Open Access
Research article
Variations of care quality for infectious pulmonary tuberculosis in
Taiwan: a population based cohort study
Wei-Sheng Chung
1,2, Ray-E Chang*
2,5and How-Ran Guo
3,4Address: 1Hualien General Hospital, Department of Heath, Executive Yuan, Hualien, Taiwan, 2Graduate Institute of Health Care Organization
Administration, College of Public Health, National Taiwan University, Taipei, Taiwan, 3Department of Environmental and Occupational Health,
College of Medicine, National Cheng Kung University Hospital, National Cheng Kung University, Tainan, Taiwan, 4Department of Occupational
and Environmental Medicine, National Cheng Kung University Hospital, National Cheng Kung University, Tainan, Taiwan and 5No. 17,
Shu-Chow Rd., Room 639, Taipei 100, Taiwan
Email: Wei-Sheng Chung - [email protected]; Ray-E Chang* - [email protected]; How-Ran Guo - [email protected] * Corresponding author
Abstract
Background: Effective and efficient care is required to prevent the spread of infectious pulmonary tuberculosis (PTB). We attempted to compare care quality among different healthcare institutions in Southern Taiwan.
Methods: This study conducted population-based retrospective cohort design. One tuberculosis sanatorium, 2 medical centers, 11 regional hospitals, and 15 district hospitals and primary practitioners in the study area had reported tuberculosis cases, registered from January 1 to June 30 2003. Those cases with sputum positive PTB were followed 15 months after anti-tuberculosis treatment initiation. Meanwhile, Level of conformance with diagnostic guidelines, efficiency of diagnostic and treatment process, and treatment were measured as main outcome. Association was investigated using Chi-square tests, Kruskal Wallis tests, Mann-Whiteney U tests, and multiple logistic regression analysis to evaluate outcome differences among different levels of institutions. Results: The analyses included 421 patients. In comparison with patients receiving treatment at medical centers, regional hospitals, and district hospitals/primary practitioners, patients at the Chest Specialty Hospital were more likely to provide at least three sputum specimens (74.1% vs. 48.2%, 36.8%, and 50.0%), shorter workdays examining sputum smears (2.4 ± 2.4 days vs. 2.6 ± 2.1, 4.5 ± 3.1, and 3.5 ± 2.6 days), shorter interval between the first consultation and treatment (10.1 ± 18.3 days vs. 31.0 ± 53.6, 31.2 ± 70.4, and 25.4 ± 37.6 days), and a higher successful treatment rate (92.6% vs. 65.2%, 63.9%, and 68.0%). Furthermore, after adjusting age and gender, the patients treated by the pulmonologists and treated at Chest Specialty Hospital had significantly more successful treatment rate, of which odds ratios were 1.74 and 4.58 respectively.
Conclusion: Differences in care quality exist among different types of healthcare institutions and among individual physicians. The implementation of practice guidelines should contribute to an improvement in the care quality of the treatment and diagnosis of PTB.
Published: 11 June 2007
BMC Public Health 2007, 7:107 doi:10.1186/1471-2458-7-107
Received: 14 October 2006 Accepted: 11 June 2007 This article is available from: http://www.biomedcentral.com/1471-2458/7/107
© 2007 Chung et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background
Pulmonary tuberculosis is a global problem currently resulting in the death of approximately 2 million people each year. If more stringent control is not implemented, approximately 1 billion people will become newly infected, 150 million people will become symptomatic, and 36 million will die from the disease between 2002 and 2020 [1].
For the past several decades, Taiwan committed itself to reduce the epidemic of tuberculosis. The mortality rate from tuberculosis has decreased from more than 100 cases per 100,000 people in the early 1950s to 5.8 cases per 100,000 people in 2003. However, in recent years, newly infected tuberculosis cases appear to be on the increase; the incidence rate has increased from approxi-mately 50 cases per 100,000 in the early 1990s to more than 60 per 100,000 since the late 1990s [2]. Tuberculosis remains the leading infectious cause of death in Taiwan. The control of tuberculosis remains one of the major chal-lenges faced by Taiwan's health care administration. Taiwan's health care system has been significantly reformed in recent years. Two reform policies, which have profoundly influenced tuberculosis care are: (1) the intro-duction of the National Health Insurance and (2) the restructure of the tuberculosis control system. In 1995, Taiwan implemented a compulsory universal health insurance program for its residents. This program main-tains a contract with more than 90% of Taiwan's health care institutions and without a referral system, insured persons are provided with complete freedom regarding choice of physician [3]. Thus, all patients with tuberculo-sis can freely seek medical aid at any healthcare institution from offices of primary practitioners to hospitals. Previously, Taiwan adopted a dedicated tuberculosis con-trol system with an extensive network reaching each town-ship. This system effectively contained the spread of tuberculosis. However, during the late 1990s, the govern-ment-owned health care institutions underwent a dra-matic reorganization. The tuberculosis control system was merged into the general health care system. Four sanatoria institutions located in northern, central, and southern Tai-wan were reduced to one. In 2001, the Chest Specialty Hospital was the only remaining tuberculosis sanatorium. These two influencing policies have resulted in an increas-ing trend in the number of tuberculosis patients treated by institutions other than tuberculosis sanatoria. By 2001, only 10% of all patients with tuberculosis were reported by tuberculosis sanatoria [4]. However, at the same time, the number of newly reported patients had increased, with a reporting rate of 75 cases per 100,000 people in 2002. Moreover, the cure rate for newly diagnosed pulmo-nary tuberculosis patients was 75%, which is lower than
the 85% target set by the World Health Organization (WHO) [5].
