Title: Patients withBlepharitis are at Elevated Risk of Anxiety and Depression Short title: Blepharitis, anxiety and depression (Version 2)
Chun-Chi Chiang, MD, PhD1,2; Cheng-Li Lin, MS3; Yi-Yu Tsai, MD, PhD1,2 ;
Chiao-Ling Peng, MS3; Ya-Tang Liao, PhD3, Fung-Chang Sung, PhD, MPH3,4,*
1Department of Ophthalmology, China Medical University Hospital, Taichung 404,
Taiwan
2School of Medicine, China Medical University, Taichung 404, Taiwan
3Management Office for Health Data, China Medical University Hospital, Taichung
404, Taiwan
4Department of Public Health, China Medical University College of Public Health,
Taichung404, Taiwan
Meeting Presentation: None
Funding: This study was supported in part by the Executive Yuan National Sciences Council (grant numbers NSC 100-2621-M-039-001), China Medical University Hospital (grant number 1MS1 and DMR-101-075), and Taiwan Department of Health Clinical Trial and Research Center for Excellence (grant number DOH101-TD-B-111-004) and Cancer Research Center of Excellence (DOH101-TD-C-111-005)
Other financial Support: None
There is no conflicting relationship exists for any author
Reprint requests and Corresponding author
Fung-Chang Sung, PhD, MPH Professor
China Medical University College of Public Health 91 Hsueh Shih Road
Taichung 404, Taiwan Tel: 886-4-2206-2295 Fax: 886-4-2201-9901
N0. words: 221 in the Abstract, 2063 in the Text, 44 references, 3 Tables and 1 Figure.
Abstract
Purpose: Population-based cohort study on the risk of anxiety and depression in patients with blepharitis is limited. This study evaluated whether blepharitis patients are at a higher risk of anxiety and depression.
Design: A retrospective cohort study.
Methods: We used the universal insurance claims data from 1997 to 2010 in Taiwan to identify annually patients with newly diagnosed blepharitis (N=9764) and without the disease (N= 39056). Incidences, rate ratios (IRR) and hazard ratios (HR) of anxiety and depression were measured for both cohorts by baseline demographic characteristics and comorbidities until the end of 2010.
Results. Compared with the non-blepharitis cohort, the blepharitis cohort had higher incidence of anxiety (15.9 vs. 9.5 per 1000 person-years), with an adjusted HR of 1.58 (95% confidence interval (CI) =1.46-1.70). The incidence of depression was also higher in the blepharitis cohort (7.66 vs. 5.05 per 1000 person-years), with an adjusted HR of 1.42 (95% CI =1.28-1.58). The blepharitis cohort to the non-blepharitis cohort IRR decreased from 1.73 in the first quartile to 1.32 in the 4th quartile for anxiety, and
Conclusions. Patients with blepharitis are at elevated risks of anxiety and depression. The risk is higher in earlier period after the diagnosis of blepharitis, and declines by time, but remains significantly higher for those with blepharitis than those without blepharitis.
Introduction
Characterized by inflamed eyelids, blepharitis is a high prevalent ophthalmic complains difficult to cure in eye care practices.1 Crust or flakes on eyelashes, stuck
eyelids, reddish eyelids, and blurred vision are the common signs and symptoms.2 The
onset of blepharitis can be acute, other than the more generally form of long standing chronic inflammation. Staphylococcal infection, seborrheic, and meibomian gland dysfunction (MGD) are major etiological cause of these conditions.3 Patients suffer
discomfort evaporative dry eye disease are mainly associated with MSG because of ocular surface inflammation.2 The ocular surface condition may further exacerbate due
to immune-mediated inflammatory processes. 4 The persistent discomfort eyes, and
unattractive appearance, and uneasy feeling may precipitate psychological stress and negative social implications for patients, including depressed and anxious mood.1
The WHO World Health Survey shows that patients with chronic diseases are more likely to have comorbidity of depression, particularly in patients with angina, arthritis, asthma, and diabetes.5 For patients with blepharitis, in addition to the burden of the
disease and vision disturbance, there are other factors that may contribute to the risk of psychologic condition. The drugs used to treat inflammatory diseases, such as
behavioral changes.6 There are also evidences that cytokines are able to cross the
blood-brain barrier linking with behavioral changes in patients with chronic inflammation.7,8 A combination of these factors may place patients with ocular
inflammatory diseases at an elevated risk for mood dysfunction.
