Identifying Factors Associated With Hospital
Readmissions Among Stroke Patients in Taipei
Kun-Yang Chuang· Shwu-Chong Wu* · Ai-Hsuan Sandra Ma** Yu-Hui Chen***· Chen-Long Wu****
ABSTRACT: Hospital readmissions contribute significantly to the cost of medical care, and may reflect unresolved problems at discharge or a lack of resources in post-hospital care. The purpose of this paper is to assess the effects of patient characteristics at discharge, the need for nursing care, discharge planning program, post-hospital care arrangements, and caregiver characteristics on readmissions of stroke patients. Patients discharged from neurological wards in seven hospitals in the Taipei area were recruited into the study. Surveys were conducted before their discharge, and at one month after discharge. Of the 489 patients included in the study, 24.3% were readmitted. After controlling for other variables, factors associated with readmissions were number of limitations in activities of daily living (ADL), first incidence of stroke, the need for wound nursing care, the adoption of a care plan, and the discharge locations. Contrary to expectation, age, length of stay, counseling before discharge, and caregiver burden were not associated with readmissions. The findings of this study indicate that ADL limitation is an effective predictor of readmissions. Increasing home nursing resources to meet the demand for wound nursing care may also be effective in reducing readmissions. Discharging patients into institutions for a short period of time may also prove to be more economically viable due to the reduction in readmissions.
Key Words: readmission, stroke patients, discharge planning.
Introduction
Hospital readmission has been used as an indicator of quality of care, and has been shown to be associated with medical care expenditure (Anderson & Steinberg, 1984; Leibson, Naessens, Campion, Krishan, & Ballard, 1991). From a quality of care standpoint, hospital read-missions may reflect unresolved problems at discharge. In terms of access to care, it may imply there is a lack of resources being allocated to post-hospital care. And, financially, readmission means the return for the most
expensive type of health services, inpatient acute care. Identifying factors associated with hospital readmissions can provide crucial information in the development of intervention programs to reduce unnecessary readmis-sion, and thus improve the quality of care and reduce costs. Research has shown that readmissions are preva-lent mostly among the more chronically ill population (Soeken, Prescott, Herron, & Creasia, 1991; Wray, DeBehnke, Ashton, & Dunn, 1988). Furthermore, com-pared to patients with other chronic conditions, stroke patients had longer length of stay, more readmissions, and PhD, Assistant Professor, School of Public Health, College of Public Health and Nutrition, Taipei Medical University; *PhD, Professor, Institute of Health Policy and Management, National Taiwan University; **PhD, Assistant Professor, Department of Sociology, National Chengchi University; ***MPH, Assistant, School of Public Health, College of Public Health and Nutrition, Taipei Medical University; ****MPH, Vice Superintendent, Taipei City Hospital.
Received: December 28, 2004 Revised: March 15, 2005 Accepted: April 25, 2005
Address correspondence to: Chen-Long Wu, No. 145, Zhengzhou Rd., Datong District, Taipei 10341, Taiwan, ROC. Tel: 886(2)2555-3000 ext. 2007; Fax: 886(2)2559-9051; E-mail: [email protected]
higher medical expenditure (Wolinsky, Gurney, Wan, & Bentley, 1998). Similar results were observed in Taiwan where stroke patients had longer lengths of stay and higher medical expenditure than patients with other chronic conditions (Department of Health, Executive Yuan, 2004a). How to reduce readmissions and medical care expenditure has become a major concern, as the num-ber of stroke patients increases in Taiwan (Department of Health, Executive Yuan, 2003, 2004b). Thus, the purpose of this research is to investigate factors that may be asso-ciated with hospital readmissions among stroke patients within 30 days after discharge, and to propose approaches to reduce readmissions.
Depending on patient characteristics and the length of follow-up, the rate of readmissions varied widely. Previous epidemiologic studies of stroke survivors estimated the readmission rate to be between 20% and 27% within one year after the initial stroke (Sloan, Taylor, & Picone, 1999; Thorngren, Westling, & Norrving, 1990). Camberg et al. (1997) studied repeated hospitalization of stroke patients 65 years or older discharged from Veteran Health Adminis-tration Hospitals and reported readmission rates of 16.6% at one month after hospital discharge. In general, the read-mission rates at six months ranged from 23.0% to 43.8% (Andersen et al., 2000; Camberg et al., 1997; Ottenbacher et al., 2001). At 12 months, they ranged from 32.5% to 58.8% (Berg & Intrator, 1999; Bohannon & Lee, 2003; Camberg et al., 1997; Claesson, Gosman-Hedstrom, Fagerberg, & Blomstrand, 2003).
Studies focused on identifying factors associated with hospital readmissions are many, but only few stud-ies have focused on stroke patients. Past studstud-ies have identified demographic, social, and health related fac-tors such age, widowhood, social support, life satisfac-tion, severity of illness, co-morbidity, depression, and caregiver burden as potential predictors of hospital readmissions (Hoskins, Walton-Moss, Clark, Schroeder, & Thiel, Sr., 1999; Krumholz et al., 1997; Levine et al., 1996; Lotus Shyu, Chen, & Lee, 2004; Nikolaus, Specht-Leible, Kruse, Oster, & Schlierf, 1992; Rich et al., 1995; Schwarz, 2000; Schwarz & Elman, 2003). However, most of the studies have been carried out among the gen-eral population or among heart patients exclusively.