To effectively contain the spread of tuberculosis, the avail-ability of quality medical care to patients is essential. The efficiency of the diagnosis process and effective treatment for cases with infectious pulmonary tuberculosis (PTB) are important factors. Therefore, the purpose of this study was to evaluate the quality of diagnosis and treatment at different levels of healthcare institutions in Taiwan.
Methods
A population-based medical record review in southern Taiwan, where the study perimeters included four admin-istrative areas: Chiayi County, Chiayi City, Tainan County, and Tainan City, covering 2.7 million residents, was performed. As authorized by law in Taiwan, all sus-pected and confirmed tuberculosis cases should be reported in a timely manner to the national computerized registry, maintained by the Center for Disease Control (CDC). Reporting of cases has been encouraged and rein-forced through the implementation of a no-notification-no-reimbursement policy and the notification-for-fee pol-icy since 1997 [6]. We requested data on all suspects and confirmed tuberculosis patients residing in the studied areas from the registry for the period January 1 to June 30, 2003.
Site visits to hospitals were arranged to review the medical records of each patient. Prior to these visits, the team, including four registered nurses (each with a minimum of 6 years clinical experience), two chief nurses (each with a minimum of 12 years clinical experience), and one pul-monologist, had received a series of training courses. The training was designed to ensure proper validation of data consistency. Medical records of the diagnostic and treat-ment processes were reviewed.
Infectious PTB
Infectious PTB is referring to sputum culture-confirmed disease caused by Mycobacterium tuberculosis or two spu-tum smear examinations positive for acid-fast bacilli [7].
Healthcare institutions
The institutions that had reported cases in the study area included the Chest Specialty Hospital (the only remaining tuberculosis sanatorium in Taiwan, which is geared towards specialized thoracic disease care, mainly for tuberculosis), 2 medical centers, 11 regional hospitals, and 15 district hospitals and primary practitioners (dis-trict hospitals and primary practitioners are regarded as at the same level in terms of the treatment of tuberculosis). In addition to inpatient services, hospitals in Taiwan pro-vide considerable outpatient services, accounting for approximately 50% of their revenues, and are accredited
by three levels. Medical centers, housing over 500 acute staffed beds, are designated to assume the responsibilities of providing healthcare services, training medical profes-sionals, and conducting research. Regional hospitals have no less than 250 acute beds and are staffed with physi-cians of various specialties with the purpose of providing healthcare services to patients and training for specialists. District hospitals are designated to provide primary healthcare services, which are similar to those offered by primary practitioners in clinics providing outpatient serv-ices.
Quality of care
Quality of care was measured using three groups of indi-cators: the level of compliance with diagnostic guidelines during diagnosis, the efficiency of diagnostic and treat-ment processes, and the outcome of treattreat-ment.
The diagnostic process should include a complete exami-nation of the patient's symptoms, chest X-ray, sputum smear and cultures. Amongst the diagnostic quality indi-cators were the percentage of successful collection of at least three sputum specimens from the patients at the institution [8-10], and the percentage of patients with a positive sputum smear who demonstrated negative spu-tum culture results, which might result from having received anti-tuberculosis treatment or laboratory errors [11,12]. For the timeliness of the diagnostic and treatment process, the number of days, between the chest X-ray examination and the hospital visit, between the sputum examination and the hospital visit, laboratory diagnostic delay and healthcare institution delay were calculated. The laboratory diagnostic delay was defined as the number of workdays required for reporting sputum smear examination results, and the healthcare institution delay was defined as the number of days from the first related hospital visit to the initiation of anti-TB medication. Indicators of the outcome of treatment included the suc-cessful treatment rate and the fatality rate. The patients who received successful treatment indicated that they had been cured or had received complete treatment. A cured case was defined as a patient with PTB who had com-pleted treatment with a negative bacteriology result dur-ing the course of treatment and at the end of treatment. A case with a completed treatment was defined as a patient with PTB who had finished treatment, but with no bacte-riology result at the end of treatment. A fatality case referred to a patient whose death occurred for any cause during the course of treatment [13].
