Sleep Quality and Morningness-Eveningness on Shift Nurses
Min-Huey Chung1, 2; Fu-Mei Chang, RN, PhD3; Cheryl C. H. Yang, PhD4;Terry B. J.
Kuo, MD, PhD4; Nanly Hsu, RN, PhD3
1
Institute of Medical Sciences, Tzu Chi University, Hualien; 2School of Nursing, National Defense Medical Center, Taipei, Taiwan. 3 School of nursing, Tzu Chi University, Hualien; 4 Institute of Brain Science, National Yang-Ming University, Taipei, Taiwan.
Running Title: morningness-eveningness on sleep quality –Chung et al. Keywrods: shift, nurse, morningness-eveingness, sleep
Address correspondence to: Nanly Hsu, School of Nursing, Tzu Chi University, No. 701, Chung
Yang Road, Section 3, Hualien 97004, Taiwan; Tel: 886 3 8565301 (ext.7034); Fax: 886 3 8580639;
ABSTRACT
Aim and objective. The aim of the study was to analyze, while controlling for identified covariates, the effects of morningness-eveningness on global sleep quality
and components of sleep quality for shift nurses.
Background. Shift nurses had greater difficulty falling asleep or staying asleep, thus resulting in higher rates of retiring from hospital. Existing research has addressed the
effects of manpower demand and personal preferences on shift assignment; however,
the concept of endogenous rhythms is considered rarely.
Methods. This analysis included 137 nurses between the ages of 21 and 47. Nurses completed the Horne and Ostberg questionnaire to assess morningness-eveningness
and the Pittsburgh Sleep Quality Index (PSQI) questionnaire to measure self-reported
sleep quality over the last month. The 18-point Chinese version had a Cronbach’s
reliability coefficient of 0.79 overall and 0.86, respectively. This study analyzed
correlates of sleep quality by comparing the groups with better or worse sleep quality
according to the median of PSQI. Univariate and multivariate analyses were used for
the risk factors of worse sleep quality.
Results. The result showed that the strongest predictor of sleep quality was morningness-eveningness not the shift schedule or shift pattern for nurses under
controlling the variable of age. Greater age and longer years employed in nursing
was properly controlled; evening types working on shifting jobs had higher risk of
poor sleep quality compared to morning types.
Conclusion. Morningness-eveningness was the strongest predictor of sleep quality under controlling the variable of age in shift nurses.
Implications for clinical practice. Our results suggested that determining if nurses were attributed to morning or evening types is an important sleep issue before
deciding the shift assignment.
Introduction
Nurses work under a shift work system (day shift, evening shift and night shift) in
response to patient needs. The shift work system disturbs the natural human circadian
rhythm and causes lack of sleep (Knauth et al. 1980), which directly or indirectly
lowers work efficiency. According to the stressor model by Olsson et al.(1990)
stressors brought by the shift system are occupational stressors, personal factors, and
non-occupational stressors. Occupational stressors included the shift system (speed
and hours) and workload. Personal factors consisted of sex, age, and circadian rhythm
types. Non-occupational stressors involved the level of stress in daily living. These
stressors cause tremendous pressure on shift workers and arouse physical and
psychological reaction; furthermore, they cause sleep disturbances and circadian
rhythms disorders. At last, the health of these workers is under duress and the vicious
cycle may cause nurses to quit their jobs. Therefore, it is necessary to continuously
study nurses’ work shift system.
The effect of shift work on worker health is determined by personal factors; for
instance, the individual biological clock and circardian rhythm. Brain resititution and
sleep are influenced by personal inner factors, such as age, circardian rhythm,
physical condition and flexible sleep habits. In other words, the shift worker tends to
work problems of pilots and indicated that age and circardian rhythm were the main
factors contributing to work shift assignment and fatigue. Age, circardian rhythm type
and sleep disturbance effectively influence work performance. The circardian rhythm
types could be categorized as Morning-types (M-types), Evening-types (E-types)and
in between the Intermediate type. The M-types get up early and sleep early, while the
E-types are active during the night and can not get up early.