Among stroke patients, worse physical function at discharge has been consistently associated with increased
readmission rates (Bohannon & Lee, 2004; Ottenbacher et al., 2001). Patients with worse physical functions tended to have more severe cases of stroke, demand more care, and thus, be more likely to be readmitted when post-hospital care resources were insufficient. The rela-tionship between length of stay and readmissions, on the other hand, has been inconclusive. While Bohannon and Lee (2003) found shorter length of stay to be associated with readmissions among stroke patients, Westert, Lagoe, Keskimaki, Leyland, and Murphy (2002) did not find such a relationship and concluded that hospital read-missions were not produced by premature discharge in the study population.
The implementation of discharge planning in hospi-tals can also be a significant factor in reducing readmis-sion. In a recent study, Dai, Chang, Hsieh, and Tai (2003) have found that stroke patients included in the discharge planning program were less likely to be readmitted, although the difference was not statistically significant. Nevertheless, the potential of discharge planning in reducing readmissions has been documented in other research (Naylor et al., 1999). Follow-up home visit after hospital discharge is also associated with reduced re-admissions. Anderson et al. (2000) randomly assigned patients to different follow-up programs with primary care physicians or therapists, and found that patients in the experimental groups were less likely to be readmitted than those in the control group. The authors speculated that the visits with physicians and therapists were able to detect health problems earlier and prevent readmissions. Another study focused on heart patients, however, found follow-up visits ineffective in reducing hospital readmissions (Kwok et al., 2004).
Studies have identified an association between the use of institutions and readmissions, (Camberg et al., 1997; Corrigan & Martin, 1992; Lockery, Dunkle, Kart, & Coulton, 1994; Naylor et al., 1999). But the findings have been inconclusive. Furthermore, none of these studies was able to identify the underlying causes associ-ated with the effects of institutionalization on reduced hospitalization. Did reduced readmissions represent better care or unmet needs in inpatient care among those in institutions? Past studies mainly attributed the differ-ence in readmission rates to disparity in patient charac-teristics.
Studies identifying variables that may influence readmissions rates among stroke patients have mainly focused on the effects on readmissions of patient demo-graphic characteristics, physical function, discharge plan-ning, and discharge location. Little information is available about the association between readmissions and the need for nursing care or caregiver characteristics. Thus, this study attempts to provide a broader perspective on read-mission of stroke patients by including variables such as the need for nursing care, caregiver characteristics, and caregiver burdens as predictor variables, in addition to other already known predictors.
Methods
This research used a longitudinal study design. Information was collected through face-to-face inter-views while the patients were in the hospital and through telephone interviews at one month after their hospital dis-charge. Stroke patients were recruited from neurology wards at seven hospitals in the Taipei area from July 1999 to June 2000. Among the hospitals, one was a medical center, five were municipal hospitals, and one was a pri-vate hospital. Patients were eligible to participate in this study if diagnosed with stroke based on the International Classification of Disease, ICD-9-CM, codes 430-434, and 436-438.
A total of eight interviewers were recruited to assist with data collection. Prior to actual data collection, the interviewers participated in a one-day workshop, consist-ing of basic trainconsist-ing in survey research and interview tech-niques, and a practice session. Systematic screening of stroke patients was performed by the trained interviewers from the hospital admissions and neurology ward registries twice a week. The interviewers would visit the stroke patients prior to their discharge and conduct in-hospital face-to-face interviews. The in-hospital interview was arranged for a time close to the day of their discharge, so that the collected information would be representative of the patient’s condition at discharge.
Formal approvals of the study were obtained from each of the participating hospitals. Patients and their fam-ilies who expressed interest were given a written state-ment describing the purpose of the study, the right to with-draw from the study at any time, and the right to refuse to
answer questions. Contact information of the principle investigator was also listed in the statement. Oral instead of written consent was obtained from each participant before interviews. When patients were cognitively im-paired, oral consent was obtained from the next of kin. In situations where a patient was unable to respond to the questionnaire, the available caregiver was selected as the proxy respondent, with the consent of the stroke patient or the next of kin.
Only stroke patients who had reported functional limitations in any activity of daily living or any instru-mental activity of daily living in the in-hospital inter-views were included in the follow-up telephone surveys. These activities included eating, dressing, bathing, transferring, toileting, walking indoors, preparing food, doing light housework, doing laundry, walking out-doors, grocery shopping, personal finances, taking med-ication, and making telephone calls. A patient was defined as having functional limitations if he or she was not able to perform the activity free of assistance. At exactly one month after their discharge, interviewers would attempt to make telephone contact with the patient or the primary caregiver. If they could not be reached at the first attempt, the interviewers would try to call again on another day. A maximum of three attempts would be made. When the patients could not be inter-viewed for health reasons, a primary caregiver was selected and asked to provide proxy responses. Oral con-sent was obtained for each of the follow-up telephone surveys.
