Inhibition of human alcohol and aldehyde dehydrogenases by aspirin and salicylate: Assessment of the effects on first-pass metabolism of ethanol
Shou-Lun Leea,*, Yung-Pin Leeb, Min-Li Wub, Yu-Chou Chib, Chiu-Ming Liub, Ching-Long Laic, Shih-Jiun Yinb
aDepartment of Biological Science and Technology, China Medical University, 91 Hsueh-Shih Road, Taichung 40402, Taiwan
bDepartment of Biochemistry, National Defense Medical Center, 161 Minchuan East Road Section 6, Taipei 11453, Taiwan
cDepartment of Nursing, Chang Gung University of Science and Technology, 261 Wenhwa 1st Road, Kweishan Township, Taoyuan 33303, Taiwan
*Corresponding author. Tel.: +886 4 22053366x2526, Fax.: +886 4 22051507
E-mail addresses: [email protected] (S-L Lee), [email protected] (Y-P Lee), [email protected] (M-L Wu), [email protected] (Y-C Chi),
[email protected] (C-M Liu), [email protected] (C-L Lai), [email protected] (S-J Yin) 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18
Abstract
Previous studies have reported that aspirin significantly reduced the first-pass metabolism (FPM) of ethanol in humans thereby increasing adverse effects of alcohol. The underlying causes, however, remain poorly understood. Alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH), principal enzymes responsible for metabolism of ethanol, are complex enzyme families that exhibit functional polymorphisms among ethnic groups and distinct tissue distributions. We investigated the inhibitions by aspirin and its major metabolite salicylate of ethanol oxidation by recombinant human ADH1A, ADH1B1, ADH1B2, ADH1B3, ADH1C1, ADH1C2, ADH2, and ADH4, and acetaldehyde oxidation by ALDH1A1 and ALDH2 at pH 7.5 and a cytoplasmic NAD+ concentration. Competitive inhibition pattern was found to be a predominant type among the ADHs and ALDHs studied, although noncompetitive and uncompetitive inhibitions were also detected in a few cases. The inhibition constants of salicylate for the ADHs and ALDHs were considerably lower than that of aspirin with the exception of ADH1A that can be ascribed to a
substitution of Ala-93 at the bottom of substrate pocket as revealed by molecular dockings. Kinetic inhibition equation-based simulations show that at higher therapeutic levels of blood plasma salicylate (1.5 mM), the decrease of activities at 2–10 mM ethanol for
ADH1A/ADH2 and ADH1B2/ADH1B3 are predicted to be 75–86% and 31–52%,
respectively; and that for ALDH1A1 and ALDH2 at 10–50 μM acetaldehyde, 62–73%. Our findings suggest that salicylate may substantially inhibit hepatic FPM of alcohol at both the ADH and ALDH steps when concurrent intaking aspirin.
Keywords: Aspirin, Salicylate, Alcohol dehydrogenase (ADH), Aldehyde dehydrogenase (ALDH), Inhibition kinetics, Alcohol first-pass metabolism
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
1. Introduction
Aspirin is one of the most widely prescribed analgesic-antipyretic and antiinflammatory agents. Because the drug is so generally available, use of aspirin and alcoholic beverages are commonly associated [1,2]. It has been shown that aspirin increases blood ethanol
concentrations by inhibition of first-pass metabolism (FPM) of ethanol [3–5], thereby increasing the adverse effects of alcohol such as impaired driving. The major sites of ethanol FPM include the stomach, small intestine, and liver, but their relative contributions to alcohol metabolism remain controversial [3,6–8]. Several factors may affect the FPM of ethanol, such as food consumption, concentration of alcoholic beverages, genetic
polymorphism of alcohol-metabolizing enzymes, medications that interfere with activity of the metabolizing enzymes or with absorption of alcohol [3,6,9].
Alcohol dehydrogenase (ADH) and aldehyde dehydrogenase (ALDH) are principal enzymes responsible for metabolism of ethanol in humans, catalyzing conversion of ethanol to acetaldehyde and then to acetate, respectively [8,9]. Both enzymes exhibit functional polymorphisms among racial populations and tissue–specific distributions [10–12]. Human ADH family members have been categorized into five classes on the basis of protein sequence and gene organization, electrophoretic, kinetic and immunochemical features [13– 15]. The class I ADH contains multiple forms, that is, ADH1A (previously denoted αα), ADH1B (ββ), and ADH1C (γγ). The classes II to IV ADHs contain a single form each, that is, ADH2 (ππ), ADH3 (χχ), and ADH4 (μμ or σσ), respectively. ADH1B and ADH1C exhibit allelic variations [11,12]. ADH1B*1 (encoding the β1 subunit polypeptide) and
ADH1B*2 (encoding β2 subunit) are predominant among Caucasians and East Asians, respectively; ADH1B*3 (encoding β3 subunit) is found exclusively in Africans and some tribes of American Indians. ADH1C*1 (encoding γ1 subunit) and ADH1C*2 (encoding γ2 subunit) are approximately equally distributed among Caucasians and American Indians, but 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
the former is highly prevalent among the East Asian and African populations. Currently, class V ADH is the only family member unavailable for catalytic function due to its extreme instability [16]. All three class I isozymes, ADH2 and ADH3 are expressed in human adult liver [12,17], while ADH4 and ADH1C are detected in the stomach [18], and ADH2 and ADH1C are detected in the small intestine [19].
In the human ALDH superfamily [20,21], class I ALDH1A1 and class II ALDH2 are predominantly expressed in human liver [12] and both isozymes are detected in the gastrointestinal tract [18,19], whereas class III ALDH3A1 is a major form found in the stomach [18]. Mitochondrial ALDH2 is the primary isozyme for oxidation of acetaldehyde derived from ethanol due to its submicromolar Km and high catalytic efficiency, whereas cytoplasmic ALDH1A1 with micromolar Km also contributes to oxidation of the
acetaldehyde, particularly in individuals who lack active ALDH2 [12,22]. About 40% of East Asians are deficient in ALDH2 activity as a result of the dominant negative variant allele ALDH2*2 [10,23]. This deficiency has been attributed to protection against
development of alcoholism [11,24], but it is a risk factor for alcohol-related diseases such as esophageal cancer [25,26].
