Increased risk of Kawasaki disease in children with common allergic diseases Chang-Ching Wei MD a,b, Cheng-Li Lin MS c,d, Chia-Hung Kao MD e,f, Yen-Hsiu Liao MD g, Jeng-Dau Tsai MD h, Yen-Jung Chang PhD c,d, Tsai-Chung Li PhD d
aDepartment of Pediatrics, China Medical University Hospital, Taichung, Taiwan; bCollege of Medicine, China Medical University, Taichung, Taiwan;
cManagement Office for Health Data, China Medical University Hospital, Taichung, Taiwan;
dDepartment of Public Health, China Medical University, Taichung, Taiwan;
eGraduateInstitute of Clinical Medicine Science and School of Medicine, College of Medicine, China Medical University, Taichung, Taiwan;
fDepartment of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan;
gDepartment of Radiology, China Medical University Hospital, Taichung, Taiwan hDepartment of Pediatrics, Chung Shan Medical University Hospital, Taichung, Taiwan;
Address correspondence to:
Yen-Jung Chang, Management Office for Health Data, China Medical University Hospital, Taichung, Taiwan, #2, Yuh-Der Road, Taichung, Taiwan 40402, R.O.C, Tel.: +886-4-2205-2121 ext. 7520,
E-mail: [email protected]; weilonger @gmail.com Short title: Kawasaki disease in allergic diseases
Key words: allergic conjunctivitis, allergic rhinitis, asthma, atopic dermatitis, Kawasaki disease, urticaria
Words: 1772, Table: 4
Funding Source: The study was supported in part by the Bureau of Health
Promotion, Department of Health, R.O.C. (Taiwan) (DOH99-HP-1205), study project grants (DMR-101-061 and DMR-100-076) from China Medical University Hospital our hospital; Taiwan Department of Health Clinical Trial and Research Center and for Excellence (DOH102-TD-B-111-004), Taiwan Department of Health Cancer
Research-Intensive Centers of Excellence in Taiwan (I-RiCE) (NSC101-2911-I-002-303).
Financial Disclosure: The authors have indicated that they have no financial relationships relevant to this article to disclosure
Conflict of Interest: none Contributor’s Statement:
Chang-Ching Wei conceptualized and designed the study, drafted the initial manuscript, and approved the final manuscript as submitted.
Cheng-Li Lin, Chia-Hung Kao, Yen-Hsiu Liao, Jeng-Dau Tsai, Tsai-Chung Li carried out the initial analysis, reviewed and revised the manuscript, and approved the final manuscript as submitted.
Yen-Jung Chang coordinated and supervised data collection, critically reviewed the manuscript, and approved the final manuscript as submitted.
Abstract
Purpose: Growing evidence reveals a link Kawasaki disease (KD) and allergic diseases. This population-based case control study is to investigate the onset of allergic diseases in children and the associated risks of KD.
Methods: From 1996 to 2008, 2748 children with KD and 10,656 randomly selected controls were enrolled. Odds ratios (OR) of KD were calculated for the association with pre-existing allergic diseases.
Results: The children with a single allergic disease had an increased risk of KD, with adjusted odds ratios of having KD of 1.77 for urticaria (95% confidence interval [CI]=1.51-2.08), 1.38 for allergic rhinitis (95% CI=1.18-1.62), and 1.18 for atopic dermatitis (95% CI=1.03-1.34). The adjusted odds ratios increased with the number of concurrent allergic diseases, from 1.55 (95% CI=1.38-1.74) for those with only one allergic disease to 1.62 (95% CI=1.41-1.85) for those with at least two allergic diseases. The children who made two or more medical visits for associated allergic diseases per year had an increased risk of KD.
Conclusions: The children with onset of allergic diseases were at increased risk for KD, and the increased risk was associated with the cumulative effect of concurrent allergic diseases and frequency of seeking medical care.