A total of 714 patients completed the in-hospital inter-views. At time of discharge, 147 patients had recovered all physical functions, and were excluded from the one-month follow-up survey. Before the one-month follow-up, 30 patients had deceased, and were excluded due to incom-plete data. Another 48 patients discontinued their partici-pation in this study. Thus, the final number in the analysis was 489.
Measurements
Independent variables included socio-demographic characteristics of the patient, stroke severity, nursing care needs, discharge planning variables, and caregiver char-acteristics. Socio-demographic characteristics included age, sex, ethnicity, years of education, and monthly
fam-ily income. Age was grouped into three categories: < 65, 65-74, and 75 or more. Due to the low number of Main-lander and Hakka respondents, they were grouped together in the analysis. Ethnicity was classified as “Fukienese” or “non-Fukienese”. Years of education was measured by the number of years of formal education. The categories were no formal education, one to six years, and more than six years of formal education. Monthly income was the total household income. Patients were grouped into low (less than NT$ 30,000), middle (NT$ 30,000 to NT$ 79,999), and high income (more than NT$ 80,000) cate-gories.
Stroke severity was assessed with three variables. In this study, we did not have direct measures of stroke severity, but had to use the number of dependencies in activity of daily living (ADL), level of consciousness, and first incidence of stroke as proxy measures for stroke severity. The number of dependency in ADL was mea-sured with the Katz index of independence in ADL. It involved assessing whether the patient was able to per-form the following activities without assistance: eating, dressing, bathing, transferring, toileting, and walking indoors. The number of limitations ranged from 0 to 6. In the analysis, scores were grouped into low (0-2), middle (3-4), and high (5-6) for comparison purposes. The level of consciousness was measured by one six-point item with 0 representing unconsciousness, and 5 representing clear consciousness. Scores 1 through 4 represented var-ious levels of confusion regarding time, place, or people. For the analysis, level of consciousness was grouped into clear consciousness, confusion, or unconscious-ness.
The need for nursing care included four variables: mouth care, wound nursing care, replacement of tubes (including Foley catheter, N-G tube and trachea), and other invasive nursing care (including bladder irrigation, enema, suctioning). It was assessed whether the patients needed such care after hospital discharge. All variables were coded as dichotomous variables.
Discharge planning variables included length of stay, consultations before discharge, the adoption of a care plan, and care arrangements after discharge. Length of stay was the number of days the patient was hospital-ized. Consultations before discharge assessed to what extent patients or caregivers received information on
how to care for the patients. The adoption of a care plan indicated whether the patient followed the arrangements for post-hospital care as proposed by the staff in the dis-charge planning program. Care arrangements included the use of institutions, the use of 24-hour attendants, other home or community-based care, and family care. The number of users for home or community-based care was small, and thus these were grouped together with family care.
Caregiver characteristics included age, sex, spousal relationship with the patient, and caregiver burden. Care-giver age was grouped into four categories: < 45, 45-54, 55-64, and 65 or more. Caregiver burden was assessed with seven questions. The seven-question caregiver bur-den index in this study was part of a 20-question index originally developed by the researchers (Lee & Wu, 1998) based on past research. Five of the seven questions as-sessed the negative effects of care-giving (physical tired-ness, emotional stress, lack of time for oneself, financial pressure, competing care demands), while the other two questions assessed the positive effects (the feeling of being wanted, and satisfaction resulted from fulfilling obligations). Each question has a 4-point scale with 1 representing ‘never’ and 4 representing ‘very often’. In terms of reliability, the five-question negative effects measure and the two-question positive effects measure had a Cronbach’s alpha of 0.80 and 0.81.respectively. Questions were recoded so that higher score indicated more burdens. The final score for caregiver burden was the sum of the seven questions, ranging from 7 to 28, with higher scores indicating more burdens. To assess the effects of caregiver burden on hospital readmissions, respondents were divided in about equal numbers into three groups representing lower, middle, and higher bur-den.
Statistical Analysis
Characteristics of patients were presented with num-bers and percentages. Comparisons between those readmit-ted and those not readmitreadmit-ted were made with t-test andc2 test. To assess the effects of predictor variables on hospital readmissions, multivariate logistic regression was used. Statistical calculation was carried out using SPSS 10.0 software. The level of significance for all tests was set at .05.
