ISSN: 1524-4628
Copyright © 2009 American Heart Association. All rights reserved. Print ISSN: 0039-2499. Online Stroke is published by the American Heart Association. 7272 Greenville Avenue, Dallas, TX 72514
DOI: 10.1161/STROKEAHA.109.562017
published online Oct 8, 2009;
Stroke
Jiunn-Horng Kang, Jau-Der Ho, Yi-Hua Chen and Herng-Ching Lin
Follow-Up Study
Increased Risk of Stroke After a Herpes Zoster Attack. A Population-Based
http://stroke.ahajournals.org
located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprints
Reprints: Information about reprints can be found online at
[email protected] 410-528-8550. E-mail:
Fax: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters
http://stroke.ahajournals.org/subscriptions/
Subscriptions: Information about subscribing to Stroke is online at
at TAIPEI MEDICAL UNIVERSITY LIB. on May 25, 2011 stroke.ahajournals.org
A Population-Based Follow-Up Study
Jiunn-Horng Kang, MSc, MD; Jau-Der Ho, PhD, MD; Yi-Hua Chen, PhD; Herng-Ching Lin, PhD
Background and Purpose—Varicella zoster virus-induced vasculopathy and postherpes zoster attack stroke syndromeshave been reported previously; nevertheless, data regarding the exact prevalence and risk of stroke occurring postherpes zoster attack are still lacking. This study aims to investigate the frequency and risk of stroke after a herpes zoster attack using a nationwide, population-based study of a retrospective cohort design.
Method—A total of 7760 patients who had received treatment for herpes zoster between 1997 and 2001 were included and matched with 23 280 randomly selected subjects. A 1-year stroke-free survival rate was then estimated using the Kaplan-Meier method. After adjusting for potential confounders, Cox proportional hazard regressions were carried out to compute the adjusted 1-year survival rate.
Results—Of the sampled patients, 439 patients (1.41%) developed strokes within the 1-year follow-up period, that is, 133 individuals (1.71% of the patients with herpes zoster) from the study cohort and 306 individuals (1.31% of patients in the comparison cohort) from the comparison cohort. The log rank test indicated that patients with herpes zoster had significantly lower 1-year stroke-free survival rates than the control (P⬍0.001). The adjusted hazard ratios of stroke after herpes zoster and herpes zoster ophthalmicus during the 1-year follow-up period were 1.31 and 4.28, respectively. Conclusion—The risk for stroke increased after a zoster attack. Although varicella zoster virus vasculopathy is a well-documented complication that may induce a stroke postherpes zoster attack, it does not fully account for the unexpectedly high risk of stroke in these patients. (Stroke. 2009;40:3443-3448.)
Key Words: herpes zoster 䡲 herpes zoster attack 䡲 stroke
T
he primary varicella zoster virus (VZV) infection usually affects children, leading to varicella (chicken pox). Although some infected children may develop serious com-plications, varicella is generally benign and transient.1 TheVZV then becomes inactive in the sensory and autonomic ganglia. Although the pathomechanisms are not fully under-stood, spontaneous reactivation of VZV manifests as skin lesions with painful vesicles spreading over one to 1 der-matomes known as a herpes zoster (shingle). Herpes zoster is an observed condition in elderly, immunocompromised, and debilitated patients.2It usually resolves itself spontaneously,
although the development of long-duration postherpetic neu-ralgia is not uncommon.3
Numerous reports of VZV-induced vasculopathy and stroke syndrome after herpes zoster attacks have been re-ported since the early 1970s.4,5 VZV is also the only
recog-nized human virus able to replicate in cerebral arteries.6It is
hypothesized to spread along the nerve fibers to the blood vessels where it induces further inflammatory and thrombotic responses.2,7,8 Two major spectrums of VZV vasculopathy
have been identified: large- and small-vessel VZV
vasculopa-thy.9In large-vessel VZV vasculopathy, the involved vessels
are damaged by virus-induced inflammation,2 presented as
granulomatous angiitis in pathology, and can result in stroke.5,10Small-vessel VZV vasculopathy has many
nonspe-cific manifestations such as fever, headache, seizures, weak-ness, consciousness disturbances, and cognitive impairments, known as small-vessel encephalitis.10
To our knowledge, despite many case reports of conditions associated with VZV vasculopathy, large sample data regard-ing the exact frequency and risk of stroke occurrregard-ing posther-pes zoster attack are still lacking. Our study’s goal was to investigate the risk and frequency of stroke after herpes zoster attacks in the general population using a nationwide population-based study of a retrospective cohort design.
