Kaohsiung J Med Sci September 2008 • Vol 24 • No 9 481 Infective endocarditis (IE) is the proliferation of
micro-organisms on the endocardium of the heart. Endocar-ditis caused by Mycobacterium abscessus (M. abscessus) is rare and only five cases have been published since 1975. Four of the five patients with M. abscessus endo-carditis were associated with prosthetic valve infec-tion. Only one patient with native valve endocarditis caused by M. abscessus has been published [1]. M. abscessus endocarditis has been found to be associ-ated with history of surgery (cardiac, valvular), foreign bodies, trauma, intravenous (IV) injections, hemodial-ysis or immunocompromised status. Here, we present a case of native valve endocarditis with M. abscessus infection.
C
ASEP
RESENTATIONA 29-year-old male patient who was an IV heroin abuser had an episode of methicillin susceptible Staphylococcus aureus (MSSA)-associated tricuspid valve infective endocarditis that was previously treated once in January 2006. Mild tricuspid regurgi-tation (TR) and vegeregurgi-tation (0.6× 0.9cm) were involved in the septal leaflet of the tricuspid valve as deter-mined by echocardiography. In June 2006, he was readmitted with a fever extending for 1 month. Vege-tation (0.75×1.66cm) with high echogenicity involving the septal leaflet of the tricuspid valve and moderate TR was found by echocardiography. A smear from cul-ture medium of blood culcul-ture (BACTEC system, SA bottle) showed acid-fast stain (AFS)-positive bacilli. He was treated for miliary tuberculosis (TB) initially with rifampin 600 mg/day and isoniazid 300 mg/day, ethambutol 800 mg/day, pyrazinamide 1,500 mg/day plus streptomycin 1 g/day, and he was discharged in July 2006 with afebrile status. He continued with oral
Received: Dec 21, 2007 Accepted: Apr 17, 2008
Address correspondence and reprint requests to: Dr Wen-Ter Lai, Division of Cardiology, Depart-ment of Internal Medicine, Kaohsiung Medical
University Hospital, 100 Tzyou 1st Road,
Kaohsiung 807, Taiwan. E-mail: [email protected]
M
YCOBACTERIUM ABSCESSUS
E
NDOCARDITIS
:
A C
ASE
R
EPORT AND
L
ITERATURE
R
EVIEW
Wei-Chung Tsai,1,2Hsiao-Cheng Hsieh,3Ho-Ming Su,1Po-Liang Lu,2Tsung-Hsien Lin,1,2 Sheng-Hsiung Sheu,1,2and Wen-Ter Lai1,2
1Division of Cardiology, Department of Internal Medicine, Kaohsiung Medical University Hospital, 2Department of Internal Medicine, Faculty of Medicine, College of Medicine, Kaohsiung Medical
University, and 3Department of Internal Medicine, Kaohsiung Municipal Hsiao-Kang Hospital, Kaohsiung, Taiwan.
Infective endocarditis owing to Mycobacterium abscessus infection is rarely reported. Most cases of infective endocarditis caused by Mycobacterium abscessus are seen in patients after valve replace-ment. Although early surgical intervention is recommended and medical treatment with antibi-otics according to the susceptibility to the pathogen, such as amikacin, imipenem, cefoxitin, quinolones and macrolides, are applied, the course of such endocarditis is usually subacute and often has fatal outcomes. The present case was a 29-year-old male patient who was an intra-venous drug user who had recurrent endocarditis caused by Mycobacterium abscessus. Unusually, our reported case was infected on his native valve. However, we experienced recurrence despite antimicrobial therapy. For culture-negative endocarditis, physicians should consider the possibility of Mycobacterium abscessus infection and related treatment difficulties.
Key Words:endocarditis, Mycobacterium abscessus (Kaohsiung J Med Sci 2008;24:481–6)
rifampin 600 mg/day and isoniazid 300 mg/day, ethambutol 800 mg/day and pyrazinamide 1,500 mg/ day after discharge.
In August 2006, he was admitted again with relapse of the fever. The blood culture obtained at the patient’s hospitalization in June 2006 was identified to be M. abscessus according to a polymerase chain reaction (PCR)-restriction fragment length polymor-phism (RFLP) analysis of the 65-kDa heat shock protein (Figure 1) [2]. Echocardiography revealed a 2.3× 1.9 cm vegetation over the septal leaflet of the tricuspid valve and severe TR. The vegetation was bigger than that recorded during the previous echo-cardiogram in June 2006. In response to the presence of M. abscessus in the blood culture, he started treat-ment with clarithromycin 500 mg/day and imipenem 250 mg twice daily for 4 weeks. He was discharged with afebrile status and was free from heart failure. Echocardiography before discharge revealed that the vegetation size had decreased to 1.73× 1.69 cm. He continued with oral clarithromycin 500 mg/day plus moxifloxacin 400 mg/day treatment until November 2006.