Results
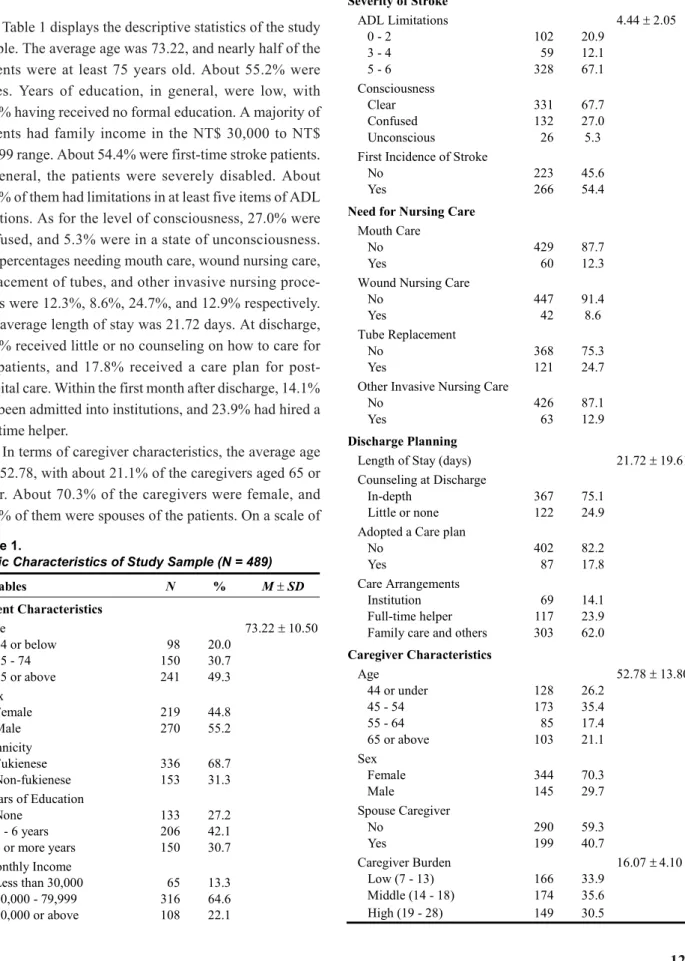
Table 1 displays the descriptive statistics of the study sample. The average age was 73.22, and nearly half of the patients were at least 75 years old. About 55.2% were males. Years of education, in general, were low, with 27.2% having received no formal education. A majority of patients had family income in the NT$ 30,000 to NT$ 79,999 range. About 54.4% were first-time stroke patients. In general, the patients were severely disabled. About 67.1% of them had limitations in at least five items of ADL functions. As for the level of consciousness, 27.0% were confused, and 5.3% were in a state of unconsciousness. The percentages needing mouth care, wound nursing care, replacement of tubes, and other invasive nursing proce-dures were 12.3%, 8.6%, 24.7%, and 12.9% respectively. The average length of stay was 21.72 days. At discharge, 24.9% received little or no counseling on how to care for the patients, and 17.8% received a care plan for post-hospital care. Within the first month after discharge, 14.1% had been admitted into institutions, and 23.9% had hired a full-time helper.
In terms of caregiver characteristics, the average age was 52.78, with about 21.1% of the caregivers aged 65 or older. About 70.3% of the caregivers were female, and 40.7% of them were spouses of the patients. On a scale of
Table 1.
Basic Characteristics of Study Sample (N = 489)
Variables N % M ± SD Patient Characteristics Age 73.22± 10.50 64 or below 98 20.0 65 - 74 150 30.7 75 or above 241 49.3 Sex Female 219 44.8 Male 270 55.2 Ethnicity Fukienese 336 68.7 Non-fukienese 153 31.3 Years of Education None 133 27.2 1 - 6 years 206 42.1 7 or more years 150 30.7 Monthly Income Less than 30,000 65 13.3 30,000 - 79,999 316 64.6 80,000 or above 108 22.1 Severity of Stroke ADL Limitations 4.44± 2.05 0 - 2 102 20.9 3 - 4 59 12.1 5 - 6 328 67.1 Consciousness Clear 331 67.7 Confused 132 27.0 Unconscious 26 5.3
First Incidence of Stroke
No 223 45.6
Yes 266 54.4
Need for Nursing Care
Mouth Care
No 429 87.7
Yes 60 12.3
Wound Nursing Care
No 447 91.4
Yes 42 8.6
Tube Replacement
No 368 75.3
Yes 121 24.7
Other Invasive Nursing Care
No 426 87.1
Yes 63 12.9
Discharge Planning
Length of Stay (days) 21.72± 19.61
Counseling at Discharge
In-depth 367 75.1
Little or none 122 24.9
Adopted a Care plan
No 402 82.2
Yes 87 17.8
Care Arrangements
Institution 69 14.1
Full-time helper 117 23.9
Family care and others 303 62.0
Caregiver Characteristics Age 52.78± 13.80 44 or under 128 26.2 45 - 54 173 35.4 55 - 64 85 17.4 65 or above 103 21.1 Sex Female 344 70.3 Male 145 29.7 Spouse Caregiver No 290 59.3 Yes 199 40.7 Caregiver Burden 16.07± 4.10 Low (7 - 13) 166 33.9 Middle (14 - 18) 174 35.6 High (19 - 28) 149 30.5
7-28, the average score for caregiver burden was 16.07. Dividing caregivers about equally into three groups of low, middle, and high burdens, the range of scores were 7-13, 14-18, and 19-28 respectively.
Among the 489 patients, 119 (24.3%) had a hospital readmission within the first month after hospital dis-charge. Table 2 compares the readmission rates among patients of different characteristics. In terms of
socio-Table 2.