After oral administration, aspirin is rapidly broken down by liver, erythrocyte, and plasma esterases to salicylate [27,28]. Lieber and colleagues [4,5] have reported that aspirin (1 g taken with a standard breakfast) significantly increased alcohol bioavailability (at a test dose 0.3 g/kg of ethanol one hour after the beginning of the meal) with a concomitant 39% decrease in the FMP of alcohol whereas it did not significantly influence the gastric emptying. However, there has been lacking a systematic investigation with regard to inhibitions by aspirin and salicylate of human ADHs and ALDHs in the context of FPM of ethanol. We report herein, the inhibition types/constants and the kinetic equation-based 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
simulation of human ADH family members and the pertinent ALDH isozymes, at a near physiological coenzyme concentration and pH, under pharmacologically relevant
concentration ranges of ethanol/acetaldehyde and the interacting drugs. 2. Methods
2.1. Expression and purification of human ADH and ALDH
The expression of recombinant enzymes in Escherichia coli and purification to apparent homogeneity for human ADH1A, ADH1B1, ADH1B2, ADH1B3, ADH1C1, ADH1C2, ADH2, ADH3, ADH4, and for human ALDH1A1, ALDH2, ALDH3A1 were carried out as described previously [6,15,29]. All of the isolated recombinant enzyme forms exhibited a single coomassie blue-staining protein band with molecular masses of 40 kDa, 55 kDa, and 54 kDa for ADHs, ALDH1A1/2, and ALDH3A1, respectively, on sodium dodecyl sulfate– polyacrylamide gel electrophoresis. Protein concentration was determined by the Lowry method [30] using bovine serum albumin as the standard.
2.2. Kinetic analysis
Kinetic studies for ADH and ALDH were performed in 0.1 M sodium phosphate at pH 7.5 and 25 °C, containing 0.5 mM NAD+, 1 mM EDTA (only for ALDH assay), and varied concentrations of substrate and inhibitor. The cytosolic NAD+ concentration in rat
hepatocytes is reported to be ca. 0.5 mM [31]. Stock solutions of aspirin and salicylate were prepared in 0.1 M sodium phosphate, pH 7.5 and 25 °C. The aspirin stock was freshly prepared every 3 h during kinetic experiments to keep minimal hydrolysis (less than 3%) to salicylate. The concentration of hydrolytic product salicylate in aspirin stock solution following storage was determined fluorometrically as described previously [28]. The
enzyme activity was determined by monitoring the production of NADH at 340 nm using an absorption coefficient of 6.22 mM-1cm-1 for ADH and ALDH assay (unless otherwise indicated), or at 460 nm for emission of the fluorescence for the assay of ADH3 (excitation at 340 nm), ALDH1A1 and ALDH2 (excitation at 360 nm for the latter two to avoid 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
interference of salicylate). Preparation of formaldehyde and calculation of the concentration of S-hydroxymethylglutathione from the equilibrium constants were performed as described previously [32]. Acetaldehyde and benzaldehyde were redistilled before use. The reaction was initiated with addition of the enzyme. Enzyme activity units (U) are expressed as micromoles of NADH formed per minute. Steady-state kinetic data were analyzed by nonlinear least-squares regression using the Cleland programs of HYPER, COMP,
NONCOMP, and UNCOMP [33]. Initial velocity data were fitted with HYPER program to the Michaelis–Menten equation
v = (Vmax × S)/(Km + S) (1)
The data from dead-end inhibition studies were fitted with the following linear inhibition equations, that is, the COMP program for competitive inhibition, the NONCOMP for noncompetitive inhibition, and the UNCOMP for uncompetitive inhibition, respectively.
v = (Vmax × S)/[(Km (1 + I/Kis) + S] (2)
v = (Vmax × S)/[(Km (1 + I/Kis) + S (1 + I/Kii)] (3)
v = (Vmax × S)/[(Km + S (1 + I/Kii)] (4)
where Vmax is the maximal velocity, S is the substrate concentration, Km is the Michaelis constant, I is the inhibitor concentration, and Kis and Kii are the slope and intercept inhibition constants, respectively. The type of inhibition was determined by evaluating the standard errors of the kinetic constants and the residual variance for the equation that best fit the data [33]. In cases where the intercepts and slopes did not vary greatly with inhibitor
concentration, Student’s t-tests were applied to determine if they were significantly different. The kinetic experiments were performed in duplicate with five substrate
concentrations usually ranging from 0.5 to 5 Km and five (including one for control, I = 0) inhibitor concentrations ranging from 0.2 to 2 Ki when applicable. Values represent means ± standard error of the mean (SEM). Standard errors of the fits to the appropriate computer 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
programs were less than 10% of the values for Km and Vmax and less than 16% of those for the inhibition constants, indicating good precision.
2.3. Molecular docking
Salicylate and aspirin were docked, respectively, into the active sites of the X-ray structures of human ADH1A [PDB ID:1HSO], ADH1B1 [PDB ID:1DEH], ADH1C2 [PDB ID:1HT0], ADH2 [PDB ID:3COS], ADH4 [PDB ID:1D1S], and ALDH2 [PDB ID:1O01], all
complexes with NAD+, using AutoDock4 with the built-in setting of parameters [34]. The illustrations were generated using PyMOL v1.5 for Linux/Ubuntu (Schrodinger, LLC, New York).
3. Results
3.1. Inhibition type
Inhibition patterns and the corresponding kinetic constants of aspirin and salicylate against ethanol oxidation with human ADH family are shown in Table 1. The inhibition against oxidation of S-hydroxymethylglutathione, instead of ethanol, for class III ADH3 was studied because ADH3 is nearly unsaturable with ethanol, S0.5 = 3.4 M [32]. Class I ADH1A, ADH1B1, ADH1C1, ADH1C2, class II ADH2, class III ADH3, and class IV ADH4 exhibited competitive inhibition for salicylate with a wide range of slope inhibition constants, that is, 0.17 to 6.8 mM, ADH1A being the lowest and ADH4 the highest; by contrast, the slope inhibition constants of aspirin were 12 to 19-fold higher (except 3.5 to 4.3-fold higher with ADH1A and ADH1C1) than the corresponding constants of salicylate. No detectable inhibition of aspirin was found with ADH1B1. Notably, class I allozymes ADH1B2 and ADH1B3 exhibited noncompetitive inhibition with a smaller range of the slope and intercept constants for salicylate (1.4 to 3.5 mM) but much greater for the aspirin (28 to 42 mM).
Table 2 shows that salicylate (Kis = 0.53 mM) and aspirin (Kis = 12 mM) were a competitive 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
inhibitor with respect to acetaldehyde for class I ALDH1A1; and that for class II ALDH2, salicyalte was a noncompetitive inhibitor with similar Kis and Kii (0.37 to 0.55 mM) whereas aspirin, an uncompetitive inhibitor (Kii = 3.9 mM). In contrast, no detectable inhibition of either salicylate or aspirin was observed with class III ALDH3A1, using benzaldehyde instead of acetaldehyde as substrate, the latter has a much higher Km (75 mM) [35]. Thus, ALDH3A1 contributes negligibly to metabolism of the ethanol-derived acetaldehyde in vivo [12,35].