Shift assignement is decided mainly by the manpower demands in hospital wards
and personal preferences; but the endogenous rhythm concept is not considered. Most
studies examined the effect of shift work on sleep (Coffey et al. 1988; Niedhammer et
al. 1994; Poissonnet & Veron 2000; Skipper et al. 1990) or focused on examining correlates of simulated shift work (Cajochen et al. 1995; Dijk et al. 1991; Finelli et al.
2000). Few studies focused on the effects of morningness-eveningness on sleep
quality, particularly in practical shiftwork nurses. We studied the sleep pattern of five
different work shifts, including day shift (07:30-15:30), evening shift (15:30-23:30),
night shift (23:30-07:30), day shift to evening shift or night shift (fast clockwise), and
night shift to day shift or evening shift (fast counter-clockwise). The aim of the study
was to analyze, while controlling for identified covariates, the effects of
morningness-eveningness on global sleep quality and components of sleep quality for
Method
The present analysis included 137 nurses between the ages of 21 and 58 enrolled in
the total. Seventy-four subjects were in their twenties, 42 subjects were in their thirties
and 21 subjects were between the ages of 40 and 58. All subjects were screened to be
clear of any personal history of psychiatric, neurological, sleep or medical disorders.
Subjects read and signed an informed consent that provided detailed information
about the nature, propose and risks of this study.
The personnel in each ward were informed about the study orally by the author at
three different personnel meetings. A contact person at each casualty department was
selected to answer any questions about the study. After the informed consent was
obtained from all women, the researcher would check the missing data to ask nurses
fill it again. The PSQI (Buysse et al. 1989) is a questionnaire that measures
self-reported sleep habits over the last month. It is a global measure with seven
components; perceived sleep quality, sleep latency, sleep duration, sleep efficiency,
sleep disturbance, use of sleep medication, and daytime dysfunction. The score for
each component ranges from 0 to 3, and the sum is a global score that ranges form 0
to 21. As those who took sleep medication were excluded, only six components were
used, with global scores form 0 to 18. Higher scores indicated poorer sleep quality.
of music on individual elements of sleep could be determined.
A score of 5 (indication poor sleep) yield a diagnostic sensitivity of 89.5% and a
specificity of 86.55, with an internal consistency of α =0.83, and test-retest reliability,
r=0.85(Buysse et al. 1989). The Chinese language of PSQI had α =0.72 and a split
half reliability of 0.84(Wang 1997). In this study, the 18-point Chinese version had a
Cronbach’s reliability coefficient of 0.79 overall and a split half reliability of 0.74 for
the six component scores. Using instrument translated into Chinese, several variables
were measured on their duty to determine whether they would confound the effects of
morningess-eveningness on sleep.
Participants were asked whether or not they had a bedtime routine, napped after
lunch, used herbal tea to sleep. Heart rate and blood pressure were measured by the
investigator in the first visit. Subjects completed the Horne and Ostberg (1976)
questionnaire in order to assess the morningness-eveningness. This questionnaire
establishes five behavioral categories (English version scoring): definitively morning
types (score=28-32), moderately morning types (score=23-27), neither types
(score=16-22), moderately evening types (score=11-15) and definitively evening
types (score=6-10). For the purpose of this study we reduced the categories from
five to three: morning type (score=23-32), neither type (score=16-22) and evening
For maximizing the statistical power, worse sleep quality was defined by being higher
than the median of PSQI (8). For basic comparisons, socio-demographic characteristics,
feature of nursing work nature (years of duty, shift schedule, and shifting pattern), blood
pressure, tea/coffee drinking habit and morningness-eveningness type were statistically
examined by using t-tests for continuous variables and Chi-square tests for categorical
variables. The major area of interest for worse sleep quality was the
morningness-eveningness type for nurses with shifting work hours. Other factors were
considered as potential confounders in the advanced statistical explorations in this study.
Afterwards, we utilized univariate logistic regressions to estimate the relative risk of each
variable on worse sleep quality. After that, potential confounders were involved in
constructing the final model of detecting the effect of morningness-eveningness type for
sleep quality among nurses. To explore which components would be sensitive to
individual morningness-eveningness types of the nurses, we performed linear regressions
by separating PSQI components to detect the effect of morningness-eveningness type for
each component. SPSS 12.0 for Windows was utilized to perform all the statistical
analyses and the significance level (P value) was set as 0.05.