Because of uncomfortable and distressing conditions, we hypothesized that patients with blepharitis would be at an increased risk of mental illness including major depression and anxiety. No large study has ever evaluated the association using prospective design. This study conducted a retrospective follow-up observation to estimate the risk of depression and anxiety in patients with blepharitis using a nationwide insurance dataset in Taiwan.
METHODS AND MATERIALS
Study design and data source
We obtained a representative claims data of one million insured people in the National Health Insurance Research Database (NHIRD). This universal health insurance program has covered nearly 99% of the 23.74 million residents and contracted with 97% of the hospitals and clinics for comprehensive health care in Taiwan.9 In this study, patients with blepharitis were identified from the NHIRD
inpatient and outpatient expenditure claims data files from 1997 until the end of 2010. These files contained the information on demographic status (birth date and sex) of insured population and services provided, and reimbursements for the services. The diagnoses of diseases used the International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM). For the confidentiality, patient identifications were scrambled according to the Department of Health regulations to strengthen data security and protect patient’s privacy. This study was exempted from full ethical review (IRB permit number: CMU-102-106).
Study subjects and comorbidities
Patients who had made at least three outpatient visits with diagnoses of blepharitis (ICD-9-CM code 373.0) were eligible for the study and identified annually from 1997 to 2010 for the blepharitis cohort. The first diagnosis date was defined as index date for estimating the follow-up time. For each blepharitis patients, 4 persons free from the disease were identified from the rest of claims data for the non-blepharitis cohort, with age, sex and index year frequency matched. Patients with the history of
depression (ICD-9-CM: 300.00, 296.2, 296.3, 300.4 and 311) or anxiety (ICD-9-CM: 300.00) before the index date or with missing information on age or sex were
CM codes 401 to 405, A260, A269), diabetes (ICD-9-CM codes 250, A181), hyperlipidemia (ICD-9-CM codes 272, A182), coronary artery disease (ICD-9-CM codes 410 to 414, A270, A279) and stroke (ICD-9-CM codes 430 to 438, A290 to A299).
Statistical analysis
Chi-square test was used to examine the distributions of baseline demographic characteristics and comorbidities between blepharitis and non-blepharitis cohorts. Follow-up person-years were estimated for all subjects in both cohorts until depression or anxiety identified, or censored because of loss to follow-up or
withdrawn from the insurance, or the end of 2010. Incidence rates of depression and anxiety were estimated by demographic status and comorbidities. The blepharitis cohort to the non-blepharitis cohort incidence rate ratio (IRR) and 95 % confidence interval (CI) were calculated using Poisson regression analysis. Cox proportional hazards regression analysis was also used to measure the hazard ratios (HR) and 95% confidence intervals (CI) of depression and anxiety associated with blepharitis, adjusting for covariates. We also depicted the blepharitis cohort to the non-blepharitis cohort IRR of depression and anxiety by follow-up years in quartiles. A p value of less than 0.05 was considered to be statistically significant. All analyses were
performed using the SAS statistical package for Windows, version 9.2 (SAS institute, Inc., Cary, NC, USA).
RESULTS
This study identified 9764 persons for the blepharitis cohort and 39056 persons for the non-blepharitis cohort. Both cohorts were similar in age and sex distributions with a mean age of 54.9±18 years and near 60% of subjects were women (Table 1). Compared with the non-blepharitis cohort, patients in the blepharitis cohort were more prevalent with hypertension, diabetes mellitus, hyperlipidemia, stroke and coronary artery disease.
