Associations of Cyclooxygenase 2 Polymorphic Genotypes with Bladder Cancer Risk in Taiwan
WEN-SHIN CHANG1,3,*, CHIA-WEN TSAI2,3,*, HONG-XUE JI3,4,*, HSI-CHIN WU3,
YI-TING CHANG3,4, CHI-SHUN LIEN3,5, WEN-LING LIAO3, WU-CHUNG SHEN4,
CHANG-HAI TSAI3 and DA-TIAN BAU1,2,3
Graduate Institutes of 1Clinical Medical Science, 2Basic Medical Science, China Medical
University, Taichung, Taiwan, ROC;
3Terry Fox Cancer Research Laboratory, China Medical University Hospital, Taichung,
Taiwan, ROC;
4Department of Biomedical Imaging and Radiological Science, China Medical University,
Taichung, Taiwan, ROC;
5Department of Urology, China Medical University Hospital, Taichung, Taiwan, ROC.
* These Authors contributed equally to this work
Correspondence to: Da-Tian Bau, Terry Fox Cancer Research Lab, China Medical University Hospital, 2 Yuh-Der Road, Taichung, 404 Taiwan, Tel: +886 422052121 Ext
1523, Fax: +886 422053366 Ext. 1511, e-mail:
[email protected]/[email protected]
Running title: Chang et al: Cox-2 Genotypes in Bladder Cancer
Abstract. Aim: Bladder cancer is the sixth most common cancer worldwide and its incidence is particularly high in southwestern Taiwan. However, the genetic contribution to its etiology is not well-understood. The aim of this study is to evaluate the association of cyclooxygenase 2 (Cox-2) polymorphic genotypes with Taiwan bladder cancer patients. Materials and Methods: Six polymorphic variants of Cox-2 were analyzed of their association with bladder cancer risk, and three hundred and seventy-five patients with bladder cancer and same amount of age- and gender-matched healthy controls recruited were genotyped by PCR-RFLP method. Results: Among the six polymorphic sites examined, only the Cox-2 promoter G-765C (rs20417) genotypes were positively associated with bladder cancer risk (p=0.0102). Individuals with the Cox-2 -765GC genotypes were associated with higher prostate cancer risk than those with -765GG. Conclusion: Our findings provide evidence that the C allele of Cox-2 promoter G-765C may be associated with the overexpression of COX-2 during bladder cancer development and may be a useful marker for early detection of bladder cancer.
Bladder cancer is the most serious urinary neoplasm all over the world. In the western countries, bladder cancer has been the fourth most common cancer among males, accounting for 7% of the total malignancies (1). In Taiwan, bladder cancer ranks seventh in incidence and mortality among common carcinomas (2). Carcinogenesis of bladder cancer is a complex, multi-step and multi-factorial process resulting from interactions between both environmental and genetic factors. In literature, the environmental risk factors for bladder carcinogenesis may include cigarette smoking, carcinogenic aromatic amine exposure and harmful drug consumption, such as phenacetine, chlornaphrazine and cyclophosphamide (3, 4).
Cyclooxygenases (also known as prostaglandin endoperoxide synthases, PTGSs) are key enzymes that convert arachidonic acids to prostaglandin H2 (5). There are two
forms of cyclooxygenases, Cox-1 and Cox-2. Cox-1 is a housekeeping enzyme involved in intracellular signaling, whereas Cox-2 is absent from many cell types unless induced by tumor promoters, growth factors, or cytokines (6-8). Accumulating evidence has shown that up-regulation of Cox-2 is closely-associated with malignant progression (9-12). Evidence collected from mRNA and protein levels of Cox-2 showed that levels may vary dramatically among the investigated subjects, and the variation may be partially determined by genetic variations, such as single nucleotide polymorphisms (SNPs) of Cox-2 itself (13, 14).