Ethical consideration
The CDC approved the present study. All staff involved in the study signed a letter of agreement to maintain patient confidentiality.
Data analysis
Chi-square tests were performed to evaluate the differ-ences in proportions of dichotomous and categorical var-iables. Since the distributions of indicators of timeliness were skewed, Kruskal Wallis tests were performed to eval-uate the differences in these indicators among different levels of institutions. In addition Mann-Whitney U tests were used to compare two individual groups of sampled data. A multiple logistic regression was constructed using successful treatment or fatality of TB as the dependent var-iable. Independent variables include age, gender, treat-ment by the pulmonologist, and treattreat-ment at the Chest Specialty Hospital. Odds ratio (OR) and 95% confidence interval (CI) of it were used to estimate the effects of inde-pendent variables on successful treatment and fatality. All analyses were conducted using SPSS 10.0 statistical soft-ware, and all statistical tests were performed at the two-tailed significance level of 0.05.
Results
From January 1 to June 30 2003, 491 patients with TB, who showed at least two positive sputum smears or a pos-itive culture, were reported in the study area. Among these patients, the medical records of 482 (98%) patients were reviewed. After reviewing medical records, 61 patients were excluded from the study; including one foreign lab-orer who was deported after diagnosis, 11 patients with extrapulmonary tuberculosis, 38 misdiagnosed patients and 11 patients without any documented positive sputum smears or positive cultures. Therefore, 421 patients, 311 male (73.9%) and 110 female (26.1%), were included in the analyses. Patient age at diagnosis ranged from 18 to 95 years, (mean, 66 years), and the number of patients increased with age (13 below 25 years of age, 35 from 25 to 44 years of age, 110 from 45 to 64 years of age, and 263 above 64 years of age). The majority (95.0%) of patients were symptomatic, and the most common symptoms observed were cough (78.8%), fever (41.7%), and dysp-nea (29.3%). The most common co-morbidity observed was diabetes (34.3%). No cases of AIDS were observed. While 134 (31.9%) out of the 420 patients revealed cavi-tations on chest X-ray examinations, one patient (0.2%) showed normal findings. Nearly one-half (201; 47.7%) of patients had provided three or more sputum specimens, and 392 (93.1%) presented sputum cultures for mycobac-teria. Fifteen months after treatment was initiated, the rate of successful treatment among patients who underwent complete follow-up was 68.9%.
Fifty-four patients (12.8%) were treated at the Chest Spe-cialty Hospital, 112 (26.6%) at medical centers, 155 (36.8%) at regional hospitals, and 100 (23.8%) at district hospitals or by primary practitioners (Table 1). The pro-portion of patients treated by pulmonologists also varied
across different levels of healthcare institutions (p < 0.001), with the Chest Specialty Hospital containing the highest proportion of patients.
Most patients (74.1%) provided at least three sputum specimens for examination at the Chest Specialty Hospi-tal; however, the proportion was only 48.2%, 36.8%, and 50.0% at medical centers, regional hospitals, and district hospitals/primary practitioners, respectively (p < 0.001) (Table 1). A positive sputum smear preceding a negative sputum culture result was more common at district hospi-tals/primary practitioners than at other institutions (p < 0.001).
Regarding efficiency in the diagnosis and treatment, the mean healthcare institution delay was 10.1 days at the Chest Specialty Hospital, which was shorter than those at medical centers, regional hospitals, and district hospitals/ primary practitioners (31.0 days, 31.2 days, and 25.4 days, respectively) (p < 0.01, for all comparisons). Whereas the number of days between the chest X-ray examination and the hospital visit were similar, the number of days between the sputum examination and the hospital visit varied among different levels of healthcare institutions (p < 0.05 for both) and was shortest at the Chest Specialty Hospital. Furthermore, the Chest Spe-cialty Hospital had the shortest mean laboratory diagnos-tic delay (2.4 days vs. 2.6 days, 4.5 days, and 3.5 days).