Comparison of Readmission Rates Among Patients of Different Characteristics
Readmission (N = 119 ) Non-readmission (N = 370) Variables N % M ± SD N % M ± SD c2/p t/p Patient Characteristics Age 73.83± 9.77 73.02± 10.73 -0.73 64 or below 19 19.4 79 80.6 65 - 74 37 24.7 113 75.3 75 or above 63 26.1 178 73.9 Sex 0.24 Female 51 23.3 168 76.7 Male 68 25.2 202 74.8 Ethnicity 0.08 Fukienese 83 24.7 253 75.3 Non-fukienese 36 23.5 117 76.5 Years of Education 2.28 None 26 19.5 107 80.5 1 - 6 years 54 26.2 152 73.8 7 or more years 39 26.0 111 74.0 Monthly Income 1.44 Less than 30,000 12 18.5 53 81.5 30,000 - 79,999 79 25.0 237 75.0 80,000 or above 28 25.9 80 74.1 Severity of Stroke ADL Limitations 38.45*** 0 - 2 3 2.9 99 97.1 3 - 4 10 16.9 49 83.1 5 - 6 106 32.3 222 67.7 Consciousness 12.59** Clear 65 19.6 266 80.4 Confused 44 33.3 88 66.7 Unconscious 10 40.0 16 61.5
First Incidence of Stroke 1.76
No 48 21.5 175 78.5
Yes 71 26.7 195 73.3
Need for Nursing Care
Mouth Care 4.22*
No 98 22.8 331 77.2
Yes 21 35.0 39 65.0
Wound Nursing Care 23.10***
No 96 21.5 351 78.5
Yes 23 54.8 19 45.2
Tube Replacement 30.34***
No 67 18.2 301 81.8
Yes 52 43.0 69 57.0
Other Invasive Nursing Care 34.49***
No 85 20.0 341 80.0
demographic characteristics, patients of different age, sex, ethnicity, education, or income did not have statisti-cally different readmission rates. Higher readmission rates were observed in patients with more ADL limita-tions, or lower levels of consciousness. Patients with the need for mouth care, wound care, replacement of tubes, or other invasive nursing care also had higher readmis-sion rates. In terms of discharge planning, patients who had longer length of stay, adopted a care plan, or used a full-time helper also had higher readmission rates. Higher readmission rates were also observed in patients with younger, non-spousal, or higher-burdened care-givers.
Table 3 shows the results of the multivariate logistic regression. The significant predictors of readmissions were number of ADL limitations, first-time stroke, need for wound nursing care, need for other invasive nursing
care, adoption of a care plan, and care arrangements after discharge. Compared to patients with 0-2 ADL limita-tions, those with 3-4, and 5-6 limitations were 6.62, and 8.63 times more likely to be readmitted. Patients who had had a first-ever incidence of stroke were 2.38 times more likely to be readmitted. Patients needing wound nursing care or other invasive nursing care were 3.25 and 2.61 times more likely to be readmitted respectively. The need for mouth care and tube replacement, although significant in the bi-variate analysis, was found to be sta-tistically insignificant by this test. Compared to patients in institutions, the odds of being re-admitted were 10.16 and 4.50 times higher for patients cared for by a full-time helper or family members respectively. Not shown in the table, patients with a full-time helper were also more likely to be readmitted compared to patients cared for by family members (OR = 2.26; 95% CI = 1.23 to 4.16).
Discharge Planning
Length of Stay (days) 27.37± 27.22 19.90± 16.07 -2.84**
Counseling at Discharge 1.30
In-depth 94 25.6 273 74.4
Little or none 25 20.5 97 79.5
Adopted a Care Plan 36.18***
No 76 18.9 326 81.1
Yes 43 49.4 44 50.6
Care Arrangements 42.94***
Institution 12 17.4 57 82.6
Full-time helper 55 47.0 62 53.0
Family care and others 52 17.2 251 82.8
Caregiver Characteristics Age 9.81* 44 or under 34 26.6 94 73.4 45 - 54 53 30.6 120 69.4 55 - 64 16 18.8 69 81.2 65 or above 16 15.5 87 84.5 Sex 0.28 Female 86 25.0 258 75.0 Male 33 22.8 112 77.2 Spouse Caregiver 6.01* No 82 28.3 208 71.7 Yes 37 18.6 162 81.4 Caregiver Burden 9.32** Low (7 - 13) 28 16.9 138 83.1 Middle (14 - 18) 44 25.3 130 74.7 High (19 - 28) 47 31.5 102 68.5 *p < .05; **p < .01; ***p < .001.
Discussion
The readmission rates for stroke patients remain high. Efforts to reduce readmissions can improve the quality of care in hospitals and reduce medical care expenditure. Although this study is exploratory in nature, it has identified some factors that are worthy of future investigation. Consistent with findings from previous research (Bohannon & Lee, 2004; Ottenbacher et al., 2001), the number of limitations in ADL before hospital discharge was a significant predictor. ADL dependency at discharge was associated with severity of stroke and was also an assessment of the extent of recovery. The results of this study provide some evidence that ADL assessment at discharge can be effective in identifying groups at high risk of readmission. Interventions aimed at reducing
Table 3.