In literature, the association between SNPs of Cox-2 and bladder cancer susceptibility has been examined in Korean (15), New England (16), and India (17) populations, however, never among Taiwanese. The present work is aiming at two purposes, one is to perform the large case-control genotyping study of bladder cancer in Taiwan, a highly genetically-conserved population; the other is to examine the biological plausibility that genetic variation of Cox-2 could alter its coded enzyme
expression levels or biochemical function and consequently have an impact on modifying the individual risk for bladder cancer. To examine the above hypothesis that the SNP variants of Cox-2 are associated with the risk of bladder cancer, the genetic polymorphisms of six Cox-2 SNPs, including G-1195A (rs689466), G-765C (rs20417), T+8473C (rs5275), intron 1 (rs2745557), intron 5 (rs16825748), and intron 6 (rs2066826), were analyzed in a Taiwanese population (control/case:375/375).
Materials and Methods
Study population and sample collection. Three hundred and seventy-five patients diagnosed with bladder cancer were recruited at the outpatient clinics of general surgery between 2003-2009 at the China Medical University Hospital, Taichung, Taiwan, Republic of China. All patients who voluntarily participated, completed a self-administered questionnaire and provided peripheral blood samples. As many of non-bladder cancer healthy controls were selected by matching for age and gender after initial random sampling from the Health Examination Cohort of the hospital. Exclusion criteria of the control group included previous malignancy, metastasized cancer from other or unknown origin, and any familial or genetic diseases. In addition, all members in the two groups completed a short questionnaire.
Genotyping assays. Genomic DNA was prepared from peripheral blood leukocytes of each subject using a QIAamp Blood Mini Kit (Blossom, Taipei, Taiwan) and further processed as previous genotyping studies (18-21). The polymerase chain reaction (PCR) cycling conditions for all the six genotyping work were: one cycle at 94°C for 5 min; 35 cycles of 94°C for 30 sec, 55°C for 30 sec, and 72°C for 30 sec, and a final extension at 72°C for 10 min. The PCR primer sequences and restriction enzyme for
each DNA product are listed in Table I.
Statistical analyses. To ensure that the controls used were representative of the general population, and to exclude the possibility of genotyping error, the deviation of the genotype frequencies of Cox-2 SNPs in the controls from those expected under the Hardy-Weinberg equilibrium was assessed using the goodness-of-fit test. Pearson’s chi-square test or Fisher’s exact test (when the number in any cell was less than five) was used to compare the distribution of the genotypes between cases and controls. Data were deemed significant when p<0.05. Cancer risk associated with the genotypes was estimated as odds ratios (ORs) and 95% confidence intervals (95%CIs) using unconditional logistic regression.
Results
The frequency distributions for age, gender, cigarette smoking and alcohol drinking habits of the 375 bladder cancer patients and 375 controls are shown in Table II. The characteristics of the patients and controls were all well-matched. None of the differences in these characteristics between both groups were statistically significant (p>0.05) (Table II).
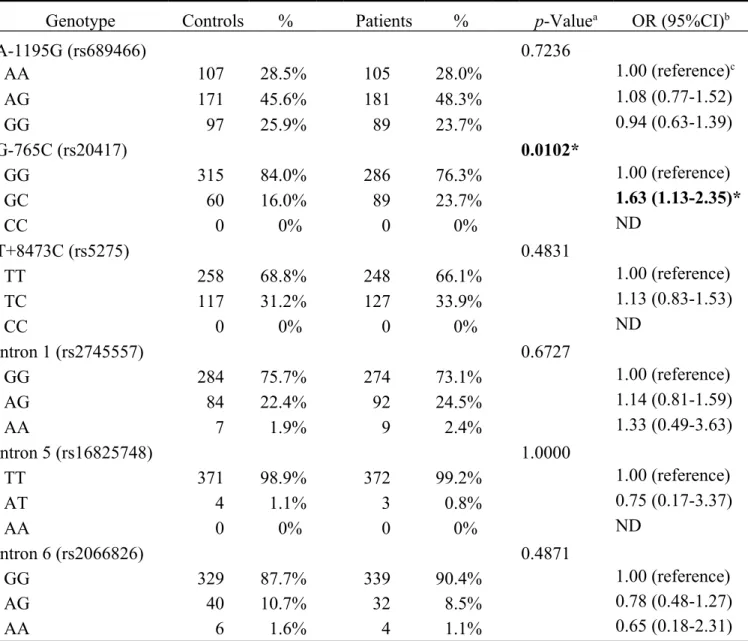
The distribution of the genotypic frequencies for the Cox-2 SNPs in controls and bladder cancer patients are shown in Table III. The genotypic frequencies of Cox-2 promoter G-765C polymorphism were differentially distributed between bladder cancer and control groups (p=0.0102), while those for other five polymorphisms were not significant, (p>0.05) (Table III). In detail, compared to those with GG, patients with the GC genotype may have 1.63-fold OR of bladder cancer susceptibility (95%CI=1.13-2.35).
