1
Epidemiology of Vertigo – A National Survey
1
Ying-Ta Lai MD, 2Ting-Chuan Wang MHA, 3Li-Ju Chuang MHA,
1
Ming-Hsu Chen MD,1,3,4,5Pa-Chun Wang MD, MSc.
Affiliations/ Institution
1
Department of Otolaryngology, Cathay General Hospital, Taipei, Taiwan
2
Department of Medical Research, Cathay General Hospital, Taipei, Taiwan
3
Cathay Medical Research Institute, Taipei, Taiwan
4
Fu Jen Catholic University School of Medicine, Taipei County, Taiwan
5
Department of Public Health, College of Public Health, China Medical University
Running title: Epidemiology of Vertigo Manuscript classification: Article Word count: 2344
Financial support: none
Disclosure: No author has conflicts of interest
Correspondence:
Pa-Chun Wang MD, MSc.
Department of Otolaryngology, Cathay General Hospital 280, Sec 4. Jen-Ai Rd. 106 Taipei, Taiwan
Telephone: 8862-27082121 ext 3333 FAX: 8862-66362836
2
ABSTRACT
Objective: Vertigo is a common complaint in general population, using the National
Health Insurance (NHI) database, this study investigates the epidemiology of vertigo.
Study Design: Retrospective, cross-sectional study.
Setting: Data was retrieved from the 2006 National Healthcare Insurance (NHI) claim
database.
Subjects and Methods: Claim data were retrieved for patients aged≧18 with
diagnosis of vertigo (ICD-9-CM codes: 386.XX or 078.81) from January to December,
2006. We describe the prevalence, recurrence and medical resources utilization of
vertigo. We use logistic regression model to assess the independent effect of age, sex,
level of care, specialty, and season on the risk of vertigo recurrence.
Results: A total of 527,807 patients suffered from vertigo in 2006 (mean age
55.1±17.3 years-old, male vs. female 1: 1.96). The prevalence of vertigo was 3.13 per
100 adults. Within 1 year of index attack, 199,210 patients (37.7%) had recurrence.
The prevalence and recurrence of vertigo significantly increased with age (x2 test,
P<0.0001). Age, sex, level of care, specialty, and season had various impacts on risk
of vertigo recurrence.
Conclusions: Vertigo is a major health burden in general adult population. We also
3
female.
Key words: vertigo, prevalence, recurrence, risk factor, National Healthcare
Insurance
4
INTRODUCTION
According to the 1995 American Academy of Otolaryngology Head and Neck
Surgery guideline, vertigo is characterized as “the sensation of motion when no
motion is occurring relative to earth’s gravity”.1 Vertigo may arise from the
dysfunction of peripheral or central balance organs. Around 80% of the vertigo (such
as benign paroxysmal positional vertigo - BPPV, vestibular neuritis, and Meniere’s
disease…etc.) are resulted from peripheral causes; central type vertigo contains
severer diseases including migrainous vertigo, brainstem ischemia, cerebellar
infarction, or intra-cranial hemorrhage.2 Vertigo can disrupt a patient’s daily activities
to incur profound negative impact on his/her quality-of-life.3,4
Vertigo is a disease prevalent in the population; to improve clinical care and to
allocate medical resources appropriately, it is important to understand the prevalence
of vertigo. Unfortunately there are limited epidemiology data currently available in
the literatures. The community health questionnaire surveys show that 20-30% of the
population might have experienced symptoms of “vertigo” or “dizziness” in their life
time.5-7 A national telephone survey of Germany reveals that the lifetime prevalence
of vertigo in adults is 7.4%, with 1-year prevalence of 4.9%, 1-year incidence of 1.4%,
and with female and the elderly predominant.4 Other retrospective medical records
5
types with great variation.8,9 The accuracy of extrapolation of these studies might
have been restricted by the sampling methodology and the inconsistency in
establishing diagnoses.10,11
Taiwan implemented its universal National Health Insurance (NHI) program in
1995. So far the NHI has covered more than 97% of the population.12,13 The NHI has
collected millions of healthcare claims that can be used for healthcare study. The NHI
claims databases are now managed by Taiwan’s National Healthcare Research
Institute (NHRI) and are opened for academic researches. NHI databases are thus a
useful data research data sources for epidemiology and medical utilization studies.
