Abstract.
This study was conducted in order to assess the
safety and tolerability of Agaricus blazei Murrill (ABM) in
general toxicological studies by Ames tests in vitro and in
28-day feeding toxicity experiments. There were no
dose-dependent increases or decreases in the number of revertant
colonies both with and without metabolic activation in Ames
tests. Doses of 10, 5 and 0.1 mg/per mouse of ABM daily were
administered by oral gavage to mice (n=10) for 28 days. The
effects on clinical observations, clinical pathology, and
histopathology were evaluated. There were no significant
changes in the brain, heart, kidney, liver, spleen, adrenal gland,
testes or ovaries visually. With increasing doses, male and
female treated mice did not show any gradual elevation of
serum concentration in any of the nine items we examined,
except for aspartate aminotransferase (AST) and alanine
aminotransferase (ALT) in females. The AST levels of the
treatment by medium or high dose and the ALT levels of the
treatment by high dose in females were abnormal in
comparison to those of the baseline control group, with
significant differences. On studying the histological changes in
mice, tissue sections of negative control and experimental
groups exhibited no apparent pathological alterations. In
summary, the Ames test, pathology determinations, biochemical
analysis and routine blood parameters were all normal, except
for AST and ALT in females. Results showed that the statistical
differences observed in one sex were not observed in the other
and were not dose dependent.
In recent years, the use of complementary and alternative
medicine (CAM) has become increasingly popular among
cancer patients in Western countries, with a prevalence as
high as 80% (1, 2). Traditional Chinese medicine (TCM),
and herbal medicines in particular, have been used in the
treatment of cancer for thousands of years in China, Japan,
and other Asian countries (3-5). These medicines are widely
accepted as current forms of CAM for cancer treatment in
the United States and Europe (6, 7). As recent pre-clinical
and clinical studies have shown, TCM combined with
conventional Western medicine (chemotherapy and
radiotherapy) can provide effective supportive care for cancer
*These Authors contributed equally to this work.
Correspondence to: Dr. Jing-Gung Chung, Department of Biological Science and Technology, China Medical University, No. 91, Hsueh-Shih Rd., Taichung 40402, Taiwan, R.O.C. Tel: +886 422053366 ext. 2161, Fax: +886 422053764, e-mail: [email protected] and Dr. Ming-Fang Wu, Animal Medicine Center, College of Medicine, National Taiwan University, 10F., No.2, Syu-Jhou Road, Taipei 10055, Taiwan, R.O.C. Tel: +886 223123456 ext. 88160, Fax: +886 223911306, e-mail: [email protected]
Key Words: Agaricus blazei Murill, genotoxicity, subclinical toxicity, Ames test, histopathology, serum biomarker analysis, ALT, AST.
Evaluation of Genotoxicity and Subclinical Toxicity of
Agaricus blazei Murrill in the Ames Test and in
Histopathological and Biochemical Analysis
JIN-BIOU CHANG
1,2*, HSU-FENG LU
3,4*, NIEN-CHIEH LIAO
4, CHING-SUNG LEE
3,
MING-YANG YEH
5, CHI-MING LIU
6, MING-TENG CHUNG
7, AU MAN-KUAN
8,
JEN-JYH LIN
9,10, MING-FANG WU
11and JING-GUNG CHUNG
12,13 1Department of Pathology, National Defense Medical Center,
Division of Clinical Pathology, Tri-Service General Hospital, Taipei, Taiwan, R.O.C.;
2
Department of Medical Laboratory Science and Biotechnology, Yuanpei University, Hsinchu, Taiwan, R.O.C.;
3Department of Restaurant, Hotel and Institutional Management,
Fu-Jen Catholic University, New Taipei, Taiwan, R.O.C.;
5
Office of Director and Departments of
4Clinical Pathology,
6Research and Education,
7Anatomical Pathology,
8Orthopedics, Cheng Hsin General Hospital, Taipei, Taiwan, R.O.C.;
9
Graduate Institute of Chinese Medicine,
12Department of Microbiology and
13
School of Biological Science and Technology, China Medical University, Taichung, Taiwan, R.O.C.;
10Division of Cardiology, Department of Medicine, China Medical University Hospital, Taichung, Taiwan, R.O.C.;
patients. TCM has great advantages in terms of increasing
the sensitivity to chemo- and radiotherapeutics, to reducing
their side-effects, and complications associated with
chemotherapy and radiotherapy, and improving patient
quality of life and survival time (8). Therefore, an
understanding of Chinese herbal medicines is needed by
physicians and other health care providers.
Since ancient times, mushrooms have been used as an
important nutritional food and therapeutic item throughout
the world on account of their composition (9). Agaricus
blazei Murrill (ABM) popularly known as ‘Cogumelo do
Sol’in Brazil, and ‘Himematsutake’ in Japan, is a mushroom
native to Brazil, and widely cultivated in Japan for its
medicinal uses, hence it is now considered as one of the most
important edible, culinary, medicinal and biotechnological
species. It was traditionally used to treat many common
diseases such as atherosclerosis, hepatitis, hyperlipidemia,
diabetes, dermatitis and cancer (10). In vitro and in vivo
ABM has shown immunomodulatory and anti-mutagenic
properties, although the biological pathways and chemical
substances involved in its pharmacological activities are still
not clear (11, 12).