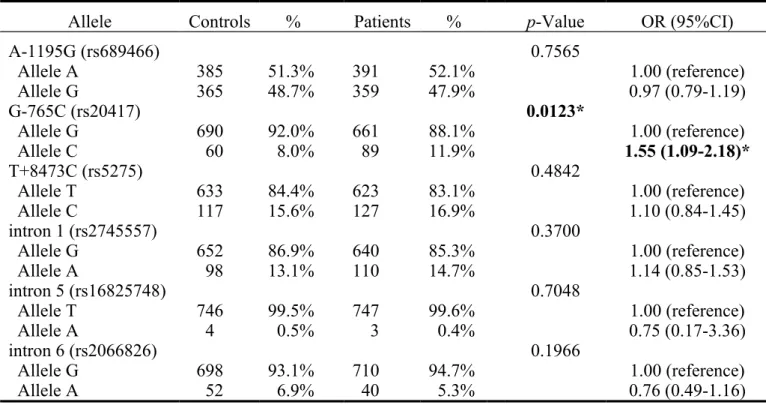
The frequencies of the alleles for Cox-2 SNPs in controls and bladder cancer patients are shown in Table IV. The C allele of the Cox-2 promoter G-765C polymorphism was found to be associated with bladder cancer (p=0.0123). Compared to those with G allele, genotypes with C allele at Cox-2 promoter G-765C may have 1.55-fold higher OR of bladder cancer susceptibility (95%CI=1.09-2.18). Thus, from the data in Tables III and IV it can be concluded that the Cox-2 promoter -765G allele appears to be associated with higher risk for bladder cancer in Taiwan, while the other Cox-2 genotypes investigated in this study do not.
In recent literature, several studies have demonstrated that variant genotypes in Cox-2 were associated with the risk of prostate cancer (22-27). However, there is no article investigating its association with bladder cancer.
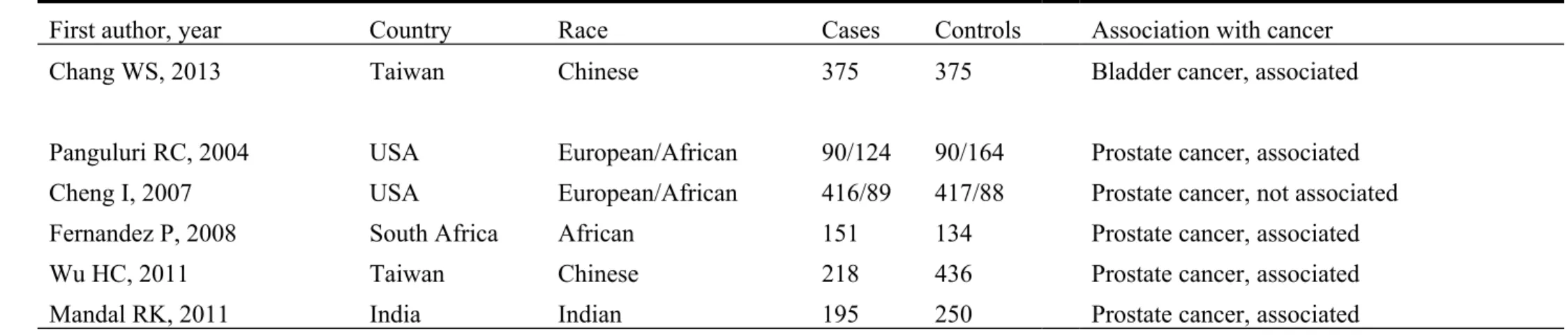
In the present study one variant, GC genotype of G-765C (rs20417) was associated with an increased risk of bladder cancer among Taiwanese, while no other variant did (Table III). In the allelic frequency analysis, the C allele was found to be associated with a higher risk of bladder cancer (Table IV). We have summarized the findings of the present study together with other reports in prostate cancer in Table V. These findings are of pioneer significance for other groups to investigate its contribution in other populations. As for ourselves, further studies with larger population and the detail mechanisms are warranted, and should be compared with updated multi-ethnic studies to elucidate the role of Cox-2 in bladder cancer. Furthermore, sophisticated gene-gene and gene-environment interactions together with the contribution of Cox-2 genotype to prognosis of bladder cancer patients may be looked forward in the near future.
