P
Puurrppoossee:: To evaluate the potential effect of a clinically relevant con-centration of propofol (PPF) on cell viability and nitric oxide-induced macrophage apoptosis.
M
Meetthhooddss:: Mouse macrophages (cell line Raw 264.7) were cul-tured and incubated with a nitric oxide donor sodium nitroprusside (SNP), PPF, and a combination of PPF and SNP for one, six and 24 hr. Cell viability was determined by the colorimetric 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide assay. Apoptotic cells were determined by analyzing the percentages of sub-G1 phase in macrophages. The amounts of nitric oxide were assayed.
R
Reessuullttss:: The amounts of nitric oxide in macrophages were increased with time when incubated with SNP (P < 0.05). Simultaneously, SNP caused cell death of macrophages in a concen-tration-and time-dependent manner (P < 0.05). PPF per se did not alter the amount of basal and SNP-provided nitric oxide in macrophages. A therapeutic concentration of PPF (30 µM) exhibited no cytotoxicity. After incubation with SNP for one and six hours, PPF could completely or partially block nitric oxide-induced cell death, respectively (P < 0.05).
Administration of SNP to macrophages resulted in a time-depen-dent pattern of increase of apoptotic cells (P < 0.05). Similar to the results of the cell viability analyses, PPF was able to protect macrophages from nitric oxide-induced apoptosis in one and six hour-treated groups (P < 0.05) but not in the 24 hr treated group. C
Coonncclluussiioonn:: PPF, at a therapeutic concentration, can protect mouse macrophages in vitro from nitric oxide-induced cell apopto-sis as well as cell death.
Objectif : Évaluer l’effet potentiel d’une concentration thérapeutique de propofol (PPF) sur la viabilité cellulaire et l’apoptose des macrophages induite par l’oxyde nitrique.
Méthode : Des macrophages de souris (souche cellulaire 264,7) ont été mis en culture et incubés avec un donneur d’oxyde nitrique, le nitroprussiate de sodium (NPS), du PPF et une combinaison de PPF et de NPS pendant une, six et 24 h. La viabilité cellulaire a été déter-minée par une analyse colorimétrique du bromure 3-(4,5-diméthylth-iazol-2-yl)-2,5-diphényltétrazolium. Les cellules apoptotiques ont été déterminées en analysant les pourcentages de phase sous-G1 dans les macrophages. Les quantités d’oxyde nitrique ont été analysées. Résultats : La quantité d’oxyde nitrique dans les macrophages a aug-menté avec le temps dans le cas de l’incubation avec le NPS (P < 0,05). Simultanément, le NPS a causé la mort cellulaire des macrophages en fonction du temps et de la concentration (P < 0,05). Le PPF par lui-même n’a pas modifié la quantité d’oxyde nitrique de base ou fournie par le NPS dans les macrophages. Une concentration thérapeutique de PPF (30 µM) n’a revélé aucune toxicité. Après l’incu-bation avec le NPS pendant une et six heures, le PPF a pu arrêter com-plètement ou partiellement la mort cellulaire induite par l’oxyde nitrique, respectivement (P < 0,05).
L’administration de NPS aux macrophages a entraîné l’augmentation du nombre de cellules apoptotiques selon un modèle dépendant du temps (P < 0,05). Le PPF a pu protéger les macrophages de l’apoptose induite par l’oxyde nitrique dans les groupes traités pendant une et six heures (P < 0,05) mais non dans le groupe de 24 h.
Conclusion : Le PPF en concentration thérapeutique peut protéger les macrophages de souris in vitro de l’apoptose cellulaire aussi bien que de la mort cellulaire induites par l’oxyde nitrique.
GENERAL ANESTHESIA 477
CAN J ANESTH 2002 / 49: 5 / pp 477–480
Therapeutic concentrations of propofol protects
mouse macrophages from nitric oxide-induced cell
death and apoptosis
[Des concentrations thérapeutiques de propofol protègent les macrophages de souris
de la mort cellulaire et de l’apoptose induites par l’oxyde nitrique]
Hang Chang MD PhD,* Shih-Ying Tsai MS,† Yi Chang MD,* Ta-Liang Chen MD PhD,‡ Ruei-Ming Chen PhD‡
From the Departments of Education and Research,* Shin-Kong Wu Ho-Su Memorial Hospital; Surgery and Anesthesiology,* College of Medicine; Physiology and Graduate Institute of Medical Science,† College of Medicine; and Anesthesiology,‡ Wan-Fang Hospital, College of Medicine, Taipei Medical University, Taipei, Taiwan.
