January 6, 2014
Professor Kamatchi Ulagappan
Editor, Journal of Materials Science: Materials in Medicine
RE: JMSM6239 Revision
Dear Professor Kamatchi Ulagappan:
Thank you very much for arranging the review process for our manuscript JMSM6239. We found that the reviewers’ comments and suggestions are very valuable and constructive in helping us revising the manuscript. Enclosed, please find the revised manuscript along with a detailed list of responses to the concerns.
Thank you again. We look forward to hearing from you soon.
Sincerely yours,
Yu-Hsin Lin, PhD Associate Professor
Department of Biological Science and Technology China Medical University,
Taichung, Taiwan, 40402 Fax: 886-4-2207-1507
Dear Reviewers:
Thank you very much for taking time and effort in reviewing our manuscript, JMSM6239. We found that your comments and suggestions were very valuable in helping us revise the manuscript. The changes made in the new manuscript as per your comments and suggestions are shown below.
Reviewer #1:
This article by Lin et al. is of high technical importance and suitable for consideration for publication in Journal of Materials Science: Materials in Medicine.
Thanks for your encouraging review.
1. I have found typos throughout the article. The quality of English throughout the article is very poor. I suggest author should take help of an expert and carefully revised the article carefully.
Thanks for pointing out the typos. This paper has been revised by a native English speaking editor as suggested.
2. In the entire article authors have incorrectly right experimentally evaluated/ measured values. For example, time is mentioned as 3hr. Instead, it should be 3 hr. Check and rectify such mistakes throughout the manuscript.
Thanks for pointing out the typo. The all mistakes of experimentally evaluated/ measured value were rectified.
3. On page 4 (Last para) authors claims that silver particles wee then broken into fine grains and deposited on the ACF. I wonder how, that is happening. I suggest authors should elaborate this part.
Thanks for your constructive suggestion. The sentence has been reworded and explained in more detailed (please refer to 2.1 Preparation of ACF and various Ag-containing ACF, page 4).
4. Page 5 (line no. 50-52): ".... inhibit growth to bacterial suspension of various..."- Redraft the sentence.
Thanks for your constructive suggestion. The sentence ".... inhibit growth to bacterial suspension of various..." has been rephrased (please refer to 2.3 Antimicrobial activity, page 5).
5. Syntax of "In vito" and "In vivo" is incorrect. It should be In-vitro and In-vivo (Both in italics).
Thanks for your comment. Syntax of “In-vitro” and “In-vivo” has all been corrected throughout the manuscript.
6. Page 9 (Line 23): Authors claim that silver ion release depends on silver preparation. I wounder how synthesis methods of silver nanoparticle preparation affect the release. Authors should provide experimental proof or relevant reference to this claim.
Thanks for your constructive suggestion. What we meant is that the silver coated on Silverlon is not in the form of nanoparticle, instead, is a sheet of metallic silver. It is like bulk silver exists in a form of thin film. Based on previous studies (Ref 8 and 24 in the manuscript), it would release lesser silver ion due to its smaller surface area. Therefore, what we said “method for silver preparation” means preparation of all kinds of silver, not limited to nanoparticle specifically (please refer to 3.2 Silver release from wound dressing, page 9).
7. Page 11 (Line 51-57): Authors claims that Acticoat 7 eliminates bacterial strains most efficiently as its cytotoxicity is extremely high. Further, authors claims that Acticoat is safe for use in patients. These are two opposite claims. More clarification is required here. Please accept our apology for the confusion. The reasonable explanation of the safety of Acticoat on patients with high in-vitro cell cytotoxicity was described. The Acticoat product might exhibit lower cytotoxicity on skin tissue compared to that on monolayer cell culture. It is also supported by our in-vivo wound healing study (please refer to 3.4 Cell cytotoxicity analysis for silver-containing ACF dressing, page 11 and 12).
Reviewer #2:
The article deals with a very interesting topic. The paper is good, interesting, well written and prepared carefully. My only comments and minor revisions are the following.
Thanks for your encouraging review.
1. The authors evaluated the silver ions release from the wound dressings after incubation in distilled water for 24 hours at 37°C. Have the authors evaluated the silver ions release in different aqueous solutions such as artificial exudate or simulated body fluid? Do the authors mean to perform further experiments about that?
Thanks for your constructive suggestion. Actually, the silver ion release of Ag-ACF in simulated body fluid (142 mM NaCl and 2.5 mM CaCl2) has been evaluated. We compared the
silver ion release of Ag-5/ACF in simulated body fluid and that in distilled water, there is no significant difference between these two aqueous solutions. We will exam more assays experiment of the various Ag-ACF dressing in our future study.
Please accept our apology for the confusion. Five rats were used in in-vivo study. The description has been added in, page 6 (2.5 Wound healing and histologic analysis in infected wound tissue) and Figure Caption (Fig 6, page 20).
3. Abstract, Line 12: Change "an silver-containing dressing" to "a silver containing dressing"
Thanks for your constructive suggestion. The grammar error has been corrected as suggested (please refer to Abstract).
4. Materials and Methods, Paragraph 2.5, Line 10: Change "S. aureu" to " S. aureus". Thanks for your suggestion. The typo “S.aureu” has been corrected as “S.aureus” (please refer to 2.5 Wound healing and histologic analysis in infected wound tissue, page 7).