3.2. Metabolic interaction
The interactions between salicylate, up to 2 mM, and the oxidation of ethanol, up to 50 mM, for ADH1A, ADH1B1, ADH2, and the oxidation of acetaldehyde, up to 0.5 mM, for
ALDH1A1 and ALDH2, at a cytosolic concentration of 0.5 mM NAD+ are shown in Figs. 1 and 2, respectively. Interaction with aspirin for ADH1A (Kis = 0.59 mM, lowest among the ADH and ALDH isozymes studied) is also presented (Fig. 1a). The ADH and ALDH forms exhibiting slope inhibition constants lower than 0.6 mM, except ADH1B1 (Kis = 1.4 mM,
Km = 0.013 mM), were chosen for illustration of the drug inhibition in a three-dimensional way. In the absence of inhibitor (I = 0), enzyme activities increase with increasing substrate concentration, that is, the substrate saturation curves reflect the Michaelis constants of the enzymes. The enzyme activities in the presence of inhibitor reflect both Km and Ki as the substrate concentration progressively increases. In the presence of high substrate
concentrations, inhibition of the noncompetitive type, such as ALDH2 in Fig. 2b, appeared not be completely overcome (cf. ADH1B1 in Fig. 1c). This is because the drug also binds to enzyme species other than the one combining with the competing substrate.
3.3. Quantitative assessment
The therapeutic, toxic, and lethal blood plasma levels of aspirin and salicylate in humans are estimated to be 0.11–1.1, 1.7–1.9, and >2.2 mM; and 0.15–1.5, 2.2–2.5, and >2.9 mM, respectively [36]. The percentages inhibition of enzyme activity by 0.1, 0.5, and 1.5 mM 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
aspirin/salicylate were assessed at 2, 10, and 20 mM ethanol for class I, II, and IV ADHs (Table 3), and at 10, 50, and 200 μM acetaldehyde for ALDH1A1 and ALDH2 (Table 4). It has been reported that following ingestion of a low dose of ethanol (0.2 g/kg body weight, roughly equivalent to a bottle of beer for a 65-kg man), the peak blood alcohol reaches 2 mM [37]; in several countries, 20 mM blood ethanol concentration is the legal definition for intoxication while driving. Hepatic steady-state concentrations of acetaldehyde reach 10–20 μM in rat livers perfused with ethanol [38], and thus it can be inferred that 200 μM
acetaldehyde or even higher levels may occur in the liver of East Asians with heterozygous
ALDH2*1/*2 genotype, whose blood acetaldehyde concentrations reached 24–76 μM, after
low to moderate alcohol intake [37,39].
At 0.1 mM salicylate, a low therapeutic plasma concentration, and 2 mM ethanol, the inhibition of ADH activities appears to be minimal (<6.6%) for the class I ADH1B1, ADH1B2, ADH1B3, ADH1C1, ADH1C2, and class IV ADH4, whereas appreciable inhibitions (25–30%) are detected for class I ADH1A and class II ADH2; by contrast, the extents of aspirin inhibition are generally less than 10% that of the corresponding salicylate inhibitions with ADHs. However, at a higher therapeutic, but nontoxic, concentration, that is, 1.5 mM, salicylate inhibits the enzyme activities in increasing order, of ADH4 (17%), ADH1B2 (34%), ADH1B3 (52%), ADH2 (83%), and ADH1A (86%); whereas that for ADH1B1, ADH1C1, and ADH1C2 still remain low (<5.2%). At 1.5 mM aspirin, the inhibitions of ADH activities were low (<5.1%) except for ADH2 (21%) and ADH1A (65%). Since ethanol concentrations in stomach fluid in a social drinking setting may reach 200 mM or higher [18,40], the inhibition of gastric ADH4 activity at 200 mM ethanol by 1.5 mM aspirin and salicylate were assessed to be 0.26% and 4.0%, respectively. At 10 μM acetaldehyde, 1.5 mM salicylate considerably inhibits activities of ALDH1A1 (71%) and ALDH2 (73%) but the inhibitions by 1.5 mM aspirin are considerably reduced, that is, 9.8% 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
and 27%, respectively. It should be noted that although inhibition of ADH and ALDH activities at a fixed drug concentration generally decreases as the substrate concentrations are increased, the inhibitions by salicylate and/or aspirin with ADH1B2, ADH1B3 and ALDH2 remain nearly unchanged at higher substrate concentrations, which can be
attributed to comparable Kis and Kii in a noncompetitive-type inhibition or only the intercept effect in uncompetitive-type inhibitions.
3.4. Model docking of salicylate binding
The activities of ADH allozymes/isozymes are inhibited by salicylate with varied potencies. This suggests that the different amino acid residues in the barrel-shaped hydropholic
substrate pockets of ADH interact with salicylate somewhat differently. We found that salicylate molecule could fit into the substrate binding sites of human ADH1A, ADH1B1, ADH1C2, ADH2 and ADH4 in the presence of NAD+. Model docking of ADH2, which exhibits strong binding with salicylate but much lower affinity to aspirin, a common observation in human ADH family with the exception of ADH1A, was chosen to illustrate the binding mode. In our model, the substrate pocket of ADH2 accommodates well the salicylate molecule (Fig 2a). The catalytic zinc atom is ligated to oxygen of the carboxyl group of salicylate, and the carbonyl oxygen of nicotinamide ring of NAD+ forms a
hydrogen bond with the hydroxyl group of salicylate. By contrast, steric hindrance between bulky acetoxy of aspirin (acetylsalicylate) and phenyl groups of Tyr-94 and Phe-146 pushes the acetyl group of aspirin toward a different orientation which substantially weakens the binding strength for aspirin compared with that of salicylate (Fig. 2a).Interestingly, the small difference in affinities of aspirin and salicylate (Kis = 0.59 mM and 0.17 mM, respectively) with ADH1A can be largely ascribed to the substitution of a much smaller amino acid at the equivalent position, that is, Ala-93 (cf. Phe-93 in ADH1B/1C allozymes, Tyr-94 in ADH2, and Phe-93 in ADH4), resulting in a better binding to aspirin among ADH family. It is worth noting that the theoretically calculated binding energies with salicylate 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
molecule varied only up to 19% for the ADH isozymes/allozymes, and the magnitudes of the calculated dissociation constants (data not shown) do not match those of the observed kinetic inhibition constants. Thus, the modeling only supports the idea that salicylate can bind to the substrate pocket of ADHs. To elucidate the exact molecular structures of
binding, future studies require X-ray crystallographic determination of the ADH-coenzyme-salicylate ternary complexes (and complexes with aspirin if available). Salicylate also can be modeled to fit into the binding pocket of human ALDH2 in the presence of NAD+ (Fig. 2b). One oxygen of the carboxyl group of salicylate forms hydrogen bonding with the nitrogen of γ-amide of Asn-169, and hydroxyl group of the drug is hydrogen-bonded the sulfhydryl of Cys-302, a catalytic nucleophile at the active site. The phenyl moiety of salicylate fits nicely into a hydrophobic tunnel lined with Phe-170, Trp-177, Phe-459 and Phe-465.