Results
the results from comparing the baseline of two groups. Age, years of duty, and
morningness-eveningness types were significantly different between the groups with
and without worse sleep quality. Specifically, older nurses and longer employment
duration showed decreased risk for worse sleep quality (OR = 0.93, 95% CI:
0.89-0.98; OR = 0.95, 95% CI: 0.90-0.99, respectively). It was noteworthy that E-
types revealed a significantly increase risk of worse sleep quality (OR = 6.56, 95% CI:
1.89-22.88). None of the other risk factors showed a significant effect on sleep quality,
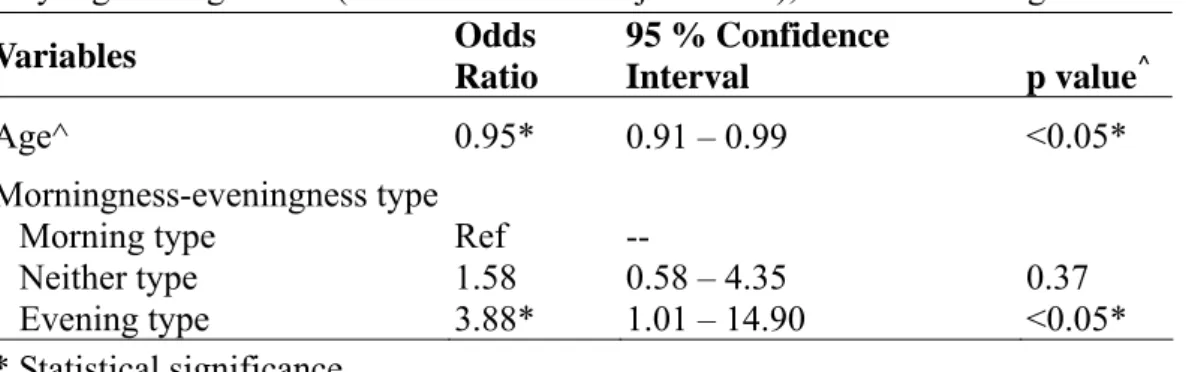
in terms of PSQI (Table 2). For precise estimation of the effects in our study
(morningness-eveningness type), confounding control was achieved for age and years
of duty. Because of the collinearity between age and years of duty, their 95% CIs were
widened and the statistical significance lost in multivariate analyses. Thus, in Table 3,
we decided to control the age as the only confounder and achieved the best relative
risk estimation for morningness-eveningness types (evening type OR = 3.88, 95% CI:
1.01-14.90, relative to morning type). Consequently, when age was properly
controlled, E-type nurses working on shifting jobs had a higher risk for poor sleep
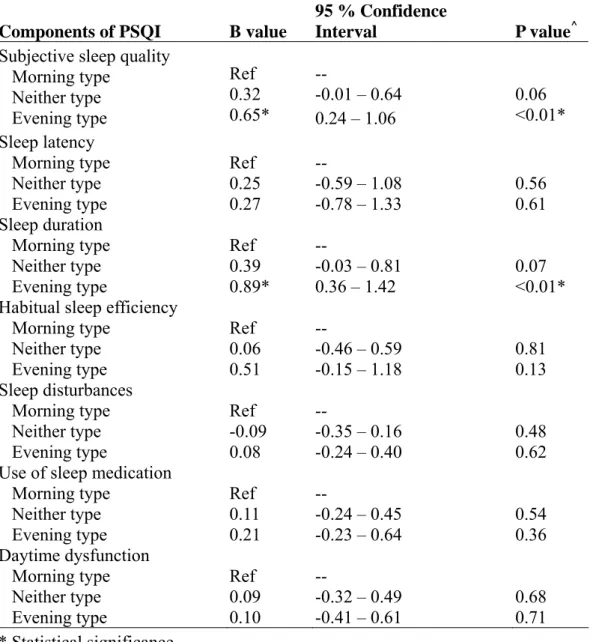
quality. To further explore the PSQI components, the scores of component 1
(subjective sleep quality) and Component 3 (sleep duration) were significantly raised
for E-type nurses. Namely, nurses with evening type had apparent poor subjective
in bed was significantly lower than the ones of morning type.