Results of Multi-Variate Logistic Regression
Variable OR 95% CI p value Patient Characteristics Age 64 or under 1.00 -65 - 74 1.72 0.74 - 4.05 0.21 75 or above 1.40 0.56 - 3.52 0.48 Sex Female 1.00 -Male 1.44 0.77 - 2.68 0.25 Ethnicity Fukienese 1.00 -Non-fukienese 0.81 0.45 - 1.46 0.49 Years of Education None 1.00 -1 - 6 years 1.79 0.87 - 3.67 0.11 7 or more years 1.59 0.68 - 3.72 0.29 Monthly Income Less than 30,000 1.00 -30,000 - 79,999 1.90 0.84 - 4.34 0.13 80,000 or above 2.01 0.74 - 5.47 0.17 Severity of Stroke ADL Limitations 0 - 2 1.00 -3 - 4 6.62 1.65 - 26.62 0.01 5 - 6 8.63 2.43 - 30.64 < 0.01 Consciousness Clear 1.00 -Confused 1.07 0.60 - 1.92 0.82 Unconscious 1.25 0.39 - 4.00 0.71
First Incidence of Stroke
No 1.00
-Yes 2.38 1.38 - 4.10 < 0.01
Need for Nursing Care
Mouth Care
No 1.00
-Yes 1.22 0.51 - 2.92 0.66
Wound Nursing Care
No 1.00
-Yes 3.25 1.33 - 7.91 0.01
Tube Replacement
No 1.00
-Yes 1.18 0.53 - 2.62 0.69
Other Invasive Nursing Care
No 1.00
-Yes 2.61 1.03 - 6.63 0.04
Discharge Planning
Length of Stay (days) 1.01 0.99 - 1.02 0.18 Counseling at Discharge
In-depth 1.00
-Little or none 0.83 0.44 - 1.56 0.56
Adopted a Care Plan
No 1.00
-Yes 3.42 1.79 - 6.54 < 0.01
Care Arrangements
Institution 1.00
-Full-time helper 10.16 3.84 - 26.89 < 0.01 Family care and others 4.50 1.72 - 11.72 < 0.01
Caregiver Characteristics Age 44 or under 1.00 -45 - 54 1.13 0.57 - 2.26 0.73 55 - 64 0.62 0.24 - 1.63 0.33 65 or above 0.44 0.13 - 1.45 0.18 Sex Female 1.00 -Male 0.96 0.53 - 1.73 0.88 Spouse Caregiver No 1.00 -Yes 1.06 0.42 - 2.71 0.90 Caregiver Burden Low (7 - 13) 1.00 -Middle (14 - 18) 1.03 0.52 - 2.05 0.93 High (19 - 28) 1.27 0.62 - 2.63 0.51
readmissions should place more attention on those severely disabled at discharge.
This finding also raises the issue of what is the balance between length of stay and the recovery of ADL functions. If a patient discharged with more ADL dependencies were more likely to be readmitted within one month, and if the potential for the patient to recover more ADL functions was imminent, then should the patient be hospitalized lon-ger until he or she has regained more function? The cost of keeping patients longer should be weighed against the additional cost of readmissions if patients are discharged early. Thus, the decision to discharge a stroke patient should not only consider the current status of the patient, but should also take the likelihood of readmission into con-sideration.
In this study, wound nursing care and other invasive nursing procedures were significant predictors. One lim-itation of this research is that it does not distinguish among the types of invasive nursing procedure needed. Thus it is not clear which of the invasive nursing proce-dures was responsible for the statistical association. However, the significant association between wound nursing care and readmissions appears to indicate a pos-sible unmet need in wound nursing care resulting from an insufficient number of nursing visits. The National Health Insurance scheme reimburses home nursing vis-its twice per month. While this may be sufficient for the replacement of tubes or mouth care, it may be insuffi-cient for wound nursing care, which at times requires more frequent nursing visits. Other previous research has indicated a need for more wound nursing visits than the twice per month reimbursed by the National Health Insurance (Wang, 2003). The Bureau of National Health Insurance should conduct additional studies to assess whether the benefit of reduced hospital readmissions resulting from offering more nursing visits would out-weigh the cost of providing such care.
The findings also indicated that patients who adopted a care plan were more likely to be readmitted. Due to a lack of standardized discharge planning pro-grams among the seven hospitals where the study took place, the adoption of care plans may, indeed, have ent implications. Similar patients discharged from differ-ent hospitals may receive differdiffer-ent care plans due to dif-ferences in practice patterns among hospitals. One
possi-ble explanation is that care plans may be associated with the severity of patient status at discharge. Patients with a severe case of stroke tended to have multiple needs for care, and thus, were more likely to receive a care plan from the discharge planning program.