The incidence rate of anxiety was 1.67-fold higher in the blepharitis cohort than in the non-blepharitis cohort (15.9 vs. 9.5 per 1000 person-years), with an adjusted HRs of 1.58 (95% CI =1.46-1.70) (Table 2). So was the incidence of depression 1.52-fold higher in the blepharitis cohort (7.66 vs. 5.05 per 1000 person-years), with an adjusted HRs of 1.42 (95% CI =1.28-1.58). The incidence rates of both anxiety and depression were higher in women than in men, and increased with age in both cohorts. The gender and age differences in the incidence rates of anxiety were greater than that of depression. However, the age-specific blepharitis cohort to non-blepharitis cohort IRR of anxiety were higher in those in less 40 years of age, with an adjusted HR of 1.97
(95% CI = 1.59–2.43). The adjusted HR reduced to 1.56 (95% CI 1.39, 1.75) for the elderly.
The comorbidity specific analysis in the multivariable Cox proportional hazards regression model showed consistently higher incidence rates of anxiety and
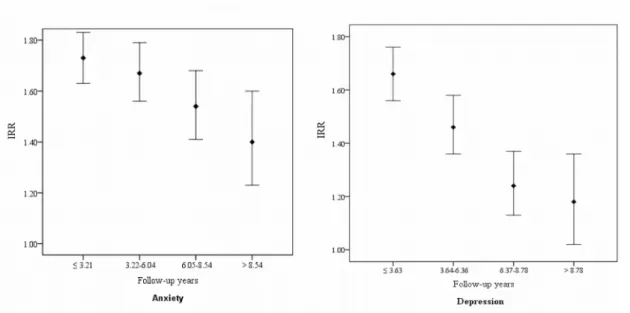
depression in the blepharitis cohort than in the non-blepharitis cohort (Table 3). The incidence increased further in blepharitis patients with comorbidity, particularly in those had a stroke. Figure 1 shows that the blepharitis cohort to the non-blepharitis cohort IRR for both anxiety and depression declined by follow-up time, from 1.73 in the first quartile to 1.40 in the 4th quartile for anxiety, and from 1.67 to 1.18 for
depression.
Discussion
Blepharitis is a common ocular disease that has been associated with many systemic medical conditions. In an age and gender matched retrospective case-control study (n = 16706 each group), Nemet et al found that patients with blepharitis are prevalent with not only psychologic conditions, but also systemic conditions and other eye conditons.10 A survey conducted in the US showed that approximately 37% of
patients seen by ophthalmologists and 47% of patients seen by optometrists have complains of blepharitis.2 Both the ophthalmologic disorder and the associated mood
dysfunction are important factors affecting the quality of life of patients. In this study, we found that patients with blepharitis had a 67% higher risk of anxiety and 52% higher risk of depression in the 9-year follow-up period. The risk of anxiety shown in our cohort analysis is consistent with the odds ratio of 1.6 (95% CI 1.4-1.9) found by Nemet et al.10.
The occurrence of blepharitis and subsequent psychologic conditions have been associated with psychoneuroimmunology and inflammation.7,8,11-17 Patients with
blepharitis are at higher risk to have other medical conditions, which may also associate the psychologic consequence.10 Recent studies have shown that chronic
inflammatory and cytokines dysregulation are significant factors relate to the pathophysiology of depression and anxiety.18,19 Levels of circulating cytokines
interleukin (IL)-1beta, IL-6, interferon gamma, and TNF-alpha are higher in
depressed patients than in controls.20 Patients with cardinal inflammation accompany
with depression have elevated inflammatory cytokines and their soluble receptors presenting in peripheral blood and cerebrospinal fluid.21,22 Concentrations of acute
phase proteins, chemokines, adhesion molecules, and inflammatory prostaglandins are also increased in peripheral blood.Eyelids are rich with blood supply. A murine model has also demonstrated that the concentration of inflammatory cytokines in tear is elevated in response to evaporative dry eye stress,which usually results from
blepharitis.23 Therefore, both psychologic disorder and blepharitis may be affected by
the inflammatory reactions.