Discussion
This study was employed questionnaires to measure morningness-eveningness and
sleep quality of shift nurses. It was to analyze correlates of sleep quality by comparing
these groups with better or worse sleep quality according to the median of PSQI (8).
Univariate and multivariate analyses were used to identify the risk factors of worse
sleep quality. The result showed that the strongest predictor of sleep quality was the
subject’s natural morningness-eveningness sleep pattern not the shift schedule or shift
pattern. Although this result could not confirm the relationship of cause and effect in
sleep quality, we indicated that considering morningness-eveningness type of nurses
was an important issue for sleep quality in rotating shift nurses.
The study found a significant change in age and years of duty on sleep quality in
shift nurses (table 1). This result was consistent with previous studies(Carrier et al.
1997). After further analyzing the results, we found that older age and longer years of
duty decreased the risk of worse sleep quality. This result was not in line with that
increasing age associated with less time asleep or increased number of awakenings
during the sleep period(Carrier et al. 1997). However, this result was consistent with
According to Harma (1993) greater tolerance to shift work was related with more
control hours of work through individual choice with regard to shift system
acceptability. This study may imply that more experienced nurses could have greater
tolerance to shift work, which allows them sleep well.
M-types show a preference for waking at an early hour and experience alertness
early in the day. E-types show a preference for sleeping at latter hours and function
better in the afternoon and evening (Giannotti et al. 2002). Previous studies indicated
that E-types find adjustment to night shifts easier (Paine et al. 2006). Therefore, it is
better to understand the effect of morningness/eveingness on sleep quality for nurses
before knowing their acceptability and adjustment to shift work. This study surveyed
the relationship among morningness-eveningness type, shift pattern and sleep quality.
We differentiated the shift schedule by checking the nurse’s actual duty time to make
the shift pattern parameter more precise. This result showed that shift schedule or shift
pattern was not correlated with sleep quality. However, the sleep quality was
correlated with morningness-eveningness. This finding may hint nurses working at
night or arranging shift schedule should assess their endogenous type (morningness
and eveningness) at first. Whether shift work reflects morningness-eveingness sleep
habit or it influence shift work is interesting and warrants further exploration.
Especially, nurses with evening type reflected negative extremes on two areas:
subjective sleep quality and sleep duration; however, changes declined on the rest five
areas: sleep latency, habitual sleep efficiency, sleep disturbances, use of sleeping
medication and daytime dysfunction. These findings may be explained as follows:
First, E-types tend to vary considerably their sleep/ waking time and sleep length
(Ishihara et al. 1992; Kerkhof 1985; Monk et al. 1994). They delayed their sleep wake
schedules more than morningness type. This study showed that E-types sleep from
1AM to 4 AM and wake up from 10AM to 2PM, while M-types sleep from 10 PM to
12 PM and wake up from 6AM to 8AM in the day shift and off duty time. We
confirmed that E-types had more changeable sleep-wake schedules than M-types.
Second, E-types were related with a greater need for sleep (Taillard et al. 1999). This
study indicated the sleep length of E-types around 5 hours to 8 hours in the day shift
and evening shift, but around 10 to 12 hours in their days off. E-types had more
irregular sleep-waking time, this situation resulted in a sleep debt during their day
shift and extended their sleep duration in their off time.
We analyzed correlates of sleep quality and tried to understand changes of
morningness-eveningness for shiftwork nurses as a reference. A longitudinal survey
would propose more efficient suggestions. We hope that shift problems of doctors and
Acknowledgements
This study was supported by Tri-service General Hospital Foundation in Taiwan
(Research Grant TSGH-C94-095).
References
Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR & Kupfer DJ (1989) The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28, 193-213.
Cajochen C, Brunner DP, Krauchi K, Graw P & Wirz-Justice A (1995) Power density in theta/alpha frequencies of the waking EEG progressively increases during sustained wakefulness. Sleep 18, 890-894.