Methods
DatabaseThis study used a data set released by the Taiwan National Health Research Institute in 2006. Taiwan began its National Health Insurance program in 1995 to finance health care for all the island’s residents. There are currently⬎25 million enrollees covered by the
Received July 4, 2009; accepted August 4, 2009.
From the Department of Physical Medicine and Rehabilitation (J.-H.K.), the Neuroscience Research Center (J.-H.K.), and the Department of Ophthalmology (J.-D.H.), Taipei Medical University Hospital, Taipei, Taiwan; and the School of Public Health (Y.-H.C.), the School of Health Care Administration (H.-C.L.), and the Dr. Chi-Chin Huang Stroke Research Center (H.-C.L.), Taipei Medical University, Taipei, Taiwan.
Correspondence to Herng-Ching Lin, PhD, School of Health Care Administration, College of Medicine, Taipei Medical University, 250 Wu-Hsing Street, Taipei 110, Taiwan. E-mail [email protected]
© 2009 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.109.562017
program, representing approximately 98% of the island’s population. This data set, which the Taiwan National Health Research Institute created by systematically selecting a representative database from the entire set of enrollees, consists of 1 000 000 randomly selected subjects. There were no statistically significant differences in age, sex, or healthcare costs between the sample group and all enrollees, as reported by the Taiwan National Health Research Institute. This data set includes all claims data for these 1 000 000 subjects, offering a unique opportunity to explore the risk of stroke among patients with herpes zoster.
Because the data set used in this study consists of deidentified secondary data released to the public for research purposes, this study was exempt from full review by the Institutional Review Board.
Study Sample
This study includes a study cohort and a comparison cohort. The study cohort comprised all patients who had visited ambulatory care centers for treatment of herpes zoster (International Classification of
Diseases, 9th Revision, Clinical Modification Code 053) over a
5-year period, from January 1, 1997, to December 31, 2001 (n⫽9841). We excluded patients ⬍18 years of age (n⫽1437) to limit the study sample to adults. We also excluded patients who had been diagnosed with a stroke (International Classification of Diseases, 9th
Revision, Clinical Modification Codes 430 to 438) before their index
ambulatory care visit (first-time ambulatory care visits for treatment of herpes zoster). Ultimately, our study cohort included 7760 patients with herpes zoster.
Meanwhile, the comparison cohort was selected from the remain-ing patients in the data set. We excluded patients who had been diagnosed with herpes zoster or stroke before 2001. We then randomly extracted 23 280 subjects (3 for every patient in the study cohort) matching the study cohort in terms of age (as a continuous variable) and sex. We also selected their first ambulatory care visit during 2001 as their index ambulatory care visit. Thereafter, each patient was tracked for 1 year from their index ambulatory to distinguish patients who had developed any type of stroke.
Statistical Analysis
The SAS statistical package (SAS System for Windows, Version 8.2) was used to perform analyses in this study. Pearson2tests were
performed to examine the differences between the 2 cohorts in terms of sociodemographic characteristics, select comorbid medical disor-ders, and stroke development risk. The 1-year stroke-free survival rate was estimated by the Kaplan-Meier method using the log rank test to examine the differences in the risk of developing stroke between the 2 cohorts.