According to enforcement rules of the Health Food Control
Act established by the Taiwan Department of Health, health
food products should be evaluated for their pharmacological
effects and safety by the Ames test and the 28-day food safety
assessment for toxicology. In this study, the Ames
Salmonella/microsome mutagenicity assay (Salmonella test;
Ames test) was used, which is a short-term bacterial reverse
mutation assay specifically designed to detect a wide range
of chemical substances that can produce genetic damage
which leads to gene mutations (13). A positive test indicates
that the chemical might act as a carcinogen (although a
number of false-positives and false-negatives are known). The
procedure is described in a series of papers from the early
1970s by Bruce Ames and his group at the University of
California, Berkeley (14-17). Safety is also evaluated by the
28-day subclinical toxicological assessment in order to
examine the blood routine, the biochemical activities and the
pathological assessment of liver, spleen and kidney.
Materials and Methods
Preparation of ABM and administration dose levels for Ames test in vitro. ABM powder (500 mg), obtained from Chang Gung Biotechnology Corporation, Ltd. (Taipei, Taiwan, ROC), and 10 ml distilled water were mixed thoroughly and filtered (0.22 μm pore size) to provide a solution with a concentration of 50 mg/ml. A series of concentrations was prepared from this stock solution by dilution, namely 3 mg/ml, 6 mg/ml, 12 mg/ml, 25 mg/ml and 50 mg/ml (10, 18). Bacterial strains. Bacterial strains were provided by the Food Science Institute, Hsinchu, Taiwan. The strains used were Salmonella typhimurium TA97 (ΔuvrB/rfa/pKM101), TA98 (ΔuvrB/rfa/pKM101),
TA100 (ΔuvrB/rfa/pKM101), TA102 (rfa/pKM101), and TA1535 (ΔuvrB/rfa). Strains were prepared by preculturing for 8 h at 37˚C in a nutrient broth. Strain properties, including their susceptibility to mutagens, were confirmed prior to use in the assays by the National Taiwan University College of Medicine Animal Medicine Center, Taipei, Taiwan, ROC.
Preparation of liver S9 fractions. Rats treated with enzyme-inducing agent β-naphthoflavone were sacrificed by spinal dislocation after 28 days. Briefly, after treatment rat livers were removed, placed in beakers on ice, rinsed with ice-cold homogenization KCl (1.15%) buffer, minced with scissors and then placed in 4 volumes of ice-cold KCl buffer. They were then homogenized with a tissue grinder. The homogenate was transferred to a close-fitting (0.045 mm clearance) Perspex [poly(methyl methacrylate)]/glass homogenizer and homogenized. After diluting the homogenate to 10% with the homogenization buffer and centrifugation at 9000 ×g, the microsomal pellets were suspended in KH2PO4buffer pH 7.4 and stored at –80˚C until use.
Bacterial reverse mutation (Ames) assay. The Ames test was used to examine the mutagenicity of ABM. For the plate incorporation method, without metabolic activation, 0.1 ml of the test solutions of various concentrations of ABM, 0.1 ml of fresh bacterial broth and 0.5 ml of sterile buffer were mixed with 2.0 ml of overlay agar. For the assay with metabolic activation, 0.5 ml of metabolic activation mixtures containing an adequate amount of post-mitochondrial fraction was mixed with the overlay agar (2.0 ml), together with the bacteria and test solution. The contents of each tube were mixed and poured over the surface of a plate with minimal glucose agar. The overlay agar was allowed to solidify before incubation. The plate was incubated for 48 h at 37˚C and the number of reverting colonies was then counted. For a proper estimate of variation, triplicate plating was used at each dose level. All plates in a given assay were incubated at 37˚C for 48 h. After the incubation period, the number of reverting colonies per plate was counted.
Agar solvent was used a negative control. The positive control without S9 fraction consisted of 0.5 μg/plate of 4-nitro-o-phenylenediamine for TA97, TA98 and TA100 strains; 0.5 μg/plate of mitomycin C for TA102 strain; and 1 μg/plate of sodium azide for TA1535 strain; for any with S9 fraction, 1 μg/plate of benzo[a]pyrene was used for TA97, TA98, TA100 and TA102 strains, and 2-aminoanthracene for TA1535 strain.
Mutagenicity was evaluated based on the rule reported previously by Claxton et al. (19). The value of the positive control should be significantly higher than that of the negative control. Mutagenicity was judged to be positive when the revertants in the test plates increased more than two-fold compared with those of the negative control. All the tests of this experiment were performed in triplicate. Preparation of ABM and administration dose levels for 28-day safety assessment in vivo. ABM powder and distilled water were mixed thoroughly at 60˚C for 10 min, then cooled to room temperature and left for 5 h with stirring at 200 rpm to form solutions of low (0.5 mg/ml), medium (25 mg/ml) and high (50 mg/ml) concentrations. The ABM solution was filtered before use (10).
Animals. Forty BALB/c male mice and forty BALB/c female mice (ten/group) were supplied from the National Taiwan University College of Medicine Animal Medicine Center (our own breeding
colony), and were four weeks of age weighing 20-25 g at the beginning of the study. The animals were housed singly in an animal room with a 12-hour light/dark cycle at a temperature and relative humidity range of 20±2˚C and 75±15%, respectively. The animals were acclimated for at least two weeks prior to testing. They were fed orally with Laboratory Rodent Diet 5001 manufactured by PMI Nutrition International (St. Louis, MI, USA) during the acclimation period and throughout the study.
Study design. Animals used in the present study were maintained in accordance with the guidelines approved up by the National Science Council of the Republic of China and the Committee for the Purpose of Control and Supervision of Experiments on Animals. Experiments were performed according to law, regulations and guidelines for animal experiments in Taiwan, which are in agreement with the Helsinki declaration. Male mice were randomized and allocated into control (group 1) and experimental (second to fourth groups) groups of ten animals each. Groups 2, 3 and 4 were orally administered high (10 mg/0.2 ml), medium (5 mg/0.2 ml) and low (0.1 mg/0.2 ml) doses of ABM daily for 28 days. Female mice were also randomized and allocated similarly into groups of ten animals each. Experimental groups were orally administered the three different dose levels daily. Negative controls were fed with distilled water.