4. Discussion
4.1. Metabolic interactions between aspirin/salicylate and ethanol
This is the first comprehensive description on aspirin and its major metabolite salicylate inhibitions of human ADHs and ALDHs at a near physiological pH and cytoplasmic NAD+ concentration. The inhibition patterns and kinetic constants of isozymes/allozymes in the ADH family provide an enzymological basis for quantitative evaluation of the potential interactions with aspirin/salicylate from a pharmacokinetics perspective. To our knowledge, it is the first report that class I ALDH1A1 and class II ALDH2 of the ALDH family can be substantially inhibited by salicylate in target tissues of FPM, indicating that the drug may interact with the metabolic pathway of ethanol at both ADH and ALDH steps. ALDH2 and ALDH1A1 contribute to hepatic metabolism of ethanol-derived acetaldehyde [12,38]; particularly ALDH1A1 in Asian individuals, who carry the variant ALDH2*2 gene alleles, due to the resulting high acetaldehyde levels after alcohol consumption [22,37,39].
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
Salicylate acts as a considerably more potent competitive inhibitor against ethanol oxidation than that of aspirin at 0.5 mM NAD+, a saturating coenzyme concentration for all members of the ADH family except ADH1B2, ADH1B3, and ADH4 [12,17]. The competitive inhibition by salicylate can be explained by the formation of a dead-end E–NAD+–inhibitor complex during catalysis, which gives rise to the slope inhibition effects (Kis). It has been well documented that ADH conforms to an ordered sequential bi mechanism with binding NAD+ first and NADH released last, rate-limited by the release of coenzyme [17]. In agreement with the proposed mechanism, salicylate could fit into the substrate binding pockets of the ADH family in the presence of NAD+, as revealed by molecular model dockings. The observed intercept effects (Kii) of salicylate with ADH1B2 and ADH1B3 could possibly be due to the formation of an additional E–NADH–inhibitor complex, or by binding of salicylate to the free E at a subsaturating level of 0.5 mM NAD+. It has been reported that salicylate can bind to adenosine site of the coenzyme pocket in horse ADH [41]. Clarification of the underlying inhibition mechanism is needed in future research.
Notably, ADH1A appears unique in exhibiting submillimolar slope inhibition constants for both salicylate and aspirin. This is in large part ascribed to the substitution of a small amino acid, Ala-93, located at the bottom of substrate pocket. It is also consistent with previous observations that secondary alcohols, such as cyclohexanol and isopropanol, are uniquely more efficient substrates than ethanol for ADH1A in the human ADH family [42,43]. By contrast, acetaminophen and cimetidine, both commonly used drugs, exhibit lower affinity with human ADH1A (Kis = 20 mM and 3.2 mM, respectively) than that with ADH2 (Kis = 0.90 mM and 0.51 mM, respectively) [44,45]; the latter shows a better binding of these two drugs at the bottom of the substrate pocket by molecular dockings.
With respect to oxidation of acetaldehyde, salicylate acts as a competitive inhibitor with 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
human ALDH1A1 but as a noncompetitive inhibitor with human ALDH2. These inhibition patterns are similar to that of acetaminophen [45], whereas the opposite was observed with cimetidine inhibitions [44]. It may involve different binding modes of the drugs to substrate pockets of the corresponding isozymes. It is also noted that ALDH1A1 shows similar binding affinities to commonly used drugs, that is, salicylate, acetaminophen, and cimitidine with Kis = 0.53 mM, 0.96 mM, and 0.84 mM, respectively, but that ALDH2 exhibits widely varied slope inhibition constants for the above three drugs, that is, 0.37 mM, 3.0 mM, and 12 mM, respectively [44,45; this study], suggesting distinct inhibition potencies of
acetaldehyde oxidation with these drugs.
4.2. Aspirin/salicylate inhibition of first-pass metabolism
Unlike the vast majority of drugs and xenobiotics, the elimination of ethanol is not proportional to its concentration in body fluids, that is, first-order kinetics. Instead, elimination of ethanol exhibits pseudolinear, near zero-order kinetics at concentrations of ethanol above 2 mM [8,9,11]. This Michaelis–Menten type of pharmacokinetics is of special interest in light of FPM, which is defined as the presystemic elimination of newly absorbed ethanol through the stomach, small intestine, and liver, before reaching peripheral blood. Variations reported for FPM using measurement of blood alcohol concentrations (peroral versus intravenous) are largely due to varying saturation of liver alcohol metabolism [3,6– 8]. The extent of FPM would depend on the Km and Vmax for ethanol and the Ki for inhibitors with the responsible ADHs, the amounts of expressed isozymes, and the concentrations of ethanol and aspirin/salicylate in target tissues. Since the half-life for the decline phase of plasma aspirin was approximately 15–20 min and that for its major metabolite salicylate was 2 to 3 h in low doses, plasma levels of salicylate rose rapidly and eventually exceeded those of aspirin because of slower elimination rather than differences in distribution [27,28]. Thus, our findings suggest that aspirin and, particularly salicylate, may effectively interact with ethanol and acetaldehyde during FPM of alcohol.
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
At higher therapeutic levels of blood plasma salicylate (1.5 mM), the decrease of activities are assessed to be 75–86% for class I ADH1A and class II ADH2 at 2–10 mM ethanol, and 62–73% for class I ALDH1A1 and class II ALDH2 at 10–50 μM acetaldehyde (Tables 3 and 4). At a low therapeutic plasma salicylate (0.5 mM), the inhibitions of ADH1A/ADH2 and ALDH1A1/ALDH2 still remain substantially, that is, 50–68% and 35–48%,
respectively. These assessments appear to be consistent with previous reports that aspirin significantly increased blood ethanol concentrations with the concomitant decrease in FPM of alcohol but had no significant effects on the gastric emptying [4,5]. Notably, the activities of class I ADH1B2 and ADH1B3 at 2–10 mM ethanol are also reduced by 31–52% with 1.5 mM salicylate whereas that the corresponding inhibition of ADH1B1 is less than 1%. This suggests that FPM of alcohol in individuals carrying allelic variants of ADH1B*2 or
ADH1B*3 would decrease when concurrent taking aspirin. It requires further research to
confirm the proposed inference. Class IV ADH4, a major isozyme in gastric mucosa, shows only modest inhibition of activity (15–17%, or less at higher ethanol concentrations) with salicylate, suggesting it would contribute to a small portion in aspirin inhibition of alcohol FPM in humans that is contrary to that proposed by Lieber and colleagues [4,5]. It is noted that the inhibitions of ADH and ALDH family members by aspirin per se are generally quite low with the exception of ADH1A (roughly similar to that of salicylate). ADH1A is a major isozyme detected in human fetal liver [46], implying that both aspirin and its metabolite salicylate may inhibit alcohol metabolism in fetus, potentially increasing the fetal tissue injury. Together, our findings support that inhibition of human hepatic FPM and hence an increase of ethanol bioavailability may become significant at moderate therapeutic levels of salicylate. To achieve an understanding of the overall effects of aspirin/salicylate on ethanol metabolism, it will require that the actual amounts of all the relevant ADH/ALDH isozymes in target tissues be determined so that the contributions of each isozyme are accounted for, 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
and such studies are in progress.