Evaluation of various silver-containing dressing on infected excision wound healing study
Yu-Hsin Lina*, Wei-Shan Hsub, Wan-Yu Chungc, Tse-Hao Kod, Jui-Hsiang Line*
a Associate Professor, Department of Biological Science and Technology, China Medical
University, Taichung, Taiwan
b Senior Researcher, Bio-medical Carbon Technology Co., Ltd., Taichung, Taiwan c Associate Researcher, Bio-medical Carbon Technology Co., Ltd., Taichung, Taiwan
d Distinguished Professor, Department of Materials Science and Engineering, Feng Chia
University, Taichung, Taiwan
e Manager, R&D Center, Bio-medical Carbon Technology Co., Ltd., Taichung, Taiwan
*Correspondence to Jui-Hsiang Lin [email protected] Tel: +886423554588#700 Yu-Hsin Lin [email protected] Tel: +886422053366#2525
* The contributions by the two collaborating parties (Dr. Jui-Hsiang Lin, [email protected] and Dr. Yu-Hsin Lin, [email protected]) are equal.
Abstract
Silver-containing dressings have been widely used for controlling wound infection. However, the relationship between different concentrations of silver in dressings and their antimicrobial activities and wound-healing efficacies remains unclear. In the present study, we (in cooperation with Bio-medical Carbon Technology) investigated various silver-containing activated carbon fibers to understand the effects of different silver concentrations on the efficacies of a silver containing dressing. Our results indicated that various silver-containing activated carbon fibers exhibited good antibacterial effects and biocompatibility in terms of cell viability and that silver concentration showed a minor influence on cell growth. The infected excision wound model indicated that compared to containing activated carbon fiber and other commercial silver-containing dressings assisted wound healing by promoting granulation and collagen deposition. Meanwhile, the silver ion can only be restrained in epidermis by intact skin. During application on the wound area, a temporary increase of serum silver can be detected, but this elevated serum silver level decreased to a subtle level after the removal of silver-containing activated carbon fiber.
1 Introduction
Intact skin provides a barrier to protect vertebrates from pathogen invasion. When damage to the skin occurs in such forms as abrasions, punctures, burns, surgical wounds or chronic wounds, the safeguard is broken and, in turn, the chance of infection is dramatically increased. Antibiotics were once powerfully effective medicines for controlling pathogenic infection. However, the emergence of various antibiotic-resistant bacteria like Methicillin-resistant Staphylococcus aureus (MRSA), Multidrug-resistant Pseudomonas aeruginosa and Multidrug-resistant Acinetobacter baumannii has impeded and limited the broad efficacy of antibiotics [1-3]. As a result, silver is now widely used in wound dressing for controlling infections [4]. Silver is a natural antimicrobial agent that is able to be effective against more than 650 disease-causing microorganisms [5-7]. The antimicrobial activity of silver results from changes to bacterial membrane permeability, the inhibition of bacterial DNA replication/RNA transcription and dysfunction of bacterial enzymes [8]. This multi-directional antimicrobial mechanism effectively eliminates positive and Gram-negative bacteria, with only sporadic cases of silver resistance ever documented since 1998 [9-10].
As of now, various commercial silver-containing dressings have been developed, and the safety and effectiveness of silver-containing dressings have been widely accepted and verified by plenty of clinical trials [8,11]. These dressings can be made of various materials, including polyethylene film, hydrofiber, foam, alginate or activated carbon, among others, and the material used could determine the property of the dressing. In addition, various factors such as the silver concentration, the type of silver used (metal particle or ionic salt), the amount of silver ion released and the manufacturing process used all affect the antimicrobial activities of silver-containing dressings. Activated carbon has been applied in wound dressings, which were originally designed to control would malodor [12,13]. Activated carbon fiber (ACF) has a high degree of microporosity and an enormous internal surface area [14-16]. These properties contribute to its excellent adsorptive capacity for chemicals and gases. The ACF made of carbonaceous source materials like coconut, wood or nutshells belongs to the category of charcoal-based activated carbon. Alternatives such as polyacrylonitrile (PAN) can serve as the raw material as well for producing PAN-based ACF. PAN-based ACF contains more uniform micropores and an even
higher surface area compared to charcoal-based activated carbon [14,15].
A commercial wound dressing composed of PAN-based ACF supporting silver particles included via the impregnation method, KoCarbonAg®, has been developed by Bio-medical Carbon
Technology Co., Ltd. Actisorb silver 220 (Systagenix) is another commercially available dressing which comprises silver impregnated charcoal activated carbon cloth enclosed in a sleeve of non-woven nylon. Acticoat 7 (Smith & Nephew) is composed of alternate layers of rayon and silver-coated polyethylene film with a physical vapor deposition process for silver coating. Silverlon (Argentium Medical) is a silver-coated nylon fabric using electroless plating technology. In this study, we examined distinct silver-containing PAN-based ACF (hereafter abbreviated as Ag-ACF) with regard to its physicochemical characteristics, namely its silver distribution phenomenon and release profile, as well as its antimicrobial activity and infected tissue wound healing, with the commercially available silver-containing dressings mentioned above used for the purpose of comparison.
2 Materials and methods
2.1 Preparation of ACF and various silver-containing ACF
The raw ACF cloths in this study came from Bio-medical Carbon Technology, Taiwan. The ACF cloths were produced from raw oxidized PAN fiber cloths (thickness: 0.73 mm; base weight: 310 g m-2). The precursor of oxidized PAN fiber was activated using steam (0.2 mL min-1) and CO
2
(0.1 mL min-1) for 10 min to prepare ACF. The ACF samples were impregnated with various
concentrations of silver nitrate solution in vacuo for 3 hrs, then heated at 350°C for 120 min under nitrogen. During heat treatment, the silver nitrate is reduced to silver metal particles. Specifically, the nitrite and nitrate are vaporized out from the surface of the ACF, resulting in fine grains of silver particles deposited on the ACF surface. The surface morphology of various silver-containing ACF dressing was investigated visually using a field-emission scanning electron microscope (HITACHI S-4800, Japan).
The dressings tested in this study were first trimmed into pieces with dimensions of 1 x 3 cm2.