Previous studies have found that women are up to 3 times more likely to experience depressive disorders than men, including depression, anxiety, and co-existing
depression and anxiety.24-30 Our results also revealed that the incidence rates of both
anxiety and depression were higher in women than in men, which is consistent with previous reports. However, the sex-specific blepharitis cohort to non-blepharitis cohort IRR shows that relative risks of both anxiety and depression are higher for men than for women. We hypothesize the sex hormone may play a role in the gender difference. Increasing evidences have shown that gene expression of the meibomiam glands, dry eye syndrome, MGD, and evaporative dry eyes are associated with sex steroids.31–39 The incidence of anxiety increased markedly with age in our study. The
hormonal therapy in postmenopausal women may have an important role leading to blepharitis and mood dysfunction.32,34,35,38
Previous clinical and community-based studies have suggested that the prevalence of depression, anxiety, and comorbid disorder decline with age.40-42 Different study
designs may attribute to the discrepancy between our finding and results from other studies. There are sufficient medical resources and facilities with convenient access to care for insured people in Taiwan. The elderly patients are easily to get the medical
attention. This may explain why the incidence rates of depression and anxiety are higher in older people in this study. Compare with non-blepharitis patients, patients with blepharitis suffer from chronic ocular discomfortable and blurred vision, which affect the quality of life, especially for older people. Hence, these patients have higher tendency to develop depression and anxiety. Nevertheless, the age-specific relative risk of anxiety was some what higher for those aged 20-39 years than the elderly in the blepharitis cohort (IRRs: 1.99 vs. 1.65). The young group is the main working force; the blepharitis symptoms such as ocular discomfortable and physical
appearance may affect their work performances and social activities, which induce higher anxiety than their peers without blepharitis.
In addition, compared with non-blepharitis cohort, patients in the blepharitis cohort were also more prevalent with hypertension, diabetes mellitus, hyperlipidemia, stroke and coronary artery disease. Studies have demonstrated a clear relationship between inflammation and the development of cardiovascular disease, diabetes, and cancer.43,44
Nemet et al also found some major cardiovascular conditions (carotid artery disease, hyperlipidemia, and hypertension) to be associated with blepharitis.10 Our results are
also consistent with their report.
There are few limitations in our study. First, we used International Classification of Diseases codes to identified diagnoses of blepharitis, depression, anxiety and other
medical conditions. People with mild symptoms may not go to the doctor resulting undiagnosed cases. Patients with blepharitis might have more clinic visits than those without blepharitis. We conducted a further data analysis and found that the average number of clinic visit was higher in blepharitis patients than in the comparisons [32.3 (SD 24.4) vs. 20.0 (SD 18.1)]. Therefore, blepharitis patients are more likely to be diagnosed and to get treatment for depression and anxiety. Second, although there may be a small number of patients with undetected blepharitis would be categorized as non-blepharitis and would have a small chance of being selected as part of the comparison cohort. The sample size of each cohort was large enough to compromise the bias. However, the results need to be interpreted with caution.
Blepharitis is characterized by discomfort eyes and unattractive appearance, which may cause uneasy feeling and negative social implications for the patients. The present study shows patients with blepharitis are at higher risk of anxiety or depression. Our findings are of clinical importance given the high prevalence of blepharitis in the general population, and the fact that depression and anxiety are disorders readily treatable and often under diagnosed because its symptoms are frequently overlooked.
Acknowledgement
This study was supported in part by the Executive Yuan National Sciences Council (grant numbers NSC 100-2621-M-039-001), China Medical University Hospital (grant number 1MS1 and DMR-101-075), and Taiwan Department of Health Clinical Trial and Research Center for Excellence (grant number DOH101-TD-B-111-004) and Cancer Research Center of Excellence (DOH101-TD-C-111-005).
