行政院國家科學委員會專題研究計畫成果報告
計畫名稱:中國人之白袍高血壓的研究 (II)
Study on White Coat Hyper tension in Chinese (II)
計畫編號:NSC 88-2314-B-002-290
執行期限:87 年 8 月 1 日至 88 年 7 月 31 日
主持人:曾淵如 教授
執行機構及單位名稱:國立台灣大學醫學院內科
E-mail: [email protected]
中文摘要
在 290 名有輕度至中度高血壓病人進行 血壓參數在預測高血壓目標器官合併症的能 力。 隨機血壓測量是利用傳統式水銀柱血壓 計測定。24 小時移動式血壓記錄是利用 Del Mar Avionics 公 司 之 Model 1990 Pressurometer IV 型。高血壓之診斷依據世界 衛生組織之條件。高血壓目標器官合併症是依 據心電圖、胸部 X 光、尿液分析及眼底檢查的 評估。 顯然,在高血壓目標器官合併症的預測 上,移動式血壓參數優於隨機血壓之條件。在 移動式血壓參數中,移動式血壓值高於隨機血 壓值,逆轉之血壓週期變化型態,及血壓夜間 未降等在目標器官合併的預測上有用。在心電 圖之左心室肥厚的預測上,移動式收縮壓平均 值高於隨機收縮壓之敏感度為 23.8%,特殊度 為 97.6%,正預測值為 79.2%,而負預測值 為 77.1%;在舒張壓之比較的四項預測值分別 為 31.3%,88.6%,51%及 77.2%。收縮壓的 逆轉之 血 壓週期 型 態之四 項 預測值 分 別 為 31.3%,88.6%,51%及 77.2%;其舒張壓的 相 對 參 數 之 四 項 預 測 值 分 別 為 32.5% , 87.1%,49.1%及 77.2%。收縮壓夜間未降之 四項預測值分別為 67.5%,51.4%,34.6%及 80.6%;其舒張壓的相對參數之四項預測值分 別為 75%,33.2%,30%及 77.8%。上述三 項血壓參數在胸部 X 光診斷之左心室肥厚、蛋 白尿及眼底病變的預測也有相似的結果。 本研究顯示在高血壓目標器官合併症之 預測上,移動式血壓參數優於隨機血壓,而血 壓的分 佈 型態比 血 壓的程 度 有較高 的 預 測 值。 關鍵詞:高血壓、目標器官合併症、移動式血 壓、隨機血壓Abstr act
The ability of blood pressure parameters to predict hypertensive target organ complications was evaluated on 290 consecutive patients with mild to moderate essential hypertension.
Casual blood pressure (CBP) measurements were obtained by standard sphygmomanometric methods during the day at an outpatient clinic. Twenty-four hour ambulatory blood pressure (ABP) recording with Del Mar Avionics, Model 1990 Pressurometer IV System was performed 1 to 3 days after CBP measurements were taken. The blood pressure level for hypertension was adopted from WHO criteria. The target organ complications of hypertension were assessed by ECG, chest x-ray, urinalysis and eye-fundus examinations.
The ABP parameters are shown to be superior to CBP criteria for hypertension in predicting hypertensive target organ complications. Among the ABP parameters, a comparison between CBP and ABP levels, reversed circadian patterns of BP and nocturnal non-reduction of BP are found to be useful in predicting the target organ complications. With regard to the
predictive value for ECG evidence of left ventricular hypertrophy (LVH), a SBP average greater than casual SBP had a sensitivity of 23.8%, specificity of 97.6%, a positive predictive value of 79.2%, and a negative predictive value of 77.1%. Their counterparts in DBP gave the corresponding values of 31.3%, 88.6%, 51.0% and 77.2%, respectively. A reversed circadian pattern of SBP achieved the corresponding values of 31.3%, 88.6%, 51% and 77.2%, respectively. Their counterparts of DBP obtained the corresponding values of 32.5%, 87.1%, 49.1% and 77.2%, respectively. The nocturnal non-reduction of SBP had the corresponding values of 67.5%, 51.4%, 34.6% and 80.6%, respectively. Their counterparts in DBP obtained the corresponding values of 75%, 33.2%, 30% and 77.8%, respectively. Similar results were found in the predictive values of the above-mentioned blood pressure parameters for LVH on chest x-ray, proteinuria and retinopathy.
The study has revealed the superiority of ABP parameters to CBP values in predicting the hypertensive target organ complications. The distribution patterns of BP have also been shown to have higher predictive values for hypertensive target organ complication than those of BP levels.
Keywords: hypertension, target organ damage, ambulatory blood pressure, casual blood pressure.