In addition, after adjusting for potential confounders, Cox propor-tional hazard regressions were carried out to compute the 1-year survival rate. Potential confounders included patient’s age, sex, monthly income, level of urbanization (including 5 levels, with Level 1 referring to “most urbanized” and Level 5 referring to “least urbanized” communities), geographical location of the community in which the patient resided (northern, central, eastern, and southern Taiwan), and whether a patient had hypertension, diabetes, renal disease, coronary heart disease, hyperlipidemia, atrial fibrillation, heart failure, heart valve/myocardium disease, and/or carotid/periph-eral vascular disease. Previous studies have reported that the occur-rence of stroke is associated with both geographical region and level of urbanization11,12; these have therefore been adjusted in the
regression modeling. The reason we selected NT $15 840 as the first income-level cutoff point was that this is the government-stipulated minimum wage for full-time employees in Taiwan. Finally, we present hazard ratios (HRs) along with 95% CIs using a significance level of 0.05.
Results
The mean age for the sampled patients was 46.7 years with a SD of 15.6 years. Table 1 presents the distribution of demographic characteristics and selects comorbid medical
disorders for both the study and comparison cohorts. After matching for sex and age, the results demonstrate that patients with herpes zoster were more likely to have comorbidities such as hypertension (P⬍0.001), diabetes (P⫽0.001),
coro-Table 1. Demographic Characteristics and Comorbid Medical Disorders for Patients in Taiwan With Herpes Zoster and Patients in the Comparison Cohort, 1999 to 2001 (nⴝ31 040)
Variable Patients With Herpes Zoster Comparison Patients P Value Total No. Column Percent Total No. Column Percent Hypertension ⬍0.001 Yes 416 5.36 993 4.27 No 7344 94.64 22 287 95.73 Diabetes 0.001 Yes 221 2.85 508 2.18 No 7539 97.15 22 772 97.82
Coronary heart disease ⬍0.001 Yes 151 1.95 303 1.30 No 7609 98.05 22 977 98.70 Hyperlipidemia 0.131 Yes 86 1.11 213 0.91 No 7674 98.89 23 067 99.09 Renal disease 0.014 Yes 28 0.36 47 0.20 No 7732 99.64 23 233 99.80 Atrial fibrillation 0.700 Yes 10 0.13 26 0.11 No 7750 99.87 23 254 99.87 Heart failure 0.006 Yes 42 0.54 75 0.32 No 7718 99.46 23 205 99.68 Heart valve/myocardium disease 0.518 Yes 27 0.35 70 0.30 No 7733 99.65 23 210 99.70 Carotid/peripheral vascular disease 0.028 Yes 16 0.21 24 0.10 No 7744 99.79 23 256 99.90 Monthly income 0.044 0 4098 52.81 12 324 52.94 NT $1-15 840 759 9.78 2308 9.91 NT $15 841-25 000 1939 24.99 6017 25.85 ⱖNT $25 001 964 12.42 2631 11.30 Urbanization level 0.794 1 1402 18.07 4240 18.21 2 1323 17.05 4025 17.29 3 711 9.16 2218 9.53 4 671 8.65 1983 8.52 5 3653 47.07 10 814 46.45 Geographic region 0.001 Northern 5351 68.96 15 886 68.24 Central 1130 14.56 3241 13.92 Southern 1150 14.82 3837 16.48 Eastern 129 1.66 316 1.36 3444 Stroke November 2009
at TAIPEI MEDICAL UNIVERSITY LIB. on May 25, 2011 stroke.ahajournals.org
nary heart disease (P⬍0.001), renal disease (P⫽0.014), heart failure (P⫽0.006), and carotid/peripheral vascular disease (P⫽0.028) at the time of their outpatient care visits as compared with the patients in the comparison cohort.