Three pieces of corresponding trimmed sample were then immersed in 3 mL distilled water at 37°C for 24 hrs. After 24 hrs, the distilled water immersed with particular samples was diluted by 10 times, followed by filtering off the debris, and then subjected to inductively coupled plasma-optical emission spectrometer (ICP-OES) to determine the sliver concentration (ppm). Standard solutions with 0.1 to 2 ppm were prepared. Values below 0.1 ppm were obtained by extrapolation.
2.3 Antimicrobial activity
We analyzed different common wound dressings [Acticoat 7, Silverlon, Actisorb silver 220, and Ag-ACF (support by Bio-medical Carbon Technology Co., Ltd)] to inhibit P. aeruginosa growth ability. The P. aeruginosa (ATCC 27853) were obtained from the American Type Culture Collection (ATCC, Manassas, VA). These bacteria were grown on tryptic soy broth (TSB) agar plates under microaerophilic conditions for 24 hrs at 37℃ [17]. A single colony was selected and cultured in TSB medium to an optical density of 1.0 at 590 nm (OD590) by a visible
spectrophotometer (Biochrom, England, UK). The tested dressings with dimensions of 2 x 2 cm2
were exposed to 5.00 mL TSB culture medium with 0.02 mL fresh bacteria broth for specific time interval as indicated. Bacterial suspension at indicated time intervals were serial diluted and plated on the TSB agar plates. The colony-forming unit (CFU mL-1) of bacterial suspension exposed to test
samples was determined by counting the amount of colonies grown on the TSB agar plates.
Furthermore, we tested various ACF containing 1 mg, 5 mg, 10 mg and 20 mg per 100 cm2 of
silver (Ag-1/ACF, Ag-5/ACF, Ag-10/ACF and Ag-20/ACF; support by Bio-medical Carbon Technology) for their growth effect. Bacterium E. coli (ATCC 25922), S. aureus (ATCC 25923), and P. aeruginosa (ATCC 27853) were obtained from the American Type Culture Collection (ATCC, Manassas, VA). The tested dressings with the same dimensions of 2 x 2 cm2 were exposed
to 5.00 mL TSB culture medium with 0.02 mL fresh bacteria broth for 24 hrs to characterize the inhibition percentage of growth on bacterial suspension of various silver-containing ACF dressings. The extent of growth inhibition was determined by counting the number of colonies, and quantification of in-vitro antibacterial activity was conducted by calculating percentage of growth
inhibition as compared to untreated bacteria [18]. The percent growth inhibition was determined using the formula:
% growth inhibition=[(colony number of control -colony number of sample) /colony number of control ] x 100%
2.4 Cell cytotoxicity for sliver containing ACF
Normal human skin fibroblast (NHF) cells were initially grown in 25 cm2 tissue culture flasks
with medium supplemented with 0.1 mM nonessential amino acids, 1.0 mM sodium pyruvate, 10% fetal bovine serum, penicillin (100 U mL-1), and streptomycin (100 μg mL-1), and were kept in an
incubator at 37°C, 95% humidity, and 5% CO2. The cells were harvested for subculture every 3
days with 0.25% trypsin plus 0.05% ethylenediaminetetraacetic acid solution and were used for the cell viability experiments. The cytotoxicity of the test samples was evaluated in-vitro using 3-(4,5-dimethyl-thiazol-yl)-2,5-diphenyltetrazolium bromide (MTT) assay. The assay is based on mitochondrial dehydrogenase activity as an indicator of cell viability [19,20]. The NHF cells were seeded at 1 x 105 cells per well in 24-well plates overnight, and then placed in growth medium
containing test samples for 24 hrs. The cells were then incubated in growth medium containing 1 mg mL-1 MTT for an additional 4 hrs. Dimethyl sulfoxide (100 μL) was added to each well to
ensure solubilization of the formazan crystals. The optical density was read with a Molecular Devices SpectraMax M2e microplate spectrofluorometer at a wavelength of 570 nm [21]. All
experiments were performed six times with eight replicate wells for every sample and control per assay.
2.5 Wound healing and histologic analysis in infected wound tissue
Animal care and use complied with the 1996 revision of the “guide for the care and use of laboratory animals’’ prepared by the Institute of Laboratory Animal Resources, National Research Council, and published by the National Academy Press. Five Sprague–Dawley (SD) rats weighing 250–300g were individually housed in polycarbonate cages maintained at constant temperature (22°C+2°C) and humidity (55%). The rats were subjected to a 12:12 hrs light-dark cycle and access
to food and water, and their average weight and behavior did not change significantly during the experiment. Rats were anesthetized with an intraperitoneal injection of ketamine (90 mg kg-1) with
xylazine (10 mg kg-1) [22]. The dorsal skin was shaved, application fields were outlined with a
marker pen before skin excision, and the surgical area was disinfected with 70% ethanol. On the back of each rat, a full-thickness wound with dimensions of 1 x 1 cm2 was created on each side of
the spine by dermo-epidermic excision. The wounded rats each received 100 μL of the bacterial mixture including P. aeruginosa, E. coli and S. aureus (1.5 OD590 of each) on the wound surface.
Wounded rats were applied with tested dressings with dimensions of 2 x 2 cm2 after 24 hrs
infection. Each dressing was covered with a sterile compress secured by a hypoallergenic elastic adhesive bandage. Animals were caged individually following identification. The dressings were changed every three days; the wounds were photographed and examined to determine wound size reduction. Wound size measurements taken during surgery, and biopsy were used to calculate percentage size reduction of wounds [23].
Wound size reduction (%) = [(A0- At)/A0] x 100
where A0 and At denote initial wound area and wound area after time interval ‘‘t’’, respectively.
Wound area was measured from photographs using the Image-Pro Plus (Media Cybernetics, Silver Spring, MD) following calibration. Histologic analysis at different healing times was carried out using light microscopy. Briefly, biopsies were fixed in buffered paraformaldehyde and embedded in paraffin wax. Sections of 5 μm were stained with hematoxylin and eosin, and Masson’s trichrome. The stained sections of each test sample were then examined under a light microscope, for analysis of tissue regeneration.