Complete blood count (CBC) analysis. At the end of the 28-day period, animals were fasted for at least 15 h and then placed in metabolism cages one day before clinical pathological evaluation. Via orbital bleeding at the end of the experiments, 20 μl whole blood samples were collected by EDTA capillary tube. Hematological parameters included erythrocyte count (RBC), hemoglobin concentration (Hb), hematocrit (Hct), mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), platelet count (PLT), total white blood cell (WBC) and differential leukocyte count (DC). Mean corpuscular hemoglobin concentration (MCHC) was also calculated. Blood smears were prepared and evaluated. The CBCs were determined on a Medonic CA530 Vet automation instrument produced by Boule Medical AB (Stockholm, Sweden). Wright-Giemsa-stained blood smears from all animals were examined microscopically for confirmation of automated results and evaluation of cellular morphology.
Serum biomarker analysis. At the end of the experiment, animals were fasted for at least 15 hours and then placed in metabolism cages one day before clinical pathological evaluation. Blood was collected via cardiac puncture (0.2 ml with 10 U/ml heparin), allowed to clot, and centrifuged (1000 ×g, 10 min, room temperature) for biochemical tests. The clinical biochemical values analyzed were: serum aspartate aminotransferase (AST), serum alanine aminotransferase (ALT), total bilirubin (T-Bil), blood urea nitrogen (BUN), blood creatinine, total cholesterol (T-Cho), fasting glucose, total serum protein (T-Pro) and albumin, all carried out on an Arkray Spotchen SP-4410 clinical chemistry analyzer using reagents manufactured by Arkray, Inc. (Kyoto, Japan).
Histopathological assessment of organs. All surviving animals at the end of the study were subjected to a complete necropsy after sacrifice under anesthesia by CO2. Major organs such as the brain, heart, kidney, liver, spleen, adrenal gland, testes, and ovaries, were weighted and examined visually for any abnormality after the removal of peripheral fat tissue. Histopathological examinations
were performed for the kidney, liver and spleen. All the collected tissues mentioned above were fixed in 10% neutral buffered formalin. Preserved organs and tissues were dehydrated, clarified, and paraffin embedded after trimming, forming paraffin tissue blocks; these were the sliced into 5 μm-thick sections using a microtome (Leica RM 2145; Leica, Nussloch, Germany), then stained with hematoxylin and eosin (H&E). Histopathology was conducted using an optical microscope by a pathology specialist and the changes were evaluated.
Statistical analysis. All data of hematological and serum biochemical analyses are expressed as the mean and standard deviation (SD). Treated and control groups were compared using a one-way analysis of variance (ANOVA). The student’s t-test was used to compare different dose treatment groups when one way ANOVA was significant. Male and female mice were evaluated separately, and differences among groups were judged to be significant at a probability value of p<0.001.
Results
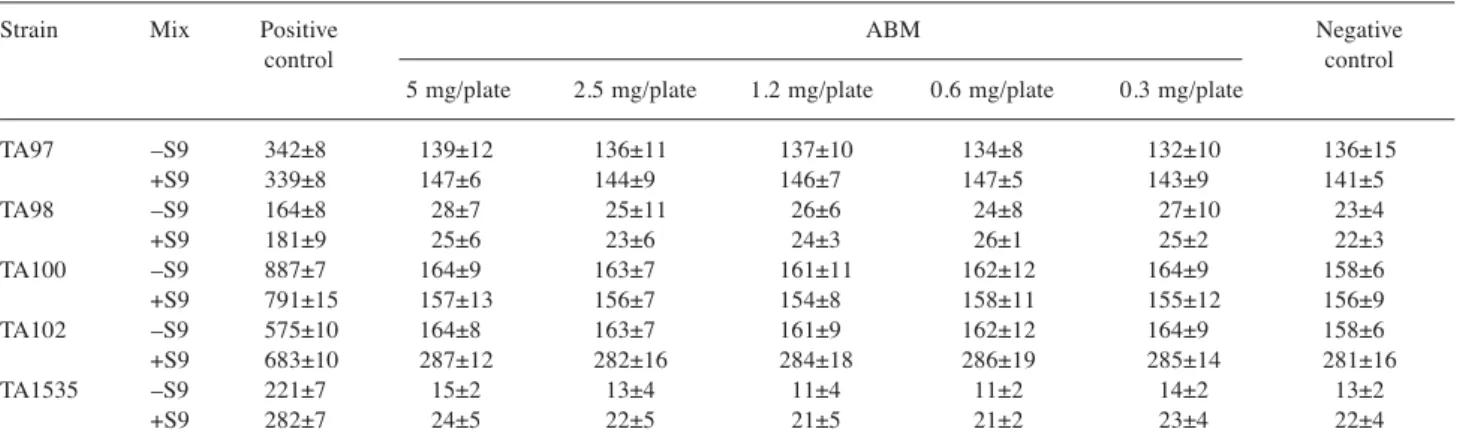
Table I shows the results of the mutagenicity of ABM
treatment using the Ames test. Compared to the negative
control, the ABM solutions with S9 and without S9 did not
affect bacterial growth. The values with S9 were lower than
these without S9 for all the TA100 strains. There were no
dose-dependent increases or decreases in the number of
revertant colonies neither with nor without metabolic
activation. Generally, mutagenicity was negative in all strains
with and without the S9 mix, as shown in Table I.