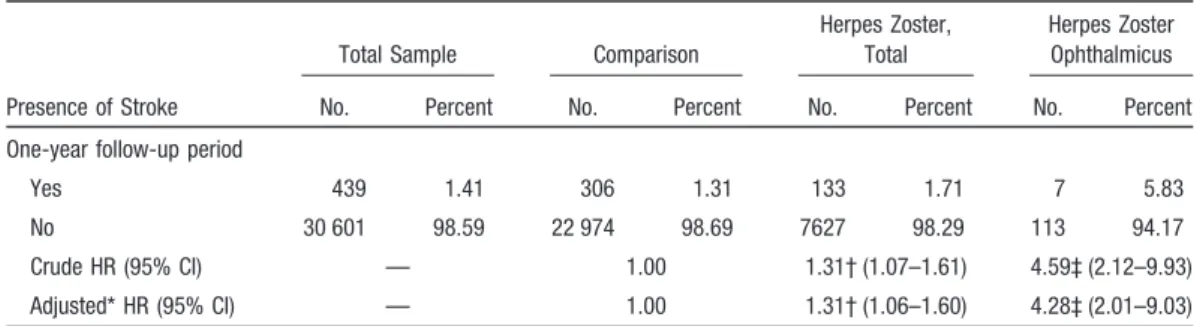
Of the total sample of 31 040 patients, 439 individuals (1.41%) developed strokes during the 1-year follow-up period, 133 (1.71%) of which were patients with herpes zoster and 306 (1.31%) that were patients in the comparison cohort (Table 2). The log rank test indicated that patients with herpes zoster had significantly lower 1-year stroke-free survival rates than patients in the comparison cohort (P⬍0.001). The results of Kaplan-Meier survival analysis are presented in the Figure.
Details of the crude and adjusted HRs for stroke, based on Cox proportional hazard regression analysis, are also present-ed in Table 2 by cohort. After adjusting for patient’s age, sex, monthly income, hypertension, diabetes, renal disease, coro-nary heart disease, hyperlipidemia, atrial fibrillation, heart failure, heart valve/myocardium disease, carotid/peripheral
vascular disease, level of urbanization, and the geographical location of the community in which the patient resided, the HR for developing stroke during the 1-year follow-up period was 1.31 (95% CI, 1.00 to 1.60; P⬍0.05) for patients with herpes zoster compared with patients in the comparison cohort. We further analyzed the risk of stroke for patients with herpes zoster ophthalmicus. We found that the adjusted HR of stroke during the 1-year follow-up period was 4.28 (95% CI, 2.01 to 9.03; P⬍0.001) for patients with herpes zoster and ophthalmic complications as compared with pa-tients without herpes zoster.
We also analyzed the risk of stroke by stroke type, finding that the adjusted HR of developing ischemic stroke and intracerebral or subarachnoid hemorrhaging during the 1-year follow-up period was 1.31 (95% CI, 1.07 to 1.65; P⫽0.009) and 2.79 (95% CI, 1.69 to 4.61; P⬍0.001), respectively, for patients with herpes zoster compared with patients of the comparison cohort.
Table 2. Crude and Adjusted HRs for Stroke Among Sample Patients During the 1-Year Follow-Up Period Starting From the Index Ambulatory Care Visit (nⴝ31 040)
Presence of Stroke
Total Sample Comparison
Herpes Zoster, Total
Herpes Zoster Ophthalmicus No. Percent No. Percent No. Percent No. Percent One-year follow-up period
Yes 439 1.41 306 1.31 133 1.71 7 5.83 No 30 601 98.59 22 974 98.69 7627 98.29 113 94.17 Crude HR (95% CI) — 1.00 1.31† (1.07–1.61) 4.59‡ (2.12–9.93) Adjusted* HR (95% CI) — 1.00 1.31† (1.06–1.60) 4.28‡ (2.01–9.03) *Adjustments are made for patient’s age, sex, hypertension, diabetes, coronary heart disease, hyperlipidemia, renal disease, atrial fibrillation, heart failure, heart valve/myocardium disease, carotid/peripheral vascular disease, monthly income, urbanization level, and geographical region.
†P⬍0.05. ‡P⬍0.001.
Figure. Stroke-free survival rates for
patients with herpes zoster in Taiwan and patients in the comparison cohort, 1999 to 2001.