2.6 Silver distribution of intact skin and blood in animal study
First, the 2 x 2 cm2 tested dressing was applied on the intact dorsal skin of SD rat for 3 days.
The applied silver-containing dressing was covered and fixed by the transparent adhesive opsite film. Rats were scarified 3 days after applying test sample dressing, the full-thickness skin tissue with dimensions of 1 x 1 cm2 underneath dressing applied area and 2 mL of blood were sampled,
subjected to ICP-OES to determine the silver concentration (ppm) of the test sample. Silver content in skin (μg cm-2) = (value of ppm) x 0.05 L x 1000 x 1 cm-2
Second, the full-thickness excisional wound on dorsal side of rat was created as mentioned in the section of “wound healing” except for no bacterial broth was added as the representative of clean wound. Various silver-containing ACF with dimensions of 2 x 2 cm2 were applied on the
wound area, covered with a sterile compress secured by a hypoallergenic elastic adhesive bandage. The dressings were changed on the 3rd and 6th day after surgery, and applying Ag-ACF was stopped since 9th postsurgery day. The 2 mL of blood was collected at the 5 days after surgery as well as at 21 days after the removal of Ag-ACF. The collected blood samples were then subjected to ICP-OES to determine the silver concentration.
2.7 Statistical analysis
Statistical analysis of differences in measured properties of the groups was performed with one-way analysis of variance and the determination of confidence intervals, with the statistical package Statistical Analysis System, version 6.08 (SAS Institute, NC). All data are presented as means and standard deviations, indicated as “mean + SD”. Differences were considered statistically significant when the p values were <0.05.
3 Results and discussion
3.1 Micrographs of silver-containing ACF wound dressings
The ACF containing 1 mg, 5 mg, 10 mg and 20 mg per 100 cm2 of silver (1/ACF,
Ag-5/ACF, Ag-10/ACF and Ag-20/ACF, respectively) were prepared, and their morphology was investigated under a scanning electron microscope. Micrographs showed that ACF is about 5 μm in diameter (Fig. 1). The silver particles are evenly distributed along the fiber and the quantity is in proportion to the silver content indicated (black arrows). Current commercial product, KoCarbonAg®, contains silver with an average of 5 mg per 100 cm2, is represented as Ag-5/ACF in
this study.
The antimicrobial activity of silver comes from the release of the silver ion when it comes in contact with an aqueous environment [8]. The amount of silver ion released from various silver-containing ACFs was examined in distilled water for 24 hrs at 37°C. After 24 hrs, 3.67, 2.12, 1.40, and 0.90 ppm of silver ion were detected, respectively, in the distilled water samples in which Ag-20/ACF, Ag-10/ACF, Ag-5/ACF, and Ag-1/ACF were immersed (Fig. 2). This indicates that the higher the silver content on the ACF, the greater the amount of silver ion that can be released in an aqueous environment. However, silver content is not the only factor that affects the amount of silver ion release. The silver content of Silverlon is 546 mg per 100 cm2, which is 27.3 times higher than
that of Ag-20/ACF. Nevertheless, the amount of silver ion released from Silverlon was measured at 3.62 ppm, which is similar to Ag-20/ACF (Fig. 2). On the other hand, the amount of silver ion released from Actisorb silver 220 was 0.13 ppm (Fig. 2), which is 7 times lower than the release rate of Ag-1/ACF, even though the silver content of Actisorb silver 220 is about 2.7 times higher than that of Ag-1/ACF.
One factor that may affect the silver ion release is the method of silver preparation. It was already known that silver nanoparticle releases silver ion at a greater rate than bulk silver and that this is due to the larger surface area of nanoparticles [8,24]. The method of electroless plating coats a layer of metallic silver on the surface of Silverlon, leaving a sheet of silver film on the surface instead of silver nanoparticles. This difference dramatically reduces the surface area of silver and could be the reason for the low silver ion release rate of this highest silver-containing dressing. Meanwhile, the fundamental material of the silver-containing dressing may also play a role in the rate of silver ion release. Actisorb silver 220 is composed of metallic silver impregnated on activated carbon (charcoal) cloth enclosed in a non-woven bag. The low level of silver ion released from Actisorb silver 220 may partially be the consequence of the adsorptive property of the activated carbon, which can adsorb metals ions such as silver ion and thus decrease the silver ion concentration in the aqueous solution [25,26].
In addition, Acticoat 7 releases an extremely high level of silver ion (Fig. 2). Acticoat 7 contains 148 mg of nanocrystalline silver per 100 cm2, with a crystallite size of ~50 nm in diameter.
In addition, both of its fundamental materials (rayon and polyethylene film) have no adsorptive property, a factor which may contribute to its high capacity for silver ion release. While monitoring the silver ion release, we found that the amount of silver ion in the distilled water in which Acticoat 7 was immersed accumulated over time, whereas the silver ion released from other samples reached
a stable level 30 min after immersion (data not shown). Such stable release of silver ion could minimize the chance of excessive silver deposition in wound tissue [27].
