I
NTERESTING
I
MAGE
Lower Neck Neurilemmoma Can Masquerade as Lymph Node
Metastasis on FDG PET/CT in Patient With Nasopharyngeal
Carcinoma
Te-Chun Hsieh, MD,*‡ Yu-Chin Wu, MD,*¶ Cheng-Nan Hsu, MD,** Chun-Fan Yang, MD,†
Kuo-Yang Yen, BS,*‡ Chia-Hung Kao, MD,*§ and Shung-Shung Sun, MD*‡
Abstract: A 50-year-old man with nasopharyngeal carcinoma was suspected
to have progressive malignant disease because of an unexpected FDG-avid finding that was suspected to be neck lymph node metastasis on the follow-up FDG PET/CT after the definite anticancer therapy. However, after carefully correlating with the relevant MRI findings because of the atypical depth of the neck lesion and possible connection with the spinal nerve, the FDG-avid finding was reconsidered to be a tumor that originated from the nerve. The subsequent histologic examination confirmed the diagnosis of neurilemmoma.
Key Words: neurilemmoma, FDG PET/CT, MRI, nasopharyngeal
carcinoma, lymph node metastasis, head and neck (Clin Nucl Med 2011;36: e217– e219)
REFERENCES
1. Halac M, Cnaral F, Sait S, et al. FDG PET/CT findings in recurrent malignant schwannoma. Clin Nucl Med. 2008;33:172–174.
2. Komatsu D, Koide N, Hiraga R, et al. Gastric schwannoma exhibiting increased fluorodeoxyglucose uptake. Gastric Cancer. 2009;12:225–228. 3. Akin M, Bozkirli B, Leventoglu S, et al. Liver schwannoma incidentally
discovered in a patient with breast cancer. Bratisl Lek Listy. 2009;110:298 – 300.
4. Nguyen BD. Lower extremity schwannoma: F-18 FDG PET and MR dem-onstration. Clin Nucl Med. 2005;30:525–527.
5. Malone JP, Lee WJ, Levin RJ. Clinical characteristics and treatment outcome for nonvestibular schwannomas of the head and neck. Am J Otolaryngol. 2005;26:108 –112.
6. Zhang H, Cai C, Wang S, et al. Extracranial head and neck schwannomas: a clinical analysis of 33 patients. Laryngoscope. 2007;117:278 –281. 7. Anil G, Tan TY. Imaging characteristics of schwannoma of the cervical
sympathetic chain: a review of 12 cases. Am J Neuroradiol. 2010;31:1408 – 1412.
8. Kang GC, Soo KC, Lim DT. Extracranial non-vestibular head and neck schwannomas: a ten-year experience. Ann Acad Med Singapore. 2007;36: 233–238.
9. Casserly P, Kiely P, Fenton JE. Cervical sympathetic chain schwannoma masquerading as a carotid body tumour with a postoperative complication of first-bite syndrome. Eur Arch Otorhinolaryngol. 2009;266:1659 –1662. 10. Wippold FJ II, Lammle M, Anatelli F, et al. Neuropathology for the
neuro-radiologist: palisades and pseudopalisades. Am J Neuroradiol. 2006;27:2037– 2041.
11. Ahmed AR, Watanabe H, Aoki J, et al. Schwannoma of the extremities: the role of PET in preoperative planning. Eur J Nucl Med. 2001;28:1541–1551. 12. Biswas D, Marnane CN, Mal R, et al. Extracranial head and neck
schwan-nomas—a 10-year review. Auris Nasus Larynx. 2007;34:353–359. 13. Beaulieu S, Rubin B, Djang D, et al. Positron emission tomography of
schwannomas: emphasizing its potential in preoperative planning. Am J
Roentgenol. 2004;182:971–974.
14. Hamada K, Ueda T, Higuchi I, et al. Peripheral nerve schwannoma: two cases exhibiting increased FDG uptake in early and delayed PET imaging. Skeletal
Radiol. 2005;34:52–57.
15. Matsuki A, Kosugi S, Kanda T, et al. Schwannoma of the esophagus: a case exhibiting high 18F-fluorodeoxyglucose uptake in positron emission tomog-raphy imaging. Dis Esophagus. 2009;22:E6 –E10.
16. Nakamura R, Ishikawa S, Sakai M, et al. Increased fluorodeoxyglucose-uptake in positron emission tomography with an endobronchial schwannoma occluding the left main stem bronchus. J Thorac Oncol. 2009;4:1183–1184. 17. Nishio M, Tamaki T, Hara M, et al. Appendiceal schwannoma detected by
FDG-PET/CT. Clin Nucl Med. 2010;35:379 –380.