Carrier J, Monk TH, Buysse DJ & Kupfer DJ (1997) Sleep and
morningness-eveningness in the 'middle' years of life (20-59 y). J Sleep Res 6, 230-237.
Coffey LC, Skipper JK, Jr. & Jung FD (1988) Nurses and shift work: effects on job performance and job-related stress. J Adv Nurs 13, 245-254.
Dijk DJ, Brunner DP & Borbely AA (1991) EEG power density during recovery sleep in the morning. Electroencephalogr Clin Neurophysiol 78, 203-214.
Finelli LA, Baumann H, Borbely AA & Achermann P (2000) Dual
electroencephalogram markers of human sleep homeostasis: correlation between theta activity in waking and slow-wave activity in sleep. Neuroscience 101, 523-529.
Gander PH, DE nguyen BE, Rosekind MR & connell LJ (1993) Age, circadian rhythms, and sleep loss in flight crews. Avitation, Space and Evironmental Medicine 64, 189-195.
Giannotti F, Cortesi F, Sebastiani T & Ottaviano S (2002) Circadian preference, sleep and daytime behaviour in adolescence. J Sleep Res 11, 191-199.
Harma M (1993) Individual differences in tolerance to shiftwork: a review. Ergonomics 36, 101-109.
Ishihara K, Miyake S, Miyasita A & Miyata Y (1992) Morningness-eveningness preference and sleep habits in Japanese office workers of different ages. Chronobiologia 19, 9-16.
review. Biol Psychol 20, 83-112.
Knauth P, Landau K, Droge C, Schwitteck M, Widynski M & Rutenfranz J (1980) Duration of sleep depending on the type of shift work. Int Arch Occup Environ Health 46, 167-177.
Monk TH, Petrie SR, Hayes AJ & Kupfer DJ (1994) Regularity of daily life in relation to personality, age, gender, sleep quality and circadian rhythms. J Sleep Res 3, 196-205.
Niedhammer I, Lert F & Marne MJ (1994) Effects of shift work on sleep among French nurses. A longitudinal study. J Occup Med 36, 667-674.
Olsson K, Kandolin I & Kauppinen-Toropainen K (1990) Stress and coping strategies of three-shift workers. Le Travail Humain 53, 213-226.
Paine SJ, Gander PH & Travier N (2006) The epidemiology of
morningness/eveningness: influence of age, gender, ethnicity, and
socioeconomic factors in adults (30-49 years). J Biol Rhythms 21, 68-76. Poissonnet CM & Veron M (2000) Health effects of work schedules in healthcare
professions. J Clin Nurs 9, 13-23.