Currently, there are limited domestic data regarding the occurrences of vertigo in
Taiwan. Using the 2006 NHI claim database, aims of this study are to investigate the
epidemiology and risk factors of vertigo in Taiwan. The prevalence and medical
resource utilization for vertigo are analyzed and reported.
METHODS
Data Sources
Data for this study were obtained from the Bureau of National Health Insurance
claim databases. Claim data from January to December 2006 were used. The database
contains “outpatient health expenditure file”, “outpatient order file”, “admission
6
International Classification of Diseases, Ninth Clinical Modification (ICD-9-CM) as
diagnostic codes. The population data was retrieved from registry for beneficiaries of
the Bureau of National Health Insurance (BNHI).14 The study was approved by the
IRB of the Cathay General Hospital.
Definition of Terminology
The following criteria are used for data management:
Patients: age ≧ 18 years-old.
Prevalence: defined as the proportion of population with existing disease during a
period of 1 year.
Vertigo: ICD code 386.XX or 078.81.
Index attack: defined as the first attack of vertigo occurred during year 2006.
Visit: defined as the times of outpatient clinic office visit for a patient.
Episode: office visits with same diagnosis occurred within 28 days period are defined
as within one episode of vertigo. Two episodes have to be at least 28 days apart
without any vertigo-related visit within the observed interval.
Recurrence: defined as numbers of vertigo episodes following index attack within at
least 12 months’ follow-up.
Study Population
7
excluding those co-morbid with cerebro-vascular diseases (ICD-9-CM codes 43300 to
43391, 43400 to 43491, 4358 to 4359, 436, 4378 to 4379, or 99702) during index
attack.
Statistical Analyses
We used descriptive statistical analyses (frequency, percentage, mean, and
standard deviation) to describe the medical utilization, prevalence, and characteristics
of vertigo population. We compared the frequency of prevalence and recurrence using
x2 test. Continuous variables were compared using unpaired Student’s t-test or
ANOVA. We used logistic regression model to assess the independent effect of age,
sex, level of care, specialty, and season on prevalence and recurrence of vertigo. All p
values used in these tests were two-tailed, with a level of 0.05 accepted as statistically
8
RESULTS
General Demographics of Vertigo Patients
The NHI beneficiary population aged ≧18 in Taiwan was 16,838,659 in 2006
(96% of the total population was covered).14 A total of 527,807 patients suffered from
at least one episode of vertigo, with male vs. female ratio of 1: 1.96
(M:F=178,192:349,615). The mean age of the patients was 55.1±17.3 years-old
(range 18-113). There were 931,238 episodes of vertigo that generated 1,873,040
vertigo-related visits; 6,761 episodes generated 7,070 admissions nation-wide.
Estimated Prevalence
The 527,807 vertigo patients accounted for 3.13% (527,807/16,838,659) of the
general adult population. The prevalence in general was equivalent to 3.13 per 100
adults.
Recurrence
Within 1 year of index attack, 199,210 patients (37.7% of all vertigo patients)
had at least 1 recurrence episode; in which 96,215 (48.3%) had 1, 42,950 (21.6%) had
2, 28,252 (14.2%) had 3, and 31,793 (15.9%) had more than 3 recurrent episodes.
