Atlas hypoplasia combined with atlantoaxial subluxation is a cause of non-traumatic cervical myelopathy.
6
0
0
全文
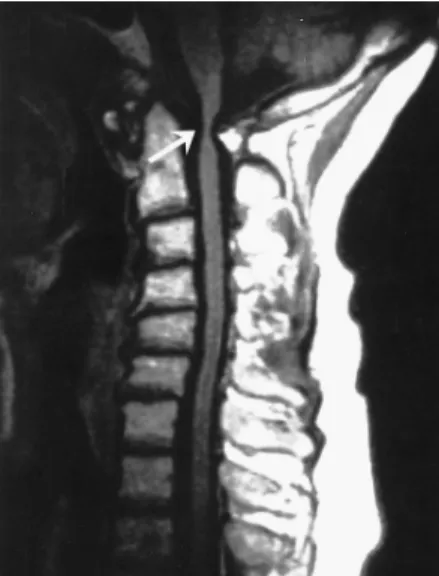
(2) 100. Fig. 1. Lateral view of the plain radiographs of the cervical spine demonstrates hypoplasia of the posterior arch of C-1, and subluxation of the atlantoaxial joint.. Fig. 3. Three-dimensional CT demonstrates markedly increased predental space, measuring 19.78 mm (black arrow), and marked spinal canal stenosis due to cleft of the posterior arch of C-1 and atlantoaxial subluxation (white arrow).. strength grading scale). Muscle tone was markedly high in the lower limbs, and Hoffman sign was noticed. The patient's gait was moderately spastic and the Babinski's reflex produced a dorsal response. Neuroimaging Studies. Plain radiographs of the cervical spine and helical three-dimensional CT disclosed a markedly narrow canal at the level of the atlas due to a cleft of the right posterior C-1 arch and atlantoaxial subluxation (Figs. 1, 2). The. Atlas Hypoplasia. Fig. 2. Axial section of the CT scan shows a hypoplastic posterior C-1 arch (white arrow), and increased predental space due to atlantoaxial subluxation (black arrow).. Fig. 4. Midsagittal T1 weighted MR image of the cervical spine shows a hypoplastic posterior C-1 arch resulting in severe constriction of the upper cervical canal and cord compression.. predental space was 19.78 mm (Fig. 3) in diameter which was significantly wider than the normal limits. Cervical spondylosis was present below the level of C-2. Magnetic resonance imaging and CT scan of the cervical spine showed a hypoplastic posterior C-1 arch resulting in severe focal constriction of the cervical canal with cord compression at the C-1 and C-2 levels (Fig. 4). Operation. The patient was intubated with a fibroscope.
(3) Han-Chung Lee, et al.. A. B. 101. when she was awake and then turned to a prone position to monitor the neurological status during positioning. General anesthesia was induced, and the reduction of the dislocated atlantoaxial joint was performed under the guide of C-arm fluoroscopy. The surgical approach was performed from the posterior midline and a partial cleft on the right posterior C-1 arch was identified. The spinal cord was compressed by a hypertrophied ligament on the right side and hypoplastic C-1 arch on the left side. The underlying dura was indented at that level and expanded after removing the hypoplastic C-1 arch and the constricted ligament. Posterior occipitalC-3 fixation was performed by SOF'WIRE cable system and Tiframe plate-cable fixation (Codman & Shurtleff, Johnson & Johnson) (Fig. 5A). Two drill holes were placed into the occipital bone 2 cm superior to the rim of the foramen magnum. Wires were passed from the holes to the foramen magnum. Another three sublaminar wires were also passed safely under the C-2 and C-3 laminae. Tiframe was fixed with the above five wires for stabilization. The occipital bone and lateral masses of C-1, C-2 and C-3 were decorticated. Autologous bone harvested from the right posterior iliac crest was overlayed on the decorticated rough bone surface. Finally, the wound was closed in layers. Postoperative Course. C. Fig. 5. A: Immediate post-operative plain radiograph of the cervical spine demonstrates widening canal after decompression and fusion; B: The follow-up radiograph of the cervical spine 6 months later, and C: Successful fusion of the occipital bone to C-3 vertebra 12 months after surgery.. The patient was able to walk without assistance one week after surgery. The muscle power of the right deltoid muscle began to improve (shoulder abduction MRC grade 4/5) and she was able to lift her right upper limb when she was discharged from the hospital. Muscle tone and deep tendon reflex were still high in the lower limbs. Post operative plain film of the cervical spine taken 6 months and 12 months later revealed successful bony fusion from the occiputal bone to C-3 (Figs. 5B, 5C). DISCUSSION. The atlas has three primary ossification centers during embryonic period [7]. In approximately 2% of the population, a fourth.