Intr oduction
It is generally believed that the higher the blood pressure the more likely it is that hypertensive complications will develop. Several reports [1-3], however, showed apparent inconsistencies in the course of illness. Present knowledge about the prognostic value of blood pressure is based mostly on the results of trials in which a casual blood pressure (CBP) was adopted [4-6]. However, casual measurements of
blood pressure have their shortcomings. The predictive value of the association of office blood pressure values with hypertensive-related target organ complication is limited. In addition to the rationale that blood pressure varies widely and that casual blood pressures are unrepresentative of blood pressure at other times, the superiority of multiple measurements of blood pressure than a single measurement in the prediction of pressure-related morbid events [7-10] underlines the value of non-invasive ambulatory blood pressure monitoring, which is now an objective technique with higher reproducibility. Ambulatory blood pressure (ABP) monitoring can provide data on blood pressure distribution, patterns and levels, pressure load and load index [11-16], the method has also the virtue of obviating some of the problems inherent in office casual blood pressure measurements. The relationship between the occurrence of blood pressure-related complications and blood pressure measurements from portable records has been examined in a number of studies [17-32]. However, the predictive values of blood pressure parameters for hypertensive complications have not been sufficiently researched [33-35]. This report is an attempt to fill the lacuna in our understanding of the predictive values of blood pressure parameters for hypertensive target organ complications.
Mater ials and Methods
A total of 290 patients with mild to moderate essential hypertension diagnosed from CBP measurements obtained by standard sphygmomanometric methods during the day at an outpatient clinic were studied. At least three measurements were taken from every patient while in a sitting position. There were 168 men and 122 women, and their ages ranged from 40 to 65 years.
All the subjects underwent 24-h blood pressure recording with a commercial
ambulatory blood pressure recorder (Del Mar Avionics, model 1990 Pressurometer IV System). Ambulatory blood pressure monitoring was performed 1 to 3 days after measuring CBP. The patients were free of medication before the measurements and were normally active. All went to bed no later than between 2100 and 2200h and rose between 0500 and 0700h. Blood pressure and heart rate were measured every 10 min with an ambulatory monitoring system. The data were analyzed by a microcomputer. At the start of the monitoring period, the readings obtained by this system were crosschecked against blood pressures measured manually through the same cuff system utilizing an Y tube connected to a mercury sphygmomanometer. The data were accepted only when the difference between these two measurements was within 5 mmHg. Ambulatory blood pressure readings that showed an inconsistent increase or decrease in systolic blood pressure or diastolic blood pressure greater than 20 mmHg were not considered in this analysis [16]. Tracings were analyzed only if more than 85% of the maximal number of readings during the 24-h period passed the deletion criteria. The average ambulatory blood pressure for the whole day was calculated and compared to CBP in every patient. The pressure load and distribution pattern of ABP as well as nocturnal blood pressure reduction were also analyzed. The non-dipper of blood pressure was defined as daytime systolic and diastolic blood pressure averages that decreased by less than 10% during the night. The patients' CBP was 157 ± 14 / 100 ± 7 mmHg and their daily ABP average was 149 ± 8 / 97 ± 6 mmHg.