Skipper JK, Jr., Jung FD & Coffey LC (1990) Nurses and shiftwork: effects on physical health and mental depression. J Adv Nurs 15, 835-842.
Taillard J, Philip P & Bioulac B (1999) Morningness/eveningness and the need for sleep. J Sleep Res 8, 291-295.
Wang YW (1997) Effect of Acupressure on the sleep disturbance of Taiwanese elderly. Unpublished doctoral dissertation Case Western Reserve University,
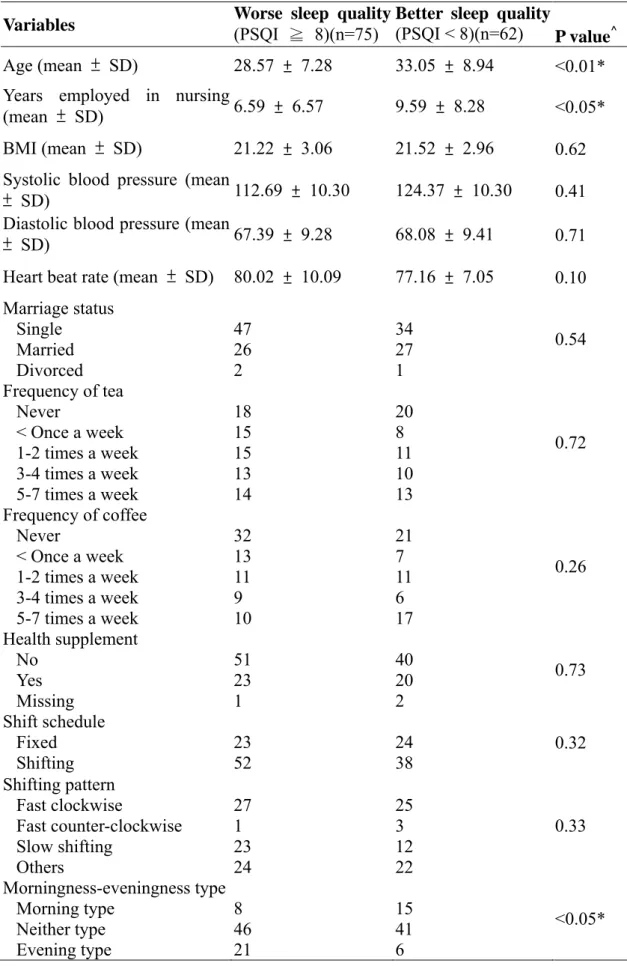
Table 1 Basic characteristics and comparisons of the groups with better or worse sleep quality by the median of PSQI (N= 137)
Variables Worse sleep quality(PSQI ≧ 8)(n=75) Better sleep quality (PSQI < 8)(n=62)
P value^ Age (mean ± SD) 28.57 ± 7.28 33.05 ± 8.94 <0.01* Years employed in nursing
(mean ± SD) 6.59 ± 6.57 9.59 ± 8.28 <0.05* BMI (mean ± SD) 21.22 ± 3.06 21.52 ± 2.96 0.62 Systolic blood pressure (mean
± SD) 112.69 ± 10.30 124.37 ± 10.30 0.41 Diastolic blood pressure (mean
± SD) 67.39 ± 9.28 68.08 ± 9.41 0.71
Heart beat rate (mean ± SD) 80.02 ± 10.09 77.16 ± 7.05 0.10 Marriage status Single Married Divorced 47 26 2 34 27 1 0.54 Frequency of tea Never < Once a week 1-2 times a week 3-4 times a week 5-7 times a week 18 15 15 13 14 20 8 11 10 13 0.72 Frequency of coffee Never < Once a week 1-2 times a week 3-4 times a week 5-7 times a week 32 13 11 9 10 21 7 11 6 17 0.26 Health supplement No Yes Missing 51 23 1 40 20 2 0.73 Shift schedule Fixed Shifting 23 52 24 38 0.32 Shifting pattern Fast clockwise Fast counter-clockwise Slow shifting Others 27 1 23 24 25 3 12 22 0.33 Morningness-eveningness type Morning type Neither type Evening type 8 46 21 15 41 6 <0.05*
variables
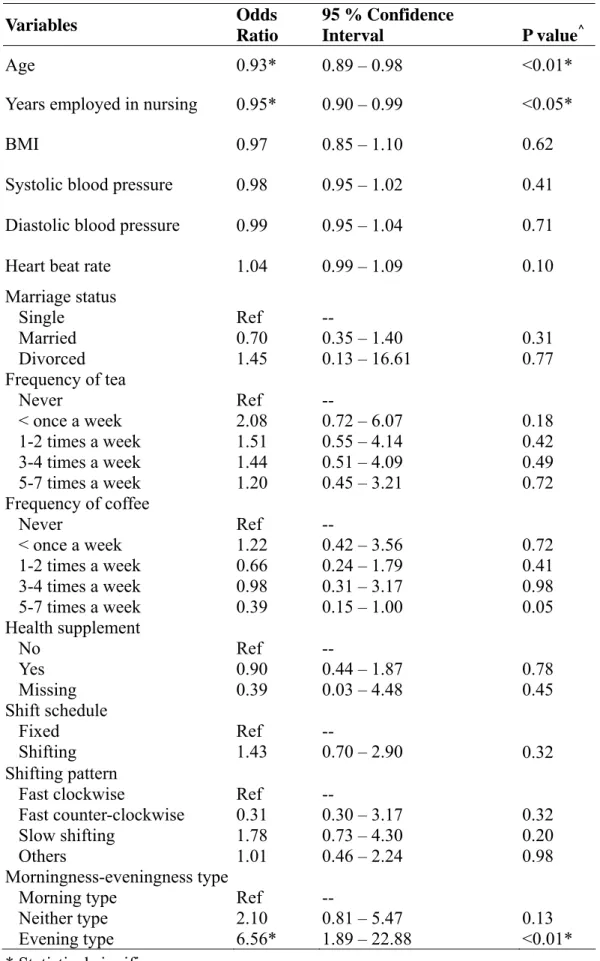
Table 2 Univariate analyses for the risk factors of worse sleep quality (PSQI ≧ 8) by logistic regressions (N= 137) Variables Odds Ratio 95 % Confidence Interval P value^ Age 0.93* 0.89 – 0.98 <0.01*
Years employed in nursing 0.95* 0.90 – 0.99 <0.05*
BMI 0.97 0.85 – 1.10 0.62
