I
NTERESTING
I
MAGE
Colovesical Fistula in a Patient With Recurrent Cervical Cancer
Detected by FDG PET/CT
Kuan-Yung Chen, MD,* Chih-Hung Hsu, MD,† Chia-Hung Kao, MD,‡ Guang-Uei Hung, MD,§¶
Jainn-Shiun Chiu, MD,§ and Kuo-Wei Ho, MD§
Abstract: We report the case of a 57-year-old woman with the history of stage IB cervical cancer. She was found to have a metastatic squamous cell carcinoma in sigmoid colon. FDG PET/CT was then performed for whole-body cancer work-up. Intense FDG activity accumulated in the sigmoid tumor, with an unusually high SUVmax of 72.42, and was seen downwardly connected with the activity of urinary bladder on PET images. On the coregistered CT images, irregular wall thickening was noted for both sig-moid colon and urinary bladder with a hypodensity tract communicating with each other. It was concluded that recurrent cervical cancer involving urinary bladder and sigmoid colon resulted in colovesical fistula.
Key Words: colovesical fistula, sigmoid, cervical cancer, FDG, PET/CT (Clin Nucl Med 2010;35: 808 – 810)
REFERENCES
1. Yen TC, Lai CH. Positron emission tomography in gynecologic cancer. Semin Nucl Med. 2006;36:93–104.
2. Win Z, O’Rourke E, Todd J, et al. Vesico-colic fistula as demonstrated by 关18F兴 FDG-PET. Eur J Nucl Med Mol Imaging. 2006;33:107.
3. Pollard SG, Macfarlane R, Greatorex R, et al. Colovesical fistula. Ann R Coll Surg Engl. 1987;69:163–165.
4. Tamam M, Yavuz HS, Hacimahmutog˘lu S, et al. Direct radionuclide cystog-raphy imaging in colovesical fistula due to inguinal hernia operation compli-cation. Ann Nucl Med. 2009;23:693– 696.
5. Slavin JD Jr, Skarzynski JJ, Spencer RP. Radionuclide demonstration of urinary bladder-to-colon fistula following radiation therapy. Clin Nucl Med. 1985;10:829.
6. Najjar SF, Jamal MK, Savas JF, et al. The spectrum of colovesical fistula and diagnostic paradigm. Am J Surg. 2004;188:617– 621.
7. Buyukdereli G, Guney IB. Demonstration of vesicorectal fistula on renal scan. Clin Nucl Med. 2005;30:510 –511.
8. Balan KK, Critchley M. Vesico-colic fistula. An unexpected finding on Tc-99m MDP bone imaging. Clin Nucl Med. 1997;22:192–193.
9. Higashi K, Ohguchi M, Okimura T, et al. Demonstration of a rectovesical fistula on a technetium-99m MDP bone image. Clin Nucl Med. 1988;13:625– 626.
Received for publication February 9, 2010; revision accepted May 26, 2010. From the *Department of Radiology, Chang Bing Show Chwan Hospital,
Chan-ghua, Taiwan; †Department of General Surgery, Chang Bing Show Chwan Hospital, Changhua, Taiwan; ‡School of Medicine, China Medical Univer-sity, Taichung, Taiwan; §Department of Nuclear Medicine, Chang Bing Show Chwan Hospital, Changhua, Taiwan; and ¶Department of Biomedical Imag-ing and Radiological Science, China Medical University, Taichung, Taiwan. Reprints: Guang-Uei Hung, MD, Department of Nuclear Medicine, Chang Bing Show Chwan Hospital, 6 Lukon Rd, Lukong Town, Changhua Shien, Taiwan 505, Taiwan. E-mail: [email protected].