The target organ complications of hypertension were assessed by ECG, chest x-ray, urinalysis and eye-fundus examinations. ECG evidence of left ventricular hypertrophy was based on the criteria of Sokolow and Lyon [36]. Cardiac enlargement by radiological examination was diagnosed as a cardiothoracic ratio >
50% [37]. Changes in the optic fundi, which were examined by ophthalmologists, were classified according to a modification of the criteria of Keith et al [38]. Urinalysis was performed with Ames Reagent Strips (Multistix 9), and proteinuria was defined when the urinalysis showed a concentration of 100 mg.dl-1 or more of protein in urine. None of the examiners had any knowledge about the patients’ ambulatory and casual blood pressures. The values of CBP and parameters of ABP in predicting hypertension-related complication were analyzed by identifying
True positive (TP) = +parameter/ +complication
True negative (TN) = -parameter/ -complication
False positive (FP) = +parameter/ -complication
False negative (FN) =-parameter/ +complication and identifying TP Sensitivity = % TP + FN TN Specificity = % TN + FP TP
Positive predict value = % TP + FP
TN
Negative predict value = % TN + FN
Results
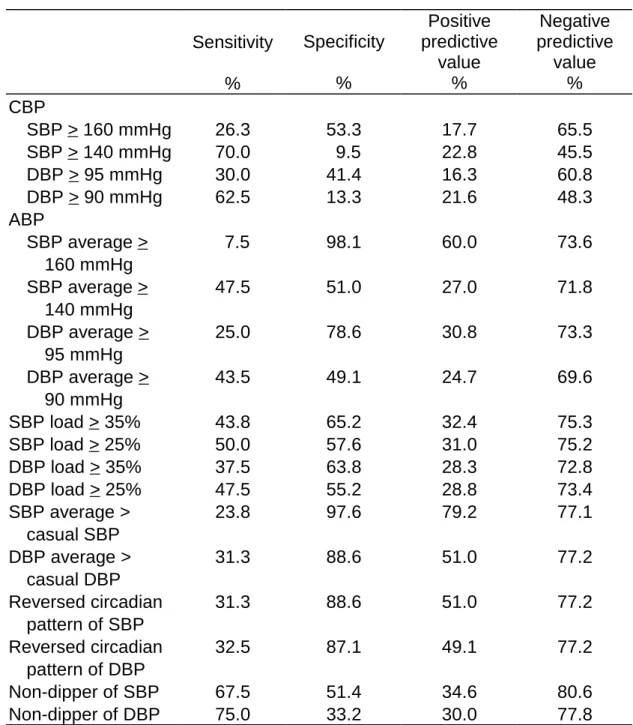
The Predictive Values of Blood Pressure Parameters for Left Ventricular Hypertrophy on Electrocardiogram
With regard to the predictive value of ECG evidence of LVH, the systolic/diastolic
CBP for borderline hypertension had a sensitivity of 70%/62.5%, a specificity of 9.5%/13.3%, a positive predictive value of 22.8%/21.6% and a negative predictive value of 45.5%/48.3%. The systolic/diastolic ABP average for borderline hypertension gave the corresponding values of 47.5%/43.5%, 51%/49.1%, 27%/24.7% and 71.8%/69.6%, respectively. The systolic/diastolic blood pressure load ≥ 25% achieved the corresponding value of 50%/47.5%, 57.6%/55.2%, 31%/28.8% and 75.2%/73.4%, respectively. An average systolic/diastolic ABP value greater than systolic/diastolic CBP value obtained the corresponding values of 23.8%/31.3%, 97.6%/88.6%, 79.2%/51% and 77.1%/77.2%, respectively. A reversal circadian pattern of systolic/diastolic ABP gave the corresponding values of 31.3%/32.5%, 88.6%/87.1%, 51%/49.1% and 77.2%/77.2%. The non-dipper of systolic/diastolic ABP had the corresponding values of 67.5%/75%, 51.4%/33.2%, 34.6%/30% and 80.6%/77.8%, respectively.
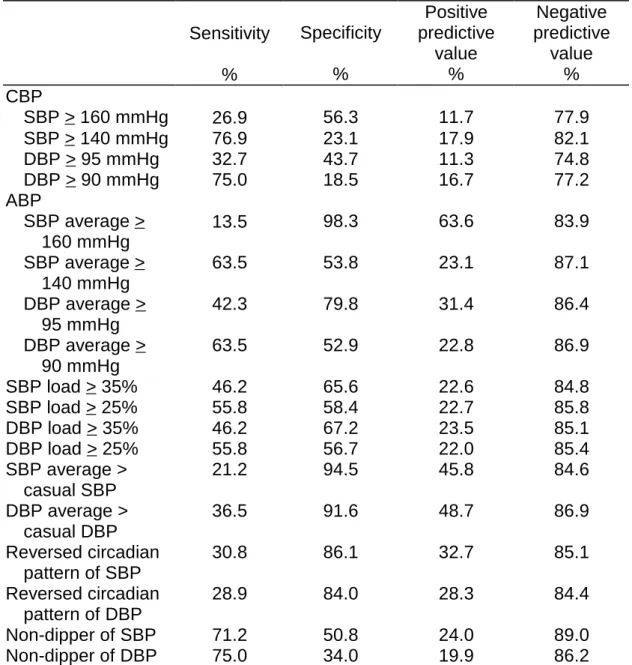
The Predictive Values of Blood Pressure Parameters for Left Ventricular Hypertrophy on Chest X-ray
As to the predictive value for LVH on chest x-ray, the diastolic CBP for borderline hypertension had a sensitivity of 75%, a specificity of 18.5%, a positive predictive value of 16.7%, and a negative predictive value of 77.2%. The diastolic ABP average for borderline hypertension gave the corresponding values of 63.5%, 52.9%, 22.8% and 86.9%, respectively. The diastolic blood pressure load ≥ 25% achieved the corresponding values of 55.8%, 56.7%, 22% and 85.4%, respectively. An average diastolic ABP value greater than diastolic CBP value obtained the corresponding values of 36.5%, 91.6%, 48.7% and 86.9%, respectively. A reversal circadian pattern of diastolic ABP gave the corresponding values of 28.9%, 84%, 28.3% and 84.4%, respectively. The non-dipper of diastolic ABP had the corresponding values of 75%, 34%, 19.9% and 86.2%,
respectively. Similar results in their systolic counterparts were obtained.