References
1. McDonald MB. The patient’s experience of blepharitis. Ocul Surf 2009; 7(suppl):S17– 8.
2. Lemp MA, Nichols KK. Blepharitis in the United States 2009: a survey-based perspective on prevalence and treatment. Ocul Surf 2009;7(suppl):S1–14. 3. AAO 2008 American Academy of Ophthalmology Retina Panel. Preferred
Practice Pattern® Guidelines. Blepharitis. San Francisco, CA: American Academy of Ophthalmology; 2008. http://www.aao.org/ppp (accessed 3 April 2012).
4. Pflugfelder SC, Solomon A, Stern ME. The diagnosis and management of dry eye: a twenty-five-year review. Cornea 2000;19:644–649.
5. Moussavi S, Chatterji S, Verdes E, Tandon A, Patel V, Ustun B: Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet 2007;370:851– 858.
6. Warrington TP, Bostwick JM. Psychiatric adverse effects of corticosteroids. Mayo Clin Proc 2006;81:1361–1367.
7. Dantzer R, O’Connor JC, Freund GG, Johnson RW, Kelley KW. From inflammation to sickness and depression: when the immune system subjugates the brain. Nat Rev Neurosci 2008;9:46 –56.
8. Miller AH. Norman Cousins Lecture. Mechanisms of cytokine-induced behavioral changes: psychoneuroimmunology at the translational interface. Brain Behav Immun. 2009;23:149-58
9. Cheng TM. Taiwan’s national health insurance system: High value for the dollar. In: Okma KGH, Crivelli L, eds. Six Countries, Six Reform Models: The Healthcare Reform, Experience of Israel, the Netherlands, New Zealand, Singapore, Switzerland and Taiwan. Hackensack, New Jersey: World
Scientific. 2009;171-204.
10. Nemet AY, Vinker S, Kaiserman I. Associated morbidity of blepharitis. Ophthalmology. 2011;118:1062-8.
11. Foulks GN. The correlation between the tear film lipid layer and dry eye disease. Surv Ophthalmol. 2007;52:369–374.
12. McCulley JP, Dougherty JM, Deneau DG. Classification of chronic blepharitis. Ophthalmology. 1982;89:1173–1180.
13. Foulks GN, Bron AJ. A clinical description of meibomian gland dysfunction. Ocul Surf. 2003;1:107–126.
14. Solomon A, Dursun D, Liu Z. Pro- and anti-inflammatory forms of
interleukin-1 in the tear fluid and conjunctiva of patients with dry-eye disease. Invest Ophthalmol Vis Sci. 2001;42:2282–2292.
15. Korb DR, Scaffidi RC, Greiner JV, et al. The effect of two novel lubricant eye drops on tear film lipid layer thickness in subjects with dry eye symptoms. Optom Vis Sci. 2005;82:594–601.
16. Pisella PJ, Brignole F, Debbasch C. Flow cytometric analysis of conjunctival epithelium in ocular rosacea and keratoconjunctivitis sicca. Ophthalmology. 2000;107:1841–1849.
17. Rubin M, Rao SN. Efficacy of topical cyclosporin 0.05% in the treatment of posterior blepharitis. J Occul Phamacol Ther. 2006;22:47–53.
18. Vogelzangs N, Duivis HE, Beekman AT, Kluft C, Neuteboom J, Hoogendijk W, Smit JH, de Jonge P, Penninx BW. Association of depressive disorders, depression characteristics and antidepressant medication with inflammation. Transl Psychiatry. 2012; 2: e79.
19. Salim S, Chugh G, Asghar M. Inflammation in anxiety. Adv Protein Chem Struct Biol. 2012;88:1-25.
20. Anisman H, Merali Z, Hayley S. Neurotransmitter, peptide and cytokine processes in relation to depressive disorder: Comorbidity between depression and neurodegenerative disorders. Prog Neurobiol 2008; 85:1–74.