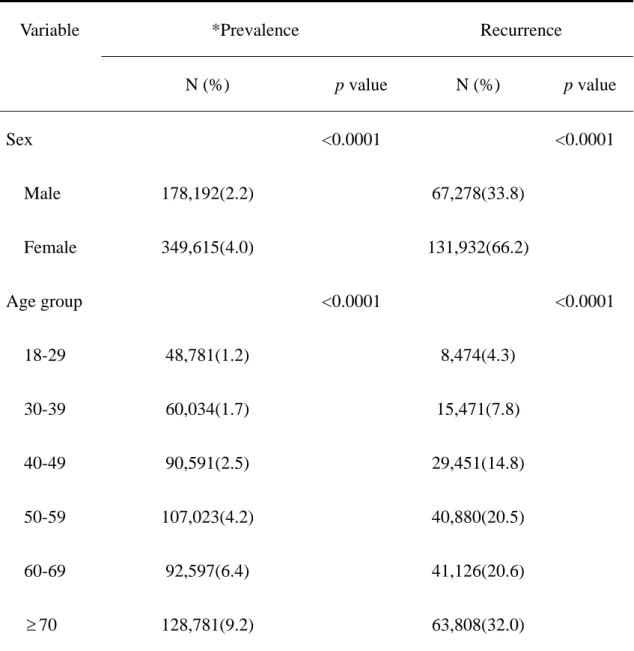
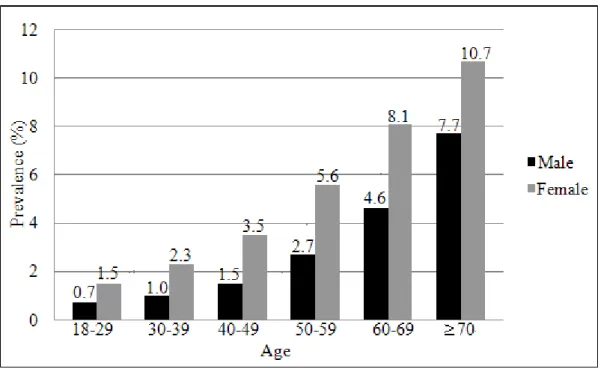
Influence of Age
Patients were categorized into 18-29, 30-39, 40-49, 50-59, 60-69, 70 age
9
(table 1, figure 1). The recurrence rates as well significantly increased with age (x2
test, P<0.0001) (table 1).
Influence of Gender
Female comprised 66.2% of the vertigo patient population. The prevalence were
2.2% in male, and 4.0% in female adult populations. There were female
predominance in all age groups (Figure 1). The recurrence rates were significantly
higher in female patients. (x2 test, P<0.0001) (Table 1).
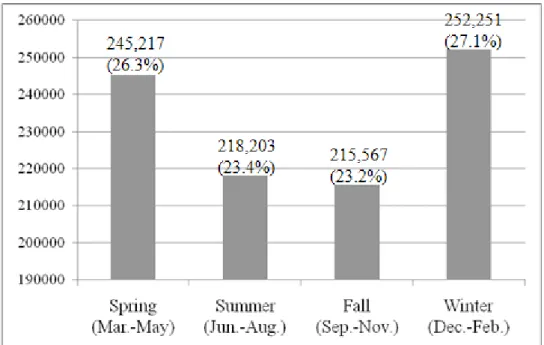
Seasonal Variation
The monthly occurrences are shown in figure 2. Winter (27.1%) and spring
(26.3%) had higher occurrences. January had highest occurrence rate (12.9%) among
all months in a year.
Diagnosis
The ICD-9 codes analyses show that 386.1 (other and unspecified peripheral
vertigo), 386.9 (unspecified vertiginous syndromes and labyrinthine disorders) and
386.0 (Meniere's disease) are the most common used codes (38.5%, 25.7%, and
21.6% respectively), followed by 386.2 (vertigo of central origin, 10.1%), 386.5
(labyrinthine dysfunction, 3.2%), 386.3 (labyrinthitis, 0.8%), 386.8 (other disorders of
labyrinth, 0.1%), and 386.4 (labyrinthine fistula, 0.01%).