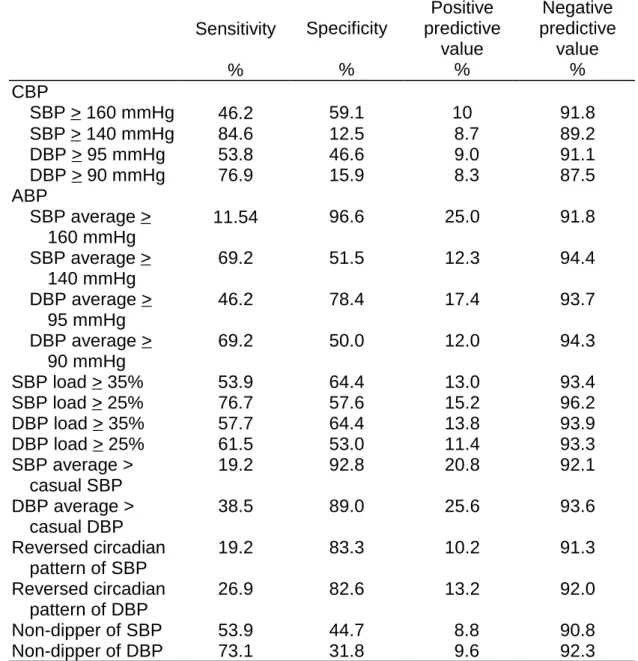
The Predictive Values of Blood Pressure Parameters for Proteinuria
Regarding the predictive value for proteinuria, the diastolic CBP for borderline hypertension had a sensitivity of 76.9%, a specificity of 15.9%, a positive predictive value of 8.3%, and a negative predictive value of 87.5%. The diastolic ABP average for borderline hypertension gave the corresponding values of 69.2%, 50%, 12% and 94.3%, respectively. The diastolic blood pressure load ≥ 25% achieved the corresponding values of 61.5%, 53%, 11.4% and 93.3%, respectively. An average diastolic ABP value greater than diastolic CBP value obtained the corresponding values of 38.5%, 89%, 25.6% and 93.6%, respectively. A reversal circadian pattern of diastolic ABP gave the corresponding values of 26.9%, 82.6%, 13.2% and 92%, respectively. The non-dipper of diastolic ABP had the corresponding values of 73.1%, 31.8%, 9.6% and 92.3%, respectively. Their systolic counterparts had similar predictive values.
The Predictive Values of Blood Pressure Parameters for Retinopathy
With regard to the predictive value for retinopathy, the diastolic CBP for borderline hypertension had a sensitivity of 87.5%, a specificity of 11%, a positive predictive value of 16.5%, and a negative predictive value of 82.9%. The diastolic ABP average for borderline hypertension gave the corresponding values of 50%, 46.7%, 15.7% and 82.5%, respectively. The diastolic blood pressure load ≥ 25% achieved the corresponding values of 58.3%, 55.4%, 20.6% and 87%, respectively. An average diastolic ABP value greater than diastolic CBP value obtained the corresponding values of 27.1%, 89.3%, 33.3% and 86.1%, respectively. A reversal circadian pattern of diastolic ABP gave the corresponding values of 37.5%, 85.5%, 34% and 87.3%, respectively. The non-dipper of diastolic
ABP had the corresponding values of 70.8%, 32.2%, 17.2% and 84.8%, respectively. Their systolic counterparts obtained similar predictive values.
Discussion
A number of important studies over the last two decades have confirmed the superiority of ABP over the CBP in predicting hypertensive target organ damage [2, 8, 17, 21, 22, 24, 25, 39, 40]. A single blood pressure measurement is reported to be predictive of the risks of end organ damage [2, 41-43]. However, these reports focus on the correlation between the level or the variability of ambulatory blood pressure and the presence of the target organ complications of hypertension [17, 18, 21, 22, 32-35, 41]. Ambulatory blood pressure monitoring can provide information not only on level of blood pressure but also its distribution patterns. It is pertinent that those patients who developed hypertensive target organ complications had a higher ambulatory pressure than casual blood pressure [19, 43-45].
Kobrin et al [46] found that hypertensive patients, who did not show nocturnal falls in systolic and diastolic blood pressures had a two-fold increase in the incidence of hypertensive complication. We have demonstrated that the frequency of a reversed circadian rhythm (systolic and diastolic) is significantly higher in hypertensive patients with target organ complications (LVH and retinopathy) [45]. Our previous report [47] also showed that a reversed circadian rhythm is found more frequently in patients with cerebral stroke. Verdecchia et al [48] found that a nocturnal reduction in systolic and diastolic blood pressure, of more than 10% of the daytime value, could delay or prevent the development of cardiac LVH, a result also confirmed in our previous report [45], but only as regards systolic blood pressure. There was no relationship between
nocturnal reduction and complications in terms of proteinuria and retinopathy.