To sum up, this is the first study to demonstrate that genetic variation in Cox-2 may influence the risk of bladder cancer. The presence of the C allele of promoter -765 was found to be associated with a higher risk of bladder cancer and this finding supports previous reports showing an association between Cox-2 variants and urinary cancer risk (23-27). We have provided evidence for a potent biomarker for bladder cancer early detection in Taiwanese and maybe for other countries.
Acknowledgements
The Authors appreciate Chieh-Lun Hsiao, Chia-En Miao, Lin-Lin Hou, Chao-Yi Lai, Tsai-Ping Ho and the Tissue Bank at the China Medical University for their technical assistance. This study was supported by research grants from the Terry Fox Cancer Research Foundation.
References
1 Franekova M, Halasova E, Bukovska E, Luptak J and Dobrota D: Gene polymorphisms in bladder cancer. Urol Oncol 26: 1-8, 2008.
2 Wang YH, Lee YH, Tseng PT, Shen CH and Chiou HY: Human NAD(P)H:quinone oxidoreductase 1 (NQO1) and sulfotransferase 1A1 (SULT1A1) polymorphisms and urothelial cancer risk in Taiwan. J Cancer Res Clin Oncol 134: 203-209, 2008.
3 Steineck G, Wiholm BE and Gerhardsson de Verdier M: Acetaminophen, some other drugs, some diseases and the risk of transitional cell carcinoma. A population-based case-control study. Acta Oncol 34: 741-748, 1995.
4 Cohen SM, Shirai T and Steineck G: Epidemiology and etiology of premalignant and malignant urothelial changes. Scand J Urol Nephrol Suppl: 105-115, 2000.
5 DeWitt DL: Prostaglandin endoperoxide synthase: regulation of enzyme expression. Biochim Biophys Acta 1083: 121-134, 1991.
6 Kujubu DA, Reddy ST, Fletcher BS and Herschman HR: Expression of the protein product of the prostaglandin synthase-2/TIS10 gene in mitogen-stimulated Swiss 3T3 cells. J Biol Chem 268: 5425-5430, 1993.
7 Kawata R, Reddy ST, Wolner B and Herschman HR: Prostaglandin synthase 1 and prostaglandin synthase 2 both participate in activation-induced prostaglandin D2 production in mast cells. J Immunol 155: 818-825, 1995. 8 Reddy ST and Herschman HR: Ligand-induced prostaglandin synthesis
requires expression of the TIS10/PGS-2 prostaglandin synthase gene in murine fibroblasts and macrophages. J Biol Chem 269: 15473-15480, 1994. 9 Fujimura T, Ohta T, Oyama K, Miyashita T and Miwa K: Role of
cyclooxygenase-2 in the carcinogenesis of gastrointestinal tract cancers: a review and report of personal experience. World J Gastroenterol 12:
1336-1345, 2006.