The use of institutions was associated with fewer readmissions. Speculations as to the reasons why the association was observed included differences in patient characteristics, caregiver burden, perceived need to re-hospitalize patients, and quality of care. However, since patients in institutions tended to be sicker, and care-giver burden was controlled for in the study, it is unlikely that these were the reasons why the difference was observed. One possible reason is that the family care-givers and the care providers in institutions do perceive the need to re-hospitalize patients differently. The deci-sion to re-hospitalize patients by a family caregiver may be made based on different criteria from those of institu-tional care providers. To understand the reasons for reduced readmissions, the decision making process for re-hospitalizing a patient should be studied extensively. Another reason could be that institutions were better at handling stroke patients immediately after discharge. In other words, family caregivers were not ready to face the complexity of the care demands of stroke patients imme-diately after discharge. Thus, it ought to be considered at what point it becomes more economically viable to dis-charge patients to institutions before sending them home. The effects on readmissions of short-term stay in institu-tions should be investigated.
As the cost of health care increases, the relationship between hospital readmissions and characteristics of patient status at discharge, discharge planning program, and post-hospital care arrangements has significant impli-cations for developing interventions that may reduce the cost of hospitalization. The limitation of two home nursing visits per month may have some negative effects on readmissions. The failure to establish scientific evidence describing the underlying mechanism of how discharge planning may reduce hospitalization have hindered the effectiveness of discharge planning in reducing medical care costs. Funding for research of this nature ought to be allocated by relevant government agencies to advance the body of knowledge in this matter. Establishing a national program without fully assessing its effectiveness will have
little effect in improving the quality of care and reducing cost.
Study Limitations
This research did not distinguish between readmissions occurring due to stroke, complications associated with stroke, or other non-stroke related causes. Furthermore, it included only patients who still experienced limitations in ADL functions at the time of hospital discharge. Therefore, findings from this research do not apply to all stroke patients at discharge, and the results should be interpreted accordingly.
In this research, hospital readmission was likely to be underestimated due to the exclusion of deceased patients. The authors do not think the exclusion of deceased patients will have an effect on the direction of association between the predictors and readmissions. However, since the deceased patients tended to have worse ADL functions and had more needs for nursing care, it might have a negative effect on the magnitude of association between readmissions and need for nursing care, or number of ADL functions. In other words, the affects of these variables on readmission might be underestimated.
Recruiting patients only from seven hospitals in the Taipei metropolitan area, this study does not intend to generalize its findings to other areas in Taiwan. Regional differences in the practice of discharge planning and in post-hospital care resources may lead to geographical variations in readmission rates. Even though this study is exploratory in nature, the authors do not expect signifi-cant differences in the association between readmissions and other variables under study if the study were carried out elsewhere in Taiwan. While this study has identified some predictors of readmission, it is unable to provide the specific underlying mechanism through which the predictors influenced readmissions. Future studies should focus on identifying the underlying mechanism and the development of specific interventions to reduce read-missions.
References
Andersen, H. E., Schultz-Larsen, K., Kreiner, S., Forchhammer, B. H., Eriksen, K., & Brown, A. (2000). Can readmission after stroke be prevented? Results of a
randomized clinical study: A postdischarge follow-up service for stroke survivors. Stroke, 31(5), 1038-1045. Anderson, G. F., & Steinberg, E. P. (1984). Hospital
read-missions in the Medicare population. New England Journal of Medicine, 311(21), 1349-1353.
Berg, K., & Intrator, O. (1999). Postacute care following stroke or hip fracture: Single services and combinations used by Medicare beneficiaries (1987-1992). Journal of Aging and Health, 11(1), 27-48.
Bohannon, R. W., & Lee, N. (2003). Hospital readmissions and deaths during the first year after hospitalization for stroke. Connecticut Medicine, 67(9), 535-539. Bohannon, R. W., & Lee, N. (2004). Association of physical
functioning with same-hospital readmission after stroke. American Journal of Physical Medicine and Rehabilita-tion, 83(6), 434-438.
Camberg, L. C., Smith, N. E., Beaudet, M., Daley, J., Cagan, M., & Thibault, G. (1997). Discharge destination and repeat hospitalizations. Medical Care, 35(8), 756-767. Claesson, L., Gosman-Hedstrom, G., Fagerberg, B., & Blomstrand, C. (2003). Hospital re-admissions in rela-tion to acute stroke unit care versus convenrela-tional care in elderly patients the first year after stroke: The Goteborg 70+ Stroke study. Age and Ageing, 32(1), 109-113.
Corrigan, J. M., & Martin, J. B. (1992). Identification of fac-tors associated with hospital readmission and develop-ment of a predictive model. Health Services Research, 27(1), 81-101.
Dai, Y. T., Chang, Y., Hsieh, C. Y., & Tai, T. Y. (2003). Effec-tiveness of a pilot project of discharge planning in Taiwan. Research in Nursing and Health, 26(1), 53-63.
Department of Health, Executive Yuan. (2003). National Health Insurance statistics: Physician visits by diseases -2002. Retrieved April 7, 2005, from http://www.goh.