21. Raison CL, Capuron L, Miller AH: Cytokines sing the blues: Inflammation and the pathogenesis of major depression. Trend Immunol 2006; 27:24 –31. 22. Zorilla EP, Luborsky L, McKay JR, Roesnthal R, Houldin A, Tax A, et al. The
relationship of depression and stressors to immunological assays: A meta-analytic review. Brain Behav Immun 2001; 15:199 –226.
23. Lam H, Bleiden L, De Paiva CS, et al. Tear cytokine profiles in dysfunctional tear syndrome. Am J Ophthalmol. 2009;147:198–205.e1.
24. Kessler R. The epidemiology of depression among women. In: Keys C, Goodman S, editors. Women and Depression: A Handbook of the Social, Behavioral, and Biomedical Sciences. New York: Cambridge University Press; 2006. 22–37.
25. Weissman M, Bland R, Canino G, Faravelli C, Greenwald S, et al. Cross-national epidemiology of major depression and bipolar disorder. JAMA. 1996;276:293–299.
26. Palanza P. Animal models of anxiety and depression: how are females different? Neurosci Biobehav Rev. 2001;25:219-33. Review
27. Kuehner C. Gender differences in unipolar depression: an update of epidemiological findings and possible explanations. Acta Psychiatr Scand. 2003;108:163–174.
28. Pigott TA. Gender differences in the epidemiology and treatment of anxiety disorders. J Clin Psychiatry. 1999;60 (Suppl 18):4–15.
29. Cohen CI, Magai C, Yaffee R, Walcott-Brown L. The prevalence of anxiety and associated factors in a multiracial sample of older adults. Psychiatr Serv. 2006;57:1719-25.
30. Mehta KM, Simonsick EM, Penninx BW, Schulz R, Rubin SM, Satterfield S, Yaffe K. Prevalence and correlates of anxiety symptoms in well- functioning older adults: findings from the health aging and body composition study. J Am Geriatr Soc. 2003;51:499-504.
31. Sullivan BD, Evans JE, Cermak JM, et al. Complete androgen insensitivity syndrome: effect on human meibomian gland secretions. Arch Ophthalmol 2002;120:1689 –99.
32. Sullivan BD, Evans JE, Dana MR, Sullivan DA. Impact of androgen deficiency on the lipid profiles in human meibomian gland secretions. Adv Exp Med Biol 2002;506:449 –58.
33. Sullivan BD, Evans JE, Krenzer KL, et al. Impact of antiandrogen treatment on the fatty acid profile of neutral lipids in human meibomian gland
secretions. J Clin Endocrinol Metab 2000;85:4866 –73.
34. Sullivan DA, Jensen RV, Suzuki T, Richards SM. Do sex steroids exert sex-specific and/or opposite effects on gene expression in lacrimal and meibomian
glands? Mol Vis 2009;15:1553–72.
35. Sullivan DA, Krenzer KL, Sullivan BD, et al. Does androgen insufficiency cause lacrimal gland inflammation and aqueous tear deficiency? Invest Ophthalmol Vis Sci 1999;40:1261–5.
36. Sullivan DA, Rocha EM, Ullman MD, et al. Androgen regulation of the meibomian gland. Adv Exp Med Biol 1998;438: 327–31.
37. Sullivan DA, Sullivan BD, Evans JE, et al. Androgen deficiency, meibomian gland dysfunction, and evaporative dry eye. Ann N Y Acad Sci
2002;966:211–22.
38. Sullivan DA, Sullivan BD, Ullman MD, et al. Androgen influence on the meibomian gland. Invest Ophthalmol Vis Sci 2000;41:3732– 42.
39. Sullivan DA, Yamagami H, Liu M, et al. Sex steroids, the meibomian gland and evaporative dry eye. Adv Exp Med Biol 2002;506:389 –99.
40. Jeste DV, Blazer DG, First M. Aging-related diagnostic variations: need for diagnostic criteria appropriate for elderly psychiatric patients. Biol Psychiatry. 2005;58:265–271.