10 Marshall SF, Bernstein L, Anton-Culver H, Deapen D, Horn-Ross PL, Mohrenweiser H, Peel D, Pinder R, Purdie DM, Reynolds P, Stram D, West D, Wright WE, Ziogas A and Ross RK: Nonsteroidal anti-inflammatory drug use and breast cancer risk by stage and hormone receptor status. J Natl Cancer Inst 97: 805-812, 2005.
11 van Rees BP and Ristimaki A: Cyclooxygenase-2 in carcinogenesis of the gastrointestinal tract. Scand J Gastroenterol 36: 897-903, 2001.
12 Wang W, Bergh A and Damber JE: Cyclooxygenase-2 expression correlates with local chronic inflammation and tumor neovascularization in human prostate cancer. Clin Cancer Res 11: 3250-3256, 2005.
13 Cok SJ and Morrison AR: The 3'-untranslated region of murine cyclooxygenase-2 contains multiple regulatory elements that alter message stability and translational efficiency. J Biol Chem 276: 23179-23185, 2001. 14 Papafili A, Hill MR, Brull DJ, McAnulty RJ, Marshall RP, Humphries SE and
Laurent GJ: Common promoter variant in cyclooxygenase-2 represses gene expression: evidence of role in acute-phase inflammatory response. Arterioscler Thromb Vasc Biol 22: 1631-1636, 2002.
15 Kang S, Kim YB, Kim MH, Yoon KS, Kim JW, Park NH, Song YS, Kang D, Yoo KY, Kang SB and Lee HP: Polymorphism in the nuclear factor kappa-B binding promoter region of cyclooxygenase-2 is associated with an increased risk of bladder cancer. Cancer Lett 217: 11-16, 2005.
16 Baris D, Karagas MR, Koutros S, Colt JS, Johnson A, Schwenn M, Fischer AH, Figueroa JD, Berndt SI, Han S, Beane Freeman LE, Lubin JH, Cherala S, Cantor KP, Jacobs K, Chanock S, Chatterjee N, Rothman N and Silverman DT: Nonsteroidal anti-inflammatory drugs and other analgesic use and bladder
cancer in northern New England. Int J Cancer 132: 162-173, 2013.
17 Gangwar R, Mandhani A and Mittal RD: Functional polymorphisms of cyclooxygenase-2 (COX-2) gene and risk for urinary bladder cancer in North India. Surgery 149: 126-134, 2011.
18 Hsia TC, Tsai CW, Liang SJ, Chang WS, Lin LY, Chen WC, Tu CY, Tsai CH and Bau DT: Effects of ataxia telangiectasia mutated (ATM) genotypes and smoking habits on lung cancer risk in Taiwan. Anticancer Res 33: 4067-4071, 2013.
19 Tsai CW, Tsai MH, Shih LC, Chang WS, Lin CC and Bau DT: Association of interleukin-10 (IL10) promoter genotypes with nasopharyngeal carcinoma risk in Taiwan. Anticancer Res 33: 3391-3396, 2013.
20 Chang WS, Ke HL, Tsai CW, Lien CS, Liao WL, Lin HH, Lee MH, Wu HC, Chang CH, Chen CC, Lee HZ and Bau DT: The role of XRCC6 T-991C functional polymorphism in renal cell carcinoma. Anticancer Res 32: 3855-3860, 2012.
21 Chang WS, Yang MD, Tsai CW, Cheng LH, Jeng LB, Lo WC, Lin CH, Huang CY and Bau DT: Association of cyclooxygenase 2 single-nucleotide polymorphisms and hepatocellular carcinoma in Taiwan. Chin J Physiol 55: 1-7, 2012.
22 Cheng I, Liu X, Plummer SJ, Krumroy LM, Casey G and Witte JS: COX2 genetic variation, NSAIDs, and advanced prostate cancer risk. Br J Cancer 97: 557-561, 2007.
23 Panguluri RC, Long LO, Chen W, Wang S, Coulibaly A, Ukoli F, Jackson A, Weinrich S, Ahaghotu C, Isaacs W and Kittles RA: COX-2 gene promoter haplotypes and prostate cancer risk. Carcinogenesis 25: 961-966, 2004.