Because ALDHs are involved in the metabolism of a variety of carbonyl compounds [21], the effects of aspirin and salicylate on the metabolism of such compounds should also be considered. For instance, salicylate may potentially reduce the efficacy of nitroglycerin, a common antianginal drug, due to its high potency in inhibition of mitochondrial ALDH2 and cytoplasmic ALDH1A1 (Table 2). Both isozymes are responsible for bioactivation of nitroglycerin [47]. Clarification of this possibility is required in future studies, especially for those who take aspirin as an antiatherosclerotic agent. It has been described that individuals carrying the variant ALDH2*2 lacked an efficacious clinical response to nitroglycerin [48].
In conclusion, the results indicate aspirin and its major metabolite salicylate can inhibit activities of human ADH family to widely varying degrees. The ALDH1A1 and ALDH2 are inhibited with distinct kinetic types. In order to quantitatively assess the overall effects of inhibition of the component isozymes by salicylate/aspirin in relation to FPM of ethanol, studies to determine protein contents of the ADH and ALDH isozymes in target tissues are warranted.
Competing interests
The authors declare that they have no competing interests.
Acknowledgements
This work was supported by grants from the National Science Council 90-2320-B016-057, 96-2320-B016-018-MY3 and 99-2320-B016-003-MY2, Republic of China.
References 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
[1] Chan LN, Anderson GD. Pharmacokinetic and pharmacodynamic drug interactions with ethanol (alcohol). Clinical pharmacokinetics. 2014;53:1115–36.
[2] Weathermon R, Crabb DW. Alcohol and medication interactions. Alcohol research & health. 1999;23:40–54.
[3] Badger TM, Ronis MJ, Seitz HK, Albano E, Ingelman-Sundberg M, Lieber CS. Alcohol metabolism: role in toxicity and carcinogenesis. Alcoholism, clinical and experimental research. 2003;27:336–47.
[4] Gentry RT, Baraona E, Amir I, Roine R, Chayes ZW, Sharma R, et al. Mechanism of the aspirin-induced rise in blood alcohol levels. Life sciences. 1999;65:2505–12. [5] Roine R, Gentry RT, Hernandez-Munoz R, Baraona E, Lieber CS. Aspirin increases
blood alcohol concentrations in humans after ingestion of ethanol. Jama. 1990;264:2406–8.
[6] Lee SL, Chau GY, Yao CT, Wu CW, Yin SJ. Functional assessment of human alcohol dehydrogenase family in ethanol metabolism: significance of first-pass metabolism. Alcoholism, clinical and experimental research. 2006;30:1132–42.
[7] Levitt MD, Levitt DG. Appropriate use and misuse of blood concentration measurements to quantitate first-pass metabolism. The Journal of laboratory and clinical medicine. 2000;136:275–80.
[8] Yin SJ, Lee SL, Yao CT, Lai CL. Functional roles of alcohol dehydrogenases in human ethanol metabolism. In: Weiner H, Maser E, Lindahl R, Plapp BV, editors.
Enzymology and Molecular Biology of Carbonyl Metabolism 13. West Lafayette: Purdue University Press, 2007. p. 134–43.
[9] Cederbaum AI. Alcohol metabolism. Clinics in liver disease. 2012;16:667–85. [10] Crabb DW, Matsumoto M, Chang D, You M. Overview of the role of alcohol dehydrogenase and aldehyde dehydrogenase and their variants in the genesis of alcohol-related pathology. The Proceedings of the Nutrition Society. 2004;63:49–63. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
[11] Chen YC, Peng GS, Wang MF, Tsao TP, Yin SJ. Polymorphism of ethanol-metabolism genes and alcoholism: correlation of allelic variations with the pharmacokinetic and pharmacodynamic consequences. Chemico-biological interactions. 2009;178:2–7. [12] Yin SJ, Agarwal DP. Functional polymorphism of alcohol and aldehyde
dehydrogenases: alcohol metabolism, alcoholism, and alcohol-induced organ damage. In: Agarwal DP, Seitz HK, editors. Alcohol in Health and Disease. New York: Marcel Dekker Inc., 2001. p. 1–26.
[13] Duester G, Farres J, Felder MR, Holmes RS, Hoog JO, Pares X, et al. Recommended nomenclature for the vertebrate alcohol dehydrogenase gene family. Biochemical pharmacology. 1999;58:389–95.
[14] Hoog JO, Ostberg LJ. Mammalian alcohol dehydrogenases: a comparative
investigation at gene and protein levels. Chemico-biological interactions. 2011;191:2– 7.
[15] Lee SP, Chiang CP, Lee SL, Hsia YJ, Chuang TL, Lin JC, et al. Immunochemical features in the classification of human alcohol dehydrogenase family. Alcohol. 2006;39:13–20.
[16] Ostberg LJ, Stromberg P, Hedberg JJ, Persson B, Hoog JO. Analysis of mammalian alcohol dehydrogenase 5 (ADH5): characterisation of rat ADH5 with comparisons to the corresponding human variant. Chemico-biological interactions. 2013;202:97–103. [17] Edenberg HJ, Bosron WF. Alcohol dehydrogenases. In: McQueen CA, editor.
Comprehensive Toxicology, Vol. 4. Oxford: Academic Press, 2010. p. 111–30.
[18] Yin SJ, Liao CS, Wu CW, Li TT, Chen LL, Lai CL, et al. Human stomach alcohol and aldehyde dehydrogenases: comparison of expression pattern and activities in
alimentary tract. Gastroenterology. 1997;112:766–75.
[19] Chiang CP, Wu CW, Lee SP, Ho JL, Lee SL, Nieh S, et al. Expression pattern, ethanol-metabolizing activities, and cellular localization of alcohol and aldehyde
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
dehydrogenases in human small intestine. Alcoholism, clinical and experimental research. 2012;36:2047–58.