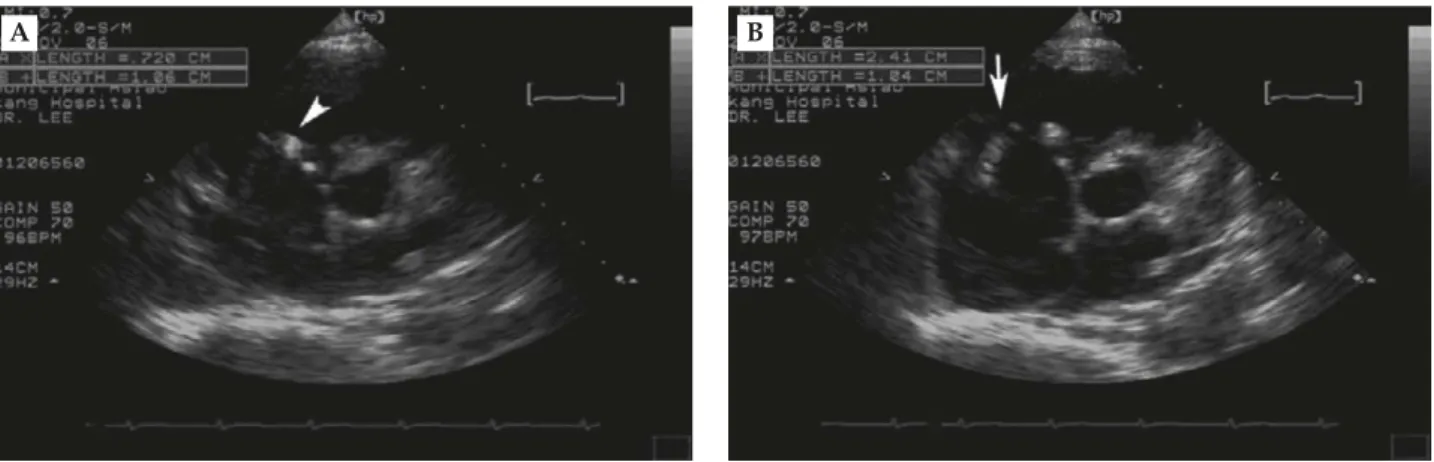
In November 2006, he was readmitted for recur-rent infective endocarditis. Echocardiography revealed severe TR with two vegetations (0.72× 1.06 cm; 2.41 × 1.04 cm) over the septal and anterior leaflets of the tricuspid valve (Figures 2A and 2B). Chest X-ray re-vealed pneumonia over the right middle lung field. Initial laboratory data revealed: white blood cell count (WBC) 7,730/μL; hemoglobin 10.1 g/dL; platelets 120,000/μL; blood urea nitrogen 35.6mg/dL; creatinine 2.04 mg/d; and C-reactive protein (CRP) 104 mg/L.
Blood culture still showed AFS-positive bacilli but neg-ative findings for common aerobic pathogens. Because of suspected TB-associated IE, he was treated with rifampin 600 mg/day and isoniazid 300 mg/day, eth-ambutol 800 mg/day plus clarithromycin 500 mg twice daily. Surgical intervention was strongly suggested, but the patient hesitated and finally received contin-ued medical therapy. Chest computed tomography
300 bp 250 bp 200 bp 150 bp 100 bp 50 bp 240 bp BstE II 210 bp 145 bp 50 bp 60 bp 70 bp Hae III M
Figure 1.PCR-RFLP for isolates of M. abscessus. The restriction
enzyme used to generate the PCR-RFLP pattern for each lane is indicated. Lane M= molecular size marker (50-bp ladder).
A B
Figure 2.Echocardiography: parasternal short axis view. Two vegetations are shown. (A) Vegetation A (0.72× 1.06 cm) was observed
at the septal leaflet of the tricuspid valve (arrowhead). (B) Vegetation B (2.41× 1.04 cm) was observed at the anterior leaflets of the tricuspid valve (arrow). The echogenicity of the vegetation is high compared with the adjacent heart tissue.
demonstrated TB pneumonia-like lesions in the right lower and middle lung with right pleural effusion and pericardial effusion. Blood cultures still produced M. abscessus. A sputum smear revealed AFS-positive bacilli and sputum culture grew M. abscessus. Since the M. abscessus endocarditis relapsed after imipenem, clarithromycin and moxifloxacin treatment, clar-ithromycin plus amikacin were chosen as the treat-ment regimen. After treattreat-ment with clarithromycin 500 mg twice daily plus amikacin 750 mg/day for 2 weeks, he became afebrile and vital signs stabilized. There were no signs of heart failure. The pneumonia-like lesions improved after antibiotic treatment, and laboratory data before discharge were: CRP 73 mg/L (normal range, <5mg/L); and WBC 6,670/μL. He was discharged with continuing oral clarithromycin 500 mg twice daily plus ciprofloxacin 400 mg twice daily for 8 weeks at our clinic, and was then lost to follow-up.