10
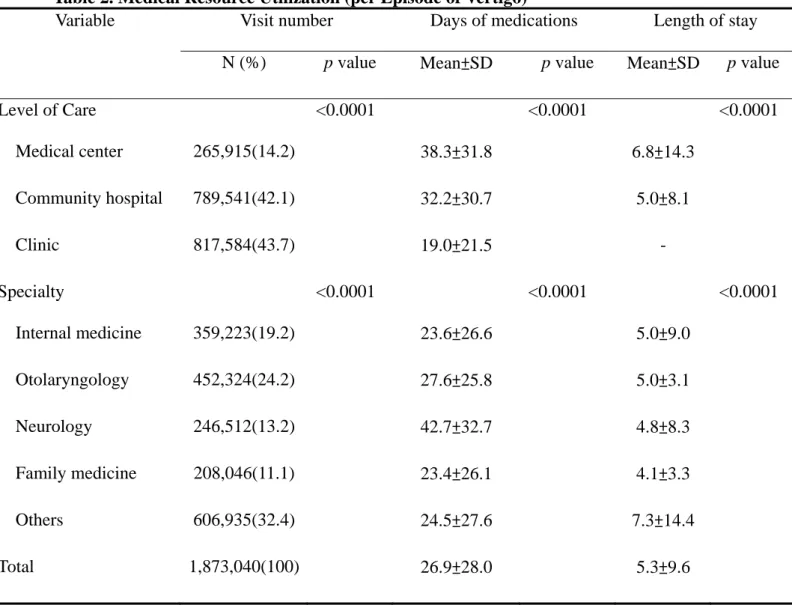
Most of the vertigo were cared at primary care level (817,534 visits, 43.7%),
followed by at community hospital (789,541 visits, 42.2%), and medical center
(265,915 visits, 14.2%) levels. The patients were treated by otolaryngology (452,324
visits, 24.2%), internal medicine (359,223 visits, 19.2%), neurology (246,512 visits,
13.2%), and general practitioner (208,046 visits, 11.1%). In general, the length of
medication for every episode was 26.9±28.0 days. The per episode lengths of
medication were different among different levels of care institutions (clinics
19.0±21.5 days, community hospital 32.2±30.7 days, medical center 38.3±31.8 days,
ANOVA, P<0.0001), among different subspecialties (internal medicine 23.6±26.6
days, otolaryngology 27.6±25.8 days, general practitioner 23.4±26.1 days, neurology
42.7±32.7 days, ANOVA, P<0.0001).
Each episode would take 2.0±1.4 visits to treat in general. The treatment visits
per episode were different among different levels of care institutions (clinics 1.9±1.5
visits, community hospital 2.1±1.4 visits, medical center 2.1±1.3 visits, ANOVA,
P<0.0001).
For the 7,070 vertigo-related admissions, the length of stay was 5.3±9.6 days in
general. The length of stay significantly differed among different levels of care
institutes (community hospital 5.0±8.1 days, medical center 6.8±14.3 days, t-test,
11
otolaryngology 5.0±3.1 days, general practitioner 4.1±3.3 days, neurology 4.8±8.3
days, P<0.0001), and among different age groups as well (Table 2).
Risk Factors for Recurrence
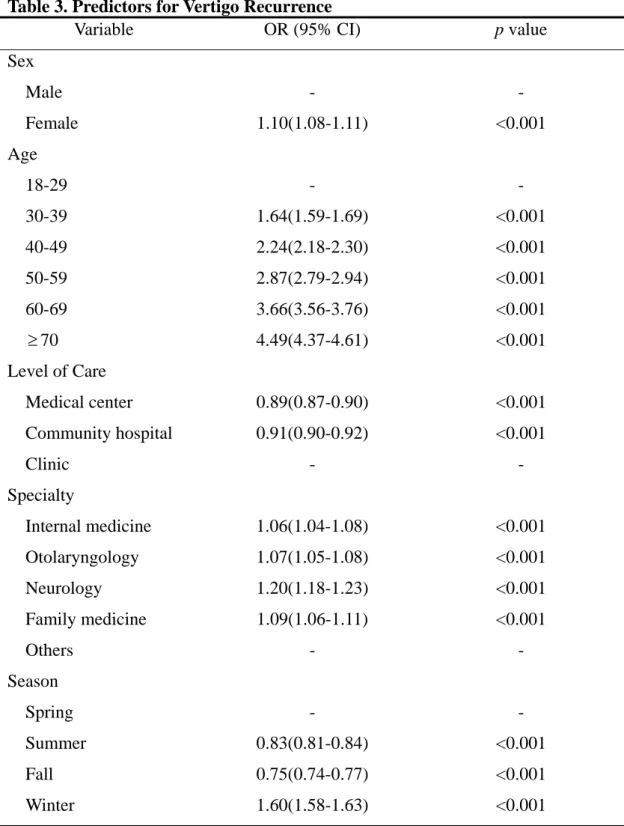
Logistic regression model revealed that age, sex, level of care, specialty, and
season had various impacts on risk of vertigo recurrence. Female patients had
significantly higher odd ratio (OR) of recurrence than male patients (OR=1.10, 95%
CI 1.08 to 1.11). Compared to those aged 18-29 years, the patients aged 30-39 years
(OR=1.64, 95% CI 1.59 to 1.69), 40-49 years (OR=2.24, 95% CI 2.18 to 2.30), 50-59
years (OR=2.87, 95% CI 2.79 to 2.94), 60-69 years (OR=3.66, 95% CI 3.56 to 3.76),
and 70 years or older (OR=4.49, 95% CI 4.37 to 4.61) all had significantly increased
OR of recurrence.