There were no mortalities nor emaciation during the course
of study and all animals appeared to be active and healthy
during the course of the study. Physical and behavioral
examinations did not reveal any treatment-related adverse
effects after dosing. Weekly mean body weight and body
weight gain for all groups that consumed ABM were
comparable to the control values. Sometimes light brown feces
were found in low, medium or high doses treatment groups,
but these findings were considered to be non-adverse as all
animals recovered by the end of the study. The overall feed
consumption of animals receiving ABM was not statistically
significantly different from that of the control groups.
The potential changes in toxicity associated with the ABM
treatment were assessed at the biochemical, hematological
and histopathological levels. The serum concentrations of the
biochemical markers ALT, AST, BUN, T-Bil and creatinine
were obtained in order to evaluate the liver and renal
functions. In addition, the histopathological changes in the
target organs such as liver, spleen and kidney were evaluated.
For the male groups, six items, namely RBC, Hb, Hct,
MCV, MCH and MCHC were not altered by exposure to the
three different doses of ABM (Table II). No increase in PLT
count was observed after administration of the high or medium
dose, but the mean PLT count of animals in the low-dose
treatment groups was higher than those of the control group
(p=0.0247), although this was not significantly increased
above the baseline control value, probably on account of the
great variability of the male group (Table II). Mice receiving
ABM did not show any statistically significant decrease or
increase in WBC levels of the low dose but a statistically
significant decrease at medium and high dose. There were no
exposure-related changes in the differential leukocyte counts,
inclusive of lymphocytes and granulocytes (p=0.0012).
Female mice treated with increasing doses of ABM did
not show any gradual elevation or decrease of MCV, MCH
and MCHC (Table III). Although for the WBC, Hb and Hct
items, it was observed that treatment groups gave higher
results compared with control groups, these were not
statistically significant (p>0.001) (Table III). For the female
groups, no increase in PLT was observed after administration
of low or medium dose. The mean PLT of the high-dose
treatment group was slightly higher than that of the control
group but did not reach statistically significant difference
compared to the baseline control value, probably on account
of the great variability. The leukocyte data are shown in
Table III. Mice did not show any statistical decrease or
increase in total leukocytes on exposure to ABM. These were
no exposure-related changes in the differential leukocyte
counts (p=0.2742).
Male mice treated with increasing doses of ABM did not
show any elevation of serum AST, ALT, Bil, BUN, CRE,
T-Cho, glucose, T-Pro and albumin concentrations (Table IV).
Although the AST levels recorded in the male control group
(251±79 IU/l) and high-dose treatment group (278±41 IU/l)
were different, this was not significant statistically.
Treated female mice did not show any difference from the
control group in serum T-Cho concentration (Table V). No
Table I. The counts of total colonies counts (CFU) including spontaneous revertant colonies that appeared on plates with different concentrations of ABM were measured by the Ames test. As positive controls without S9 (–S9), 0.5 μg/plate of 4-nitro-o-phenylenediamine for TA97, TA98 and TA100 strains, 0.5 μg/plate of mitomycin C for TA102 strain and 1 μg/plate of sodium azide for TA1535 strains were used. As positive controls but with S9 mixtures (+S9), 1 μg/plate of benzo [a] pyrene was used for TA97, TA98, TA100 and TA102 strains, and 2-aminoanthracene (1 μg/plate) for TA1535 strains were used. Control solvent was used as the negative control.
Strain Mix Positive ABM Negative
control control
5 mg/plate 2.5 mg/plate 1.2 mg/plate 0.6 mg/plate 0.3 mg/plate
TA97 –S9 342±8 139±12 136±11 137±10 134±8 132±10 136±15 +S9 339±8 147±6 144±9 146±7 147±5 143±9 141±5 TA98 –S9 164±8 28±7 25±11 26±6 24±8 27±10 23±4 +S9 181±9 25±6 23±6 24±3 26±1 25±2 22±3 TA100 –S9 887±7 164±9 163±7 161±11 162±12 164±9 158±6 +S9 791±15 157±13 156±7 154±8 158±11 155±12 156±9 TA102 –S9 575±10 164±8 163±7 161±9 162±12 164±9 158±6 +S9 683±10 287±12 282±16 284±18 286±19 285±14 281±16 TA1535 –S9 221±7 15±2 13±4 11±4 11±2 14±2 13±2 +S9 282±7 24±5 22±5 21±5 21±2 23±4 22±4
Table II. Results of mean hematological counts of male mice administered with different doses of ABM for 28-days.
Dose (mg/kg/day) Parameter Control Low Medium High
(0.5 mg/ml) (25 mg/ml) (50 mg/ml)
Erythrocyte count (106/mm3) 10.8±0.3 11.3±0.5 10.8±0.3 10.8±0.5
Hemoglobin concentration (g/dl) 16.10±0.54 16.73±0.59 16.13±0.37 15.97±0.64
Hematocrit (%) 51.2±1.8 53.3±2.0 50.7±0.9 51.0±2.0
Mean corpuscular volume (μm3) 47.4±0.9 47.3±0.4 47.1±0.9 47.1±0.4
Mean corpuscular hemoglobin (pg) 14.90±0.26 14.83±0.21 14.96±0.37 14.74±0.16 Mean corpuscular hemoglobin concentration (g/dl) 31.50±0.18 31.39±0.30 31.78±0.29 31.31±0.21
Platelet count (103/mm3) 607±60 688±69# 633±50 641±44
White blood cell count (103/mm3) 7.9±2.6 8.2±2.1 5.1±0.8# 5.8±1.8#
Differential leukocyte count
Lymphocytes (%) 89±6 86±7 86±5 87±7
Granulocytes (%) 7±2 8±2 7±1 9±3
increase in fasting glucose levels was observed after
administration of different doses of ABM for the female
groups (Table V). As for total serum protein and albumin
concentrations, there was no significant difference between
the serum concentrations in the control group and those
found in mice treated with increasing doses of ABM (Table
V). Renal biomarkers included BUN and creatinine. Female
mice treated with increasing doses of ABM did not show any
gradual elevation of serum concentrations of BUN and
creatinine, except for the low-dose treatment (Table V). The
Table III. Results of mean hematological counts of female mice administered with different doses of ABM for 28-days.