Abbreviations: Kawasaki disease (KD); allergic conjunctivitis (AC); allergic rhinitis (AR); asthma, atopic dermatitis (AD); T helper type 1 cells (Th1); T helper type 2 cells (Th2)
Introduction
Kawasaki disease (KD) is a systemic vasculitis which mainly affects infants and young children [1]. Although KD is an acute illness in most patients, coronary artery aneurysms develop in about 25% of patients without prompt diagnosis and treatment, and this is a leading cause of acquired heart disease in children [2]. The incidence of KD has increased globally in recent years [3]. Asian populations have a much higher incidence of KD, and Taiwan has the third highest incidence of KD worldwide [4]. In Japan, the incidence of KD has doubled during the past two decades [5]. Even though KD has been identified for more than 40 years, the etiology remains unclear.
There is a growing interest in a potential link between atopic disorders and autoimmune diseases, and there is increasing epidemiological evidence for an
association of KD and allergic disease [6-12]. However, the relationship between pre-existing allergic diseases and KD risk remains unclear. In this nationwide, population-based case-control study, we investigated temporal interactions and relationships between subsequent KD risk and the onset of allergic diseases in children to better understand the pathogenesis of these diseases.
Methods
Data source
The National Health Insurance (NHI) program in Taiwan was implemented in 1995, and is a single-payer, social insurance plan [13]. The Bureau of NHI (BNHI) has contracts with 99% of hospitals and the NHI program covers up to 99% of the population of Taiwan. The NHI program also provides datasets from the National Health Research Insurance Database (NHIRD) for corresponding research on issues related to cost, quality of health services, medical practice patterns, accessibility to healthcare programs and treatment outcomes at national and local levels
(http://www.nhi.gov.tw/english/index.aspx) [13,14]. The dataset used in this study consisted of a randomly selected sample of half of all insured children in Taiwan, which included more study subjects than previous studies using the claims data of the Longitudinal Health Insurance Database (LHID) which includes one million
randomly selected individuals [10-12]. This study was exempt from institutional review board approval because the NHIRD database contains de-identified encrypted information which is publicly available through the proper application process. Study design
The claim data retrospectively collected since 1996 and prospectively recorded up to 2008, contained demographic information on insured children (including sex, birth
date, and residential area) and medical care received for ambulatory and inpatient visits. The diagnosis of KD was confirmed by the International Classification of Diseases, 9th Revision of the Clinical Modification (ICD-9-CM) code, and the Registry for Catastrophic Illness Patient Database (RCIPD), which includes selected major injuries or illnesses and is published by the Department of Health, Executive Yuan, Taiwan. To register as having KD, the diagnosis must be made by a board-certified specialist, and the application is further reviewed and approved by the BNHI, which ensures the accuracy and reliability of the diagnosis.
We identified a total of 2748 patients aged 1 to 18 years with newly diagnosed KD (ICD-9-CM code 446.1) from 1998 to 2008 as the KD group. For each KD patient, 4 controls with no history of KD were matched by age (every 1-year span), sex, and urbanization level. Urbanization level was defined according to a NHRI report. City districts and townships where subjects were registered for insurance purposes were grouped in to four levels of urbanization based on population density (people/km2).
Level 1 indicates the most urbanized area and level 4 indicates the least urbanized area. We identified the subjects who were diagnosed with allergic conjunctivitis (AC) (ICD-9 codes: 372.05, 372.10, and 372.14), allergic rhinitis (AR) (ICD-9 code: 477), asthma (ICD-9 codes: 493 and 494), atopic dermatitis (AD) (ICD-9 code: 691), and urticaria (ICD-9 codes: 708.0 and 708.9) before the diagnosis of KD. All diagnoses of
the allergic disorders were given at least twice by physicians for diagnostic validity. The cumulative effect of disease severity was evaluated by the number of allergic comorbidities and frequency of seeking medical care.
Statistical analysis
We used the chi-square and t-tests to analyze the demographic data between the KD and non-KD control groups, and multivariate logistic regression models to calculate the odds ratios (OR) and 95% confidence intervals (CI) after adjusting for sex, gender and urbanization of residential area for the association between allergic diseases and KD. All data analyses were performed using SAS 9.1 (SAS Institute Inc., Carey, NC), and a p value less than 0.05 was considered to be statistically significant.