24 Shahedi K, Lindstrom S, Zheng SL, Wiklund F, Adolfsson J, Sun J, Augustsson-Balter K, Chang BL, Adami HO, Liu W, Gronberg H and Xu J:
Genetic variation in the COX-2 gene and the association with prostate cancer risk. Int J Cancer 119: 668-672, 2006.
25 Fernandez P, de Beer PM, van der Merwe L and Heyns CF: COX-2 promoter polymorphisms and the association with prostate cancer risk in South African men. Carcinogenesis 29: 2347-2350, 2008.
26 Wu HC, Chang CH, Ke HL, Chang WS, Cheng HN, Lin HH, Wu CY, Tsai CW, Tsai RY, Lo WC and Bau DT: Association of cyclooxygenase 2 polymorphic genotypes with prostate cancer in taiwan. Anticancer Res 31: 221-225, 2011.
27 Mandal RK and Mittal RD: Polymorphisms in COX-2 gene influence prostate cancer susceptibility in a northern Indian cohort. Arch Med Res 42: 620-626, 2011.
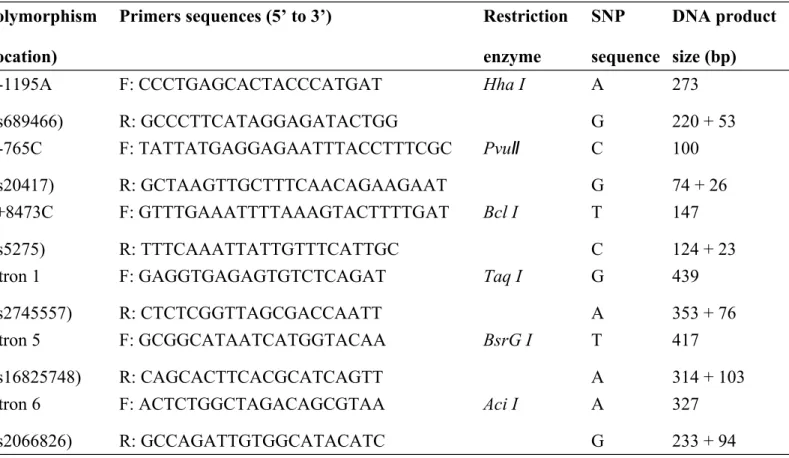
Table I. Primer sequences, PCR and restriction fragment length polymorphism (RFLP) conditions for the Cox-2 genotyping.
Polymorphism (location)
Primers sequences (5’ to 3’) Restriction enzyme SNP sequence DNA product size (bp) G-1195A (rs689466) F: CCCTGAGCACTACCCATGAT R: GCCCTTCATAGGAGATACTGG Hha I A G 273 220 + 53 G-765C (rs20417) F: TATTATGAGGAGAATTTACCTTTCGC R: GCTAAGTTGCTTTCAACAGAAGAAT PvuⅡ C G 100 74 + 26 T+8473C (rs5275) F: GTTTGAAATTTTAAAGTACTTTTGAT R: TTTCAAATTATTGTTTCATTGC Bcl I T C 147 124 + 23 intron 1 (rs2745557) F: GAGGTGAGAGTGTCTCAGAT R: CTCTCGGTTAGCGACCAATT Taq I G A 439 353 + 76 intron 5 (rs16825748) F: GCGGCATAATCATGGTACAA R: CAGCACTTCACGCATCAGTT BsrG I T A 417 314 + 103 intron 6 (rs2066826) F: ACTCTGGCTAGACAGCGTAA R: GCCAGATTGTGGCATACATC Aci I A G 327 233 + 94 *F and R indicate forward and reverse primers, respectively.
Table II. Characteristics of bladder cancer patients and non-cancer healthy controls.