[20] Anonymous. Nomenclature of mammalian aldehyde dehydrogenases. Progress in clinical and biological research. 1989;290:xix–xxi.
[21] Sladek NE. Human aldehyde dehydrogenases: potential pathological, pharmacological, and toxicological impact. Journal of biochemical and molecular toxicology. 2003;17:7– 23.
[22] Peng GS, Yin SJ. Effect of the allelic variants of aldehyde dehydrogenase ALDH2*2 and alcohol dehydrogenase ADH1B*2 on blood acetaldehyde concentrations. Human genomics. 2009;3:121–7.
[23] Lai CL, Yao CT, Chau GY, Yang LF, Kuo TY, Chiang CP, et al. Dominance of the inactive Asian variant over activity and protein contents of mitochondrial aldehyde dehydrogenase 2 in human liver. Alcoholism, clinical and experimental research. 2014;38:44–50.
[24] Chen YC, Peng GS, Tsao TP, Wang MF, Lu RB, Yin SJ. Pharmacokinetic and pharmacodynamic basis for overcoming acetaldehyde-induced adverse reaction in Asian alcoholics, heterozygous for the variant ALDH2*2 gene allele.
Pharmacogenetics and genomics. 2009;19:588–99.
[25] Brooks PJ, Enoch MA, Goldman D, Li TK, Yokoyama A. The alcohol flushing
response: an unrecognized risk factor for esophageal cancer from alcohol consumption. PLoS medicine. 2009;6:e50.
[26] Peng GS, Chen YC, Wang MF, Lai CL, Yin SJ. ALDH2*2 but not ADH1B*2 is a causative variant gene allele for Asian alcohol flushing after a low-dose challenge: correlation of the pharmacokinetic and pharmacodynamic findings. Pharmacogenetics and genomics. 2014;24:607–17.
[27] Williams FM. Clinical significance of esterases in man. Clinical pharmacokinetics. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
1985;10:392–403.
[28] Rowland M, Riegelman S, Harris PA, Sholkoff SD. Absorption kinetics of aspirin in man following oral administration of an aqueous solution. Journal of pharmaceutical sciences. 1972;61:379–85.
[29] Chiang CP, Wu CW, Lee SP, Chung CC, Wang CW, Lee SL, et al. Expression pattern, ethanol-metabolizing activities, and cellular localization of alcohol and aldehyde dehydrogenases in human pancreas: implications for pathogenesis of alcohol-induced pancreatic injury. Alcoholism, clinical and experimental research. 2009;33:1059–68. [30] Lowry OH, Rosebrough NJ, Farr AL, Randall RJ. Protein measurement with the Folin
phenol reagent. The Journal of biological chemistry. 1951;193:265–75.
[31] Bucher T, Brauser B, Conze A, Klein F, Langguth O, Sies H. State of oxidation-reduction and state of binding in the cytosolic NADH-system as disclosed by
equilibration with extracellular lactate-pyruvate in hemoglobin-free perfused rat liver. European journal of biochemistry. 1972;27:301–17.
[32] Lee SL, Wang MF, Lee AI, Yin SJ. The metabolic role of human ADH3 functioning as ethanol dehydrogenase. FEBS letters. 2003;544:143–7.
[33] Cleland WW. Statistical analysis of enzyme kinetic data. Methods in enzymology. 1979;63:103–38.
[34] Morris GM, Huey R, Lindstrom W, Sanner MF, Belew RK, Goodsell DS, et al. AutoDock4 and AutoDockTools4: automated docking with selective receptor flexibility. Journal of computational chemistry. 2009;30:2785–91.
[35] Yin SJ, Wang MF, Han CL, Wang SL. Substrate binding pocket structure of human aldehyde dehydrogenases: a substrate specificity approach. Advances in experimental medicine and biology. 1995;372:9–16.
[36] Schulz M, Schmoldt A. A compilation of therapeutic and toxic plasma drug concentrations. Anaesthesist. 1994;43:835–44. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
[37] Peng GS, Wang MF, Chen CY, Luu SU, Chou HC, Li TK, et al. Involvement of acetaldehyde for full protection against alcoholism by homozygosity of the variant allele of mitochondrial aldehyde dehydrogenase gene in Asians. Pharmacogenetics. 1999;9:463–76.
[38] Yao CT, Lai CL, Hsieh HS, Chi CW, Yin SJ. Establishment of steady-state metabolism of ethanol in perfused rat liver: the quantitative analysis using kinetic mechanism-based rate equations of alcohol dehydrogenase. Alcohol. 2010;44:541–51.
[39] Peng GS, Chen YC, Tsao TP, Wang MF, Yin SJ. Pharmacokinetic and pharmacodynamic basis for partial protection against alcoholism in Asians,
heterozygous for the variant ALDH2*2 gene allele. Pharmacogenetics and genomics. 2007;17:845–55.
[40] Haber PS, Gentry RT, Mak KM, Mirmiran-Yazdy SA, Greenstein RJ, Lieber CS. Metabolism of alcohol by human gastric cells: relation to first-pass metabolism. Gastroenterology. 1996;111:863–70.
[41] Einarsson R, Eklund H, Zeppezauer E, Boiwe T, Branden CI. Binding of salicylate in the adenosine-binding pocket of dehydrogenases. European journal of biochemistry. 1974;49:41–7.
[42] Stone CL, Li TK, Bosron WF. Stereospecific oxidation of secondary alcohols by human alcohol dehydrogenases. The Journal of biological chemistry. 1989;264:11112– 6.
[43] Lee SL, Shih HT, Chi YC, Li YP, Yin SJ. Oxidation of methanol, ethylene glycol, and isopropanol with human alcohol dehydrogenases and the inhibition by ethanol and 4-methylpyrazole. Chemico-biological interactions. 2011;191:26–31.
[44] Lai CL, Li YP, Liu CM, Hsieh HS, Yin SJ. Inhibition of human alcohol and aldehyde dehydrogenases by cimetidine and assessment of its effects on ethanol metabolism. Chemico-biological interactions. 2013;202:275–82. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
[45] Lee YP, Liao JT, Cheng YW, Wu TL, Lee SL, Liu JK, et al. Inhibition of human alcohol and aldehyde dehydrogenases by acetaminophen: assessment of the effects on first-pass metabolism of ethanol. Alcohol. 2013;47:559–65.
[46] Smith M, Hopkinson DA, Harris H. Developmental changes and polymorphism in human alcohol dehydrogenase. Annals of human genetics. 1971;34:251–71.