Address correspondence to: Dr. Ruei-Ming Chen, Department of Anesthesiology, Wan-Fang Hospital, College of Medicine, Taipei
Medical University, No. 111, Sec. 3, Hsing-Lung Rd., Taipei, 116, Taiwan. Phone: 886-2-29307930, ext. 2159; Fax: 886-2-86621150; E-mail: [email protected]
Accepted for publication December 7, 2001. Revision accepted February 6, 2002.
ROPOFOL (PPF; 2,6-diisopropylphenol) has been used worldwide in a variety of sur-gical procedures for induction and mainte-nance of anesthesia.1 Being similar to the
phenol-containing α-tocopherol and butylated hydroxytoluene in structure, PPF has been reported to possess an antioxidant effect.2 Studies in human
alveolar macrophages have shown that PPF has poten-tial effects on the suppression of immune responses.3
Nitric oxide has been regarded as an important medi-ator of non-specific cell-mediated immunity when macrophages release the radical to kill infected pathogens.4The massive induction of nitric oxide can
cause macrophages and neighbouring cells to undergo apoptosis.4,5The present study was designed to
inves-tigate the protective role of a clinically relevant con-centration of PPF on nitric oxide-induced macrophage insults.
M
Maatteerriiaallss aanndd mmeetthhooddss
Macrophage Raw 264.7 cells were maintained in Roswell Park Memorial Institute 1640 medium (Gibco, BRL, Grand Island, NY, USA) supplemented with 10% fetal calf serum, L-glutamine, penicillin (100 IU·mL–1), and streptomycin (100 µg·mL–1) in 75 cm2
flasks at 37C in a humidified atmosphere of 5% CO2. PPF was donated by Zeneca Limited (Macclesfield, Cheshire, UK). Clinically, plasma levels of PPF range between 10 and 50 µM6and our preliminary analyses
for macrophage viability revealed that PPF at 300 µM would cause cell death. Therefore, PPF was adminis-tered in a concentration of 30 µM in the present study. Cell viability was analyzed following the 3-(4, 5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bro-mide assay.7 Measure of apoptosis was carried out
according to the method of Nicoletti et al.8 The
amounts of nitrite, an oxidated product of nitric oxide, were determined as described in the technical bulletin of Promega Griess Reagent System (Promega Corporation, Madeson, WI, USA).
The statistical difference between groups was con-sidered significant when the P value of the Duncan’s multiple- range test was less than 0.05. Statistical analysis between groups over time was carried out by two way ANOVA.
R Reessuullttss
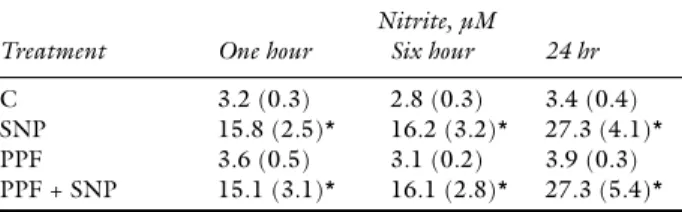
Exposure of macrophages to 2 mM sodium nitroprus-side (SNP) resulted in a time-dependent increase in nitrite (P < 0.05, n = 12; Table I). PPF at the thera-peutic concentration of 30 µM did not affect the basal and SNP- induced amounts of nitric oxide in macrophages. Treatment with SNP was associated
with concentration- and time-dependent decreases in macrophage viability (P < 0.05, n = 12; Table II). PPF was not cytotoxic for macrophages (Figure 1). Exposure of macrophages to a combination of PPF and SNP for one and six hours prevented cell death completely and partially, respectively (P < 0.05, n = 9). In the 24-hr treated group, PPF provided no protec-tion against cell death secondary to SNP.