A significant relationship between urine albumin and the level of ambulatory blood pressure was reported in Opsahl et al [28], and Giaconi et al [29]. However, in our previous report [45], proteinuria seemed to be related to pressure load but not to ambulatory blood pressure average. A positive result was also found in the relationship between proteinuria and an ambulatory blood pressure with a value greater than that of the casual blood pressure, but the difference was significant for diastolic blood pressure only.
Obviously, there is a close relationship between hypertensive target organ damage (LVH, proteinuria and retinopathy) and the parameters of 24 hour ambulatory blood pressure measurements in terms of reversed circadian pattern, nocturnal non-dip, comparisons between casual blood pressure and ambulatory blood pressure, pressure load and blood pressure average. The clinical value of the parameters of the 24-hour ambulatory blood pressure monitoring is still a matter of debate and remains to be established.
Massabuau et al [34] found the predictive value and specificity of daytime mean systolic blood pressure > 140 mmHg for echocardiographic LVH were 53% and 79% respectively, and those of nighttime mean systolic blood pressure > 120 mmHg were 80% and 45.8% respectively. In our study, for predicting electrocardiographically derived LVH, the casual SBP ≥ 160 mmHg or casual DBP ≥ 95 mmHg had a low sensitivity, specificity and positive predictive value (< 50%), and a negative predictive value of about 60%. The casual SBP ≥ 140 mmHg or casual DBP ≥ 90 mmHg had a sensitivity of about 60-70%, but a low specificity, positive predictive value and negative predictive value (< 50%). The blood pressure loads had higher sensitivity but comparable specificity, positive predictive value and negative predictive value as compared to criteria of ABP average. The comparison between ABP
average and CBP had a high specificity (> 85%), a low positive predictive value (> 50%), and a negative predictive value (> 75%). The reversed circadian pattern of BP had similar predictive values as those of comparison between ABP average and CBP. The nocturnal reduction of BPs had a low specificity and positive predictive value (≤ 50%), but a higher negative predictive value (>75%). Obviously, ABP is superior to CBP in predicting hypertension related LVH on ECG. Among ABP parameters, the ABP average > CBP and reversed circadian pattern of ABP are valuable in predicting hypertension related LVH on ECG. The ABP average, BP load, and non-significant nocturnal reduction had a high specificity and negative predictive value but a low positive predictive value. Regarding radiographically derived LVH, the above ABP parameters had a similar specificity and negative predictive value but a low positive predictive value. Similar results were found in the predictive values of blood pressure parameter for proteinuria. The predictive values of the ABP parameters for retinopathy were similar to those for electrocardiographically derived LVH.
There is a close relationship between hypertensive target organ damage (LVH, proteinuria and retinopathy) and the parameters of 24-hour ambulatory blood pressure measurements. Nevertheless, the sensitivity of these parameters for predicting target organ damage was not high. The ABP average, ABP load and nocturnal non-reduction of BP had a high specify and negative predictive value. The comparison between ABP average and CBP levels and reversed circadian pattern of BP had a higher positive predictive value in addition to high specificity and negative predictive value. Accordingly, these parameters are valuable predictors of hypertension related target organ disease.
Refer ences
1 Sokolow M, Perloff D. Prognosis of essential hypertension treated
conservatively. Circulation 1961; 23:697-713.
2 Smirk FH. Observations on the mortality of 270 treated and 199 untreated retinal grade I and II hypertensive patients followed in all instances for five years. New Zeal Med J 1964; 63:413-443.
3 Simposon FO, Gilchrist AR. Prognosis in untreated hypertensive vascular disease. Scot Med J 1958;
3:1-14.
4 Kaplan NM. Whom to treat: the dilemma of mild hypertension. Am Heart J 1981; 101:867-870.
5 Moser M. Treating hypertension: a review of clinical trials. Am J Med
1986; 81 (suppl 6C):25-32.
6 Robertson JIS. The large studies in hypertension: what have they shown?
Br J Clin Pharmac 1987; 24 (suppl
1):3S-14S.
7 Perloff D, Sokolow M, Cowan R. The prognostic value of ambulatory blood pressure monitoring in treated hypertensive patients. J Hypertens
1991; 9 (suppl 1):S33-S40.