(4) 102. ossification center forms on the posterior tubercle of the atlas. During the ossification process of the atlas, two different types of anomalies can develop: 1) the formation of a posterior cleft, and 2) varying degrees of posterior arch dysplasia [8]. Our case belongs to type 2 because of a partial cleft of the posterior arch of the atlas. The older classification of congenital clefts and defects of the posterior arch of the atlas was divided into five types [1]. Type A: failure of midline fusion of the two hemiarches. It is estimated to occur in 4% of the population and represents 97% of all posterior arch defects [9]. Type B: Unilateral cleft which ranges from a small gap to a complete absence of the hemiarch and posterior tubercle. Our case was classified as type B. Type C: Bilateral clefts of the lateral aspects of the arches with preservation of the most dorsal part of the arch. Type D: Absence of the posterior arch with a persistent posterior tubercle. Type E: Absence of the entire arch including the tubercle. Types B to E occur in 0.69% of all indivisuals. The classification system was reviewed by Currarinos et al [1], and clinically subdivided into five groups: Group 1, asymptomatic with incidental findings; Group 2, neck pain or stiffness after trauma to the head or neck; Group 3, Chronic symptoms related to the neck or cervical spine; Group 4, various chronic neurological problems; and Group 5, acute neurological symptoms after minor cervical trauma [1-2]. This patient belonged to Group 4 because of her chronic symptoms and neurologic deficits. The average saggital canal diameter ranges from 17 to 25 mm at the level of the atlas; the cord diameter ranges from 10 to 12 mm [10]. In cases of cranio-cervical junction lesions, cord compression occurs when the sagittal diameter behind the dens is 14 mm or less [11]. Patients with a saggital canal diameter of less than 10 mm usually show clinical manifestations [10,12,13]. Payne and Spillane were the first to notice the importance of congenital stenosis of the spinal canal and suggested that the development of myelopathy may also be related to the initial size. Atlas Hypoplasia. of the canal [14]. If the spinal canal is congenitally small, the spinal cord will be encroached upon easily by osteophyte, vertebral subluxation, or hypertrophied ligamentum flavium. Our patient also had subluxation of the dens. Her retrodental space was only 8.8 mm. Posterior displacement of the dens while flexing the neck might further compromise the cervical cord. The combination of atlas hypoplasia, segmental cervical canal stenosis and atlantoaxial subluxation as found in our patient has only been reported by Duong et al [15]. A variety of surgical options are available for the treatment of atlantoaxial subluxation. The patient in this report had a narrow spinal canal caused by partial agenesis of the posterior arch of the atlas and atlantoaxial subluxation. To widen the canal, we decided to remove the remnants of the posterior arch of the atlas. In this situation, the application of C1-C2 arthrodeses is difficult in the absence of a posterior arch of C-1. There are two surgical options: 1) the use of bilateral transarticular screws to stabilize the lateral masses of C-1 and C-2, and 2) fusion of the occiput with C-2 and C-3. The first operation can be achieved by transarticular screw fixation of C-1 and C-2. However, the left lateral mass of C-1 was partially hypoplastic in our case. Therefore, this procedure is difficult to perform because the hypoplastic bone may be fractured while purchasing a screw larger than its diameter. Therefore, we applied posterior decompression, internal fixation with Tifram and bone graft for the treatment of atlas hypoplasia, segmental cervical narrowing, cord compression and cervical myelopathy in this case and the outcome was satisfactory. Solid bony fusion from the occiput to C-3 lamina and good neurological recovery of the patient were obtained. REFERENCES. 1. Currarino G, Rollins N, Diehl JT. Congenital defects of the posterior arch of the atlas: a report of seven cases including an affected mother and son. [Review] AJNR Am J Neuroradiol 1994;15:249-54. 2. Logan WW, Stuard ID. Absent posterior arch of the atlas. Am J Roentgenol Radium Ther Nucl Med 1973;.