3.3 In-vitro antimicrobial activity
In-vitro study of P. aeruginosa elimination indicates that the antibacterial activity of the silver-containing dressing is partially correlated with the amount of silver ion release. With the start of microbial load of 108CFU mL-1 (8log
10 CFU mL-1), Acticoat 7, which releases the most abundant
silver ion, decreased the level of P. aeruginosa to 1 log10 CFU mL-1 at 2 hrs, whereas Actisorb
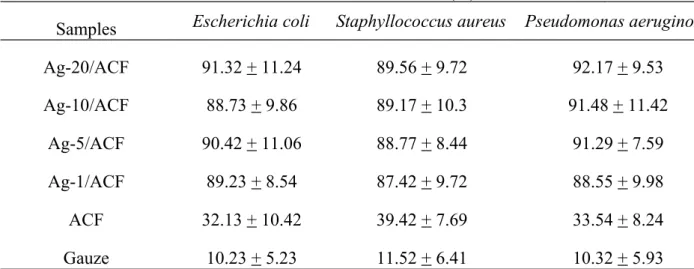
Silver 220, which releases lowest level of silver ion, took 2.5 hrs to approach the same log reduction (Fig. 3a). These results indicate that the more silver ion released from the dressing, the rapidest bacterial elimination can be achieved. However, Ag-5/ACF and Silverlon, which have 2.5 times difference in their silver ion release (Fig. 2), exhibited a similar efficacy for P. aeruginosa elimination (Fig. 3a). This may be the consequence of the adsorptive property of ACF [28-30]. ACF has been known as an excellent adsorbent and been widely used in drinking water system for removal of unpleasant tastes, odor and even germs [29,30]. Therefore, the adsorption of bacteria by ACF allows Ag-5/ACF achieving similar antimicrobial efficacy as Silverlon did while the silver ion released from Ag-5/ACF is lower than Silverlon. Notably, even various levels of silver ion eliminated P. aeruginosa with distinct rates, all these dressings examined in this study suppressed the bacterial growth to a stable condition (Fig. 3a, at 4 hrs). In addition, the antimicrobial activities of various silver-containing ACFs (Ag-1/ACF, Ag-5/ACF, Ag-10/ACF and Ag-20/ACF) against P. aeruginosa, S. aureus and E. coli for 24 hrs were then examined (Fig. 3b). Consistent with the result mentioned above, even though these various silver-containing dressings exhibited different efficiencies for bacterial elimination during the first couple hrs, they all showed inhibition effects of approximately 90% at 24 hrs for all three bacterial strains that were tested (Table 1, Fig. 3b).
3.4 Cell cytotoxicity analysis for silver-containing ACF dressing
The potential toxicity of silver is always a concern to patients and health care professionals when applying silver derivatives on the wound area. An in-vitro study indicated that the silver
nitrate solution with > 25 μg mL-1 has 80% significantly toxic effect to human keratinocyte and
fibroblast monolayer culture [31]. Similarly, a study showed that silver sulfadiazine at 100 μg mL-1
concentration may exhibit cytotoxic effects to human keratinocyte cell [32]; both studies showed that the cytotoxic effects are dose-dependent. It is worth notice that for silver sulfadiazine or silver nitrate, once the concentration reaches the level with sufficient antimicrobial activity, it usually comes along with the considerable degree of cytotoxicity.
Therefore, we tested the silver-containing ACF for their cytotoxic effects by examining the survival percentage of human fibroblast cells after treating with different samples for 24 hrs. As shown in Fig. 4, the ACF dressing without coated silver could express biocompatibility and good human fibroblast cells viability. Then, ACF with various silver content showed some degree of cytotoxic effect, 90.72+5.35, 81.54+4.81, 77.49+6.54 and 79.85+7.42% of cell viability were obtained by Ag-1/ACF, Ag-5/ACF, Ag-10/ACF and Ag-20/ACF, respectively. In consistent with previous studies, the cytotoxic effect is related to the concentration of silver. However, our result showed that silver-containing ACF exhibited only a minor cytotoxic effect related to silver concentration, with a decrease of 10% viability from silver content of Ag-1/ACF to Ag-20/ACF. With the standard of ISO 10993-5:2009 “Biological evaluation of medical devices Part 5: Tests for in vitro cytotoxicity”, Ag-1/ACF and Ag-5/ACF exhibit slight cytotoxicity (Grade 1, not more than 20% of the cells are dead); Ag-10/ACF and Ag-20/ACF exhibit mild cytotoxicity (Grade 2, not more than 50% of the cells are dead).
The cytotoxic effect is not solely determined by the silver content of or silver ion released from the dressing. While Silverlon and Actisorb silver 220 have similar or much lower level of silver ion release compared to Ag-20/ACF did (Fig. 2), both of them show considerable degrees of cytotoxicity as 35.64+8.6% and 68.5+2.24% cell viability, respectively (Fig. 4). These results suggest that the material of the dressing, in addition to the amount of silver and silver ion release, may also contribute to the cytotoxicity of a silver-containing dressing. Notably, despite Acticoat 7 eliminating bacteria most efficiently (Fig. 3a), its cytotoxicity is extremely high (17.64 + 10.27% cell viability, Fig. 4). Nevertheless, several studies have shown evidence that Acticoat is safe to use on patients [33,34]. This indicates that there is a difference between cytotoxicity effects on in-vitro
cell cultures and in-vivo models when applying silver-containing dressings. The Acticoat product might exhibit lower cytotoxicity when used on skin tissue than when used on a monolayer cell culture.
3.5 Wound healing of various silver containing ACF in infected wound tissue
Evidence indicated that the application of silver particles can promote re-epithelialization and speed up wound healing using either burn wound model or excisional wound model in mice [35,36]. In order to understand the efficacy of various silver-containing ACF applied in-vivo study, the closure area of the combination of P. aeruginosa, S. aureus and E. coli infected wound in rat model was investigated (Fig. 5 and 6). The result indicates that on the third day after applying the tested dressing, the percentages of wound closure area were 39.2+9.5% for Ag-20/ACF, 34.7+2.5% for Ag-5/ACF, 26.3+11.8% for Acticoat 7 and 21+5.6% for Actisorb silver 220. On day 6, the wound healing of Ag-20/ACF, Ag-5/ACF and Acticoat 7 are apparently better than that of Actisorb silver 220, the closure percentage of them were 67.1+2.4%, 66.0+3.1%, 60.3+5.6% and 46+1.8%, respectively. In general, Ag-20/ACF exhibited the greatest reduction of wound area in this study. However, the difference of closure area after 9 days is not significant among these tested dressings except for the control gauze.