As compared to level of care at clinics, the patients cared in community hospital
(OR=0.91, 95% CI 0.90 to 0.92) and in medical centers (OR=0.89, 95% CI 0.87 to
0.90) both had significantly reduced OR of recurrence.
As compared to non-categorized physicians (others), patients cared by
neurologist (OR=1.20, 95% CI 1.18 to 1.23), general practitioner (OR=1.09, 95% CI
1.06 to 1.11), otolaryngologists (OR=1.07, 95% CI 1.05 to 1.08), and internist
(OR=1.06, 95% CI 1.04 to 1.08) were associated with a significantly increased OR of
12
As compared to spring attack, the patients had significantly reduced OR of
recurrence when their initial attack occurred in summer (OR=0.83, 95% CI 0.81 to
0.84) and in fall (OR=0.75, 95% CI 0.74 to 0.77). Patients with initial attack in winter
had a significantly higher OR of recurrence than those in spring (OR=1.60, 95% CI
1.58 to 1.63) (Table 3).
DISCUSSION
Vertigo Epidemiology in General
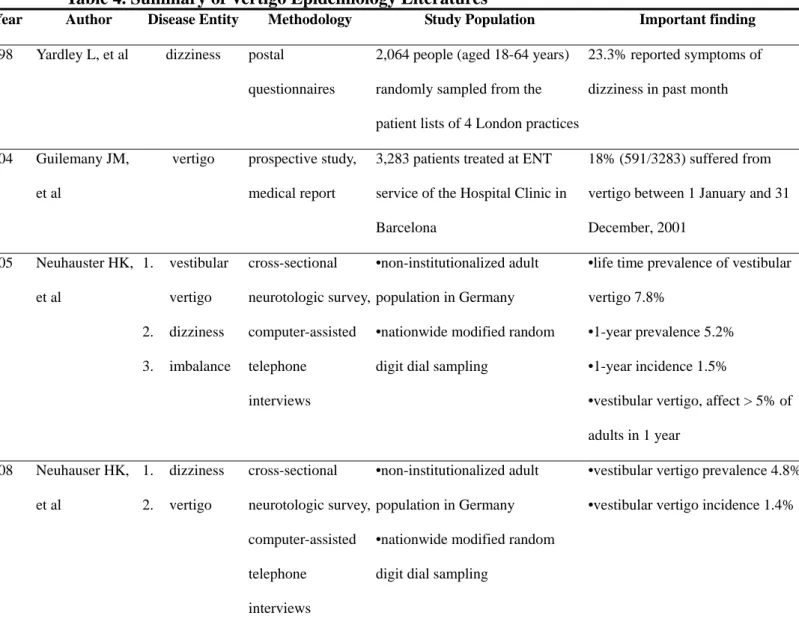
Dizziness, vertigo, and imbalance are common patient complaints. Hannaford et
al. reported that nearly 21% of ear, nose, throat patients had “spinning dizziness”
problem in the previous year.7 Yardley L et al. 6 by studying 4 London local practices,
reported that dizziness may account for 23.3% of the patient complaints (Table 4). As
an important disease entity in neurology and otolaryngology clinical practice, accurate
prevalence is however hard to estimate due to the difficulty in making differential
diagnoses.2 There are currently limited information on the epidemiology of vertigo in
general (Table 4), and the data are hardly comparable owing to the variability of study
designs.4,6,15,16 In this claim database study, we estimated that during year 2006, the
prevalence of vertigo was 3.13% in Taiwan. The data was close to the 4.8%-5.2%
1-year prevalence estimated by Neuhauser’s national telephone questionnaire
13
Recurrence
Recurrence is commonly seen in vertigo patients; the nature course of vertigo is
a topic of interest in several studies.17-20 Neuhauser et al.4 showed life-long recurrent
vestibular vertigo in 89% of patients. In a 10-year follow-up study of patients with
BPPV, the recurrence rate was 50%; 80% of these recurred in the 1st year.20
Tokumasu et al. reported 51.7% of Meniere’s disease recurrence in a 16-year
observation study; 78.6% recurred in the 1st year following initial attack.18 The mean
vertigo frequency was 4.5 episodes per year.19 In this study, we estimated that the
1-year vertigo recurrence rate was 37.7% in general; 15.9% of them had more than 3
recurrent episodes in 1 year. Patients cared by specialists (otolaryngologist, internal
medicine, and neurologist) had higher recurrence rates, probably attributed to the
severity or patterns of diseases.