The Chest Specialty Hospital achieved a 92.6% successful treatment rate, which was higher than medical centers, regional hospitals, and district hospitals/primary practi-tioners (65.2%, 63.9%, and 68.0%, respectively, p < 0.01 for all comparisons) (Table 1). Moreover, the fatality rate at the Chest Specialty Hospital was the lowest among the institutions (5.6% vs. 27.7%, 32.3%, and 28.0%, p < 0.05 for all comparisons).
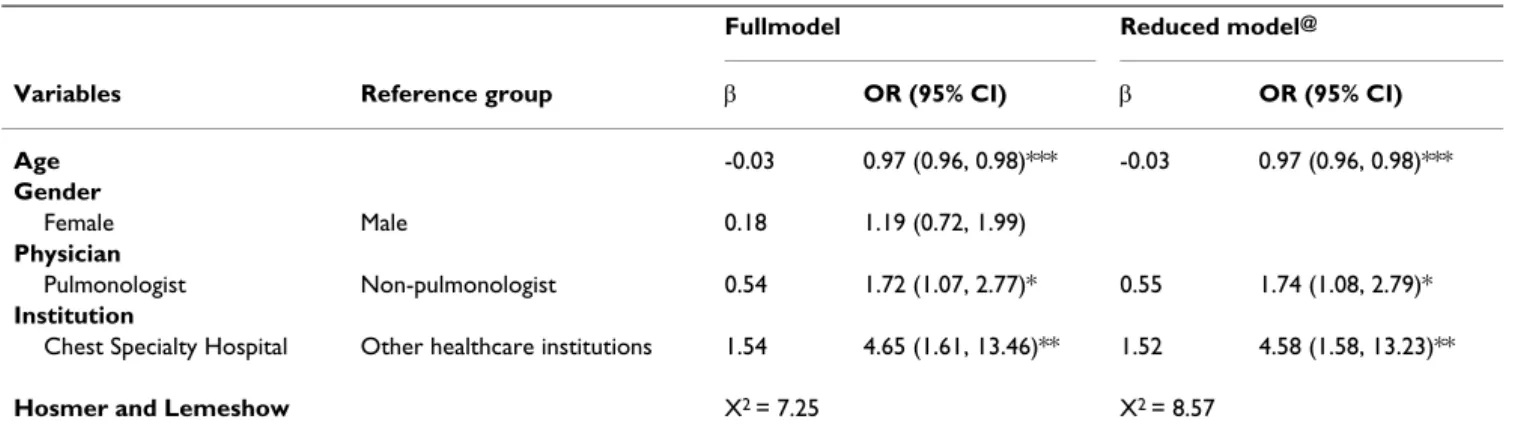
Full model and reduced model of multiple regression analyses revealed that patients of advanced age had less successful treatment rate, of which OR (95% CI) was 0.97 (0.96, 0.98). The patients who were treated by the pulmo-nologists and treated at Chest Specialty Hospital had more successful treatment rate, which OR were 1.74 (1.08, 2.97) and 4.58 (1.58, 13.23) respectively (Table 2). Mean-while, we also discovered that amongst pulmonologists, those who provided services at the Chest Specialty Hospi-tal had more successful treatment rate with OR 4.23 (1.45, 12.40) after adjusting age and gender (Table 3).
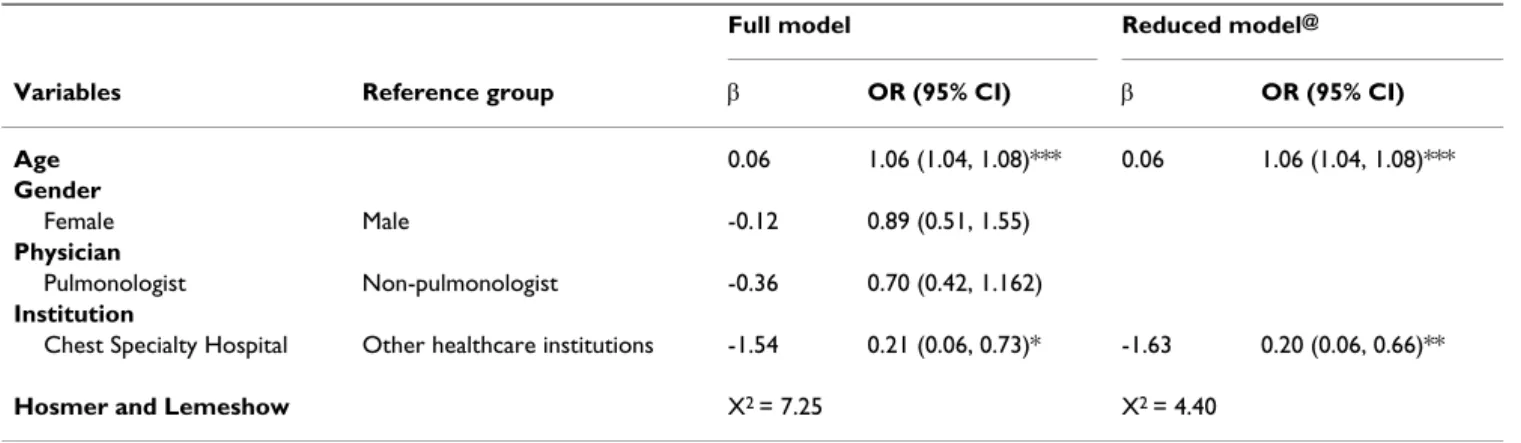
Furthermore, the patients of advanced age had more fatal-ity rate, of which OR 1.06 (1.04, 1.09). The patients who were treated at Chest Speciatly Hospital had less fatality with OR 0.20 (0.06, 0.66) (Table 4).
