Kaohsiung J Med Sci March 2010 • Vol 26 • No 3 154
© 2010 Elsevier. All rights reserved.
Kaposiform hemangioendothelioma (KHE) is a very infrequent tumor found predominantly in infants and adolescents with intermediate malignant and locally aggressive characteristics [1]. It is more often located in the limbs and is uncommon in the head and neck regions [2], as well as rarely involving the nose and paranasal sinuses [3]. Radiologically, hemangioen-dothelioma shows as hyperintense on T2-weighted images or inversion-recovery sequences and when well-enhanced, and it resembles a hemangioma. Hema-ngioendothelioma may contain flow voids of vascular structures or hemorrhagic foci [1]. We report a case of KHE of the maxillary sinus with unusual imaging manifestations.
C
ASEP
RESENTATIONA 4-month-old female infant had progressive swelling of the right cheek without associated local heat, tender-ness, or redness for 2 weeks. In addition, swelling of the right soft palate and upper gingiva, nasal obstruc-tion, sclera injecobstruc-tion, and ecchymosis of the lower eyelids were also depicted on physical examination. She was not hospitalized for other medical or surgi-cal disease and received vaccination as scheduled. Findings of laboratory studies included thrombocyto-penia, consumption coagulopathy, and microangio-pathic hemolysis.
Computed tomography and magnetic resonance imaging were arranged to determine the cause of swelling of the right cheek. Sinus computed tomog-raphy showed an isodense to hyperdense mass mainly in the right maxillary sinus with bone destruction, the right middle cranial fossa, and right orbital extension (Figure 1). Magnetic resonance imaging revealed that the mass was markedly hypointense on fat-suppressed T2-weighted sequences, and was slightly hypointense
Received: Jun 15, 2009 Accepted: Jul 6, 2009 Address correspondence and reprint requests to: Dr Twei-Shiun Jaw, Department of Medical Imag-ing, Kaohsiung Medical University Hospital, 100 Tzyou 1stRoad, Kaohsiung 807, Taiwan.
E-mail: [email protected]
K
APOSIFORM
H
EMANGIOENDOTHELIOMA
A
RISING
F
ROM THE
M
AXILLARY
S
INUS
: A C
ASE
R
EPORT
Chin-Ho Lee,1Twei-Shiun Jaw,1,3Sheau-Fang Yang,2,3and Ding-Kwo Wu1,3
Departments of 1Medical imaging and 2Pathology, Kaohsiung Medical University Hospital, and 3Faculty of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Kaposiform hemangioendothelioma is a very infrequent, locally aggressive vascular neoplasm, characterized by fascicular spindle cell proliferation. It occurs almost exclusively in infants and adolescents, and is often associated with Kasabach-Merritt phenomenon. The tumor is predomi-nantly located subcutaneously or in the deep soft tissue of the extremities and trunk, peritoneum, or retroperitoneum. However, this tumor can sometimes be located on the head and neck. We report a case of kaposiform hemangioendothelioma of the maxillary sinus in a 4-month-old female infant presenting with cheek swelling, thrombocytopenia, anemia, and disseminated intravascular coagulation. Sinus computed tomography presented an enhancing, bone-destructing tumor. Magnetic resonance images showed an uncommon appearance as mostly low signal inten-sity on T2-weighted images.
Key Words:head and neck, kaposiform hemangioendothelioma, Kasabach-Merritt phenomenon, maxillary sinus
KHE of the maxillary sinus
Kaohsiung J Med Sci March 2010 • Vol 26 • No 3 155
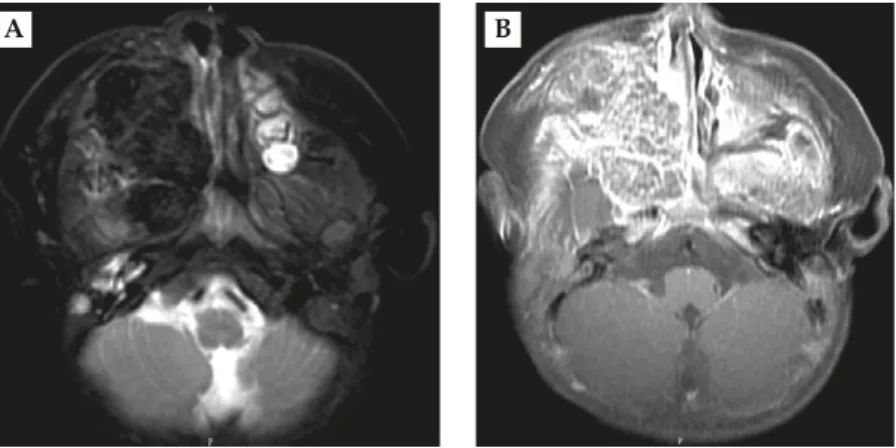
on T1-weighted sequences with moderate peculiar reticular enhancement after intravenous administra-tion of contrast material (Figure 2). There was no imag-ing evidence of prominent vascularity. A biopsy was performed and microscopic examination showed KHE with spindle cell proliferation with fascicular growth interspersed with slit-like vascular lumina containing numerous red blood cells. Nuclear atypia and mitotic figures were inconspicuous. Immunohistochemical study demonstrated CD34+ and CK− for the tumor, which confirmed the vascular nature (Figure 3).