8 Perloff D, Sokolow M, Cowan R. The prognostic value of ambulatory blood pressures. JAMA 1983; 249:2792-2798.
9 Mann S, Millar-Craig MW, Raftery EB. Superiority of 24-hour measurement of blood pressure over clinic values in determining prognosis in hypertension.
Clin Exp Hypertens 1985; 7:279-281.
10 Clement DL. Home versus office monitoring of blood pressure: a European multicentre study of high blood pressure. J Hypertens 1989; 7
(suppl 3):S49-S51.
11 Pickering TG, Harshfield GA, Kleinert HD, Blank S, Laragh JH. Blood pressure during normal daily activities, sleep, and exercise: comparison of values in normal and hypertensive subjects. JAMA 1982; 247:992-996.
12 Messerli FH, Glade LB, Ventura HO et al. Diurnal variations of cardiac rhythm,
catecholamines in borderline and established essential hypertension.
Am Heart J 1982; 104:109-114.
13 Kennedy HL, Horan MJ, Sprague MK, Padgett NE, Shriver KK. Ambulatory blood pressure in healthy normotensive males. Am Heart J 1983; 106:717-722.
14 Weber MA, Drayer JIM, Nakamura DK, Wyle FA. The circadian blood pressure pattern in ambulatory normal subjects. Am J Cardiol 1984;
54:115-119.
15 Tseng YZ, Tseng CD, Chiang FT, Hsu KL, Wu TL. The normalcy of blood pressure in well-controlled hypertensive patients. Am J Noninvas Cardiol 1992;
6:95-98.
16 Drayer JIM, Weber MA, DeYoung JL, Wyle FA. Circadian blood pressure patterns in ambulatory hypertensive patients. Am J Med 1982; 73:493-499.
17 Sokolow M, Werdegar D, Kain HK, Hinman AT. Relationship between level of blood pressure measured casually and by portable recorders and severity of complications in essential hypertension. Circulation 1966; 34:279-298.
18 Perloff D, Sokolow M. The representative blood pressure: usefulness of office, basal, home and ambulatory readings. Cardiovasc Med
1978; 3:665-668.
19 White WB, Schulman P, McCabe EJ, Dey HM. Average daily blood pressure, not office blood pressure, determines cardiac function in patients with hypertension. JAMA 1989;
261:873-877.
20 White WB, Dey HM, Schulman P. Assessment of the daily blood pressure load as a determinant of cardiac function in patients with mild-to-moderate hypertension. Am Heart J 1989; 118:782-795.
21 Devereux RB, Pickering TG, Harshfield GA et al. Left ventricular hypertrophy
in patients with hypertension: importance of blood pressure response
to regularly recurring stress.
Circulation 1983; 68:470-476.
22 Drayer JIM, Weber MA, DeYoung JL. BP as a determinant of cardiac left ven-tricular muscle mass. Arch Intern Med
1983; 143: 90-92.
23 Devereux RB. Importance of left ventricular mass as a predictor of cardiovascular morbidity in hypertension. Am J Hypertens 1989;
2:650-654.
24 Alicandri CL, Fariell OR, Boni E. Left ventricular hypertrophy and ambulatory monitoring of blood pressure. J Clin Hypertens 1987; 3:197-202.
25 Heber ME, Brigden GS, Prince H, Lahiri A, Raftery EB. Is there a relationship between ambulatory intra-arterial blood pressure and left ventricular function?
Hypertension 1988; 11:464-469.
26 Pickering TG, Devereux RB. Ambulatory monitoring of blood pressure as a predictor of cardiovascular risk. Am Heart J 1987;
114:925-928.
27 Casale PN, Devereux RB, Milner M et al. Value of echocardiographic measurements of left ventricular mass in predicting cardiovascular morbid events in hypertensive men. Ann Intern Med 1986; 105:173-178.
28 Opsahl JA, Abraham PA, Halsternson CE, Keane WF. Correlation of office and ambulatory blood pressure measurements with urine albumin and N-acetyl-β-D-glucosaminidase
excretions in essential hypertension.
Am J Hypertens 1988; 1:117S-120S.
29 Giaconi S, Levanti C, Fommei E et al.
Microalbuminuria and casual and ambulatory blood pressure monitoring in normoten-sives and in patients with borderline and mild essential hypertension. Am J Hypertens 1989;
2:259-261.
30 Asmar RG, Brunel PC, Pannier BM, Lacolley PJ, Safar ME. Arterial distensibility and ambulatory blood pressure monitoring in essential hypertension. Am J Cardiol 1988;
61:1066-1070.
31 Parati G, Pornidossi G, Albini F, Malaspina D, Mancia G. Relationship of 24-hour blood pressure mean and variability to severity of target organ damage in hypertension. J Hypertens
1987; 5:93-98.