This result indicates that Ag-20/ACF and Ag-5/ACF accelerate the early phase of infected wound healing; presumably due to its high biocompatibility to wound tissue as well as its antimicrobial activity to control infection, leading to the shorter inflammatory phase and the early entry of proliferation phase. Although in-vitro data shows that Acticoat 7 eliminates bacterial more efficiently than Ag-ACF (Fig. 3a), its cytotoxic effect may offset its wound healing efficacy in in-vivo study, resulting in less dramatic improvement for infected wound healing. On the other hand, Actisorb silver 220 exhibited a similar healing rate as the control gauze for the first 6 days. This might due to its inefficient antimicrobial activity, resulting in nearly no improvement for early phase of infected wound healing. Additionally, the healing area was not significantly different between 5/ACF and 20/ACF through entire investigated times. This suggests that Ag-5/ACF can effectively control the infection like Ag-20/ACF did in this model. This result also
supports our previously study [37] and in-vitro data in this study (Fig. 4) that silver content in silver-containing ACF only contribute a minor effect on cytotoxicity; further indicates that once the infection is under control, the healing rate is then less affected by the silver concentration of silver-containing ACF.
3.6 Histological evaluation in infected wound healing
Fig. 7 shows the histological results for hemaoxylin-eosin and Masson’s trichrome stain of infected wound treated with Ag-5/ACF and Actisorb silver 220 as mentioned above. On day 3, both Ag-5/ACF and Actisorb Silver 220-treated infected wounds presented aggregations of neutrophils and macrophages as the inflammatory response occurs. Ag-5/ACF-treated infected wound exhibited certain degree of granulation (Fig. 7a, yellow arrow). Actisorb Silver 220-treated infected wounds showed less granulation tissue formation but more neo-capillary formation (Fig. 7a, black arrow) than Ag-5/ACF. On day 6, elevated proliferation of granuloma was observed for both Ag-5/ACF and Actisorb Silver 220-treated infected wounds. Notably, Actisorb Silver 220-treated infected wounds showed less compact granulated tissue than Ag-20/ACF-treated infected wounds did. The results of Masson’s trichrome staining on day 6 (Fig. 7b) indicated that more collagen were produced on Ag-5/ACF-treated infected wound than that on Actisorb Silver 220, and in addition, collagen fibers deposit evenly on Ag-5/ACF-treated infected wound (Fig. 7b).
This result indicated that silver-containing ACF promotes the fibroblast proliferation and the deposition of collagen fiber. These effects are the consequence of the emission of far-infrared ray (FIR) from activated carbon [38]. Many studies of FIR related to wound healing have been reported. In support with our data, FIR has been shown to promote wound healing by increasing the proliferation of fibroblast as well as the secretion of collagen fiber and TGF-β in a full-thickness wound model in rat [39]. Another study indicated that FIR increases skin microcirculation in rats [40], which is believed to be the mechanism of FIR therapy for treating acute and chronic wound of trauma, surgery or diabetes mellitus. In addition, other effects of FIR such as anti-inflammation and protecting cells from apoptosis may play roles as well in promoting wound healing by FIR-emitting ACF [41,42].
3.7 Silver distribution of intact skin and blood in animal study
It has been noticed that exposure of excessive silver could result in argyria, the bluish or grey-blue discoloration of the skin [6]. Although it is not a toxic effect, argyria is undesirable and usually permanent. It has been known that long term exposure of Acticoat 7 could result in temporary discoloration of human skin. Thus, we investigated the quantity of silver deposit in intact rat skin after the application of Ag-5/ACF or Acticoat 7. After three consecutive days of the application, the silver detected in skin applied for Ag-5/ACF is 0.45 μg cm-2, whereas for Acticoat 7 is 6.47 μg cm-2
(Table 2), which is 14 times more than that of Ag-5/ACF. The silver was blocked in epidermis of intact skin apparently because there is no silver detected in serum, which means the silver did not penetrate into dermis, where plenty of capillaries are distributed. Meanwhile silver-containing dressings were applied on wound area, serum silver level increases during the applied period, but the level decreases to less than 0.1 ppm 21 days after removal of the dressing (Table 3), which is within the normal range of silver concentration in mammalian tissue [43]. This result using rat excisional wound model is consistent with the report by Moiemen et.al, which shows serum silver level in follow-up patients decreases with the median half-life of silver elimination as about 45 days [44]. Presumably, majority of the serum silver is eliminated through biliary excretion to the feces as several previous studies reported [45,46].
4 Conclusions
The various silver-containing ACF were produced by Bio-medical Carbon Technology exhibit benefits for medical application. All tested silver-containing ACF performed high biocompatibility with sufficient antimicrobial activity in-vitro. An in-vivo study further indicated that various produced Ag-ACF can promote infected wound healing in early phase compared to other commercial silver-containing dressing and promoting granulation and collagen deposition. Lastly, applying silver-containing dressing to a wound would temporarily increase the serum silver level. Nevertheless, the serum silver is eliminated after the removal of the dressing, falling to a subtle level eventually.
References
1. Poole MD. Are we facing the end of the antibiotic era? Ear Nose Throat J. 1993;72:433.
2. Baron EJ, Tenover FC. Methicillin-resistant Staphylococcus aureus diagnostics: state of the art. Expert Opin Med Diagn. 2012;6:585-92.
3. Martins A, Hunyadi A, Amaral L. Mechanisms of resistance in bacteria: an evolutionary approach. Open Microbiol J. 2013;7:53-8.
4. Aziz Z, Abu SF, Chong NJ. A systematic review of silver-containing dressings and topical silver agents (used with dressings) for burn wounds. Burns. 2012;38:307-18.