41. Hybels CF, Blazer DG. Epidemiology of late-life mental disorders. Clin Geriatr Med. 2003;19:663–696.
42. Henderson AS, Jorm AF, Korten AE, Jacomb P, Christensen H, Rodgers B. Symptoms of depression and anxiety during adult life: evidence for a decline in prevalence with age. Psychol Med. 1998;28: 1321–1328.
43. Aggarwal BB, Shishodia S, Sandur SK, Pandey MK, Sethi G. Inflammation and cancer: How hot is the link? Biochem Pharmacol 2006; 72:1605–1621. 44. Ridker PM . Inflammatory biomarkers and risks of myocardial infarction,
stroke, diabetes, and total mortality: Implications for longevity. Nutr Rev 2007; 65:S253–259.
Figure Legend
Figure 1. Blepharitis cohort to non-blepharitis cohort incidence rate ratio of anxiety and depression by quartile of follow-up years
Table 1 Demographic characteristics and comorbidities in blepharitis cohort and non-blepharitis cohort
Variable Blepharitis p-value& No Yes N = 39056 N = 9764 Sex n(%) n(%) Female 23756(60.8) 53939(60.8) 0.99 Male 15300(39.2) 3825(39.2) Age, years Mean±SD 54.9±18.0 54.8±18.0 0.68 20-39 9320(23.9) 2331(23.9) 0.70 40-64 15009(38.4) 3711(38.0) 65+ 14727(37.7) 3722(38.1) Comorbidity Diabetes 5512(14.1) 1721(17.6) <0.0001 Hypertension 12936(33.1) 3658(37.5) <0.0001 Hyperlipidemia 6892(17.7) 2349(24.1) <0.0001 Coronary artery disease 6165(15.8) 2028(20.8) <0.0001
Stroke 4251(10.9) 1288(13.2) <0.0001
Table 2 Incidence rates by sex, age and cohort, and blepharitis cohort to non-blepharitis cohort rate ratios and Cox model measured hazard ratios
Blepharitis
No Yes
Variables Event PY Rate# Event PY Rate# IRR*(95% CI) Adjusted HR † (95% CI) Anxiety 2208 232509 9.50 932 58652 15.9 1.67(1.59, 1.76)** 1.58(1.46, 1.70)** Sex Female 1575 143637 11.0 638 35934 17.7 1.62(1.51, 1.73)** 1.53(1.40, 1.68)** Male 633 88871 7.12 294 22718 12.9 1.82(1.67, 1.98)** 1.68(1.46, 1.93)** Stratify age 20-39 262 59831 4.38 131 15062 8.70 1.99(1.78, 2.22)** 1.97(1.59, 2.43)** 40-64 1003 95058 10.5 394 23232 17.0 1.61(1.48, 1.75)** 1.50(1.33, 1.68)** 65+ 943 77620 12.1 407 20358 20.0 1.65(1.51, 1.79)** 1.56(1.39, 1.75)** Depression 1199 237529 5.05 468 61066 7.66 1.52(1.43, 1.61)** 1.42(1.28, 1.58)** Sex Female 832 147335 5.65 297 37696 7.88 1.43(1.33, 1.53)** 1.32(1.16, 1.51)** Male 367 90194 4.07 171 23371 7.32 1.82(1.68, 1.98)** 1.63(1.36, 1.96)** Stratify age 20-39 214 59993 3.57 79 15318 5.16 1.47(1.31, 1.64)** 1.44(1.11, 1.87)** 40-64 500 97717 5.12 180 24318 7.40 1.47(1.35, 1.61)** 1.36(1.15, 1.62)** 65+ 485 79818 6.08 209 21430 9.75 1.64(1.51, 1.78)** 1.48(1.26, 1.74)**