32 Lin JM, Hsu KL, Chiang FT, Tseng CD, Tseng. Influence of isolated diastolic hypertension identified by ambulatory pressure on target organ damage. Int J Cardiol 1995; 48:311-316.
33 Pessina AC, Palatini P, Sperti G. Evaluation of hypertension and related target organ damage by average day-time blood. Clin Exp Hypertens A
1985; 7:267-278.
34 Massabuau P, Fourcade J, Galinier M, Fauvel JM, Bounhoure JP. Ambulatory blood pressure monitoring and left ventricular hypertrophy: correlations and trials of predictive value. Arch des Maladies du Coeur et des Varisseaux 1992; 85:1173-1175.
35 Macia G, Gamba PL, Omboni S, Paleari F, Parati G, Sega R, Zanchetti A. Ambulatory blood pressure monitoring. J Hypertens 1996; 14
(suppl):S61-S66.
36 Sokolow M, Lyon TP. The ventricular complex in left ventricular hypertrophy as obtained by unipolar precordial and limb leads. Am Heart J 1949;
37:161-186.
37 Ungerleider HE, Gubner R. Evaluation of heart size measure-ments. Am Heart J 1942; 24:494-510.
38 Keith NM, Wagener HP, Barker NW. Some different types of essential hypertension: their course and prognosis. Am J Med Sci 1974;
268:336-345.
39 National High Blood Pressure Education Program Working Group Report on Ambulatory Blood Pressure Monitoring. Arch Int Med 1990;
150:2270-2280.
40 White WB. Ambulatory blood pressure and target organ involvement in hypertension. Clin Invest Med 1991;
14:224-230.
41 Kannel WB. Role of blood pressure in cardiovascular morbidity and mortality.
Prog Cardiovasc Dis 1974; 17:5-24.
42 Kobrin I, Messerli FM. Clinical importance of 24-hour recording of blood pressure. Pract Cardiol 1984;
10:117-135.
43 Floras JS, Hassan MO, Sever PS, Jones JV, Osikowska B, Sleight P. Cuff and ambulatory blood pressure in subjects with essential hypertension.
Lancet 1981; 2:107-109.
44 Sokolow M, Perloff D, Cowan R. Contribution of ambulatory blood pressure to the assessment of patients with mild to moderate elevation of office blood pressure. Cardiovasc Rev Rep 1980; 1: 295-303.
45 Tseng YZ, Tseng CD, Lo HM, Chiang FT, Hsu KL. Characteristic abnormal findings of ambulatory blood pressure indicative of hypertensive target organ complications. Eur Heart J 1994;
15:1037-1043.
46 Kobrin I, Oigman W, Kumar A et al.
Diurnal variation of blood pressure in elderly patients with essential hypertension. J Am Geriatr Soc 1984;
32:896-899.
47 Lin LJ, Tseng YZ, Chiang FT, Lee TK, Tseng WP. Altered circadian rhythm of blood pressure in patients with cerebral stroke. Am J Noninvas Cardiol 1992; 6:62-65.
48 Verdecchia P, Schillaci G, Guerrieri M
et al. Circadian blood pressure
changes and left ventricular hypertrophy in essential hypertension.
9
Table 1 The Predictive Values of Blood Pressure Parameters for Left Ventricular Hypertrophy on Electrocardiogram
Sensitivity % Specificity % Positive predictive value % Negative predictive value % CBP SBP > 160 mmHg 26.3 53.3 17.7 65.5 SBP > 140 mmHg 70.0 9.5 22.8 45.5 DBP > 95 mmHg 30.0 41.4 16.3 60.8 DBP > 90 mmHg 62.5 13.3 21.6 48.3 ABP SBP average > 160 mmHg 7.5 98.1 60.0 73.6 SBP average > 140 mmHg 47.5 51.0 27.0 71.8 DBP average > 95 mmHg 25.0 78.6 30.8 73.3 DBP average > 90 mmHg 43.5 49.1 24.7 69.6 SBP load > 35% 43.8 65.2 32.4 75.3 SBP load > 25% 50.0 57.6 31.0 75.2 DBP load > 35% 37.5 63.8 28.3 72.8 DBP load > 25% 47.5 55.2 28.8 73.4 SBP average > casual SBP 23.8 97.6 79.2 77.1 DBP average > casual DBP 31.3 88.6 51.0 77.2 Reversed circadian pattern of SBP 31.3 88.6 51.0 77.2 Reversed circadian pattern of DBP 32.5 87.1 49.1 77.2 Non-dipper of SBP 67.5 51.4 34.6 80.6 Non-dipper of DBP 75.0 33.2 30.0 77.8 Abbreviations:
CBP: casual blood pressure; ABP: ambulatory blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure.
