington, D.C.: National Academy Press, 1991.
[4] Yansnoff, W. A., Humphreys, B. L., Overhage, J. M., et al., “Consensus action agenda for achieving the
National Health Information infrastructure”, Journal of American Medical Informatics Association, Vol. 11(4), pp. 332-338, 2004.
[5] Thompson, T. G., & Brailer, D. J., “The decade of health information technology: delivering consumer-centric and information-rich health care”, Department of Health and Human Services, USA., 2004.
[6] Yansnoff, W. A., “Public health informatics and the health information infrastructure”, in E. H. Shortliffe (ed.), Biomedical informatics: computer applications in healthcare and medicine, New York: Springer-Verlag Press, pp. 537-562., 2006.
[7] Science & Technology Advisory Group (STAG), Executive Yuan, Taiwan, “Building a national health information infrastructure”, Strategic Review Board conference proceedings: pp. 21-25, 2003.
[8] Department of Health (DOH), Executive Yuan, Taiwan, “National Health Information Project Proposal”, 2007. [9] Department of Health (DOH), Executive Yuan, Taiwan,
“Intelligent Healthcare Project Proposal”, 2009. [10] Adler-Milstein, J., McAfee, A. P., Bates, D. W., and
Jha, A. K., “The state of regional health information organizations: Current activities and financing”. Health Affairs, pp. w60-w69, 2007.
[11] Halamka, J., Aranow, M. A., Bates, D., et al., “Health c are IT collaboration in Massachusetts: The experience of creating regional connectivity”, Journal of the American Medical Informatics Association, Vol. 12(6), pp. 596-601, 2005.
[12] Thielst, C. B. & Jones, L. E., Guide to establishing a Regional Health Information Organization, Chicago, IL: Healthcare Information and Management Systems Society (HIMSS), 2007.
Health Information Network is really used”, Communications of the ACM, Vol. 42(12), pp. 85-88, 1999.
[14] Leonard, K. J. & Mercer, K., “A framework for information systems evaluation: The case of an integrated community-based health services delivery system”, International Journal of Health Care Quality Assurance, Vol. 13(2), pp. vii-xiv, 2000.
[15] Lorenzi, N. M., “Strategies for creating successful local health information infrastructure initiatives”, U.S. Department of Health and Human Service, 2003, http://aspe.hhs.gov/sp/nhii/LHII-Lorenzi-12.16.03.pd f/. Accessed May 30, 2009.
[16] Foundation of Research and Education of AHIMA (FORE), “Development of State Level Health Information Exchange Initiatives – Final Report”, 2006, http://www.staterhio.org/. Accessed June 10, 2009.
[17] eHealth Initiative (eHI), “Fourth annual survey of health information exchange at the state, regional and
community levels”, 2007, http://www.ehealthinitiative.org/2007HIESurvey/.
Accessed June 10, 2009.
[18] Labkoff, S. E. & Yansnoff, W. A., “A framework for systematic evaluation of health information infrastructure progress in communities”, Journal of Biomedical Informatics, Vol. 40, pp. 100-105, 2007. [19] Halamka, J., Aranow, M., Ascenzo, C., Bates, D. W.,
et al., “E-prescribing collaboration in Massachusetts: Early experiences from regional prescribing projects”, Journal of the American Medical Informatics Association, Vol. 13(3), pp. 239-244, 2006.
[20] Massachusetts Health Data Consortium (MHDC), The consortium of MA-SHARE, 2008, http://www.mahealthdata.org/, accessed June 1, 2009.