Results
In total 2748 subjects with KD were identified, including 1744 males (63.5%) and 1004 females (36.5%). The mean age at the diagnosis of KD was 2.83 (SD, 2.80) years. More than half of the subjects with KD resided in urban areas (approximately 57%) and were younger than 2 years (67.3%). The prevalence of all atopic diseases was significantly higher in the KD group compared to the non-KD group, with AC (6.62% vs. 4.95%), AR (12.0% vs. 7.96%), asthma (7.61% vs. 6.45%), AD (14.7% vs. 11.2%), and urticaria (9.75% vs. 5.19%), respectively (Table 1).
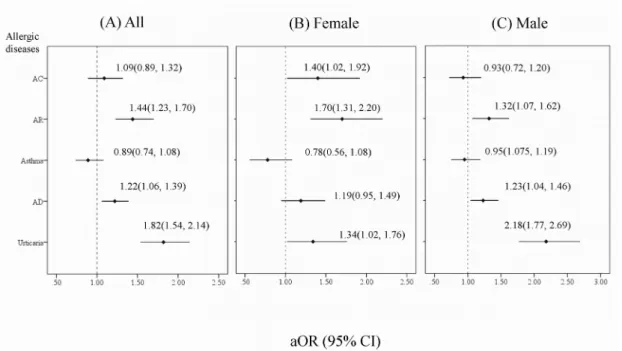
In the whole study population, an increased subsequent risk of KD was observed in the children with each allergic disease except for asthma (Figure 1). The mean
duration between diagnosis of allergic diseases and KD is 21.7 months (median=15.1; IQR=5.07-31.0). The adjusted ORs (aOR) were 1.77 for urticaria (95% CI, 1.51-2.08), 1.38 for AR (95% CI, 1.18-1.62), and 1.18 for AD (95% CI, 1.03-1.34). When the association was evaluated by gender, the adjusted risk for both genders was significantly related to AR and urticaria (Figure 1). The aOR increased with the number of allergic diseases, from 1.55 (95% CI, 1.38-1.74) for those with only one allergic disease to 1.62 (95% CI, 1.41-1.85) for those with at least two allergic diseases (p-value for trend <0.0001) (Table 2) in multivariate logistic regression. The
adjusted ORs of KD increased to 1.68 (95% CI, 1.41-1.84), 1.34 (95% CI, 1.38-2.03), 2.15 (95% CI, 1.54-3.02) and 2.46 (95% CI, 1.04-5.81) in each age group (≤2, 2-5, 5-12, and >12 years) for those with two or more allergic diseases (Table 2). Comparing the allergic patients with those without any allergic diseases, the adjusted OR of having KD increased with the number of allergic comorbidities. Among the children aged 12 or more, those with at least two allergic comorbidities had a 2.48-fold higher risk of KD than those without any allergic diseases (95% CI=1.03-5.94) (Table 2). We further examined the association between the annual frequency of medical visits due to allergic diseases and the risk of KD, and found that the aORs increased in AR, AD and urticaria with two or more medical visits per year (1.45 (95% CI, 1.21-1.74); 1.52 (95% CI, 1.27-1.83); and 2.92 (95% CI, 2.33-3.66), respectively) (Table 3).
Discussion
There are a number of strengths to this study. First, it robustly demonstrates the relationship between atopic diathesis and risk of KD using a large number of study subjects. Second, we analyzed the effect not only of a specific type of allergic disease but a large number of common allergic diseases, the cumulative effect of comorbid allergic diseases, and the frequency of seeking medical care. Third, the current study is a population-based study with physician-diagnosed atopic diseases which
minimizes selection and recall bias. Fourth, the diagnosis of KD was determined by both ICD-9-CM and RCIPD thereby ensuring internal validity. Fifth, we adjusted for possible confounding factors including age, gender and urbanization level. Ethic influence was not considered in this study because of homogenous ethnicity in Taiwan.