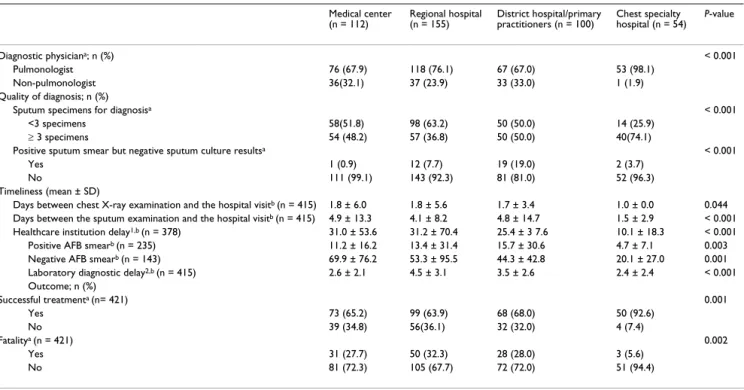
Table 1: Comparison of care quality at different levels of institutions
Medical center (n = 112) Regional hospital (n = 155) District hospital/primary practitioners (n = 100) Chest specialty hospital (n = 54) P-value Diagnostic physiciana; n (%) < 0.001 Pulmonologist 76 (67.9) 118 (76.1) 67 (67.0) 53 (98.1) Non-pulmonologist 36(32.1) 37 (23.9) 33 (33.0) 1 (1.9) Quality of diagnosis; n (%)
Sputum specimens for diagnosisa < 0.001
<3 specimens 58(51.8) 98 (63.2) 50 (50.0) 14 (25.9)
≥ 3 specimens 54 (48.2) 57 (36.8) 50 (50.0) 40(74.1)
Positive sputum smear but negative sputum culture resultsa < 0.001
Yes 1 (0.9) 12 (7.7) 19 (19.0) 2 (3.7)
No 111 (99.1) 143 (92.3) 81 (81.0) 52 (96.3)
Timeliness (mean ± SD)
Days between chest X-ray examination and the hospital visitb (n = 415) 1.8 ± 6.0 1.8 ± 5.6 1.7 ± 3.4 1.0 ± 0.0 0.044
Days between the sputum examination and the hospital visitb (n = 415) 4.9 ± 13.3 4.1 ± 8.2 4.8 ± 14.7 1.5 ± 2.9 < 0.001
Healthcare institution delay1,b (n = 378) 31.0 ± 53.6 31.2 ± 70.4 25.4 ± 3 7.6 10.1 ± 18.3 < 0.001
Positive AFB smearb (n = 235) 11.2 ± 16.2 13.4 ± 31.4 15.7 ± 30.6 4.7 ± 7.1 0.003
Negative AFB smearb (n = 143) 69.9 ± 76.2 53.3 ± 95.5 44.3 ± 42.8 20.1 ± 27.0 0.001
Laboratory diagnostic delay2,b (n = 415) 2.6 ± 2.1 4.5 ± 3.1 3.5 ± 2.6 2.4 ± 2.4 < 0.001
Outcome; n (%) Successful treatmenta (n= 421) 0.001 Yes 73 (65.2) 99 (63.9) 68 (68.0) 50 (92.6) No 39 (34.8) 56(36.1) 32 (32.0) 4 (7.4) Fatalitya (n = 421) 0.002 Yes 31 (27.7) 50 (32.3) 28 (28.0) 3 (5.6) No 81 (72.3) 105 (67.7) 72 (72.0) 51 (94.4)
AFB, acid-fast bacilli
aUsing the chi-square test bUsing the Kruskal Wallis test
1Healthcare institution delay indicates days between the first related hospital visit and the initiation of anti-TB medication 2Laboratory diagnostic delay indicates workdays for reporting sputum smear examination results at the hospital
Discussion
The persistence of infectious PTB as a major public health problem results from the presence of individuals with active infection in whom the disease remains undiag-nosed or in whom a delay in diagnosis occurs [14-17]. The varied quality of healthcare provided by public and pri-vate sectors, and the failure of some healthcare providers to diagnose tuberculosis promptly and to ensure the deliv-ery of adequate treatment are two major factors contribut-ing to the poor control of tuberculosis [18]. Despite the fact that the NHI program has improved the accessibility of healthcare services to patients, tuberculosis cases con-tinue to increase in Taiwan. This phenomenon prompted our investigation into the variations in care quality for infectious PTB patients at different levels within health-care institutions.