(5) Han-Chung Lee, et al.. 118:431-4. 3. Torreman M, Verhagen IT, Sluzewski M, et al. Recurrent transient quadriparesis after minor cervical trauma associated with bilateral partial agenesis of the posterior arch of the atlas. Case report. J Neurosurg 1996;84:663-5. 4. Komatsu Y, Shibata T, Yasuda S, et al. Atlas hyoplasia as a cause of high cervical myelopathy. Case report. J Neurosurg 1993;79:917-9. 5. P h a n N , M a r r a s C , M i d h a R , e t a l . C ervical myelopathy caused by hypoplasia of the atlas: Two case reports and review of the literature. [Review] Neurosurgery 1998;43:629-33. 6. Tokiyoshi K, Nakagawa H, Kadota T. Spinal canal stenosis at the level of the atlas: case report. Surg Neurol 1994;41:238-40. 7. Vangilder JC. Menezes AH. Craniovertebral junction abnormalities. Clin Neurosurg 1983;30:514-30. 8. Brown CE. Complete absence of the posterior arch of the atlas. Ana Rec 1941;81:499-503. 9. Gehweiler JA Jr, Danffner RH, Roberts L Jr. Malformations of the atlas vertebra simulating the. 103. Jefferson fracture. AJNR Am J Roentgenol 1983;140: 1083-6. 10. Hinck VC, Sachdev NS. Developmental stenosis of the cervical spinal canal. Brain 1966;89:27-36. 11. Greenberg AD. Atlanto-axial dislocations. Brain 1968;91:655-84. 12. Epstein JA, Carras R, Hyman RA, et al. Cervical myelopathy caused by developmental stenosis of the spinal canal. J Neusurg 1979;51:362-7. 13. Menezes AH, VanGilder JC, Graf CJ, et al. Craniocervical abnormalities. A comprehensive surgical approach. J Neurosurg 1980;53:444-55. 14. Payne EE, Spillane JD. The cervical spine: An Anatomic-pathological study of 70 specimens (using a special technique) with particular reference to the problem of cervical spondylosis. Brain 1957;80:57192. 15. Duong DH, Chadduck WM . Reconstruction of the hypoplastic posterior arch of the atlas with calvarial bone grafts for posterior atlantoaxial fusion : technical report. Nurosurgery 1994;35:1168-70..
(6) 104. -. 2003;8:99-104. -. 404. -. 2. 2002. 7. 1. 2003. 3. 26. 2003. 3. 5.
(7)
數據

相關文件
For 5 to be the precise limit of f(x) as x approaches 3, we must not only be able to bring the difference between f(x) and 5 below each of these three numbers; we must be able
[This function is named after the electrical engineer Oliver Heaviside (1850–1925) and can be used to describe an electric current that is switched on at time t = 0.] Its graph
You are given the wavelength and total energy of a light pulse and asked to find the number of photons it
Reading Task 6: Genre Structure and Language Features. • Now let’s look at how language features (e.g. sentence patterns) are connected to the structure
develop a better understanding of the design and the features of the English Language curriculum with an emphasis on the senior secondary level;.. gain an insight into the
• Introduction of language arts elements into the junior forms in preparation for LA electives.. Curriculum design for
Wang, Solving pseudomonotone variational inequalities and pseudocon- vex optimization problems using the projection neural network, IEEE Transactions on Neural Networks 17
We explicitly saw the dimensional reason for the occurrence of the magnetic catalysis on the basis of the scaling argument. However, the precise form of gap depends