Table 3 reveals results from further analyses stratified by patient age and sex. Among male and female patients, the adjusted HR of stroke during the 1-year follow-up period was, respectively, 1.32 (95% CI, 1.01 to 1.75; P⬍0.05) and 1.30 (95% CI, 1.01 to 1.75; P⬍0.05) times greater for those with herpes zoster than for those without. In addition, the adjusted HR for stroke occurring during the 1-year follow-up period was 1.31 (95% CI, 1.06 to 1.63; P⬍0.05) times higher for patients with herpes zoster ⱖ45 years old than for the same age group of the comparison cohort. However, there were no significant differences in stroke risk between patients with herpes zoster⬍45 years old and patients in the same age group of the comparison cohort.
Discussion
Varicella is considered an important risk factor for stroke in children.13Askalan et al showed that compared with the
general population, there is a 3-fold increase in acute ischemic stroke among children with preceding varicella infection.13However, data regarding stroke frequency after
zoster attacks in adults are lacking. VZV vasculopathy resulting in stroke is considered a rare complication of postherpes zoster attacks in adults; nevertheless, our data suggest that stroke patterns after instances of herpes zoster may not only be sporadic cases. According to the 1-year follow-up data, the frequencies of stroke after herpes zoster and herpes zoster ophthalmicus attacks were 1.71% and 5.83%, respectively. After adjusting for other cerebro-vascular risks, we found that the risk of having a stroke increased by 31% postherpes zoster attacks, and approxi-mately 4-fold in the patients with herpes zoster ophthal-micus, compared with the comparison cohort. Because previous studies demonstrate that herpes zoster (shingles) frequency could be as high as 1.3 to 1.6 per 1000 people per year, and the OR for lifetime occurrences is approxi-mately one to 4,14,15the possibility of developing a stroke
after a herpes zoster attack should not be overlooked.
Furthermore, we found that the elevated HR for stroke development after herpes zoster was significant among patients who wereⱖ45 years old. We hypothesize that the frequency and severity of vasculopathy after herpes zoster may increase in elderly individuals prone to pre-existing arthrosclerosis and attenuated immunological statuses. In-terestingly, although the risks for hemorrhagic and ische-mic stroke both increased in patients with herpes zoster, the HR for the former was higher. Previous articles have illustrated that VZV vasculopathy can result in a variable spectrum of clinical manifestations, including arterial thrombosis,4 arterial dolichoectasia,16 dissection,17
aneu-rysm,18 and hemorrhaging.19,20 The frequency of stroke
subtypes varies by ethnicity.21 For instance, scientific
literature indicates a higher prevalence of hemorrhagic stroke in Asian/Chinese populations.21,22 It is still
un-known whether stroke subtypes postherpes zoster attack are influenced by such ethnic distinctions. We suggest further exploration into this matter.