Treatment of macrophages with SNP was associat-ed with a time-dependent increase in cell apoptosis (P < 0.05, n = 9; Figure 2). PPF at 30 µM did not affect apoptosis. PPF completely and partially blocked SNP-induced macrophage apoptosis in the one-hour and six-hour treated groups, respectively. In the 24-hr treated group, PPF showed no protection of macrophages from nitric oxide-induced cell apoptosis. D
Diissccuussssiioonn
Macrophages play a crucial role in the cellular defense of surgical patients suffering from infection by provid-ing reactive oxygen species to attack and decompose the invading microorganisms (and tumour cells as well).4Nitric oxide can either be the mediator of
non-specific cellular immunity or the cause of autoimmune
478 CANADIAN JOURNAL OF ANESTHESIA
P
TABLE I The amount of nitrite in macrophages exposed to sodium nitroprusside, propofol and a combination of propofol and sodium nitroprusside.Nitrite, µM
Treatment One hour Six hour 24 hr
C 3.2 (0.3) 2.8 (0.3) 3.4 (0.4) SNP 15.8 (2.5)* 16.2 (3.2)* 27.3 (4.1)* PPF 3.6 (0.5) 3.1 (0.2) 3.9 (0.3) PPF + SNP 15.1 (3.1)* 16.1 (2.8)* 27.3 (5.4)* Data is expressed as mean (SEM) for n = 12. *Values significantly different from the respective control, P < 0.05; C = control; SNP = sodium nitroprusside; PPF = propofol.
TABLE II Concentration-and time-dependent effects of sodium nitroprusside on macrophage viability.
Cell viability, optical density at 570 nm
SNP, mM One hour Six hour 24hr
0 0.84 (0.06) 0.81 (0.04) 1.08 (0.09) 0.5 0.79 (0.05) 0.73 (0.03)* 0.56 (0.06)* 1.0 0.81 (0.08) 0.67 (0.05)* 0.27 (0.03)* 1.5 0.74 (0.04)* 0.64 (0.04)* 0.04 (0)* 2.0 0.71 (0.05)* 0.56 (0.03)* 0.04 (0)* Macrophages were treated with 0, 0.5, 1.0, 1.5 and 2 mM SNP for one, six and 24 hr. Cell viability was determined by the 2,5-diphenyltetrazolium bromide assay. Data is expressed as mean (SEM) for n = 12. *Values significantly differ from the respective control; P < 0.05; SNP = sodium nitroprusside.
injury during inflammation.5 After treatment with
SNP, the amount of nitrite, an oxidative product of nitric oxide, is significantly augmented, meaning that the oxidative stress in macrophages is activated (Table I). Treatment with SNP causes concentration-and time-dependent decreases of macrophage viability (Table II). The present results are compatible with previous studies which showed that nitric oxide at
high concentrations would be cytotoxic to macrophages.
Surgery is frequent in intensive care unit patients suf-fering from sepsis and PPF is one of the widely used iv anesthetic agents for these patients. Structurally, this anesthetic has a potent antioxidant effect on hydrogen peroxide, hydroxyl radical and superoxide induced tis-sue or cell injury.2In the present study, a clinically
rele-Chang et al.: PROPOFOL AND APOPTOSIS 479
FIGURE 1 Protective effect of propofol (PPF) on sodium nitro-prusside (SNP)-induced macrophage death. Macrophages were treated with SNP, PPF and a combination of PPF and SNP for one, six and 24 hr. Cell viability was determined by the 2,5-diphenyltetrazolium bromide assay. Data is expressed as mean ± SEM for n = 9. * Values significantly differ from the respective control, P < 0.05. † Values significantly differ between SNP and the combination of PPF and SNP, P < 0.05.
FIGURE 2 Protective effect of propofol (PPF) on sodium nitro-prusside (SNP)-induced macrophage apoptosis. Macrophages were treated with SNP, PPF and a combination of PPF and SNP for one, six and 24 hr. Apoptotic cell was determined by flow cytome-try. Data is expressed as mean ± SEM for n = 9. * Values signifi-cantly differ from the respective control when P < 0.05. † Values significantly differ between SNP and the combination of PPF and SNP, P < 0.05.
vant concentration of PPF (30 µM) could block nitric oxide-induced cell death.6This concentration of PPF is
not cytotoxic to macrophages (Figure 1). When SNP is combined with PPF, this anesthetic agent protects macrophages from nitric oxide-induced cell apoptosis (Figures 1, 2). Thus, our data suggest that PPF is able to prevent nitric oxide-induced cell death.