5. Singh M, Singh S, Prasad S, Gambhir IS. Nanotechnology in medicine and antibacterial effect of silver nanoparticles. Dig J Nanomater Bios. 2008;3:115-22.
6. Madhumathi K , Sudheesh Kumar PT, Abhilash S, Sreeja V, Tamura H, Manzoor K, Nair SV, Jayakumar R. Development of novel chitin/nanosilver composite scaffolds for wound dressing applications. J Mater Sci Mater Med. 2010;21:807-13.
7. Gaisford S, Beezer AE, Bishop AH, Walker M, Parsons D. An in vitro method for the quantitative determination of the antimicrobial efficacy of silver-containing wound dressings. Int J Pharm. 2009;366:111-6.
8. Wilkinson LJ, White RJ, Chipman JK. Silver and nanoparticles of silver in wound dressings: a review of efficacy and safety. J Wound Care. 2011;20:543-9.
9. Percival SL, Bowler PG, Russell D. Bacterial resistance to silver in wound care. J Hosp Infect. 2005;60:1-7.
10. Ip M, Lui SL, Poon VK, Lung I, Burd A. Antimicrobial activities of silver dressings: an in vitro comparison. J Med Microbiol. 2006;55:59-63.
11. Bolton L. Are silver products safe and effective for chronic wound management? J Wound Ostomy Continence Nurs. 2006;33:469-77.
12. Williams C. Role of CarboFlex in the nursing management of wound odour. Br J Nurs. 2001;10:122-5.
13. Morris C. Wound odour: principles of management and the use of CliniSorb. Br J Nurs. 2008;17:S40-2.
14. Lee J, Kim J, Hyeon T. Recent progress in the synthesis of porous carbon caterials. Adv Mater. 2006;18:2073-94.
15. Lin JH, Ko TH, Lin YH, Pan CK. Various treated conditions to prepare porous activated carbon fiber for application in supercapacitor electrodes. Energy Fuels. 2009;23:4668-77.
16.Huang WY , Yeh CL, Lin JH, Yang JS, Ko TH, Lin YH. Development of fibroblast culture in three-dimensional activated carbon fiber-based scaffold for wound healing. J Mater Sci Mater Med. 2012;23:1465-78.
17. Lin YH, Lin JH, Peng SF, Yeh CL, Chen WC, Chang TL, Liu MJ, Lai CH. Multifunctional gentamicin supplementation of poly(γ-glutamic acid)-based hydrogels for wound dressing application. J Appl Polym Sci. 2011;120:1057-68.
18. Lipp C, Kirker K, Agostinho A, James G, Stewart P. Testing wound dressings using an in vitro wound model. J Wound Care. 2010;19:220-6.
19. Lin YH, Chiou SF, Lai CH, Tsai SC, Chou CW, Peng SF, He ZS. Formulation and evaluation of water-in-oil amoxicillin-loaded nanoemulsions using for Helicobacter pylori eradication. Process Biochem. 2012;47:1469-78.
20. Chang CH, Huang WY, Lai CH, Hsu YM, Yao YH, Chen TY, Wu JY, Peng SF, Lin YH. Development of novel nanoparticles shelled with heparin for berberine delivery to treat Helicobacter pylor. Acta Biomater. 2011;7:593-603.
21. Lin YH, Tsai SC, Lai CH, Lee CH, He ZS, Tseng GC. Genipin-cross-linked fucose-chitosan/heparin nanoparticles for the eradication of Helicobacter pylori. Biomaterials. 2013;34:4466-79.
22.Lee WR , Park JH, Kim KH, Kim SJ, Park DH, Chae MH, Suh SH, Jeong SW, Park KK. The biological effects of topical alginate treatment in an animal model of skin wound healing. Wound Repair Regen. 2009;17:505-10.
23. Balakrishnan B, Mohanty M, Fernandez AC, Mohanan PV, Jayakrishnan A. Evaluation of the effect of incorporation of dibutyryl cyclic adenosine monophosphate in an in situ-forming hydrogel wound dressing based on oxidized alginate and gelatin. Biomaterials. 2006;27:1355-61.
in medical devices. Adv Pharmacol Sci. 2010;2010:910686.
25. Song X, Gunawan P, Jiang R, Leong SS, Wang K, Xu R. Surface activated carbon nanospheres for fast adsorption of silver ions from aqueous solutions. J Hazard Mater. 2011;194:162-8. 26. Moreno-Piraján JC, Giraldo L. Heavy metal ions adsorption from wastewater using activated
carbon from orange peel. E-J CHEM. 2012;9:926-37.
27. Walker M, Cochrane CA, Bowler PG, Parsons D, Bradshaw P. Silver deposition and tissue staining associated with wound dressings containing silver. Ostomy Wound Manage. 2006;52:42-50.
28. Peel RG, Benedek A. Biodegradation and adsorption within activated carbon adsorbers. J Water Pollut Control. 1983;55:1168-73.
29. Suffet IH. National academy of sciences report--an evaluation of activated carbon for drinking water treatment. J Environ Pathol Toxicol Oncol. 1987;7:9-32.
30. Matsunaga T, Nakasono S, Kitajima Y, Horiguchi K. Electrochemical disinfection of bacteria in drinking water using activated carbon fibers. Biotechnol Bioeng. 1994;43:429-33.
31. Poon VK, Burd A. In vitro cytotoxity of silver: implication for clinical wound care. Burns. 2004;30:140-7.
32. Cho Lee AR, Leem H, Lee J, Park KC. Reversal of silver sulfadiazine-impaired wound healing by epidermal growth factor. Biomaterials. 2005;26:4670-6.
33. Khundkar R, Malic C, Burge T. Use of Acticoat dressings in burns: what is the evidence? Burns. 2010;36:751-8.
34.Muangman P , Chuntrasakul C, Silthram S, Suvanchote S, Benjathanung R, Kittidacha S, Rueksomtawin S. Comparison of efficacy of 1% silver sulfadiazine and Acticoat for treatment of partial-thickness burn wounds. J Med Assoc Thai. 2006;89:953-8.