At his last visit to our clinic in January 2007, we repeated the echocardiography. It revealed that the size of the vegetations had decreased to 0.8× 1.5 cm and 2.2× 1.1 cm over the septal and anterior leaflets of the tricuspid valve, respectively, and the TR was still severe. The patient had poor medication compli-ance and “doctor shopping” between hospitals. Even though we planned for him to receive surgical inter-vention and a full course of antibiotic treatment, he hesitated and was subsequently lost to follow-up and did not receive further management from us. The patient had positive rheumatoid factor, decreased com-plement level (C3, 28.1 mg/dL; C4, 9.25 mg/dL) and decreased CD4 count (155/mm3), but was negative for human immunodeficiency virus antibody and negative for antinuclear antibodies.
D
ISCUSSIONInfective endocarditis caused by M. abscessus is very rare and unique; accordingly, we have reviewed the literature about the care and prognosis of this dis-ease. M. abscessus is grouped with a number of rapid-growth nontuberculous mycobacteria (NTM), which includes M. fortuitum, M. chelonae, and M. abscessus. These rapid-growth NTM have been found in potable and natural water, and in soil. They can also be iso-lated from contaminated tap water. Infection with M. abscessus may lead to localized infections such as subcutaneous abscesses, lymphadenitis, pneumonia,
keratitis, prosthetic valve endocarditis, osteomyelitis, meningitis and disseminated infection [3–5]. The pulmonary lesion and the endocarditis caused by M. abscessus in this case were identified based on the PCR-RFLP study of the gene encoding for the 65-kDa heat shock protein [2].
To our knowledge, only one other case has been reported in the literature to have native valve endo-carditis caused by M. abscessus [1]. In a review of the English-language publications, endocarditis caused by M. chelonae (formerly M. chelonae subspecies chelonae) or M. abscessus (formerly M. chelonae subspecies abscessus) has been documented in only nine cases. Since M. abscessus has also been classified as M. che-lonae before, we reviewed endocarditis with the search terms of M. chelonae and M. abscessus but not of M. fortuitum. Five of the nine cases were infected with M. abscessus and the others were infected by M. che-lonae. Seven of them were associated with prosthetic valve endocarditis, but none of them survived after treatment. The only surviving case was associated with native valve endocarditis [1,3,5–10]. Most of the cases infected with NTM endocarditis were subacute and had fatal outcomes, especially those with pros-thetic valve endocarditis (Table). Infective endocarditis owing to NTM infection was considered when asso-ciated with the status after valvular and cardiac sur-gery, immunocompromised hosts, intravenous drug abuse, dialysis, patients who received renal transplant and immunosuppressive therapy, and individuals on corticosteroid therapy [3,5,6,9].
The case we reported is only the second patient to have native valve endocarditis infected by M. abscessus. The portal of entry in our case was not clear, but may be attributed to his use of tap water for heroin pow-der dilution and for injection. Another contributing factor was his immune system compromise with low complement, low CD4 level and positive rheumatoid factor, which may be related to his drug abuse, although the decreased complement level and posi-tive rheumatoid factor may be the result of IE.
Rapid-growth NTM has been reported to be re-sistant to many antimicrobial agents, including most primary and secondary line antituberculosis agents in vitro. However, some strains of M. abscessus and M. chelonae were found to be sensitive to amikacin, clarithromycin, cefoxitin, erythromycin and quinolone [3,10]. Combination therapy with different classes of antimicrobial agents is usually recommended because
T
able.