Characteristics Controls (n=375) Patients (n=375) p-Valuea
n % Mean (SD) n % Mean (SD) Age (years) 62.3 (9.7) 61.4 (10.3) 0.73
Age group (years) 0.71
≦55 152 40.5% 158 42.1% >55 223 59.5% 217 57.9% Gender 0.55 Male 287 76.5% 279 74.4% Female 88 23.5% 96 25.6% Habits Cigarette smokers 186 49.6% 201 53.6% 0.31 Alcohol drinkers 176 46.9% 189 50.4% 0.38
Table III. Distribution of Cox-2 genotypes among bladder cancer patient and control subjects.
Genotype Controls % Patients % p-Valuea OR (95%CI)b
A-1195G (rs689466) 0.7236 AA 107 28.5% 105 28.0% 1.00 (reference)c AG 171 45.6% 181 48.3% 1.08 (0.77-1.52) GG 97 25.9% 89 23.7% 0.94 (0.63-1.39) G-765C (rs20417) 0.0102* GG 315 84.0% 286 76.3% 1.00 (reference) GC 60 16.0% 89 23.7% 1.63 (1.13-2.35)* CC 0 0% 0 0% ND T+8473C (rs5275) 0.4831 TT 258 68.8% 248 66.1% 1.00 (reference) TC 117 31.2% 127 33.9% 1.13 (0.83-1.53) CC 0 0% 0 0% ND intron 1 (rs2745557) 0.6727 GG 284 75.7% 274 73.1% 1.00 (reference) AG 84 22.4% 92 24.5% 1.14 (0.81-1.59) AA 7 1.9% 9 2.4% 1.33 (0.49-3.63) intron 5 (rs16825748) 1.0000 TT 371 98.9% 372 99.2% 1.00 (reference) AT 4 1.1% 3 0.8% 0.75 (0.17-3.37) AA 0 0% 0 0% ND intron 6 (rs2066826) 0.4871 GG 329 87.7% 339 90.4% 1.00 (reference) AG 40 10.7% 32 8.5% 0.78 (0.48-1.27) AA 6 1.6% 4 1.1% 0.65 (0.18-2.31)
ND, not determined for the observed counts in case or control are zero; Significant ap-values and bORs, 95% CIs are bold and followed with a star; cset as control for comparison
Table IV. Cox-2 Allelic frequencies among bladder cancer patient and control subjects.
Allele Controls % Patients % p-Value OR (95%CI)
A-1195G (rs689466) 0.7565 Allele A 385 51.3% 391 52.1% 1.00 (reference) Allele G 365 48.7% 359 47.9% 0.97 (0.79-1.19) G-765C (rs20417) 0.0123* Allele G 690 92.0% 661 88.1% 1.00 (reference) Allele C 60 8.0% 89 11.9% 1.55 (1.09-2.18)* T+8473C (rs5275) 0.4842 Allele T 633 84.4% 623 83.1% 1.00 (reference) Allele C 117 15.6% 127 16.9% 1.10 (0.84-1.45) intron 1 (rs2745557) 0.3700 Allele G 652 86.9% 640 85.3% 1.00 (reference) Allele A 98 13.1% 110 14.7% 1.14 (0.85-1.53) intron 5 (rs16825748) 0.7048 Allele T 746 99.5% 747 99.6% 1.00 (reference) Allele A 4 0.5% 3 0.4% 0.75 (0.17-3.36) intron 6 (rs2066826) 0.1966 Allele G 698 93.1% 710 94.7% 1.00 (reference) Allele A 52 6.9% 40 5.3% 0.76 (0.49-1.16)
Table V. Summary of current and previous studies on the association of Cox-2 G-765C (rs20417) polymorphism and bladder/prostate cancer risk.
First author, year Country Race Cases Controls Association with cancer
Chang WS, 2013 Taiwan Chinese 375 375 Bladder cancer, associated
Panguluri RC, 2004 USA European/African 90/124 90/164 Prostate cancer, associated
Cheng I, 2007 USA European/African 416/89 417/88 Prostate cancer, not associated
Fernandez P, 2008 South Africa African 151 134 Prostate cancer, associated
Wu HC, 2011 Taiwan Chinese 218 436 Prostate cancer, associated