A few studies have reported a high prevalence of allergic diseases in patients with KD, however these findings have been inconsistent due to the limited number of patients and because most of the studies only investigated one or two diseases such as AD, AR and asthma [6-9]. More recently, several population-based studies in Taiwan enhanced the understanding of the interaction between KD and allergy. One cohort study revealed that KD was a risk factor for the subsequent development of asthma
and AR [10].Another two studies revealed an association between KD and the risk of AD [11,12]. However, there are several limitations to these studies. First, they used claims data of a sample of one million subjects from the NHIRD, which limited the number of study subjects resulting in a loss of statistical significance for some atopic diseases. Second, no previous study has included large scale of allergic diseases as the current study. Third, the relationship between allergy and KD risk has not been discussed. Only one recent study using a large population investigated the association between KD and large scale of allergic disease [15]. However, the KD risk after the onset of allergic diseases has not been elucidated. This study is the first to report that the children with pre-existing allergic diseases had an increased future risk of KD, and that this risk increased with the number of concurrent allergic diseases and associated medical care visits.
Our findings may suggest that atopic diseases have a positive influence on the
development of KD, or that they may share common early life determinants. Sstudies have shown that KD is associated with immune dysregulation involving not only Th1/Th2 but also Th17 cells/ regulatory T cell imbalance [16-18]. This immune dysregulation may therefore explain the temporal interaction between KD and allergic diseases. In addition, autoimmune and allergic diseases may share genetic
Therefore, immunogenetic factors and early-life environmental factors may both contribute to the development of allergies and KD.
There are several limitations to this study. This is a cross-sectional study and the causality between allergic diseases and KD could not be established. However, this study clearly shows an association between allergy and the risk of KD by using a large number of subjects. Another limitation is the lack of data on genetic and environmental factors which might have affected the risks for KD and atopic diathesis.
Conclusions
Current study indicates the temporal relationship between the allergic diseases and the subsequent development of Kawasaki disease. In addition, the risk of KD was consistently associated with the number and severity of comorbid allergic diseases. Future investigations on environmental and genetic factors related to the childhood onset of allergies and subsequent risk of KD are warranted.
Acknowledgements
The study was supported in part by the study projects (DMR-101-061 and DMR-100-076) in China Medical University Hospital; Taiwan Department of Health Clinical Trial and Research Center and for Excellence (DOH102-TD-B-111-004), Taiwan Department of Health Cancer Research Center for Excellence (DOH102-TD-C-111-005); and International Research-Intensive Centers of Excellence in Taiwan (I-RiCE) (NSC101-2911-I-002-303).
References
[1] Yim D, Curtis N, Cheung M, Burgner D. Update on Kawasaki disease:
Epidemiology, aetiology and pathogenesis. J Paediatr Child Health 2013; 49: 704-8.
[2] Uehara R, Belay ED. Epidemiology of Kawasaki disease in Asia, Europe, and the United States. J Epidemiol2012; 22: 79-85.
[3] Hahn Y, Kim Y, Jo S, Han H. Reduced frequencies of peripheral interferon-gamma-producing CD4+ and CD4- cells during acute Kawasaki disease. Int Arch Allergy Immunol 2000; 122: 293-8.
[4] Huang WC, Huang LM, Chang IS, Chang LY, Chiang BL, Chen PJ, et al. Epidemiologic features of Kawasaki disease in Taiwan, 2003-2006. Pediatrics 2009; 123: e401-5.
[5] Hirao J, Hibi S, Andoh T, Ichimura T. High levels of circulating interleukin-4 and interleukin-10 in Kawasaki disease. Int Arch Allergy Immunol 1997; 112: 152-6. [6] Brosius CL, Newburger JW, Burns JC, Hojnowski-Diaz P, Zierler S, Leung DY.
Increased prevalence of atopic dermatitis in Kawasaki disease. Pediatric infect Dis J 1988; 7: 863-6.
[7] Matsuoka S, Tatara K, Nakagawa R, Mori K, Kuroda Y. Tendency toward atopy in Kawasaki disease. Eur J Pediatr 1997; 156: 30-2.
[8] Liew WK, Lim CW, Tan TH, Wong KY, Tai BC, Quek SC, et al. The effect of Kawasaki disease on childhood allergies - a sibling control study. Pediatr allergy and Immunol2011; 22: 488-93.