Dose (mg/kg/day) parameter Control Low Medium High
(0.5 mg/ml) (25 mg/ml) (50 mg/ml)
Erythrocyte count (106/mm3) 11.5±0.5 11.7±0.3 12.1±0.5 12.1±0.6
Hemoglobin concentration (g/dl) 17.08±0.68 17.52±0.56 17.89±0.59 18.39±1.58
Hematocrit (%) 52.1±2.6 53.7±1.8 55.2±2.0 54.9±2.9
Mean corpuscular volume (μm3) 45.4±0.5 45.7±0.5 45.7±0.9 45.5±0.8
Mean corpuscular hemoglobin (pg) 14.86±0.22 14.91±0.19 14.82±0.31 14.88±0.25 Mean corpuscular hemoglobin concentration (g/dl) 32.79±0.40 32.60±0.19 32.46±0.27 32.74±0.61
Platelet count (103/mm3) 496±55 542±70 523±74 589±91
White blood cell count (103/mm3) 6.10±1.43 5.88±1.69 7.17±1.88 6.69±1.28
Differential leukocyte count
Lymphocytes (%) 85±5 86±5 81±5 83±9
Granulocytes (%) 10±2 9±2 12±4 11±4
Table IV. Mean serum biochemical values of male mice administered with different doses of ABM for 28 days.
Dose (mg/kg/day) parameter Control Low Medium High
(0.5 mg/ml) (25 mg/ml) (50 mg/ml)
Aspartate aminotransferase (IU/l) 251±79 253±58 270±44 278±41
Alanine aminotransferase (IU/l) 65±17 69±35 54±10 61±13
Total bilirubin (mg/dl) 1.01±0.45 0.83±0.32 0.95±0.46 0.98±0.35
Blood urea nitrogen (mg/dl) 22±4 20±2 22±4 19±3
Blood creatinine (mg/dl) 0.63±0.25 0.53±0.32 0.55±0.17 0.54±0.17
Total cholesterol (mg/dl) 72±9 76±8 76±6 78±7
Fasting glucose (mg/dl) 94±19 89±13 95±23 86±12
Total serum protein (g/dl) 4.63±0.31 4.66±0.27 4.72±0.36 4.85±0.27
Albumin (g/dl) 2.10±0.12 2.18±0.13 2.13±0.07 2.15±0.11
Table V. Mean serum biochemical values of female mice administered with different doses of ABM for 28 days.
Dose(mg/kg/day) parameter Control Low Medium High
(0.5 mg/ml) (25 mg/ml) (50 mg/ml)
Aspartate aminotransferase (IU/l) 258±27 272±32 427±71* 396±69*
Alanine aminotransferase (IU/l) 94±13 88±12 142±23* 112±26
Total bilirubin (mg/dl) 2.41±0.81 2.44±1.48 2.80±0.99 1.87±0.71
Blood urea nitrogen (mg/dl) 31±3 35±3 32±4 37±10
Blood creatinine (mg/dl) 0.62±0.16 1.28±0.50# 0.61±0.09 0.99±0.21
Total cholesterol (mg/dl) 77±11 82±9 83±7 78±17
Fasting glucose (mg/dl) 114±31 104±21 131±24 121±21
Total serum protein (g/dl) 5.68±0.41 6.07±0.85 6.17±0.56 5.56±0.57
Albumin (g/dl) 2.22±0.08 2.29±0.12 2.28±0.13 2.28±0.13
blood creatinine concentrations for the females were
significantly increased (1.28±0.52 mg/dl) after administration
of the low dose in comparison to those of the control group
(0.62±0.16 mg/dl) (p=0.0011) (Table V). For the female
groups, no increase in AST levels was observed after
administration of the low dose but at medium (427±71 IU/l)
and high dose (396±69 IU/l), the mean serum AST
concentrations were significantly (p<0.001) higher than
those of the control group (258±27 IU/l). ALT concentrations
were increased (142±23 IU/l) after administration of the
medium dose in comparison to those of the baseline of the
control group (94±13 IU/l) with significant differences
(p<0.001) (Table V). The value of T-Bil was elevated by the
therapy of the medium dose (2.80±0.99 mg/dl) although this
did not reach statistical significance compared with the
baseline control value, probably due to the large variability
(Table V).
The results from the subclinical toxicity study did not
show any changing trends of dose dependency on individual
body weight or individual organ weight inclusive of liver,
spleen and kidney after 28 days of ABM administration
compared with control group. We also examined other
organs, including lung, brain, pancreas, ovary, uterus, testis
by eye and no tumor mass was found.
Liver, spleen and kidney tissue sections were stained for
all groups with H&E. The histopathological assessments in
liver, spleen and kidney were performed for the control and
the experimental groups.
Histopathological examination of liver sections from mice
treated with different concentrations of ABM revealed
non-significant hepatocellular necrosis in centrilobular regions,
without any signs of vascular or inflammatory changes. No
apoptotic morphology, such as nuclear chromatin
margination and apoptotic bodies were observed, and normal
hepatocytes were observed primarily in centrilobular regions.