Gov.tw/statistic/data/ /2002/
2002.htm
Department of Health, Executive Yuan. (2004a). Statistical annual report of medical care, National Health Insur-ance: 2003. Retrieved April 7, 2005, from http://www. doh.gov.tw/EN/Webpage/List.aspx?Lmenu=Lmenu6& Rmenu=&show=show&goon=1
Department of Health, Executive Yuan. (2004b). National Health Insurance statistics: Physician visits by diseases -2003. Retrieved April 7, 2005, from http:// www. doh.
gov.tw/statistic/data/ /2003/ 2003.htm
Hoskins, L. M., Walton-Moss, B., Clark, H. M., Schroeder, M. A., & Thiel, L., Sr. (1999). Predictors of hospital read-mission among the elderly with congestive heart failure. Home Healthcare Nurse, 17(6), 373-381.
Krumholz, H. M., Parent, E. M., Tu, N., Vaccarino, V., Wang, Y., Radford, M. J., et al. (1997). Readmission after hos-pitalization for congestive heart failure among Medicare beneficiaries. Archives of Internal Medicine, 157(1), 99-104.
Kwok, T., Lum, C. M., Chan, H. S., Ma, H. M., Lee, D., & Woo, J. (2004). A randomized, controlled trial of an intensive community nurse-supported discharge pro-gram in preventing hospital readmissions of older patients with chronic lung disease. Journal of the Ameri-can Geriatrics Society, 52(8), 1240-1246.
Lee, S. H., & Wu, S. C. (1998). Determinants of burden and depression among family caregivers. Journal of Nursing Research, 6(1), 57-68.
Leibson, C. L., Naessens, J. M., Campion, M. E., Krishan, I., & Ballard, D. J. (1991). Trends in elderly hospital-ization and readmission rates for a geographically defined population: Pre- and post-prospective payment. Journal of the American Geriatrics Society, 39(9), 895-904.
Levine, J. B., Covino, N. A., Slack, W. V., Safran, C., Safran, D. B., Boro, J. E., et al. (1996). Psychological predictors of subsequent medical care among patients hospitalized with cardiac disease. Journal of Cardiopulmonary Re-habilitation, 16(2), 109-116.
Lockery, S. A., Dunkle, R. E., Kart, C. S., & Coulton, C. J. (1994). Factors contributing to the early rehospitalization of elderly people. Health and Social Work, 19(3), 182-191.
Lotus Shyu, Y. I., Chen, M. C., & Lee, H. C. (2004). Care-giver’s needs as predictors of hospital readmission for the elderly in Taiwan. Social Science and Medicine, 58(7), 1395-1403.
Naylor, M. D., Brooten, D., Campbell, R., Jacobsen, B. S., Mezey, M. D., Pauly, M. V., et al. (1999). Comprehen-sive discharge planning and home follow-up of hospital-ized elders: A randomhospital-ized clinical trial. The Journal of the American Medical Association, 281(7), 613-620.
Nikolaus, T., Specht-Leible, N., Kruse, W., Oster, P., & Schlierf, G. (1992). The early rehospitalization of elderly patients. Causes and prevention. Deutsche Medizinische Wochenschrift, 117(11), 403-407.
Ottenbacher, K. J., Smith, P. M., Illig, S. B., Fiedler, R. C., Gonzales, V., & Granger, C. V. (2001). Characteristics of persons rehospitalized after stroke rehabilitation. Ar-chives of Physical Medicine and Rehabilitation, 82(10), 1367-1374.
Rich, M. W., Beckham, V., Wittenberg, C., Leven, C. L., Freedland, K. E., & Carney, R. M. (1995). A multi-disciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. New England Journal of Medicine, 333(18), 1190-1195.
Schwarz, K. A. (2000). Predictors of early hospital read-missions of older adults who are functionally impaired. Journal of Gerontological Nursing, 26(6), 29-36. Schwarz, K. A., & Elman, C. S. (2003). Identification of
fac-tors predictive of hospital readmissions for patients with heart failure. Heart and Lung, 32(2), 88-99.
Sloan, F. A., Taylor, D. H. Jr., & Picone, G. (1999). Costs and outcomes of hip fracture and stroke, 1984 to 1994. Amer-ican Journal of Public Health, 89(6), 935-937. Soeken, K. L., Prescott, P. A., Herron, D. G., & Creasia, J.
(1991). Predictors of hospital readmission. A meta-analysis. Evaluation and the Health Professions, 14(3), 262-281.
Thorngren, M., Westling, B., & Norrving, B. (1990). Outcome after stroke in patients discharged to independent living. Stroke, 21(2), 236-240.
Wang, Y. H. (2003). The effects of implementing the expanded payment of National Health Insurance in home health care. Unpublished master’s thesis, National Taiwan University. Westert, G. P., Lagoe, R. J., Keskimaki, I., Leyland, A., & Murphy, M. (2002). An international study of hospital readmissions and related utilization in Europe and the USA. Health Policy, 61(3), 269-278.
Wolinsky, F. D., Gurney, J. G., Wan, G. J., & Bentley, D. W. (1998). The sequelae of hospitalization for ischemic stroke among older adults. Journal of the American Geriatrics Society, 46(5), 577-582.
Wray, N. P., DeBehnke, R. D., Ashton, C. M., & Dunn, J. K. (1988). Characteristics of the recurrently hospitalized adult. An information synthesis. Medical Care, 26(11), 1046-1056.