10
Table 2 The Predictive Values of Blood Pressure Parameters for Left Ventricular Hypertrophy on Chest X-ray
Sensitivity % Specificity % Positive predictive value % Negative predictive value % CBP SBP > 160 mmHg 26.9 56.3 11.7 77.9 SBP > 140 mmHg 76.9 23.1 17.9 82.1 DBP > 95 mmHg 32.7 43.7 11.3 74.8 DBP > 90 mmHg 75.0 18.5 16.7 77.2 ABP SBP average > 160 mmHg 13.5 98.3 63.6 83.9 SBP average > 140 mmHg 63.5 53.8 23.1 87.1 DBP average > 95 mmHg 42.3 79.8 31.4 86.4 DBP average > 90 mmHg 63.5 52.9 22.8 86.9 SBP load > 35% 46.2 65.6 22.6 84.8 SBP load > 25% 55.8 58.4 22.7 85.8 DBP load > 35% 46.2 67.2 23.5 85.1 DBP load > 25% 55.8 56.7 22.0 85.4 SBP average > casual SBP 21.2 94.5 45.8 84.6 DBP average > casual DBP 36.5 91.6 48.7 86.9 Reversed circadian pattern of SBP 30.8 86.1 32.7 85.1 Reversed circadian pattern of DBP 28.9 84.0 28.3 84.4 Non-dipper of SBP 71.2 50.8 24.0 89.0 Non-dipper of DBP 75.0 34.0 19.9 86.2 Abbreviations:
CBP: casual blood pressure; ABP: ambulatory blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure.
11
Table 3 The Predictive Values of Blood Pressure Parameters for Proteinuria Sensitivity % Specificity % Positive predictive value % Negative predictive value % CBP SBP > 160 mmHg 46.2 59.1 10 91.8 SBP > 140 mmHg 84.6 12.5 8.7 89.2 DBP > 95 mmHg 53.8 46.6 9.0 91.1 DBP > 90 mmHg 76.9 15.9 8.3 87.5 ABP SBP average > 160 mmHg 11.54 96.6 25.0 91.8 SBP average > 140 mmHg 69.2 51.5 12.3 94.4 DBP average > 95 mmHg 46.2 78.4 17.4 93.7 DBP average > 90 mmHg 69.2 50.0 12.0 94.3 SBP load > 35% 53.9 64.4 13.0 93.4 SBP load > 25% 76.7 57.6 15.2 96.2 DBP load > 35% 57.7 64.4 13.8 93.9 DBP load > 25% 61.5 53.0 11.4 93.3 SBP average > casual SBP 19.2 92.8 20.8 92.1 DBP average > casual DBP 38.5 89.0 25.6 93.6 Reversed circadian pattern of SBP 19.2 83.3 10.2 91.3 Reversed circadian pattern of DBP 26.9 82.6 13.2 92.0 Non-dipper of SBP 53.9 44.7 8.8 90.8 Non-dipper of DBP 73.1 31.8 9.6 92.3 Abbreviations:
CBP: casual blood pressure; ABP: ambulatory blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure.
12
Table 4 The Predictive Values of Blood Pressure Parameters for Retinopathy Sensitivity % Specificity % Positive predictive value % Negative predictive value % CBP SBP > 160 mmHg 41.7 55.8 18.7 82.8 SBP > 140 mmHg 83.3 9.1 15.4 73.3 DBP > 95 mmHg 62.5 45.9 18.6 86.1 DBP > 90 mmHg 87.5 11.0 16.5 82.9 ABP SBP average > 160 mmHg 2.1 96.3 10.0 83.2 SBP average > 140 mmHg 58.3 49.6 18.7 85.7 DBP average > 95 mmHg 31.3 77.3 21.4 85.0 DBP average > 90 mmHg 50.0 46.7 15.7 82.5 SBP load > 35% 37.5 62.8 16.7 83.5 SBP load > 25% 50.0 55.8 18.3 84.9 DBP load > 35% 43.8 62.8 18.9 84.9 DBP load > 25% 58.3 55.4 20.6 87.0 SBP average > casual SBP 16.7 93.4 33.3 85.0 DBP average > casual DBP 27.1 89.3 33.3 86.1 Reversed circadian pattern of SBP 35.4 86.8 34.7 87.1 Reversed circadian pattern of DBP 37.5 85.5 34.0 87.3 Non-dipper of SBP 52.1 46.3 16.1 83.0 Non-dipper of DBP 70.8 32.2 17.2 84.8 Abbreviations:
CBP: casual blood pressure; ABP: ambulatory blood pressure; SBP: systolic blood pressure; DBP: diastolic blood pressure.