[47] Beretta M, Gruber K, Kollau A, Russwurm M, Koesling D, Goessler W, et al. Bioactivation of nitroglycerin by purified mitochondrial and cytosolic aldehyde dehydrogenases. The Journal of biological chemistry. 2008;283:17873–80. [48] Li Y, Zhang D, Jin W, Shao C, Yan P, Xu C, et al. Mitochondrial aldehyde
dehydrogenase-2 (ALDH2) Glu504Lys polymorphism contributes to the variation in efficacy of sublingual nitroglycerin. The Journal of clinical investigation.
2006;116:506–11. 1 2 3 4 5 6 7 8 9 10 11 12
Figure Legends
Fig. 1. Interactions between aspirin and ethanol oxidation with human (a) ADH1A, and between salicylate and ethanol oxidation with human (b) ADH1A, (c) ADH1B1, and (d) ADH2. Enzyme activity was simulated at 0.5 mM NAD+ and varied concentrations of substrate ethanol, 0–50 mM, and inhibitors aspirin or salicylate, 0–2 mM, using Eq. (2) for competitive inhibition. In the absence of inhibitor, Eq. (2) is virtually reduced to Eq. (1). For the corresponding kinetic constants of ADHs for the simulation, see Table 1.
Fig. 2. Interaction between salicylate and acetaldehyde oxidation with human (a) ALDH1A1 and (b) ALDH2. Enzyme activity was simulated at 0.5 mM NAD+ and varied concentrations of substrate acetaldehyde, 0–0.5 mM, and inhibitor salicylate, 0–2 mM, using Eq. (2) for competitive inhibition and Eq. (3) for noncompetitive inhibition. In the absence of inhibitor, Eq. (2) and Eq. (3) are virtually reduced to Eq. (1). For inhibition patterns and the
corresponding kinetic constants of ALDHs for the simulation, see Table 2.
Fig. 3. Modeled salicylate binding to the binary complexes of NAD+ with (a) human ADH2 [PDB:3COS] and (b) human ALDH2 [PDB:1O01]. Binding of aspirin, superimposed with that of salicylate, is also presented in panel (a) for comparison. The side chains of amino acid residues lining the active site that are in close vicinity, ≤5 Å, to the drug, are shown. In panel (a), catalytic Zn2+ is ligated to oxygen of the carboxylate group of salicylate or aspirin, and the carbonyl oxygen of the nicotinamide ring of NAD+ is hydrogen-bonded to the hydroxyl of salicylate. By contrast, the acetyl group of aspirin points toward an other direction due to steric hindrance of the bulky side chains of Tyr-94 and Phe-146. In panel (b) shown by using docking mode with a flexible side chain of Met-124 to allow entry of salicylate into the substrate binding pocket. γ-amide of Asn-169 and sulfhydryl of Cys-302 are, respectively, hydrogen-bonded to the carboxylate and the hydroxyl of salicylate, 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26
respectively. Phe-170, Trp-177, Phe-459 and Phe-465 form part of a hydrophobic tunnel accommodating the aryl ring of salicylate.
1 2
Table 1 Kinetic constants for inhibition of ethanol oxidation by aspirin and salicylate with human ADHs.
Class Isozyme/ Km Vmax Drug Inhibition Kis Kii
allozyme (mM) (U/mg) pattern (mM) (mM)
I ADH1A 5.2 ± 0.3 0.34 ± 0.01 Aspirin C 0.59 ± 0.03 Salicylate C 0.17 ± 0.01 ADH1B1 0.013 ± 0.001 0.112 ± 0.001 Aspirin ˗˗a Salicylate C 1.4 ± 0.2 ADH1B2 2.1 ± 0.1 7.7 ± 0.2 Aspirin N 34 ± 4 42 ± 3 Salicylate N 2.6 ± 0.2 3.5 ± 0.2 ADH1B3 86 ± 3 4.4 ± 0.1 Aspirin N 28 ± 3 33 ± 2 Salicylate N 1.4 ± 0.1 2.2 ± 0.1 ADH1C1 0.36 ± 0.03 0.64 ± 0.02 Aspirin C 26 ± 1 Salicylate C 6.0 ± 0.2 ADH1C2 0.23 ± 0.02 0.44 ± 0.01 Aspirin C 35 ± 1 Salicylate C 2.8 ± 0.1 II ADH2 18 ± 1 0.198 ± 0.002 Aspirin C 5.2 ± 0.2 Salicylate C 0.27 ± 0.01 III ADH3 0.00096 ± 0.00005b 1.58 ± 0.03b Aspirin C 4.1 ± 0.3
Salicylate C 0.30 ± 0.03
IV ADH4 47 ± 5 20 ± 1 Aspirin C 110 ± 20
Salicylate C 6.8 ± 0.4
Enzyme activity was determined in 0.1 M sodium phosphate at pH 7.5 and 25 °C, containing 0.5 mM NAD+ and varied substrate concentrations at various fixed concentrations of inhibitor. Km and Vmax are kinetic constants for substrate ethanol except ADH3. The Km, Vmax, Ki for ADH1B2, ADH1B3, and ADH4 are apparent values due to the subsaturating concentration of 0.5 mM NAD+ used. Values represent means ± SEM.
aNo detectable inhibition up to 40 mM aspirin at 0.1 mM ethanol.
Table 2 Kinetic constants for inhibition of acetaldehyde oxidation by aspirin and salicylate with human ALDHs.
Class Isozyme/ Km Vmax Drug Inhibition Kis Kii
allozyme (μM) (U/mg) pattern (μM) (μM)
I ALDH1A1 67 ± 7 0.61 ± 0.03 Aspirin C 12 ± 1
Salicylate C 0.53 ± 0.05
II ALDH2 0.28 ± 0.03 0.45 ± 0.02 Aspirin U 3.9 ± 0.2
Salicylate N 0.37 ± 0.04 0.55 ± 0.03 III ALDH3A1 0.16 ± 0.01a 84 ± 2a Aspirin ˗˗b
Salicylate ˗˗b
Enzyme activity was determined in 0.1 M sodium phosphate at pH 7.5 and 25 °C, containing 0.5 mM NAD+, 1 mM EDTA, and varied substrate concentrations at various fixed concentrations of inhibitor. Km and Vmax are kinetic constants for substrate acetaldehyde except ALDH3A1. Values represent means ± SEM.
aSubstrate, benzaldehyde.