In our study, male predominance and elderly susceptibil-ity to infection by infectious PTB were observed, which are consistent with other published data [19-21]. Patients treated at the Chest Specialty Hospital were more likely to follow the international diagnostic guideline, which is the presentation of at least three sputum specimens for
exam-ination [9,10]. This might be due to more education and awareness of infectious PTB among patients cared for at the Chest Specialty Hospital. A higher proportion of pos-itive sputum smears with subsequent negative sputum culture results was observed in district hospitals/primary practitioners. It is possible that district hospitals/primary practitioners are not as experienced as larger institutions or specialty institution. Thus, the laboratory performance at district hospitals/primary practitioners was not compa-rable to the quality at larger institutions. Poor laboratory diagnoses may affect the prescribing of anti-TB medica-tions by physicians, which in turn may adversely affect the patient's safety [22]. Sputum smear microscopy is a sim-ple, inexpensive, and appropriate technique for diagnos-ing tuberculosis, and laboratories in healthcare institutions should have qualified technicians performing this technique [8,9]. Failing this, sputum examinations should be referred to the central laboratories responsible for testing sputum specimens in each district [23]. The present study has shown that laboratory diagnostic delay and healthcare institution delay, regardless of acid-fast smear, were shorter at the Chest Specialty Hospital,
Table 2: Multiple logistic regression for factors affecting the successful treatment
Fullmodel Reduced model@
Variables Reference group β OR (95% CI) β OR (95% CI) Age -0.03 0.97 (0.96, 0.98)*** -0.03 0.97 (0.96, 0.98)*** Gender Female Male 0.18 1.19 (0.72, 1.99) Physician Pulmonologist Non-pulmonologist 0.54 1.72 (1.07, 2.77)* 0.55 1.74 (1.08, 2.79)* Institution
Chest Specialty Hospital Other healthcare institutions 1.54 4.65 (1.61, 13.46)** 1.52 4.58 (1.58, 13.23)** Hosmer and Lemeshow X2 = 7.25 X2 = 8.57
@ reduced model using forward substitution; * p < 0.05, ** p < 0.01, *** p < 0.001
Table 3: Multiple logistic regression for factors affecting the successful treatment
Full model Reduced modela
Varia bles Reference group β OR (95% CI) β OR (95% CI) Age -0.04 0.96 (0.94, 0.98)*** -0.04 0.97 (0.94, 0.98)*** Gender
Female Male 0.29 1.33 (0.72, 2.47)
Pulmonologist at
Chest Specialty Hospital Other healthcare institutions 1.44 4.23(1.45, 12.40)** 1.42 4.13 (1.41, 12.05)** Hosmer and Lemeshow X2 = 9.06 X2=ll.96
which is most likely due to its greater vigilance for infec-tious PTB detection. However, even this prompt care can-not be initiated until a patient has sought or been referred for treatment. In this regard, patients themselves contrib-uted to seeking treatment, and such delays were inde-pendent of the healthcare institution. Further extensive public health education programs may be necessary to strengthen the public awareness of infectious PTB and thereby decrease patient delay in seeking care.