Although VZV vasculopathy is a well-documented cause of stroke after herpes zoster attacks, it does not fully explain the unexpectedly high risk of stroke observed among these patients. In addition to direct causation by VZV vasculopathy, we hypothesize several possible patho-logical stroke mechanisms. First, although current data are limited, it is possible that for patients with mild VZV vasculopathy, the damaged vessel initiates secondary ath-erosclerosis in the long run. The gradual progression of atherosclerosis may cause delayed stroke in these patients. Second, patients often experience postherpetic neuralgia after a herpes zoster attack.23 Chronic pain may be
asso-ciated with elevated sympathetic statuses and adverse emotional reactions,23,24 theoretically increasing
cerebro-vascular risks. Third, it is generally accepted that persons who experience stressful events and medical conditions may be associated with the herpes zoster reactivation and attack. Despite adjusting for several well-known
cardio-Table 3. Crude and Adjusted HRs for Stroke Among Sample Patients During the 1-Year Follow-Up Period Stratified by Patient Age and Sex (nⴝ31 040)
Presence of Stroke
Patient Sex* Patient Age,† Years
Male Female ⬍45 ⱖ45 Comparison No. (%) Herpes Zoster No. (%) Comparison No. (%) Herpes Zoster No. (%) Comparison No. (%) Herpes Zoster No. (%) Comparison No. (%) Herpes Zoster No. (%) One-year follow-up period Yes 161 (1.4) 72 (1.9) 149 (1.2) 65 (1.6) 28 (0.3) 10 (0.3) 282 (2.2) 127 (2.9) No 11 047 (98.6) 3664 (98.1) 11 923 (98.9) 3959 (98.4) 10 190 (99.7) 3396 (99.7) 12 780 (97.8) 4227 (97.1) Crude HR (95% CI) 1.00 1.35‡ (1.02–1.79) 1.00 1.32‡ (1.01–1.76) 1.00 1.07 (0.52–2.21) 1.00 1.36§ (1.10–1.68) Adjusted HR (95% CI) 1.00 1.32‡ (1.01–1.75) 1.00 1.30‡ (1.01–1.75) 1.00 1.02 (0.49–2.12) 1.00 1.31‡ (1.06–1.63) *The HR was calculated by adjusting for patient’s age, hypertension, diabetes, coronary heart disease, hyperlipidemia, renal disease, atrial fibrillation, heart failure, heart valve/myocardium disease, carotid/peripheral vascular disease, monthly income, urbanization level, and geographical region.
†The HR was calculated by adjusting for patient’s sex, hypertension, diabetes, coronary heart disease, hyperlipidemia, renal disease, atrial fibrillation, heart failure, heart valve/myocardium disease, carotid/peripheral vascular disease, monthly income, urbanization level, and geographical region.
‡P⬍0.05. §P⬍0.001.
3446 Stroke November 2009
at TAIPEI MEDICAL UNIVERSITY LIB. on May 25, 2011 stroke.ahajournals.org
vascular risk factors, the immunologic status and general health condition of the subjects could not be inferred from the administrative data. Therefore, the possibility that stroke development is associated with underlying debili-tating or stressful conditions cannot be excluded. Further study is recommended to verify our hypotheses.
A majority of previous reports show that contralateral hemiplegia is the most common manifestation of VZV vasculopathy resulting in stroke, particularly after herpes zoster ophthalmicus.4,25Our findings are consistent with this
observation.
It is worthy to mention that some authors reported a relationship between VZV vasculopathy and stroke develop-ing when shdevelop-ingles involved distant dermatomes such as cervical, thoracic, and even sacral regions.7,26,27Similarly, we
found that the overall risk for having a stroke increased in patients with herpes zoster. The pathomechanisms explaining this phenomenon are still unknown; however, there is some speculation that it involves the dissemination or co-occurrence of viral reactivation in cerebral ganglia spreading to the supplying vessels.7Systemic factors may also
contrib-ute to stroke. Recently, coagulation abnormalities have been reported in association with herpes zoster attacks.28 The
clinical implications of these findings could be important for stroke prevention and patient management.
Finally, we found a higher frequency of several cardiovas-cular risk factors among the patients with herpes zoster compared with the case-matching group. To our knowledge, the data regarding cardiovascular risk frequency among patients with herpes zoster are still lacking. The “herpesvirus burden” could accelerate arthrosclerosis development, which could be associated with some cardiovascular factors.29,30In
addition, the patient who has cardiovascular factors might also have poorer health, putting them at risk of herpes zoster. We postulate that this cause-and-effect relationship between shingles and cardiovascular risk factors is bidirectional. Nevertheless, stroke development risk remained higher in patients with herpes zoster after adjusting for these cardio-vascular risk factors.
Our study has some limitations. Skin lesions are a common diagnosis indicator for herpes zoster and, when absent, may make accurate clinical diagnoses more difficult.31 Hence,
patients may have been absent or and miscoded in our database. Furthermore, the clinical features and manifesta-tions of herpes zoster vasculopathy may be different among comorbid patients. For example, the VZV small-vessel vas-culopathy in a patient with HIV could manifest as encepha-litis rather than a stroke,10 which was not included in our
study. Finally, potential confounding variables, including obesity, physical activity, smoking and alcohol use, dietary habits, and family history, are associated with stroke but not indicated in our database. The association between herpes zoster and theses factors remains unknown. Further study is suggested to clarify these issues.