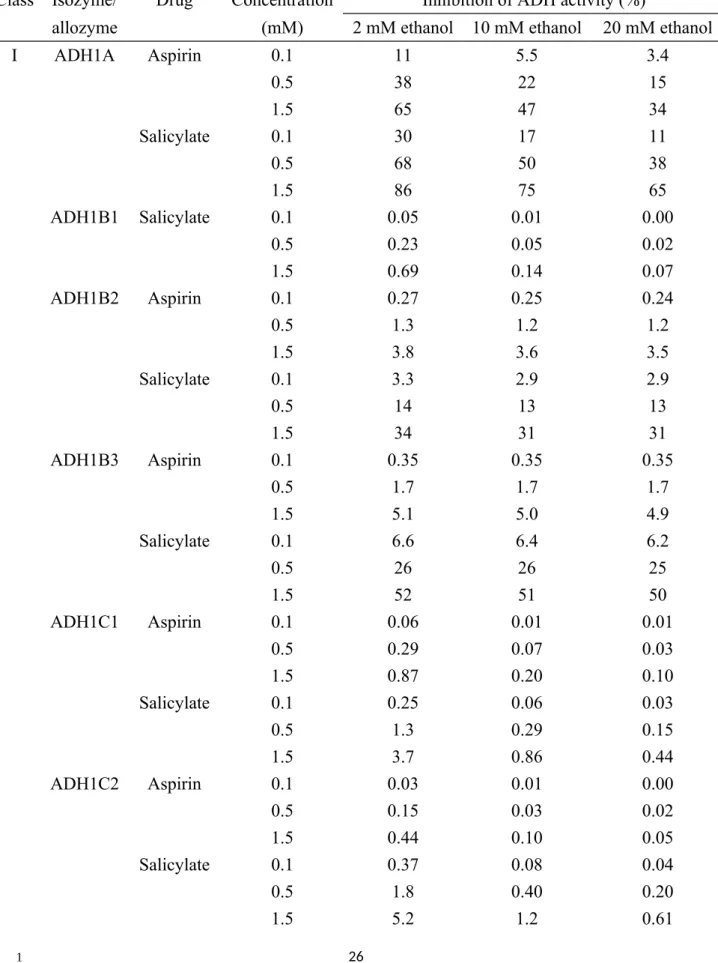
Table 3 Quantitative assessment of inhibition of ethanol oxidation by aspirin and salicylate with human ADHs.
Class Isozyme/ Drug Concentration Inhibition of ADH activity (%)
allozyme (mM) 2 mM ethanol 10 mM ethanol 20 mM ethanol
I ADH1A Aspirin 0.1 11 5.5 3.4 0.5 38 22 15 1.5 65 47 34 Salicylate 0.1 30 17 11 0.5 68 50 38 1.5 86 75 65 ADH1B1 Salicylate 0.1 0.05 0.01 0.00 0.5 0.23 0.05 0.02 1.5 0.69 0.14 0.07 ADH1B2 Aspirin 0.1 0.27 0.25 0.24 0.5 1.3 1.2 1.2 1.5 3.8 3.6 3.5 Salicylate 0.1 3.3 2.9 2.9 0.5 14 13 13 1.5 34 31 31 ADH1B3 Aspirin 0.1 0.35 0.35 0.35 0.5 1.7 1.7 1.7 1.5 5.1 5.0 4.9 Salicylate 0.1 6.6 6.4 6.2 0.5 26 26 25 1.5 52 51 50 ADH1C1 Aspirin 0.1 0.06 0.01 0.01 0.5 0.29 0.07 0.03 1.5 0.87 0.20 0.10 Salicylate 0.1 0.25 0.06 0.03 0.5 1.3 0.29 0.15 1.5 3.7 0.86 0.44 ADH1C2 Aspirin 0.1 0.03 0.01 0.00 0.5 0.15 0.03 0.02 1.5 0.44 0.10 0.05 Salicylate 0.1 0.37 0.08 0.04 0.5 1.8 0.40 0.20 1.5 5.2 1.2 0.61
II ADH2 Aspirin 0.1 1.7 1.2 0.90 0.5 8.0 5.8 4.4 1.5 21 16 12 Salicylate 0.1 25 19 15 0.5 63 54 47 1.5 83 78 72 IV ADH4 Aspirin 0.1 0.09 0.08 0.06 0.5 0.43 0.37 0.32 1.5 1.3 1.1 0.95 Salicylate 0.1 1.4 1.2 1.0 0.5 6.6 5.7 4.9 1.5 17 15 13
Enzyme activity at indicated concentrations of substrate and inhibitor was calculated using the competitive (Eq. (2)) or noncompetitive (Eq. (3)) equations based on the determined inhibition patterns and the corresponding kinetic constants for ADH isozymes/allozymes shown in Table 1. The enzyme activity in the absence of inhibitor (Eq. (1)) was used as control for calculation of the
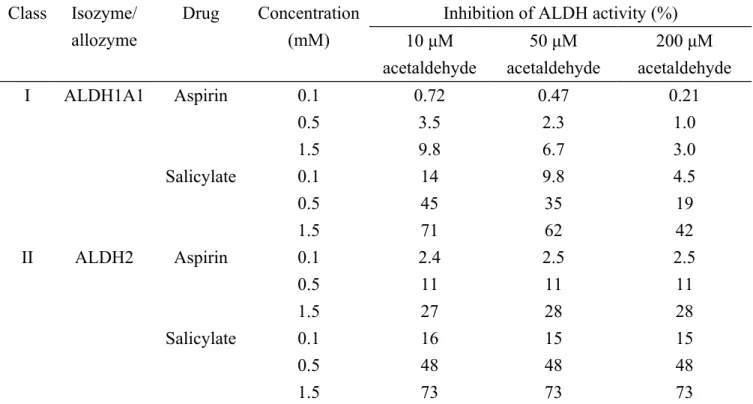
Table 4 Quantitative assessment of inhibition of acetaldehyde oxidation by aspirin and salicylate with human ALDHs. Class Isozyme/ allozyme Drug Concentration (mM)
Inhibition of ALDH activity (%) 10 μM acetaldehyde 50 μM acetaldehyde 200 μM acetaldehyde I ALDH1A1 Aspirin 0.1 0.72 0.47 0.21 0.5 3.5 2.3 1.0 1.5 9.8 6.7 3.0 Salicylate 0.1 14 9.8 4.5 0.5 45 35 19 1.5 71 62 42 II ALDH2 Aspirin 0.1 2.4 2.5 2.5 0.5 11 11 11 1.5 27 28 28 Salicylate 0.1 16 15 15 0.5 48 48 48 1.5 73 73 73
Enzyme activity at indicated concentrations of substrate and inhibitor was calculated using the competitive (Eq. (2)), noncompetitive (Eq. (3)) or uncompetitive (Eq. (4)) equations based on the determined inhibition patterns and the corresponding kinetic constants for ALDH isozymes shown in Table 2. The enzyme activity in the absence of inhibitor (Eq. (1)) was used as control for calculation of the corresponding drug inhibitions.