18. Wu YC, Hsieh TC, Kao CH, et al. Simultaneous rectal schwannoma and prostatic adenocarcinoma detected on FDG PET/CT. Clin Nucl Med. In press. 19. Wang CL, Neville AM, Wong TZ, et al. Colonic schwannoma visualized on
FDG PET/CT. Clin Nucl Med. 2010;35:181–183.
20. Som PM, Sacher M, Stollman AL, et al. Common tumors of the parapharyn-geal space: refined imaging diagnosis. Radiology. 1988;169:81– 85. 21. Wax MK, Shiley SG, Robinson JL, et al. Cervical sympathetic chain
schwan-noma. Laryngoscope. 2004;114:2210 –2213.
22. de Araujo CE, Ramos DM, Moyses RA, et al. Neck nerve trunks schwanno-mas: clinical features and postoperative neurologic outcome. Laryngoscope. 2008;118:1579 –1582.
Received for publication March 8, 2011; revision accepted June 3, 2011. From the Departments of *Nuclear Medicine and PET Center, **Radiology, and
†Pathology, China Medical University Hospital, Taichung, Taiwan; ‡Depart-ment of Biomedical Imaging and Radiological Science, and §School of Medicine, China Medical University, Taichung, Taiwan; and ¶Department of Nuclear Medicine, National Taiwan University Hospital Hsin-Chu Branch, Hsinchu City, Taiwan.
Conflicts of interest and sources of funding: none declared.
Reprints: Shung-Shung Sun, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Rd, Taichung 404, Taiwan. E-mail: [email protected] and Yu-Chin Wu, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Rd, Taichung 404, Taiwan. E-mail: [email protected]. Copyright © 2011 by Lippincott Williams & Wilkins
ISSN: 0363-9762/11/3612-0217
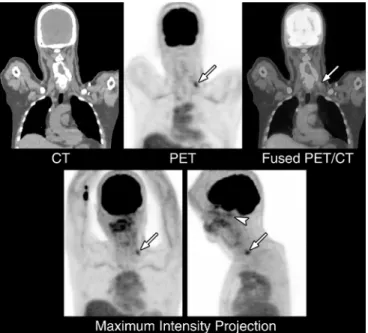
FIGURE 2. The FDG PET/CT demonstrated mildly increased
radioactivity in the nasopharyngeal region (arrowhead) that was probably due to the inflammation. However, there was an unexpected focus with intense radioactivity (SUVmax: 3.6) in the left lower neck region (arrows). Initially, the finding was suspected as lymph node metastasis that would be regarded as progression of malignancy. However after carefully examining the anatomic reference on CT component of FDG PET/CT, the lesion seemed unusually deep and possibly within the left scalene muscle.
FIGURE 1. A 50-year-old man was diagnosed with
nasopharyngeal carcinoma. The initial presentation on the magnetic resonance imaging (MRI) with gadolinium
enhancement revealed an enhanced bulging mass in the left nasopharynx with adjacent skull-base invasion (asterisk in panel A, T1-weighted fast spoiled gradient echo image with gadolinium enhancement) without locoregional lymph node or distant metastasis. After completing the concurrent chemoradiation therapy, several studies were performed for restaging, including the endoscopic examination, MRI, and 2-关18F兴fluoro-2-deoxy-D-glucose positron emission
tomography/computed tomography (FDG PET/CT). The follow-up MRI revealed disappearance of the previous tumor in the left nasopharynx (panel B, T1-weighted fast spin-echo image with gadolinium enhancement) in accordance with the normal endoscopic finding, suggesting good response to the anticancer therapy.
FIGURE 3. After reexamining the aforementioned follow-up
MRI, we noticed a small, well-circumscribed, hyperintense lesion with relatively central hypointensity in the left lower neck region on the T2-weighted image with fat suppression (arrow). In addition, the location of this lesion seemed connecting with the root of left sixth cervical spinal nerve. The image features revealed that the lesion might originate from the spinal nerve, and most frequently, it might be a periphery nerve sheath tumor such as neurilemmoma.