Efficient diagnosis and prompt treatment are the key com-ponents to the effective control of infectious PTB [14,24,25]; and, according to practice guidelines for the treatment of tuberculosis [10], the rate of successful treat-ment is a good performance indicator of diagnosis and treatment. The high successful treatment rate observed at the Chest Specialty Hospital (up to 92.6%), moreover, after adjusting age and gender, the patients treated at Chest Specialty Hospital still had more successful treat-ment rate and less fatality rate. That might be due to the physicians' expertise with the disease and more efficient diagnostic and treatment process. Patients treated by pul-monologists appeared to have a higher successful treat-ment rate than patients treated by non-pulmonologist physicians. Perhaps a pivotal factor lies within the unfa-miliarity non-pulmonologist physicians have with the treatment of TB patients. Furthermore, the fact that patients treated by pulmonologists at the Chest Specialty Hospital had a higher successful treatment rate than those who were treated by pulmonologists at other institutions might indicate that both training of care providers and the institution providing the care are important factors affect-ing the quality of care. Whereas clinical status and severity of the disease might affect successful treatment rate and fatality rates, no variables are available in the database we obtained to address this issue. Therefore, we were unable to evaluate the effects of these factors to the results, which could be a major limitation of the current study. Issues regarding patient delays have previously been studied
[26-28]. The aim of this study was to identify variations in the quality of diagnosis and treatment of infectious PTB patients at different levels within healthcare institutions, and we found that both training of care providers and the institution providing the care are important factors affect-ing the quality of care. Our study showed that non-adher-ence to a consistent approach to the diagnosis and treatment for PTB at different levels within healthcare institutions might result in various successful treatment rates and that although pulmonologists provided better care than other physicians, the successful treatment rates achieved seemed different between pulmonologists at the Chest Specialty Hospital and pulmonologists at other institutions. In order to promote the quality of infectious PTB patient care in Taiwan to the same level as that at the Chest Specialty Hospital, extensive education programs and implementation of practice guidelines for tuberculo-sis for medical staff at the other institutions are strongly recommended. Furthermore, it is recommended that the healthcare institutions should also monitor their own diagnostic quality and the efficiency and effectiveness of treatment to patients.
Conclusion
Differences in quality of care exist among different types of healthcare institutions and among individual physi-cians. The implementation of practice guidelines should contribute to an improvement in the quality of care in the treatment and diagnosis of PTB.
List of abbreviations
PTB pulmonary tuberculosis WHO World Health Organization CDC Center for Disease Control AFB acid-fast bacilliTable 4: Multiple logistic regression for factors affecting the fatality rate
Full model Reduced model@
Variables Reference group β OR (95% CI) β OR (95% CI) Age 0.06 1.06 (1.04, 1.08)*** 0.06 1.06 (1.04, 1.08)*** Gender Female Male -0.12 0.89 (0.51, 1.55) Physician Pulmonologist Non-pulmonologist -0.36 0.70 (0.42, 1.162) Institution
Chest Specialty Hospital Other healthcare institutions -1.54 0.21 (0.06, 0.73)* -1.63 0.20 (0.06, 0.66)** Hosmer and Lemeshow X2 = 7.25 X2 = 4.40
Publish with BioMed Central and every scientist can read your work free of charge "BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK Your research papers will be:
available free of charge to the entire biomedical community peer reviewed and published immediately upon acceptance cited in PubMed and archived on PubMed Central yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
Competing interests
The author(s) declare that they have no competing inter-ests.
Authors' contributions
WSC and REC contributed to conception and design, acquisition of data, analysis and interpretation of data, and were involved in drafting the manuscript. HRG devoted himself to revising it and providing critical and important intellectual content. All authors read and approved the final manuscript.
Acknowledgements
The authors are grateful to the Department of Health in Taiwan for pro-viding research grants.
References
1. WHO, Tuberculosis Fact Sheet [http://www.who.int/mediacen
tre/factsheet/whol04]
2. Department of Health: Main causes of death in Taiwan 2002. Health and National Health Insurance Health Annual Statistics Information Service 2003.
3. Cheng SH, Chiang TL: The effect of universal health insurance
on health care utilization in Taiwan. Results from a natural experiment. JAMA 1997, 278:89-93.
4. Wu YJ: Overview of tuberculosis prevalence, problems, and
policy in Taiwan. Tuberculosis prevention policy convention in Taiwan,
Center for Disease Control, Department of Health, Taiwan. Taipei 2004. 5. Center for Disease Control: Tuberculosis Annual Report 2002.
Center for Disease Control, Department of Health, Taiwan. Taipei 2003:1-158.
6. Chiang CY, Enarson DA, Yang SL, Suo J, Lin TP: The impact of
National Health Insurance on the notification of tuberculosis in Taiwan. Int J Tuberc Lung Dis 2002, 6:974-979.
7. Migliori GB, Raviglione MC, Schaberg T, Davies PD, Zellweger JP, Grzemska M, Mihaescu T, Clancy L, Casali L: Tuberculosis
man-agement in Europe. Task Force of the European Respiratory Society (ERS), the World Health Organisation (WHO) and the International Union against Tuberculosis and Lung Dis-ease (IUATLD) Europe Region. Eur Respir J 1999, 14:978-992.