Conclusion
To our knowledge, this is the first attempt at investigating epidemiological data on strokes after zoster attacks in a large nationwide population-based study. We confirmed that in the
general population, the risk for stroke increased after a zoster attack and additionally found that strokes after such attacks were more frequent than expected. Further studies should be conducted to explore the underlying pathomechanisms and intervention strategies for patients experiencing herpes zoster attacks.
Acknowledgments
This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insur-ance, Department of Health and managed by National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Disclosure
None.
References
1. Ziebold C, von Kries R, Lang R, Weigl J, Schmitt HJ. Severe compli-cations of varicella in previously healthy children in Germany: a 1-year survey. Pediatrics. 2001;108:E79.
2. Gilden DH, Cohrs RJ, Mahalingam R. Clinical and molecular patho-genesis of varicella virus infection. Viral Immunol. 2003;16:243–258. 3. Volpi A. Severe complications of herpes zoster. Herpes. 2007;14(suppl 2):
35–39.
4. Gilbert GJ. Herpes zoster ophthalmicus and delayed contralateral hemi-paresis. Relationship of the syndrome to central nervous system granu-lomatous angiitis. JAMA. 1974;229:302–304.
5. Rosenblum WI, Hadfield MG. Granulomatous angiitis of the nervous system in cases of herpes zoster and lymphosarcoma. Neurology. 1972; 22:348 –354.
6. Kleinschmidt-DeMasters BK, Gilden DH. Varicella-zoster virus infections of the nervous system: clinical and pathologic correlates. Arch Pathol Lab Med. 2001;125:770 –780.
7. Gilden DH, Lipton HL, Wolf JS, Akenbrandt W, Smith JE, Mahalingam R, Forghani B. Two patients with unusual forms of varicella-zoster virus vasculopathy. N Engl J Med. 2002;347:1500 –1503.
8. Mayberg M, Langer RS, Zervas NT, Moskowitz MA. Perivascular men-ingeal projections from cat trigeminal ganglia: possible pathway for vascular headaches in man. Science. 1981;213:228 –230.
9. Kleinschmidt-DeMasters BK, Amlie-Lefond C, Gilden DH. The patterns of varicella zoster virus encephalitis. Hum Pathol. 1996;27:927–938. 10. Gilden DH. Varicella zoster virus vasculopathy and disseminated
enceph-alomyelitis. J Neurol Sci. 2002;195:99 –101.
11. Engstrom G, Jerntorp I, Pessah-Rasmussen H, Hedblad B, Berglund G, Janzon L. Geographic distribution of stroke incidence within an urban population: relations to socioeconomic circumstances and prevalence of cardiovascular risk factors. Stroke. 2001;32:1098 –1103.
12. Lin HC, Lin YJ, Liu TC, Chen CS, Chiu WT. Urbanization and stroke prevalence in Taiwan: analysis of a nationwide survey. J Urban Health. 2007;84:604 – 614.
13. Askalan R, Laughlin S, Mayank S, Chan A, MacGregor D, Andrew M, Curtis R, Meaney B, deVeber G. Chickenpox and stroke in childhood: a study of frequency and causation. Stroke. 2001;32:1257–1262. 14. Bowsher D. The lifetime occurrence of herpes zoster and prevalence of
post-herpetic neuralgia: a retrospective survey in an elderly population. Eur J Pain. 1999;3:335–342.
15. Glynn C, Crockford G, Gavaghan D, Cardno P, Price D, Miller J. Epidemiology of shingles. J R Soc Med. 1990;83:617– 619.