Clinical characteristics of patients with infective endocar
ditis due to Mycobacterium abscessus infection Case Refer ence Age (yr)/ Involved Pr osthetic Pathogen Cultur e Antibiotics Disease duration Outcome sex valve valve sour ce 1 Rumisek et al [9] 25/F Mitral, Hancock M. chelonei ssp Pr osthesis RIF + ER Y 1979.4–1982.10 Died pr osthesis por cine chelonei biopr osthesis 2 Levy et al [7] 55/M Aortic, Hancock M. chelonei Pr osthesis Isoniazid + 1976.12–1977.1 Unknown pr osthesis por cine AMK + RIF + biopr osthesis clofazimine 3 Liebeskind et al [1] 35/M Mitral, None M. chelonei ssp Blood, CSF , CLR + FOX 7 mo Died native abscessus BM 4 Galil et al [3] 66/M T ricuspid, None M. chelonei ssp Blood, lung, CIP + CLR 1994.10–1995 Alive native chelonei tricuspid valve 5 Repath et al [8] 43/M Mitral, Starr -Edwar ds M. chelonei Blood, BM ER Y + KAN 1971.4–1972.1 Died aortic, pr osthesis pr osthesis 6 Altmann et al [6] 45/M Aortic, Bjork-Shiley M. chelonei ssp Blood, Lincomycin + 1972.6–1973.7 Died pr osthesis artificial abscessus pr osthesis cloxacillin 7 V iscidi et al [10] 55/M Mitral, Kay-Shiley/ M. chelonei ssp Blood, urine, AMK + ER Y + 1979.3–1979.8 Died pr osthesis Bjork-Shiley abscessus BM, sputum, ethionamide pr osthesis × 2 wound 8 W allace et al [5] 53/M Pr osthesis N/A M. chelonei ssp N/A N/A N/A Died abscessus 9 W allace et al [5] 50/M Pr osthesis N/A M. chelonei ssp N/A N/A N/A Died abscessus 10 This case 29/M T ricuspid, None M. chelonei ssp Blood, AMK + CIP + 2006.8–2007.5 Alive native abscessus sputum CLR M. chelonei = Mycobacterium chelonei ; ssp = subspecies; RIF = rifampin; ER Y = erythr omycin; AMK = amikacin; CSF = cer ebr ospinal fluid; BM = bone marr ow; CLR = clarithr omycin; FOX = cefoxitin; CIP = cipr ofloxacin; KAN = kanamycin; N/A =
monotherapy was found to cause resistance of NTM [11]. The duration of antimicrobial therapy in patients with NTM-related endocarditis is still controversial. Previous reports have suggested that the antimicro-bial treatment should last for at least 6 months or 3 months after aggressive surgical intervention [3]. Owing to frequent failure of medical treatment, early surgical intervention in combination with antimicro-bial treatment has been recommended for patients with NTM-related endocarditis [3,4,9,10]. Our case was treated with clarithromycin plus amikacin, and antimicrobial therapy was shifted to the oral form of ciprofloxacin plus clarithromycin for 8 weeks after discharge. It is not clear whether the exacerbation of IE could be restrained by clarithromycin plus ciprofloxacin treatment because the patient in our case study was treated for only 8 weeks and then lost to follow-up.
In summary, infective endocarditis caused by M. abscessus and other rapid-growth mycobacterium is not readily diagnosed and treated. For culture-negative endocarditis, awareness of the possibility of NTM infection should be considered, especially when patients have related predisposing factors.
R
EFERENCES1. Liebeskind DS, Ostrzega N, Wasterlain CG, et al. Neurologic manifestations of disseminated infection with Mycobacterium abscessus. Neurology 2001;56:810–3.
2. Telenti A, Marchesi F, Balz M, et al. Rapid identifica-tion of mycobacteria to the species level by polymerase chain reaction and restriction enzyme analysis. J Clin
Microbiol 1993;31:175–8.
3. Galil K, Thurer R, Glatter K, et al. Disseminated
Mycobacterium chelonae infection resulting in
endo-carditis. Clin Infect Dis 1996;23:1322–3.
4. Robicsek F, Hoffman PC, Masters TN, et al. Rapidly growing nontuberculous mycobacteria: a new enemy of the cardiac surgeon. Ann Thorac Surg 1988;46: 703–10.
5. Wallace RJ Jr, Swenson JM, Silcox VA, et al. Spectrum of disease due to rapidly growing mycobacteria. Rev
Infect Dis 1983;5:657–79.
6. Altmann G, Horowitz A, Kaplinsky N, et al. Prosthetic valve endocarditis due to Mycobacterium chelonei. J Clin
Microbiol 1975;1:531–3.
7. Levy C, Curtin JA, Watkins A, et al. Mycobacterium
chelonei infection of porcine heart valves. N Engl J Med
1977;297:667–8.
8. Repath F, Seabury JH, Sanders CV, et al. Prosthetic valve endocarditis due to Mycobacterium chelonei. South
Med J 1976;69:1244–6.
9. Rumisek JD, Albus RA, Clarke JS. Late Mycobacterium
chelonei bioprosthetic valve endocarditis: activation
of implanted contaminant? Ann Thorac Surg 1985;39: 277–9.
10. Viscidi R, Geller A, Caplan W, et al. Prosthetic valve endocarditis caused by Mycobacterium chelonei: case report and literature review. Heart Lung 1982;11:555–9. 11. Tebas P, Sultan F, Wallace RJ Jr, et al. Rapid
de-velopment of resistance to clarithromycin following monotherapy for disseminated Mycobacterium chelonae infection in a heart transplant patient. Clin Infect Dis 1995;20:443–4.
收文日期:96 年 12 月 21 日 接受刊載:97 年 4 月 17 日 通訊作者:賴文德主任 高雄醫學大學附設醫院心臟內科 高雄市 807 三民區自由一路 100 號