Representative microphotographs did not show any nuclear
pyknosis, vascular congestion involving the portal triad and
dilation of central vein, nor fatty change in liver parenchyma.
The histopathological analysis of the liver revealed no signs
of toxicity after administration of ABM (Figure 1).
The spleen did not show any significant loss of volume,
and nor was any splenic hyperplasia observed. These was no
micronodular lymphoid infiltrate located in white pulp, nor
variable red pulp infiltration, marginal zone differentiation,
or follicular replacement by neoplastic cells. The histological
assessment of the spleen revealed normal morphology and
no vascular changes at any dose of ABM. Furthermore, no
inflammatory changes were observed at any dose in the
control and experimental groups (Figure 1).
Normal histology of the glomerulus and tubules was found
in kidney tissue of mice that received control, and ABM
treatment. ABM did not induce any vascular or inflammatory
changes, or signs of vascular congestion, tubular necrosis or
glomerular atrophy, which is a degenerative phenomenon. No
areas of red blood cells extravasating into the interstitium
and amidst the spaces between the tubules were found
(Figure 1).
Discussion
The use of dietary supplements is increasing globally and
this includes the use of plant food supplements. A variety of
factors may be influencing this increased consumption,
including the increasing number of older people in society,
mistrust in conventional medicine and the perception that
natural is healthy.
CAM is defined as a medical intervention which is not
widely taught at medical schools or is not generally available
in hospitals (20). The use of CAM has become popular
among many cancer patients all over the world. A summary
of 26 surveys conducted across 13 countries estimated the
prevalence of the use of CAM at 31.4% of all cancer
patients, ranging from 7 to 64% (21), and this market may
be growing as fast as 30% annually in the USA (22).
The incidence of acute hepatitis is mostly limited to a
single or very few clinical case report(s) among cancer
patients who have undergone chemotherapy with episodic
consumption of ABM, although no such severe acute hepatitis
or fatal liver failure was observed in many placebo-controlled
clinical studies involving ABM intake (23). It is noteworthy
that the most extensively consumed species of mushroom,
Agaricus bisporus, contains a number of aromatic hydrazines,
among which the most abundant is agaritine,
β-N-(γ-L(+)glutamyl)-4-(hydroxymethyl) phenylhydrazine, being
present at concentrations as high as 1.7 mg/g raw mushroom
(23-30). Following the studies of Toth and Erickson (31) in
which this mushroom was shown to induce tumors at a
number of sites in mice, hydrazines such as agaritine were
considered as being most likely responsible for the
carcinogenicity induced by this mushroom, since hydrazines
are an established class of chemical carcinogens (32).
Agaritine has been shown to induce adenomas and
adenocarcinomas in the lungs of mice when administered
through drinking water (33). It has also been shown to induce
mutation in DNA of the bacterium Salmonella typhimurium
(34). Upon mammalian ingestion, agaritine is metabolized
into its highly reactive diazonium ion (35). The mutagenic
activity of the diazonium ion is due to its reaction with
oxygen to produce hydrogen peroxide, which then covalently
modifies DNA through a radical mechanism (36). Agaritine
itself has also been shown to covalently bind to DNA in vivo
(37). Agaritine is a weak carcinogen, however, and estimates
for cumulative lifetime risk from mushroom consumption are
approximately 1 in 10,000 (38).
Despite the numerous reports regarding the preclinical safety
and efficacy of ABM derivatives (39), further evaluation is
Figure 1. Representative photomicrographs of liver, spleen and kidney from mice treated with high dose ABM, compared with those of the control groups. After ABM treatment, liver sections revealed no hepatocellular necrosis in centrilobular regions and were without any signs of vascular or inflammatory changes. Signs of toxicity were not found. The spleen did not show any hyperplasia, nor was there any micronodular lymphoid infiltrate located in white pulp, nor variable red pulp infiltration, marginal zone differentiation or follicular replacement by neoplastic cells. The histological assessment of the spleen displayed normal morphology and did not reveal any vascular changes. Photomicrographs also showed there were no lesions involved in the cortical and the medullary zones of kidney.
needed on account of many subspecies and various
manufactures presenting different contents. Here, we have
completed an oral safety study using ABM. The goal of this
study was to determine the suitability of ABM for future use in
food safety studies. The Ames test is used worldwide as an
initial screen to determine the mutagenic potential of new
chemicals and drugs because there is a high predictive value for
rodent carcinogenicity when a mutagenic response is obtained.
Although mutagenicity was not shown in any of the strains
with and without the S9 mix, in this experiment, we cannot
definitively state whether this particular extract is capable of
causing cancer or not. The Ames test is useful as a screening
tool for setting priorities because it is an inexpensive and
quick way to help single out chemicals that should be subjects
of further testing. More extensive testing, such as chromosome
aberration test, micronucleus test, 28-day subacute feeding
toxicity test or 90-day subchronic feeding toxicity test, is
needed to determine whether a chemical is likely to produce
cancer in humans. Because the micronucleus test and 90-day
subchronic feeding toxicity test are so labor-intensive and
time-consuming, we chose to carry out a 28-day subacute
feeding toxicity test to support food safety of ABM.
The results from the 28-day subchronic toxicity study did
not show any dose-dependent trends on individual body weight
or individual organ weight after 28 days of administration. For
the male and female groups on blood routine tests, all the eight
items exclusive of WBC counts of male were not altered by
treatment to three different doses of ABM (Table II and III).
Although exposure of male mice to ABM did not cause any
statistically significant decrease or increase in total leukocytes
counts, we take notice that p=0.0012 is near to the cut-off
p-value of 0.001, this decrease of WBC by medium- or high-dose
treatment cannot be neglected.