16. Dalton CM, Jager HR, Losseff NA, Greenwood RJ. Neurological picture. Varicella zoster virus and intracranial dolichoectasia in a late adult cancer survivor. J Neurol Neurosurg Psychiatry. 2008;79:573.
17. Constantinescu CS. Association of varicella-zoster virus with cervical artery dissection in 2 cases. Arch Neurol. 2000;57:427.
18. Gursoy G, Aktin E, Bahar S, Tolun R, Ozden B. Post-herpetic aneurysm in the intrapetrosal portion of the internal carotid artery. Neuroradiology. 1980;19:279 –282.
19. de Broucker T, Verollet D, Schoindre Y, Henry C, Martinez-Almoyna L, Tourret J, Joly V, Yeni P. Cerebral vasculitis with aneurysms caused by varicella-zoster virus infection during aids: a new clinicoangiographical syndrome [in French]. Rev Neurol (Paris). 2008;164:61–71.
20. Gilden D. The ever-widening spectrum of varicella zoster virus vascu-lopathy. Eur J Neurol. 2008;15:e88 – e89.
21. Shen AY, Yao JF, Brar SS, Jorgensen MB, Chen W. Racial/ethnic differences in the risk of intracranial hemorrhage among patients with atrial fibrillation. J Am Coll Cardiol. 2007;50:309 –315.
22. Potluri R, Natalwala A. Increasing prevalence of haemorrhagic stroke among South Asian patients in the United Kingdom from 1997 to 2005. J Clin Neurosci. 2009;16:605– 606.
23. Feller L, Jadwat Y, Bouckaert M. Herpes zoster post-herpetic neuralgia. SADJ. 2005;60:432, 436 – 432, 437.
24. Daniel HC, Narewska J, Serpell M, Hoggart B, Johnson R, Rice AS. Comparison of psychological and physical function in neuropathic pain and nociceptive pain: implications for cognitive behavioral pain man-agement programs. Eur J Pain. 2008;12:731–741.
25. Hilt DC, Buchholz D, Krumholz A, Weiss H, Wolinsky JS. Herpes zoster ophthalmicus and delayed contralateral hemiparesis caused by cerebral angiitis: diagnosis and management approaches. Ann Neurol. 1983;14: 543–553.
26. Horten B, Price RW, Jimenez D. Multifocal varicella-zoster virus leu-koencephalitis temporally remote from herpes zoster. Ann Neurol. 1981; 9:251–266.
27. Patrick JT, Russell E, Meyer J, Biller J, Saver JL. Cervical (C2) herpes zoster infection followed by pontine infarction. J Neuroimaging. 1995;5: 192–193.
28. Massano J, Ferreira D, Toledo T, Mansilha A, Azevedo E, Carvalho M. Stroke and multiple peripheral thrombotic events in an adult with varicella. Eur J Neurol. 2008;15:e90 – e91.
29. Gomez E, Laures A, Baltar JM, Melon S, Diez B, de Ona M. Cytomeg-alovirus replication and ‘herpesvirus burden’ as risk factor of cardiovas-cular events in the first year after renal transplantation. Transplant Proc. 2005;37:3760 –3763.
30. Zhu J, Nieto FJ, Horne BD, Anderson JL, Muhlestein JB, Epstein SE. Prospective study of pathogen burden and risk of myocardial infarction or death. Circulation. 2001;103:45–51.
31. Nagel MA, Cohrs RJ, Mahalingam R, Wellish MC, Forghani B, Schiller A, Safdieh JE, Kamenkovich E, Ostrow LW, Levy M, Greenberg B, Russman AN, Katzan I, Gardner CJ, Hausler M, Nau R, Saraya T, Wada H, Goto H, de MM, Ueno M, Brown WD, Terborg C, Gilden DH. The varicella zoster virus vasculopathies: clinical, CSF, imaging, and virologic features. Neurology. 2008;70:853– 860.
3448 Stroke November 2009
at TAIPEI MEDICAL UNIVERSITY LIB. on May 25, 2011 stroke.ahajournals.org