8. Enarson DA, Reider HL, Arnadottir T, Trébucq A: Management of
tuberculosis: a guide for low-income countries. 5th edition.
Paris: IUATLD; 2000.
9. American Thoracic Society: Diagnostic standards and
classifica-tion of tuberculosis in adults and children. Am J Respir Crit Care
Med 2000, 161:1376-1395.
10. Horsburgh CR Jr, Feldman JS, Ridzon R: Practice guidelines for
the treatment of tuberculosis. Clin Infect Dis 2000, 31:633-639.
11. Lipsky BA, Gates J, Tenover FC, Plorde JJ: Factors affecting the
clinical value of microscopy for acid-fast bacilli. Rev Infect Dis
1984, 6:214-222.
12. Al-Moamary MS, Black W, Bessuille E, Elwood RK, Vedal S: The
sig-nificance of the persistent presence of acid-fast bacilli in spu-tum smears in pulmonary tuberculosis. Chest 1999, 116:726-731.
13. World Health Organization, International Union Against Tuberculosis and Lung Disease, Royal Netherlands Tuberculosis Association:
Revised international definitions in tuberculosis control. Int J
Tuberc Lung Dis 2001, 5:213-215.
14. Mathur P, Sacks L, Auten G, Sail R, Levy C, Gordin F: Delayed
diag-nosis of pulmonary tuberculosis in city hospitals. Arch Intern
Med 1994, 154:306-310.
15. Brudney K, Dobkin J: A tale of two cities: tuberculosis control
in Nicaragua and New York City. Semin Respir Infect 1991, 6:261-272.
16. Centers for Disease Control: National action plan to combat
multidrug-resistant tuberculosis. MMWR Morb Mortal Wkly Rep
1992, 41(RR-11):1-30.
17. Centers for Disease Control: Initial therapy for tuberculosis in
the era of multidrug resistance: recommendations of the
Advisory Council for the Elimination of Tuberculosis. MMWR
Morb Mortal Wkly Rep 1993, 42(RR7):l-8.
18. Pronyk PM, Makhubele MB, Hargreaves JR, et al.: Assessing health
seeking behaviour among tuberculosis patients in rural South Africa. Int J Tuberc Lung Dis 2001, 5:619-627.
19. Alvarez S, Shell C, Berk SL: Pulmonary tuberculosis in elderly
men. Am J Med 1987, 82:602-606.
20. Teale C, Goldman JM, Pearson SB: The association of age with
the presentation and outcome of tuberculosis: a five-year survey. Age Aging 1993, 22:289-293.
21. Korzeniewska-Kosela M, Krysl J, Muller N, Black W, Allen E, FitzGer-ald JM: Tuberculosis in young adults and the elderly: a
pro-spective comparison study. Chest 1994, 106:28-32.
22. Centers for Disease Control and Prevention (CDC): American
Thoracic Society. Update: adverse event data and revised American Thoracic Society/CDC recommendations against the use of rifampin and pyrazinamide for treatment of latent tuberculosis infection-United States, 2003. MMWR. Morbidity
& Mortality Weekly Report 2003, 52(31):735-739.
23. Hsu CP: Strategies for implementing a tuberculosis
labora-tory network. Tuberculosis prevention policy convention in Taiwan,
Center for Disease Control, Department of Health, Taiwan. Taipei 2004. 24. Rao VK, lademacro EP, Fraser VJ, Kollef MH: Delays in the
suspi-cion and treatment of tuberculosis among hospitalized patients. Ann Intern Med 1999, 130:404-411.
25. The American Lung Association Conference on Re-establishing Con-trol of Tuberculosis in the United States: Conference report. Am J Respir Crit Care Med 1996, 154:251-262.
26. Yamasaki-Nakagawa M, Ozasa K, Yamada N, Osuga K, Shimouchi A, Ishikawa N, Bam DS, Mori T: Gender difference in delays to
diag-nosis and healthcare seeking behaviour in a rural area of Nepal. Int J Tuberc Lung Dis 2001, 5:24-31.
27. Lonnroth K, Thuong LM, Linh PD, Diwan VK: Delay and
disconti-nuity – a survey of TB patients' search of a diagnosis in a diversified healthcare system. Int J Tuberc Lung Dis 1999, 3:992-1000.
28. Chiang CY, Chang CT, Chang RE, Li CT, Huang RM: Patient and
health system delays in the diagnosis and treatment of tuberculosis in Southern Taiwan. Int J Tuberc Lung Dis 2005, 9:1006-1012.
Pre-publication history
The pre-publication history for this paper can be accessed here:
http://www.biomedcentral.com/1471-2458/7/107/pre pub