With increasing doses of ABM, male mice did not show
any gradual elevation of serum biochemical concentration in
any of the nine items examined (Table IV). Treated female
mice did not exhibit any differences from the control group
in T-Bil, BUN, T-Cho, fasting glucose, or total serum protein
and albumin concentrations (Table V). In creatinine levels
observed after administration of different doses in the female
groups, attention should be paid that p=0.0011 is near to the
cut-off p-value of 0.001. This suggests that the renal function
is possibly impaired by the low-dose treatment. The AST
levels of the mice treated with medium or high dose and the
ALT levels of those treated with high dose are abnormal in
comparison to those of the control group, with significant
differences. Results showed the statistical differences
observed in one sex were not observed in the other and were
not dose-dependent. No significant differences were noticed
in other parameters for either sex.
ABM (Himematsutake) is widely used among cancer
patients in Japan, however, only few cases causing liver
damage were reported. On account of different side-effects
from modern medical therapy, ABM should be safe and its
concurrent use with conventional therapies should be
evaluated, especially for female patients. So far as we know,
there are no serious side-effects reported for normal persons.
In summary, based on our findings, no infiltration,
aggregation, necrosis and atrophy were found in the control
and the experimental sections of liver, spleen and kidney.
Tissue sections of negative control and experimental groups
exhibited no apparent pathological alterations (Figure 1).
Upon microscopic examination, there was no hepatic
histopathological change correlated with the elevated
transaminase findings for female mice treated with
medium-or high-doses, and liver weights and macroscopic
appearances were normal. In female mice, the creatinine
level of the low-dose group was borderline significantly
higher than that of the control group but normal histology of
the glomerulus and tubules was found in kidney tissues.
Acknowledgements
This present study was supported by Department of Clinical Pathology, Cheng Hsin General Hospital, Taipei, Taiwan, R.O.C.
References
1 Xu W, Towers AD, Li P and Collet JP: Traditional Chinese medicine in cancer care: perspectives and experiences of patients and professionals in China. Eur J Cancer Care (Engl) 15(4): 397-403, 2006.
2 Cui X, Wang Y, Kokudo N, Fang D and Tang W: Traditional Chinese medicine and related active compounds against hepatitis B virus infection. Biosci Trends 4(2): 39-47, 2010.
3 Chiang JH, Yang JS, Ma CY, Yang MD, Huang HY, Hsia TC, Kuo HM, Wu PP, Lee TH and Chung JG: Danthron, an anthraquinone derivative, induces DNA damage and caspase cascades-mediated apoptosis in SNU-1 human gastric cancer cells through mitochondrial permeability transition pores and Bax-triggered pathways. Chem Res Toxicol 24(1): 20-29, 2011. 4 Lu CC, Yang JS, Huang AC, Hsia TC, Chou ST, Kuo CL, Lu HF, Lee TH, Wood WG and Chung JG: Chrysophanol induces necrosis through the production of ROS and alteration of ATP levels in J5 human liver cancer cells. Mol Nutr Food Res 54(7): 967-976, 2010.
5 Wu CL, Huang AC, Yang JS, Liao CL, Lu HF, Chou ST, Ma CY, Hsia TC, Ko YC and Chung JG: Benzyl isothiocyanate (BITC) and phenethyl isothiocyanate (PEITC)-mediated generation of reactive oxygen species causes cell cycle arrest and induces apoptosis via activation of caspase-3, mitochondria dysfunction and nitric oxide (NO) in human osteogenic sarcoma U-2 OS cells. J Orthop Res 29(8): 1199-1209, 2011.
6 Wong R, Sagar CM and Sagar SM: Integration of Chinese medicine into supportive cancer care: a modern role for an ancient tradition. Cancer Treat Rev 27(4): 235-246, 2001. 7 Gai RY, Xu HL, Qu XJ, Wang FS, Lou HX, Han JX, Nakata M,
Kokudo N, Sugawara Y, Kuroiwa C and Tang W: Dynamic of modernizing traditional Chinese medicine and the standards system for its development. Drug Discov Ther 2: 2-4, 2008.
8 Konkimalla VB and Efferth T: Evidence-based Chinese medicine for cancer therapy. J Ethnopharmacol 116(2): 207-210, 2008. 9 Murakawa K, Fukunaga K, Tanouchi M, Hosokawa M, Hossain
Z and Takahashi K: Therapy of myeloma in vivo using marine phospholipid in combination with Agaricus blazei Murill as an immune respond activator. J Oleo Sci 56(4): 179-188, 2007. 10 Wu MF, Lu HF, Hsu YM, Tang MC, Chen HC, Lee CS, Yang
YY, Yeh MY, Chung HK, Huang YP, Wu CC and Chung JG: Possible reduction of hepatoma formation by Smmu 7721 cells in SCID mice and metastasis formation by B16F10 melanoma cells in C57BL/6 mice by Agaricus blazei murill extract. In Vivo 25(3): 399-404, 2011.
11 Lima CU, Cordova CO, Nobrega Ode T, Funghetto SS and Karnikowski MG: Does the Agaricus blazei Murill mushroom have properties that affect the immune system? An integrative review. J Med Food 14(1-2): 2-8, 2011.
12 Wu MF, Hsu YM, Tang MC, Chen HC, Chung JG, Lu HF, Lin JP, Tang NY, Yeh C and Yeh MY: Agaricus blazei Murill extract abrogates CCl4-induced liver injury in rats. In Vivo 25(1): 35-40, 2011.