Hsieh et al Clinical Nuclear Medicine • Volume 36, Number 12, December 2011
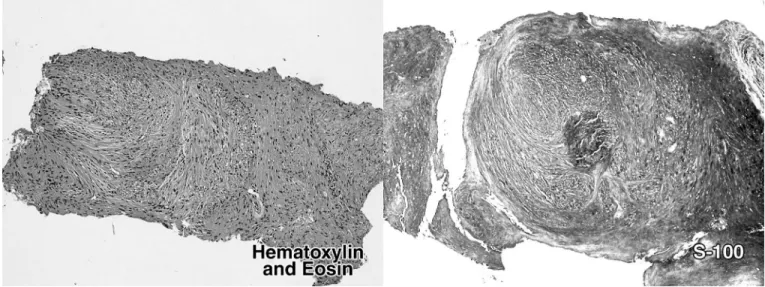
FIGURE 4. This patient then underwent ultrasonography-guided needle biopsy for pathologic confirmation. The histologic
findings revealed spindle tumor cells arranged in fascicles with focal nuclear palisading (hematoxylin and eosin stain, 100⫻) and the immunohistochemical study showed positive staining for S-100 protein (100⫻), which were characteristics for neurilemmoma and confirmed the diagnosis. Neurilemmoma is a benign, slow-growing, encapsulated nerve sheath tumor derived from Schwann cells and is most commonly observed in the extremities and head and neck regions.1,2It is also known
as schwannoma, neurinoma, neuroma, and perineural fibroblastoma and is the most common tumor of the peripheral nervous system.1,3–5Neurilemmoma can originate from virtually any peripheral nerve, except the olfactory and optic nerves
that lack Schwann cells.5,6This tumor occurs at all ages, but is most commonly found in individuals between the second and
fifth decades.1Neurilemmoma in the parapharyngeal space with the vagus nerve or the cervical sympathetic chain serving as
the nerve of origin is the second most common site of head and neck region after the acoustic neuroma in the vestibular region.5A neurilemmoma in the neck region may be difficult to differentiate from a solitary metastatic node from an
unknown or known primary cancer without periadenitis or extranodal extension of disease.7In addition, neurilemmoma may
mimic other diseases in the head and neck region, such as thyroglossal duct cyst, branchial arch cyst, carotid body tumor, thyroid cyst/nodule, thyroid carcinoma, parotid cyst/tumor, paraganglioma, chemodectoma, aneurysm of internal carotid artery, lipoma, meningioma, and rhabdomyoma.6,8,9Characteristic histologic features of neurilemmomas include palisade
arrangement of nuclei and Verocay bodies.10The encapsulation and the presence of 2 components, a highly ordered cellular
component (Antoni A area) and a looser myxoid component (Antoni B area), distinguish neurilemmoma from
neurofibroma.11Immunohistochemical studies with S-100 stain may be helpful for diagnosis of neurilemmoma.12High FDG
uptake of neurilemmomas has been reported in those most common sites of extremities4,13and head and neck regions14as
well as other uncommon sites such as the esophagus,15stomach,2bronchus,16liver,3appendix,17and colon.18,19Therefore,
it may be difficult to distinguish a neurilemmoma from malignant peripheral neural sheath tumor or other malignancies based on the FDG PET/CT findings only. MRI may be helpful for providing the anatomic details and characteristic findings of neurilemmoma. Typical MRI findings of neurilemmoma manifest low-to-intermediate signal intensity on T1-weighted images, heterogeneous hyperintensity on T2-weighted images, and intense heterogeneous postgadolinium enhancement.7,20Similar
to most neurogenic tumors of the head and neck region, the majority of neurilemmomas present as asymptomatic head and neck masses at the time of presentation.21The treatment of neurilemmoma is surgery, but may be left for those with growing
potential and compression symptoms,22because there may be a considerable morbidity because of surgical treatment in
some patients.12The current case reveals an incidental finding of focal FDG-avid lesion that masquerades neck lymph node
metastasis in a patient with nasopharyngeal carcinoma. However, the unusual depth of the neck lesion on the CT component of FDG PET/CT is an important clue for differential diagnoses and may suggest etiologies other than lymph node metastasis. The concurrent MRI provides further evidences of the characteristic features and anatomic details that strongly suggest the origin from the nerve. Therefore, it is important that when interpreting an FDG PET/CT scan for a known malignancy, the clinicians should keep in mind that any FDG-avid lesion presenting with an atypical anatomic location relevant to the etiology of known malignancy should not be simply regarded as a variant presentation of malignancy. Other more probable
explanation should be considered and examined, so that the patient will not be treated improperly.
Clinical Nuclear Medicine • Volume 36, Number 12, December 2011 Lower Neck Neurilemmoma