Risk Factor
Most of the epidemiological studies on vertigo dealt with age and gender. It is
generally agreed that vertigo prevalence may increase with age, especially in female.
A cross-sectional, nation-wide neurological survey in Germany showed the mean age
of vertigo onset was 49.4 years; and the prevalence was higher in women.21 Dieterich
et al.22 reported 1.5 times higher prevalence rate for migrainous vertigo in female. As
14
age was 42 in men and 41 in women. In this study, our data attest that prevalence and
recurrence both increased with age, and with female predominance (Table 3, Figure
2).
Season of vertigo onset is another interesting issue. Wladislavosky-Waserman et
al.24 found that patients with Meniere’s disease were evenly distributed throughout the
year, except for a slight increase at the end of the winter and beginning of the spring.
Similar findings were reported by Mizukoshi et al.8 Our data are compatible with
others by showing relatively higher vertigo occurrences in winter and spring (Figure
1).
Healthcare Utilization
Vertigo ranks among the most frequent complaints in neurology and
otolaryngology practices, as so it is important to understand the medical resource
consumption resulted from vertigo treatment. Neuhauser et al.16 reported that 58% of
patients with dizziness would have at least 1 medical consultation in their life time.
Half of the patients were seen by primary care physicians, and the other half
frequently went to neurologists or otolaryngologists. Our data show most of vertigo
patients were taken care by otolaryngologists, internal medicine doctors, or
neurologists at primary care level (Table 2). The admission rate of 1.2%
15
It is note-worthy to find that recurrence rates were lower in patients treated in
hospital level care institutions. We speculate that this may attribute to the longer and
complete medication prescribed by these institutions (Table 2).
Methodology and Study Limitation
The NHI data base proves to be useful to provide epidemiological data of vertigo.
However, there is no clinical and severity information in the dataset. The accuracy of
diagnosis coding from healthcare provider may affect the validity of data, fortunately
the BNHI has enforced several measures to cross-check and to monitor the accuracy
of diagnostic coding. We found most of the providers were not able to further
differentiate actual diagnoses of vertigo at index visits. The prevalence of Meniere’s
disease, BPPV, or vestibular neuritis can not be estimated from this study. And, since
we defined “2 vertigo episodes have to be a least 28 days apart” to overcome the
arbitrary NHI prescription days restriction (3 days for clinics, 7 days for hospitals, 28
days for chronic condition), this may cause under-estimation of actual prevalence and
recurrences of vertigo.
CONCLUSION
There are limited epidemiological data currently available in the literatures. In
this study we found vertigo is a major health burden in general adult population.
16
representing an annual prevalence of 3.13 per 100 adults; the overall recurrence rate
was 37.7%. We found elder female patients had higher vertigo occurrence rates.
ACKNOWLEDGEMENT
This study is based in part on data from the National Health Insurance Research
Database provided by the Bureau of National Health Insurance, Department of Health
and managed by National Health Research Institutes. The interpretation and
conclusions contained herein do not represent those of Bureau of National Health
Insurance, Department of Health or National Health Research Institutes of Taiwan,
17
REFERENCES
1. Monsell EM, Balkany TA, Gates GA, et al. Committee on hearing and equilibrium
guidelines for the diagnosis and evaluation of therapy in Meniere's disease.