Systolic blood pressure 0.98 0.95 – 1.02 0.41 Diastolic blood pressure 0.99 0.95 – 1.04 0.71 Heart beat rate 1.04 0.99 – 1.09 0.10 Marriage status Single Married Divorced Ref 0.70 1.45 -- 0.35 – 1.40 0.13 – 16.61 0.31 0.77 Frequency of tea Never < once a week 1-2 times a week 3-4 times a week 5-7 times a week Ref 2.08 1.51 1.44 1.20 -- 0.72 – 6.07 0.55 – 4.14 0.51 – 4.09 0.45 – 3.21 0.18 0.42 0.49 0.72 Frequency of coffee Never < once a week 1-2 times a week 3-4 times a week 5-7 times a week Ref 1.22 0.66 0.98 0.39 -- 0.42 – 3.56 0.24 – 1.79 0.31 – 3.17 0.15 – 1.00 0.72 0.41 0.98 0.05 Health supplement No Yes Missing Ref 0.90 0.39 -- 0.44 – 1.87 0.03 – 4.48 0.78 0.45 Shift schedule Fixed Shifting Ref 1.43 -- 0.70 – 2.90 0.32 Shifting pattern Fast clockwise Fast counter-clockwise Slow shifting Others Ref 0.31 1.78 1.01 -- 0.30 – 3.17 0.73 – 4.30 0.46 – 2.24 0.32 0.20 0.98 Morningness-eveningness type Morning type Neither type Evening type Ref 2.10 6.56* -- 0.81 – 5.47 1.89 – 22.88 0.13 <0.01* * Statistical significance
Table 3 Multivariate analysis for the risk factors of worse sleep quality (PSQI ≧ 8) by logistic regression (Total number of subjects: 137), controlled for age
Variables Odds Ratio 95 % Confidence Interval p value^ Age^ 0.95* 0.91 – 0.99 <0.05* Morningness-eveningness type Morning type Neither type Evening type Ref 1.58 3.88* -- 0.58 – 4.35 1.01 – 14.90 0.37 <0.05* * Statistical significance
Table 4 The effect of morningness-eveningness type by each component of Pittsburgh Sleep Quality Index (PSQI) with linear regressions, adjusted by age (N=137)
Components of PSQI B value
95 % Confidence
Interval P value^
Subjective sleep quality Morning type Neither type Evening type Ref 0.32 0.65* -- -0.01 – 0.64 0.24 – 1.06 0.06 <0.01* Sleep latency Morning type Neither type Evening type Ref 0.25 0.27 -- -0.59 – 1.08 -0.78 – 1.33 0.56 0.61 Sleep duration Morning type Neither type Evening type Ref 0.39 0.89* -- -0.03 – 0.81 0.36 – 1.42 0.07 <0.01* Habitual sleep efficiency
Morning type Neither type Evening type Ref 0.06 0.51 -- -0.46 – 0.59 -0.15 – 1.18 0.81 0.13 Sleep disturbances Morning type Neither type Evening type Ref -0.09 0.08 -- -0.35 – 0.16 -0.24 – 0.40 0.48 0.62 Use of sleep medication
Morning type Neither type Evening type Ref 0.11 0.21 -- -0.24 – 0.45 -0.23 – 0.64 0.54 0.36 Daytime dysfunction Morning type Neither type Evening type Ref 0.09 0.10 -- -0.32 – 0.49 -0.41 – 0.61 0.68 0.71 * Statistical significance