35.Tian J , Wong KK, Ho CM, Lok CN, Yu WY, Che CM, Chiu JF, Tam PK. Topical delivery of silver nanoparticles promotes wound healing. ChemMedChem. 2007;2:129-36.
36.Liu X , Lee PY, Ho CM, Lui VC, Chen Y, Che CM, Tam PK, Wong KK. Silver nanoparticles mediate differential responses in keratinocytes and fibroblasts during skin wound healing. ChemMedChem. 2010;5:468-75.
37. Lin YH, Lin JH, Wang SH, Ko TH, Tseng GC. Evaluation of silver-containing activated carbon fiber for wound healing study: in vitro and in vivo. J Biomed Mater Res B Appl Biomater. 2012;100:2288-96.
38. Frost RL, Cash GA, Kloprogge T. “Rocky Mountain leather”, sepiolite and attapulgite-an infrared emission spectroscopic study. Vib Spectrosc. 1998;16: 173-184.
39.Toyokawa H , Matsui Y, Uhara J, Tsuchiya H, Teshima S, Nakanishi H, Kwon AH, Azuma Y, Nagaoka T, Ogawa T, Kamiyama Y. Promotive effects of far-infrared ray on full-thickness skin wound healing in rats. Exp Biol Med (Maywood). 2003;228:724-9.
40. Yu SY, Chiu JH, Yang SD, Hsu YC, Lui WY, Wu CW. Biological effect of far-infrared therapy on increasing skin microcirculation in rats. Photodermatol Photoimmunol Photomed. 2006;22:78-86.
41.Lin CC , Liu XM, Peyton K, Wang H, Yang WC, Lin SJ, Durante W. Far infrared therapy inhibits vascular endothelial inflammation via the induction of heme oxygenase-1. Arterioscler Thromb Vasc Biol. 2008;28:739-45.
42. Tu YP, Chen SC, Liu YH, Chen CF, Hour TC. Postconditioning with far-infrared irradiation increases heme oxygenase-1 expression and protects against ischemia/reperfusion injury in rat testis. Life Sci. 2013;92:35-41.
43. Fuller FW, Parrish M, Nance FC. A review of the dosimetry of 1% silver sulfadiazine cream in burn wound treatment. J Burn Care Rehabil. 1994;15: 213-23.
44. Moiemen NS, Shale E, Drysdale KJ, Smith G, Wilson YT, Papini R. Acticoat dressings and major burns: systemic silver absorption. Burns. 2011;37: 27-35.
45. Gregus Z, Klaassen CD. Disposition of metals in rats: a comparative study of fecal, urinary, and biliary excretion and tissue distribution of eighteen metals. Toxicol Appl Pharmacol. 1986;85:24-38.
46.Loeschner K , Hadrup N, Qvortrup K, Larsen A, Gao X, Vogel U, Mortensen A, Lam HR, Larsen EH. Distribution of silver in rats following 28 days of repeated oral exposure to silver nanoparticles or silver acetate. Part Fibre Toxicol. 2011;8:doi: 10.1186/1743-8977-8-18.
Tables
Table 1. The inhibition of bacterial growth (%) of the various Ag-ACF dressing (n=5)
Table 2. Silver concentration of intact skin and blood after applying distinct silver-containing dressing
Table 3. Silver concentration of blood after applying Ag-ACF dressing (Bio-Medical Carbon Technology) on wound area
Blood silver content (ppm) Applied after 5 day 21 day after removal of dressing
Control (without sample) 0 0
Ag-5/ACF 0.97 0.09
Ag-10/ACF 0.43 0.09
Ag-20/ACF 0.25 0.07
Bacterial Growth Inhibition (%)
Samples Escherichia coli Staphyllococcus aureus Pseudomonas aeruginosa
Ag-20/ACF 91.32 + 11.24 89.56 + 9.72 92.17 + 9.53 Ag-10/ACF 88.73 + 9.86 89.17 + 10.3 91.48 + 11.42 Ag-5/ACF 90.42 + 11.06 88.77 + 8.44 91.29 + 7.59 Ag-1/ACF 89.23 + 8.54 87.42 + 9.72 88.55 + 9.98 ACF 32.13 + 10.42 39.42 + 7.69 33.54 + 8.24 Gauze 10.23 + 5.23 11.52 + 6.41 10.32 + 5.93 Silver content Skin (μg cm-2) Blood (ppm)
Control (without sample) 0 0
Ag-5/ACF (Bio-Medical Carbon Technology) 0.45 0
Figure Captions
Fig. 1 Scanning electronic microscope micrographs of the Ag-1/ACF, Ag-5/ACF, Ag-10/ACF and Ag-20/ACF.
Fig. 2 The release of silver ion from silver-containing dressings in distilled water for 24 hrs.
Fig. 3 Antibacterial activity of silver-containing dressings. (a) The colony-forming unit (CFU) of P. aeruginosa after treated with silver-containing dressings within 4 hrs; (b) The growth inhibition of E. coli, S. aureus and P. aeruginosa after treated with various Ag-ACF for 24 hrs (n = 5).
Fig. 4 Cell viability after treatment with silver-containing dressings for 24 hrs (n = 6).
Fig. 5 Representative photographs of the infected wound on days 3, 6, 9, 12, and 15 postoperative with the treatment of indicated silver-containing dressings.
Fig. 6 The percentage of infected wound closure treated with silver-containing dressings (n=5). Fig. 7 Histologic image of the infected wound treated with Ag-5/ACF and Actisorb Silver 220 on
days 3 and 6 by hematoxylin-eosin staining (a) and days 6 by Masson’s trichrome staining (b).
Fig. 3a