Otolaryngol Head Neck Surg 1995;113:186-7.
2. Kroenke K, Hoffman RM, Einstadter D. How common are various causes of
dizziness? South Med J 2000;93:160-7.
3. Lopez-Escamez JA, Gamiz MJ, Fernandez-Perez A, et al. Impact of treatment on
health-related quality of life in patients with posterior canal benign paroxysmal
positional vertigo. Otol Neurotol 2003;24:637-41.
4. Neuhauser HK, von Brevern M, Radtke A, et al. Epidemiology of vestibular
vertigo: a neurotologic survey of the general population. Neurology
2005;27;65:898-904.
5. Kroenke K, Price RK. Symptoms in the community. Prevalence, classification,
and psychiatric comorbidity. Arch Intern Med 1993;153:2474-80.
6. Yardley L, Owen N, Nazareth I, et al. Prevalence and presentation of dizziness in
a general practice community sample of working age people. Br J Gen Pract
1998;48:1131-5.
7. Hannaford PC, Simpson JA, Bisset AF, et al. The prevalence of ear, nose and
18
survey in Scotland. Fam Pract 2005;22:227-33.
8. Mizukoshi K, Watanabe Y, Shojaku H, et al. Epidemiological studies on benign
paroxysmal positional vertigo in Japan. Acta Otolaryngol Suppl 1988;447:67-72.
9. Froehling DA, Silverstein MD, Mohr DN, et al. Benign positional vertigo:
incidence and prognosis in a population-based study in Olmsted County,
Minnesota. Mayo Clin Proc 1991;66:596-601.
10. Neuhauser H K. Epidemiology of vertigo. Curr Opin Neurol 2007;20:40–6.
11. da Costa SS, de Sousa LC, Piza MR. Meniere's disease: overview, epidemiology,
and natural history. Otolaryngol Clin North Am 2002;35:455-95.
12. Cheng TM. Taiwan's new national health insurance program: genesis and
experience so far. Health Aff (Millwood) 2003;22:61-76.
13. Lu JF, Hsiao WC Does universal health insurance make health care unaffordable?
Lessons from Taiwan. Health Aff (Millwood) 2003;22:77-88.
14. Bureau of National Health Insurance. Beneficiaries by gender and age (May,
2007). Available at: www.nhi.gov.tw/webdata/AttachFiles/
Attach_10358_1_95-T6.XLS. Accessed November 18, 2009.
15. Guilemany JM, Martínez P, Prades E,et al. Clinical and epidemiological study of
19
16. Neuhauser HK, Radtke A, von Brevern M, et al. Burden of dizziness and vertigo
in the community. Arch Intern Med 2008;168:2118-24.
17. Perez-Garrigues H, Lopez-Escamez JA, Perez P, et al. Time course of episodes of
definitive vertigo in Meniere's disease. Arch Otolaryngol Head Neck Surg
2008;134:1149-54.
18. Tokumasu K, Fujino A, Naganuma H, et al. Initial symptoms and retrospective
evaluation of prognosis in Menière's disease. Acta Otolaryngol Suppl
1996;524:43-9
19. Tokumasu K, Fujino A, Yoshio S, et al. Prognosis of Menière's disease by
conservative treatment: retrospective study on the time course of the disease. Acta
Otolaryngol Suppl 1995;519:216-8.
20. Brandt T, Huppert D, Hecht J, et al. Benign paroxysmal positioning vertigo: a
long-term follow-up (6-17 years) of 125 patients. Acta Otolaryngol
2006;126:160-3.
21. von Brevern M, Radtke A, Lezius F, et al. Epidemiology of benign paroxysmal
positional vertigo: a population based study. J Neurol Neurosurg Psychiatry
2007;78:710-5.
22. Dieterich M, Brandt T. Episodic vertigo related to migraine (90 cases): vestibular
20
23. Watanabe Y, Mizukoshi K, Shojaku H, et al. Epidemiological and clinical
characteristics of Meniere’s disease in Japan. Acta Otolaryngol 1995;519:206–10.
24. Wladislavosky-Waserman P, Facer GW, Mokri B, et al. Meniere's disease: a
30-year epidemiologic and clinical study in Rochester, Mn, 1951-1980.