Copyright © 2010 by Lippincott Williams & Wilkins ISSN: 0363-9762/10/3510-0808
Clinical Nuclear Medicine • Volume 35, Number 10, October 2010
FIGURE 1. The presented case was a 57-year-old woman who had been treated for cervical cancer with radical hysterectomy,
bilateral salpingo-oophorectomy, and pelvic lymph node dissection in June 2006, and finally staged as IB. The surgery was also complicated with urinary bladder perforation, which was repaired intraoperatively. Follow-up examinations had been un-eventful until August 2009, when she was bothered by frequent dysuria and hematuria in the following 5 months. In addi-tion, she had complaints of pneumaturia occasionally. She was initially treated for urinary tract infection until she was referred for colofibroscopy in January 2010, due to an episode of bloody stool. A semicircular ulcerative mass with easy touch bleeding was found in colon at 25 cm from anal verge, initially impressed as a sigmoid colon cancer (A). However, the histopathologic ex-amination revealed a squamous cell carcinoma, hence it was considered as direct invasion of the recurrent cervical cancer (B).
Clinical Nuclear Medicine • Volume 35, Number 10, October 2010 Colovesical Fistula Detected by FDG PET/CT
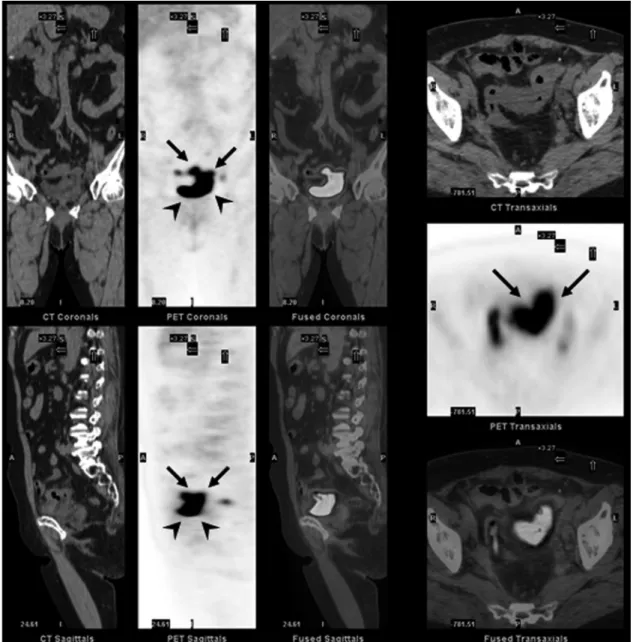
FIGURE 2. Under the impression of recurrent cervical cancer, FDG PET/CT was performed for whole-body cancer work-up.1
The transaxial, coronal, and sagittal views of CT, PET, and fused PET/CT images revealed intense accumulation of FDG activity in the sigmoid colon (arrows), which was seen downwardly connected with the activity in the urinary bladder on PET images (arrow heads). The measured 1-hour SUVmax in sigmoid colon was unusually high as 72.42, which was very close to that measured in the urinary bladder (SUVmax: 87.74) and was considered to be contaminated by urine FDG activity via a fistula.2
In addition, there was irregular wall thickening for sigmoid colon and urinary bladder, with a hypodensity tract communicat-ing both organs on the coregistered CT images, compatible with tumor invasion involvcommunicat-ing both sigmoid colon and urinary blad-der with a fistula formation (best seen on coronal views). The following cystoscopy revealed mass lesions involving superior walls of bladder. Combining the typical symptoms and the findings of PET/CT, it was concluded that recurrent cervical cancer involving both urinary bladder and sigmoid colon resulted in colovesical fistula (CVF). CVF is an abnormal connection between the bladder and large intestine, usually sigmoid colon. The most common underlying etiology was diverticular disease, followed by colon cancer, Crohn’s disease, bladder cancer, radiotherapy, and trauma.3–5The orders of presented symptoms were pneumaturia,
urinary tract infection, dysuria, fecaluria, and hematuria. CT was the modality of choice to establish the diagnosis of CVF, and colofibroscopy was followed to rule out malignancy as a cause of CVF. Barium enema and cystography were also suggested to be useful, whereas, cystoscopy and intravenous pyelogram were nondiagnostic.6The experience of FDG PET/CT, an
inte-grated metabolic and anatomic imaging modality, on CVF has not been reported before. As presented in our case, the physi-ologic urine excretion of FDG, as well as other renal excreting agents, like Tc-99m MDP and Tc-99m DTPA, makes it a very good contrast agent of urinary tracts to visualize CVF.7–9FDG PET/CT is promising in detecting CVF.
Chen et al Clinical Nuclear Medicine • Volume 35, Number 10, October 2010