D
ISCUSSIONKHE is a rare vascular tumor that occurs almost exclusively in children. Only a few cases have been reported in the literature since the first described case
A B
Figure 1.(A) Axial non-enhanced computed tomographic image showing a soft tissue mass (arrowhead) in the right maxillary sinus with adjacent bony destruction. (B) Coronal contrast-enhanced computed tomography shows the enhanced soft tissue mass (arrowhead) involving the right middle cranial fossa.
A B
Figure 2. (A) Axial T2-weighted image demonstrating an extremely hypointense expansile mass in the right maxillary sinus. (B) Gadolinium-enhanced T1-weighted axial image demonstrating a peculiar reticular enhancing tumor without definite vascular structure within the mass.
Figure 3.Microscopy shows spindle cell proliferation with fasci-cular growth interspersed with slit-like vasfasci-cular lumina contain-ing numerous red blood cells (original magnification, 100×). The spindle cells are labeled with the endothelial cell marker CD34 (insert; original magnification, 400×).
Kaohsiung J Med Sci March 2010 • Vol 26 • No 3 156
C.H. Lee, T.S. Jaw, S.F. Yang, and D.K. Wu
in 1971 [2]. Nearly 75% of cases present as cutaneous lesions of trunk and limbs and the second most com-mon location (18%) is in the retroperitoneum [4]. Cases in the head and neck regions are uncommon; we found only one report of a KHE in the ethmoid sinus of an 8-year-old girl [5]. We present here KHE of the maxil-lary sinus in an infant.
KHE is classified as an intermediate malignant vascular neoplasm [1] due to locally aggressive behav-ior but without distant metastasis, and can present as multifocal lesions [6]. In contrast to infantile heman-giomas, there is no tendency of spontaneous regression for KHE.
Radiologically, KHE can present as an expansile osteolytic lesion with irregular margins and exten-sion into the adjacent soft tissue. Hemorrhagic foci and flow voids of vascular structures may be seen [1]. KHE typically has a well-enhancing soft tissue component with magnetic resonance hyperintensity on T2-weighted images and hypointensity on T1-weighted images compared with muscle [7]. Unlike these characteristic imaging appearances, our case showed mostly extremely low signal intensity on fat-suppressed T2-weighted images and irregular enhanc-ing margins. Histologically, KHE consists of infiltrative multilobular spindle cell proliferation with slit-like vascular spaces resembling capillary hemangioma and Kaposi’s sarcoma [6]. Differentiation from the latter two is made by the presence of well-formed spindle cell fascicles and the absence of periodic-acid-Schiff-positive globules [1]. Lesions demonstrate low or no mitotic appearance and minimal cellular atypia in the endothelial cells. Immunohistochemi-cally, there is a heterogeneous population of immature endothelial cells expressing CD31 and CD34. Positive reactions for factor VIII or alpha smooth muscle actin also can be detected [5].
KHE is frequently associated with Kasabach–Merritt phenomenon (KMP) including thrombocytopenia, consumption coagulopathy, and microangiopathic
hemolysis, especially in younger patients and patients with larger vascular tumors [8]. This association is known as a poor prognostic predictor. Another feature of KHE is the involvement of adjacent bony struc-tures [8]. In our case, there was destruction of the maxillary bone, as well as elevation of D-dimers, and low platelet and red blood cell counts. More than 90% of cases with KMP are secondary to KHE [7].
It is important to consider the diagnosis of KHE when KMP is present, even in patients with an un-common location and atypical imaging findings.
R
EFERENCES1. Chang JM, Kwon BJ, Han MH, et al. Kaposiform he-mangioendothelioma arising from the internal auditory canal. AJNR Am J Neuroradiol 2006;27:931–3.
2. Maseda E, Blanco R, Ablanedo A, et al. Oropha-ryngeal Kaposiform Hemangioendothelioma. Acta
Otorrinolaringol Esp 2008;59:198–9.
3. Semino L, Pagella F, Delù G, et al. Endoscopic treat-ment of ethmoidal hemangioendothelioma: case report and review of the literature. Am J Otolaryngol 2006;27: 287–90.
4. Mac-Moune Lai F, To KF, Choi PC, et al. Kaposiform hemangioendothelioma: five patients with cutaneous lesion and long follow-up. Mod Pathol 2001;14:1087–92. 5. Birchler MT, Schmid S, Holzmann D, et al. Kaposiform hemangioendothelioma arising in the ethmoid sinus of an 8-year-old girl with severe epistaxis. Head Neck 2006;28:761–4.
6. Deraedt K, Vander Poorten V, Van Geet C, et al. Multi-focal kaposiform haemangioendothelioma. Virchows Arch 2006;448:843–6.
7. Chen YJ, Wang CK, Tien YC, et al. MRI of multifocal kaposiform haemangioendothelioma without Kasabach– Merritt phenomenon. Br J Radiol 2009;82:e51–4. 8. Vetter-Kauczok CS, Ströbel P, Bröcker EB, et al.
Kaposiform hemangioendothelioma with distant lym-phangiomatosis without an association to Kasabach-Merritt-Syndrome in a female adult! Vasc Health Risk
Kaohsiung J Med Sci March 2010 · Vol 26 · No 3 157