13 Mortelmans K and Zeiger E: The Ames Salmonella/microsome mutagenicity assay. Mutat Res 455(1-2): 29-60, 2000.
14 Ames BN, Gurney EG, Miller JA and Bartsch H: Carcinogens as frameshift mutagens: metabolites and derivatives of 2-acetylaminofluorene and other aromatic amine carcinogens. Proc Natl Acad Sci USA 69(11): 3128-3132, 1972.
15 Ames BN, Lee FD and Durston WE: An improved bacterial test system for the detection and classification of mutagens and carcinogens. Proc Natl Acad Sci USA 70(3): 782-786, 1973. 16 McCann J, Spingarn NE, Kobori J and Ames BN: Detection of
carcinogens as mutagens: bacterial tester strains with R factor plasmids. Proc Natl Acad Sci USA 72(3): 979-983, 1975. 17 Ames BN, Durston WE, Yamasaki E and Lee FD: Carcinogens
are mutagens: a simple test system combining liver homogenates for activation and bacteria for detection. Proc Natl Acad Sci USA 70(8): 2281-2285, 1973.
18 Wu MF, Chen YL, Lee MH, Shih YL, Hsu YM, Tang MC, Lu HF, Tang NY, Yang ST, Chueh FS and Chung JG: Effect of Agaricus blazei Murrill extract on HT-29 human colon cancer cells in SCID mice in vivo. In Vivo 25(4): 673-677, 2011. 19 Claxton LD, Allen J, Auletta A, Mortelmans K, Nestmann E and
Zeiger E: Guide for the Salmonella typhimurium/mammalian microsome tests for bacterial mutagenicity. Mutat Res 189(2): 83-91, 1987.
20 Eisenberg DM, Kessler RC, Foster C, Norlock FE, Calkins DR and Delbanco TL: Unconventional medicine in the United States. Prevalence, costs, and patterns of use. N Engl J Med 328(4): 246-252, 1993.
21 Fernandez CV, Stutzer CA, MacWilliam L and Fryer C: Alternative and complementary therapy use in pediatric oncology patients in British Columbia: prevalence and reasons for use and nonuse. J Clin Oncol 16(4): 1279-1286, 1998. 22 Eisenberg DM, Davis RB, Ettner SL, Appel S, Wilkey S, Van
Rompay M and Kessler RC: Trends in alternative medicine use in the United States, 1990-1997: results of a follow-up national survey. JAMA 280(18): 1569-1575, 1998.
23 Teschke R, Schwarzenboeck A, Schmidt-Taenzer W, Wolff A and Hennermann KH: Herb induced liver injury presumably caused by black cohosh: a survey of initially purported cases and herbal quality specifications. Ann Hepatol 10(3): 249-259, 2011. 24 Aeschbacher HU, Finot PA and Wolleb U: Interactions of
histidine-containing test substances and extraction methods with the Ames mutagenicity test. Mutat Res 113(2): 103-116, 1983. 25 Arimoto S, Negishi K and Hayatsu H: A modification of the
Ames test procedure: accelerated growth of the His+ revertants. Mutat Res 91(4-5): 407-411, 1981.
26 Ellertsen LK and Hetland G: An extract of the medicinal mushroom Agaricus blazei Murill can protect against allergy. Clin Mol Allergy 7: 6, 2009.
27 Koivikko A and Savolainen J: Mushroom allergy. Allergy 43(1): 1-10, 1988.
28 Hopkins HH: Mushroom dermatitis; report of a case. AMA Arch Derm Syphilol 67(6): 632-633, 1953.
29 Korstanje MJ and van de Staak WJ: A case of hand eczema due to mushrooms. Contact Dermatitis 22(2): 115-116, 1990. 30 Liu JW, Beelman RB, Lineback DR and Speroni JJ: Agaritine
Content of Fresh and Processed Mushrooms [Agaricus bisporus (Lange) Imbach]. J Food Sci 47(5): 1542-1544, 1982.
31 Toth B and Erickson J: Cancer induction in mice by feeding of the uncooked cultivated mushroom of commerce Agaricus bisporus. Cancer Res 46(8): 4007-4011, 1986.
32 Toth B: Synthetic and naturally occurring hydrazines as possible cancer causative agents. Cancer Res 35(12): 3693-3697, 1975. 33 Toth B, Nagel D, Patil K, Erickson J and Antonson K: Tumor
induction with the N'-acetyl derivative of 4-hydroxymethyl-phenylhydrazine, a metabolite of agaritine of Agaricus bisporus. Cancer Res 38(1): 177-180, 1978.
34 Rogan EG, Walker BA, Gingell R, Nagel DL and Toth B: Microbial mutagenicity of selected hydrazines. Mutat Res 102(4): 413-424, 1982.
35 Kondo K, Watanabe A, Akiyama H and Maitani T: The metabolisms of agaritine, a mushroom hydrazine in mice. Food Chem Toxicol 46(3): 854-862, 2008.
36 Freese E, Sklarow S and Freese EB: DNA damage caused by antidepressant hydrazines and related drugs. Mutat Res 5(3): 343-348, 1968.
37 Shephard SE and Schlatter C: Covalent binding of agaritine to DNA in vivo. Food Chem Toxicol 36(11): 971-974, 1998. 38 Shephard SE, Gunz D and Schlatter C: Genotoxicity of agaritine
in the lacI transgenic mouse mutation assay: evaluation of the health risk of mushroom consumption. Food Chem Toxicol 33(4): 257-264, 1995.
39 Ohno S, Sumiyoshi Y, Hashine K, Shirato A, Kyo S, Inoue M. Phase I clinical study of the dietary supplement, Agaricus blazei Murill, in cancer patients in remission. Evid Based Complement Alternat Med 2011: 1-9, 2011.