21
FIGURE LEGEND
Figure 1. Gender and Age Distribution of Vertigo
22
TABLES AND FIGURES
Table 1. Prevalence and Recurrence of Vertigo
Variable *Prevalence Recurrence
N (%) p value N (%) p value Sex <0.0001 <0.0001 Male 178,192(2.2) 67,278(33.8) Female 349,615(4.0) 131,932(66.2) Age group <0.0001 <0.0001 18-29 48,781(1.2) 8,474(4.3) 30-39 60,034(1.7) 15,471(7.8) 40-49 90,591(2.5) 29,451(14.8) 50-59 107,023(4.2) 40,880(20.5) 60-69 92,597(6.4) 41,126(20.6) 70 128,781(9.2) 63,808(32.0)
23
Table 2. Medical Resource Utilization (per Episode of Vertigo)
Variable Visit number Days of medications Length of stay
N (%) p value Mean±SD p value Mean±SD p value
Level of Care <0.0001 <0.0001 <0.0001 Medical center 265,915(14.2) 38.3±31.8 6.8±14.3 Community hospital 789,541(42.1) 32.2±30.7 5.0±8.1 Clinic 817,584(43.7) 19.0±21.5 - Specialty <0.0001 <0.0001 <0.0001 Internal medicine 359,223(19.2) 23.6±26.6 5.0±9.0 Otolaryngology 452,324(24.2) 27.6±25.8 5.0±3.1 Neurology 246,512(13.2) 42.7±32.7 4.8±8.3 Family medicine 208,046(11.1) 23.4±26.1 4.1±3.3 Others 606,935(32.4) 24.5±27.6 7.3±14.4 Total 1,873,040(100) 26.9±28.0 5.3±9.6
24
Table 3. Predictors for Vertigo Recurrence
Variable OR (95% CI) p value
Sex Male - - Female 1.10(1.08-1.11) <0.001 Age 18-29 - - 30-39 1.64(1.59-1.69) <0.001 40-49 2.24(2.18-2.30) <0.001 50-59 2.87(2.79-2.94) <0.001 60-69 3.66(3.56-3.76) <0.001 70 4.49(4.37-4.61) <0.001 Level of Care Medical center 0.89(0.87-0.90) <0.001 Community hospital 0.91(0.90-0.92) <0.001 Clinic - - Specialty Internal medicine 1.06(1.04-1.08) <0.001 Otolaryngology 1.07(1.05-1.08) <0.001 Neurology 1.20(1.18-1.23) <0.001 Family medicine 1.09(1.06-1.11) <0.001 Others - - Season Spring - - Summer 0.83(0.81-0.84) <0.001 Fall 0.75(0.74-0.77) <0.001 Winter 1.60(1.58-1.63) <0.001
25
Table 4. Summary of Vertigo Epidemiology Literatures
Year Author Disease Entity Methodology Study Population Important finding
1998 Yardley L, et al dizziness postal questionnaires
2,064 people (aged 18-64 years) randomly sampled from the patient lists of 4 London practices
23.3% reported symptoms of dizziness in past month
2004 Guilemany JM, et al
vertigo prospective study, medical report
3,283 patients treated at ENT service of the Hospital Clinic in Barcelona
18% (591/3283) suffered from vertigo between 1 January and 31 December, 2001 2005 Neuhauster HK, et al 1. vestibular vertigo 2. dizziness 3. imbalance cross-sectional neurotologic survey, computer-assisted telephone interviews •non-institutionalized adult population in Germany •nationwide modified random digit dial sampling
•life time prevalence of vestibular vertigo 7.8%
•1-year prevalence 5.2% •1-year incidence 1.5%
•vestibular vertigo, affect > 5% of adults in 1 year 2008 Neuhauser HK, et al 1. dizziness 2. vertigo cross-sectional neurotologic survey, computer-assisted telephone interviews •non-institutionalized adult population in Germany •nationwide modified random digit dial sampling
•vestibular vertigo prevalence 4.8% •vestibular vertigo incidence 1.4%
26
27
Figure 2. Seasonal Variation of Vertigo
245,217 (26.3%) 218,203 (23.4%) 215,567 (23.2%) 252,251 (27.1%)