PY, person-years;Rate#, incidence per 1,000 person-years; IRR*, incidence rate ratio
Adjusted HR†: adjusted for age, sex, diabetes, hyperlipidemia, hypertension, coronary
artery disease and stroke *p<0.05, **p<0.01
Table 3. Incidence of depression and anxiety, blepharitis cohort to non-blepharitis cohort rate ratio and Cox model measured hazards ratio by comorbidity
Blepharitis
No Yes
Event PY Rate† Event PY Rate† IRR*(95% CI) Adjusted HR † (95% CI) Anxiety Comorbidity No 857 141785 6.04 332 31190 10.64 1.76(1.63, 1.90)** 1.76(1.55, 1.99)** Yes 1351 90724 14.89 600 27462 21.85 1.47(1.36, 1.58)** 1.45(1.32, 1.60)** Diabetes No 1832 204332 8.97 746 49355 15.11 1.69(1.59, 1.79)** 1.59(1.46, 1.73)** Yes 376 28176 13.34 186 9297 20.01 1.50(1.32, 1.71)** 1.48(1.24, 1.76)** Hypertension No 1153 163805 7.04 488 38450 12.69 1.80(1.69, 1.93)** 1.70(1.53, 1.89)** Yes 1055 68703 15.36 444 20203 21.98 1.43(1.31, 1.56)** 1.42(1.27, 1.58)** Hyperlipidemia No 1624 196174 8.28 636 45767 13.90 1.68(1.58, 1.78)** 1.63(1.49, 1.79)** Yes 584 36335 16.07 296 12886 22.97 1.43(1.28, 1.60)** 1.44(1.26, 1.66)** Coronary artery disease No 1624 201095 8.08 657 47786 13.75 1.70(1.61, 1.81)** 1.66(1.52, 1.82)** Yes 584 31413 18.59 275 10867 25.31 1.36(1.21, 1.53)** 1.37(1.18, 1.58)** Stroke No 1861 212124 8.77 752 51842 14.51 1.65(1.56, 1.75)** 1.58(1.45, 1.72)** Yes 347 20385 17.02 180 6810 26.43 1.55(1.34, 1.79)** 1.54(1.29, 1.85)** Depression Comorbidity No 523 143223 3.65 170 31998 5.31 1.45(1.34, 1.58)** 1.45(1.22, 1.72)** Yes 676 94306 7.17 298 29069 10.25 1.43(1.32, 1.55)** 1.39(1.22, 1.60)** Diabetes No 992 208513 4.76 364 51376 7.09 1.49(1.40, 1.59)** 1.41(1.25, 1.59)**
Yes 207 29016 7.13 104 9691 10.73 1.50(1.31, 1.73)** 1.46(1.15, 1.85)** Hypertension No 668 166162 4.02 241 39710 6.07 1.51(1.40, 1.63)** 1.45(1.25, 1.68)** Yes 531 71367 7.44 227 21356 10.63 1.43(1.30, 1.57)** 1.38(1.18, 1.62)** Hyperlipidemia No 915 199653 4.58 319 47360 6.74 1.47(1.38, 1.57)** 1.41(1.24, 1.60)** Yes 284 37876 7.50 149 13706 10.87 1.45(1.28, 1.64)** 1.45(1.19, 1.77)** Coronary artery disease No 894 204529 4.37 326 49435 6.59 1.51(1.41, 1.61)** 1.47(1.29, 1.67)** Yes 305 33000 9.24 142 11632 12.21 1.32(1.16, 1.50)** 1.31(1.07, 1.60)** Stroke No 993 216354 4.59 349 53930 6.47 1.41(1.32, 1.50)** 1.37(1.20, 1.53)** Yes 206 21175 9.73 119 7136 16.68 1.71(1.48, 1.99)** 1.68(1.34, 2.11)**
Rate#, incidence rate, per 1,000 person-years; IRR*, incidence rate ratio
Adjusted HR† : adjusted for age, sex, diabetes, hyperlipidemia, hypertension, coronary
artery disease and stroke *p<0.05, **p<0.01