The protective role of PPF on nitric oxide-induced macrophage death appears to decrease with time. In the one- hour treated group, PPF completely protect-ed macrophages from nitric oxide-inducprotect-ed cell death, but the effect decreased rapidly at six hours and 24 hr (Figures 1, 2). The major explanation for the time-dependent decrease of the protective effect of PPF might be that PPF progressively decomposes after exposure to visible light and in aerobic conditions.1
Metabolism of PPF by cytochrome P450-dependent monooxygenases to 2,6-diisopropyl-1,4-quinol or uri-dine diphosphate glucuronosyltransfease-mediated glucuronidation to glucuronide complex may be another reason explaining the decreasing protective effect of the iv anesthetic agent.9
The present study directly assayed the amount of nitrite corresponding to nitric oxide production in macrophages. Our data shows that PPF does not influence nitric oxide production in untreated and in SNP-treated cells (Table I). In a human leukocyte chemiluminescence study, Demiryurek et al. reported that PPF possesses a direct scavenging effect on hydroxyl chloride, superoxide, hydrogen peroxide and hydroxyl radical.10Our data suggest that PPF has no
such effects on the direct scavenging of nitric oxide. Therefore, the protective mechanism of PPF against nitric oxide-mediated cellular damage may be through other signal transduction pathways rather than direct scavenging of nitric oxide.
In conclusion, this study has demonstrated that a therapeutic concentration of PPF could protect mouse macrophage Raw 264.7 cells from nitric oxide-induced cell insults, as measured by cell viability and apoptosis. Our results also suggest that PPF exhibited cellular protection through a mechanism other than the direct scavenging of nitric oxide.
A
Acckknnoowwlleeddggeemmeennttss
This study is supported by grants NSC89-2314-B-038-038 (R.-M. Chen) and NSC89-2314-038-067 (T.-L. Chen) from the National Science Council, Taiwan, ROC.
R
Reeffeerreenncceess
1 Sebel PS, Lowdon JD. Propofol: a new intravenous anes-thetic. Anesthesiology 1989; 71: 260–77.
2 Murphy PG, Myers DS, Davies MJ, Webster NR, Jones JG. The antioxidant potential of propofol (2,6- diiso-propylphenol). Br J Anaesth 1992; 68: 613–8.
3 Kotani N, Hashimoto H, Sessler DI, et al. Intraoperative modulation of alveolar macrophage function during isoflurane and propofol anesthesia. Anesthesiology 1998; 89: 1125–32.
4 Nathan C. Nitric oxide as a secretory product of mam-malian cells. FASEB J 1992; 6: 3051–64.
5 Marshall JC. Inflammation, coagulopathy, and the pathogenesis of multiple organ dysfunction syndrome. Crit Care Med 2001; 29(Suppl.): S99–106.
6 Gepts E, Camu F, Cockshott ID, Douglas EJ. Disposition of propofol administered as constant rate intravenous infusions in humans. Anesth Analg 1987; 66: 1256–63.
7 Carmichael J, DeGraff WG, Gazdar AF, Minna JD, Mitchell JB. Evaluation of a tetrazolium-based semiau-tomated colorimetric assay: assessment of chemosensi-tivity testing. Cancer Res 1987; 47: 936–42.
8 Nicoletti I, Migliorati G, Pagliacci MC, Grignani F, Riccardi C. A rapid and simple method for measuring thymocyte apoptosis by propidium iodide staining and flow cytometry. J Immunol Methods 1991; 139: 271–9.
9 Simons PJ, Cockshott ID, Douglas EJ, Gordon EA, Hopkins K, Rowland M. Disposition in male volunteers of a subanaesthetic intravenous dose of an oil in water emulsion of 14C-propofol. Xenobiotica 1988; 18: 429–40.
10 Demiryürek AT, Cinel I, Kahraman S, et al. Propofol and intralipid interact with reactive oxygen species: a chemiluminescence study. Br J Anaesth 1998; 80: 649–54.