[9] Webster RJ, Carter KW, Warrington NM, Loh AM, Zaloumis S, Kuijpers TW, et al. Hospitalisation with Infection, Asthma and Allergy in Kawasaki Disease Patients and Their Families:Genealogical Analysis Using Linked Population Data. Plos One 2011; 6: e28004.
[10] Kuo HC, Chang WC, Yang KD, Yu HR, Wang CL, Ho SC, et al. Kawasaki disease and subsequent risk of allergic diseases: a population-based matched cohort study. BMC pediatrics 2013; 13: 38.
[11] Peng YW, Wei CC, Liang CC, Hsu CH, Klahan S, Huang YH, et al. Increased Risk of Atopic Dermatitis in Preschool Children with Kawasaki Disease: A Population-Based Study in Taiwan.Evid Based Complement Alternat Med2013; 10: 1-7.
[12] Hwang CY, Hwang YY, Chen YJ, Chen CC, Lin MW, Chen TJ, et al. Atopic diathesis in patients with kawasaki disease. J Pediatr 2013; 163: 811-5.
[13] Davis K, Huang AT. Learning from Taiwan: experience with universal health insurance. Ann intern Med2008; 148: 313-4.
nephrotic syndrome during hospitalizations. Nephrology 2012; 178: 681-688. [15] Tsai YJ, Lin CH, Fu LS, Fu YC, Lin MC, Jan SL. The association between
Kawasaki disease and allergic diseases, from infancy to school age. Allergy and Asthma Proceedings. 2013; 5: 467-72.
[16]Jason J, Gregg L, Han A, Hu A, Inge KL, Eick A, et al. Immunoregulatory changes in Kawasaki disease. Clin Immunol Immunopathol1997; 84: 296-306. [17] Afzali B, Mitchell P, Lechler RI, John S, Lombardi G. Translational mini-review
series on Th17 cells: induction of interleukin-17 production by regulatory T cells. Clin Exp immunol 2010; 159: 120-30.
[18] Furuno K, Yuge T, Kusuhara K, Takada H, Nishio H, Khajoee V, et al. CD25(+) CD4(+) regulatory T cells in patients with Kawasaki disease. J Pediatr 2004; 145: 385-90.
[19] Simpson CR, Anderson WJ, Helms PJ, Taylor MW, Watson L, Prescott GJ, et al. Coincidence of immune-mediated diseases driven by Th1 and Th2 subsets
suggests a common aetiology. A population-based study using computerized general practice data. Clin Exp Allergy 2002; 32: 37-42.
[20] Kim JJ, Hong YM, Sohn S, Jang GY, Ha KS, Yun SW, et al. A genome-wide association analysis reveals 1p31 and 2p13.3 as susceptibility loci for Kawasaki disease. Hum Genet 2011; 129: 487–95.
[21] Burgner D, Davila S, Breunis WB, Ng SB, Li Y, Bonnard C, et al. A genome-wide association study identifies novel and functionally related susceptibility loci for Kawasaki disease. PLoS Genet 2009; 5: e1000319 .
[22] Tsai FJ, Lee YC, Chang JS, Huang LM, Huang FY, Chiu NC, et al. Identification of novel susceptibility loci for Kawasaki disease in a Han Chinese population by a genome-wide association study. PLoS ONE 2011; 6: e16853.
[23]Liao WL, Tsai FJ. Personalized medicine: A paradigm shift in healthcare. BioMedicine 2013; 3: 66-72.
Table 1
Comparisons in socio-demographic factors and co-morbidities between cases with Kawasaki disease (KD) and non-KD controls
Total (n=13404) Control (n=10656) KD (n=2748) P value
n (%) n (%) n (%) Age (years), mean ± SD* 2.83±2.8 2.82±2.8 2.83±2.8 0.87* Age (years) 0.99 ≤ 2 9038 (67) 7188 (68) 1850 (67) 2-5 2960 (22) 2352 (22) 608 (22) 5-12 1174 (9) 932 (9) 242 (9) > 12 232 (1) 184 (2) 48 (2) Gender 0.93 Female 4888 (37) 3884 (37) 1044 (37) Male 8516 (64) 6772 (64) 1744 (64) Urban status† 0.99 Level 1 3940 (30) 3132 (30) 808 (30) Level 2 3718 (28) 2952 (28) 766 (28) Level 3 2669 (20) 2124 (20) 545 (20) Level 4 2927 (22) 2328 (22) 599 (22) Co-morbidity AC 0.0005 No 12,695 (95) 10,129 (95) 2566 (93) Yes 709 (5) 527 (5) 182 (7) AR <0.0001 No 12,227 (91) 9808 (92) 2419 (88) Yes 1177 (9) 848 (8) 329 (12) Asthma 0.03 No 12,508 (91) 9969 (94) 2539 (92) Yes 896 (7) 687 (6) 209 (8) AD <0.0001 No 11,805 (88) 9462 (84) 2343 (85) Yes 1599 (12) 1194 (11) 405 (15) Urticaria <0.0001 No 12,583 (88) 10,103 (85) 2480 (90) Yes 821 (6) 553 (5) 268 (10)
Abbreviations: Kawasaki disease (KD), allergic conjunctivitis (AC), allergic rhinitis (AR), atopic dermatitis (AD)
Chi-square test, *t-test
†The urbanization level was categorized by the population density of the residential area into 4 levels, with level 1 as the most urbanized and level 4 as the least urbanized.
Figure 1 †Odds ratio and 95% confidence interval between specific allergic disease and subsequent risk of Kawasaki disease
Abbreviations: allergic conjunctivitis (AC); allergic rhinitis (AR); atopic dermatitis (AD)
†Estimates from multiple conditional logistic regression models adjusted for sex, age, urbanization, and mutual five allergic diseases
Table 3
†Association between frequency of annual medical visit due to allergic disease and Kawasaki disease
Frequency None ≤ 2 > 2
aOR (95% CI) aOR (95% CI) aOR (95% CI) p for trend
Allergic diseases AC 1.00 (Reference) 1.09 (0.86, 1.38) 1.08 (0.79, 1.47) 0.46 AR 1.00 (Reference) 1.27 (0.97, 1.65) 1.53 (1.27,1.83)*** 0.22 Asthma 1.00 (Reference) 0.82 (0.62, 1.10) 0.94 (0.75, 1.17) 0.46 AD 1.00 (Reference) 0.99 (0.83, 1.18) 1.57 (1.30, 1.89)*** 0.0002 Urticaria 1.00 (Reference) 1.14 (0.90, 1.44) 3.05 (2.43, 3.83)*** <0.0001
Abbreviations: Kawasaki disease (KD); allergic conjunctivitis (AC); allergic rhinitis (AR); atopic dermatitis (AD); adjusted odds ratio (aOR); confidence interval (CI)
†Estimates from multiple conditional logistic regression models adjusted for sex, age, urbanization, and mutual five allergic diseases
* p<0.001 Table 2
†Association between the number of allergic diseases and Kawasaki disease
Age(yrs) All ≤ 2 2-5 5-12 >12
aOR (95% CI) aOR (95% CI) aOR (95% CI) aOR (95% CI) aOR (95% CI)
Number of concurrent allergic disease
0 1.00 (Reference) 1.00 (Reference) 1.00 (Reference) 1.00 (Reference) 1.00 (Reference)
1 1.61 (1.43, 1.82)*** 1.71 (1.48, 1.97)** 1.37 (1.06, 1.77)* 1.57 (1.01, 3.36)* 1.15 (0.41, 3.23)
2+ 1.71 (1.48, 1.98)*** 1.79 (1.45, 2.20)** 1.36 (1.06, 1.75)* 2.30 (1.57, 3.26)*** 2.19 (0.80, 6.02)
p for trend <0.0001 <0.0001 0.0085 <0.0001 0.057
Abbreviations: adjusted odds ratio (aOR); confidence interval (CI)
†Estimates from multiple conditional logistic regression models adjusted for sex, age, urbanization, and mutual five allergic diseases * p<0.05, ** p<0.001