Date: January 26, 2013
Type of manuscript:Letter to the editor
Manuscript title: No association between gout and Alzheimer’s disease: results of a case control study in older people in Taiwan
Running head:gout and Alzheimer’s disease Authors' full names:
SHIH-WEI LAI1,2; CHENG-LI LIN3,4; KUAN-FU LIAO5,6,7*
1School of Medicine, 3Department of Public Health, and 5Graduate Institute of
Integrated Medicine, China Medical University, Taichung, Taiwan
2Department of Family Medicine, and 4Management Office for Health Data,
China Medical University Hospital, Taichung, Taiwan
6Department of Internal Medicine, Taichung Tzu Chi General Hospital,
Taichung, Taiwan
7Department of Health Care Administration, Central Taiwan University of
Science and Technology, Taichung, Taiwan
*Corresponding author: KUAN-FU LIAO
Department of Internal Medicine, Taichung Tzu Chi General Hospital, No.66, Sec. 1, Fongsing Road, Tanzi District, Taichung City, 427, Taiwan
Phone: 886-4-2205-2121 Fax: 886-4-2203-3986
E-mail: [email protected]
Dear Editor,
The evidence shows that uric acid has a free-radical scavenging capacity and possesses an antioxidant effect that may reduce oxidative stress in vivo. Because oxidative stress is found to be involved in Alzheimer’s disease , it is a plausible hypothesis that there may be an potential link between gout and Alzheimer’s disease. In order to elucidate this issue, we conducted a case-control study to examine whether there is an association between gout and the risk of Alzheimer’s disease in older people in Taiwan.
This case-control study utilized a database from the National Health Insurance
program in Taiwan. The insurance program details can be cited in the previous study. There were 989 subjects aged 65 years old or above with newly diagnosed
Alzheimer's disease in 2000-2010 as the case group (451 men, mean age 75.9 years and standard deviation 4.9 years, and 538 women, mean age 75.8 years and standard deviation 5.0 years, respectively), according to International Classification of
Diseases 9th Revision Clinical Modification (ICD-9 codes 331.0). The index date for
each case was defined as the date of diagnosing Alzheimer's disease. We randomly selected 3956 subjects aged 65 years or older from those without Alzheimer's disease as the control group (1804 men, mean age 75.1 years and standard deviation 5.3 years, and 2152 women, mean age 74.8 years and standard deviation 5.3 years,
respectively). The case and control groups were matched with gender, age (every 5-year span) and index date. Individuals with other dementia (ICD-9 codes 290.0,
290.1, 290.2, 290.3, 290.4 and 294.1), other major psychiatric diseases (ICD-9 codes 291-293 and 295-298), or mental retardation (ICD-9 codes 317–319) were excluded from this study.
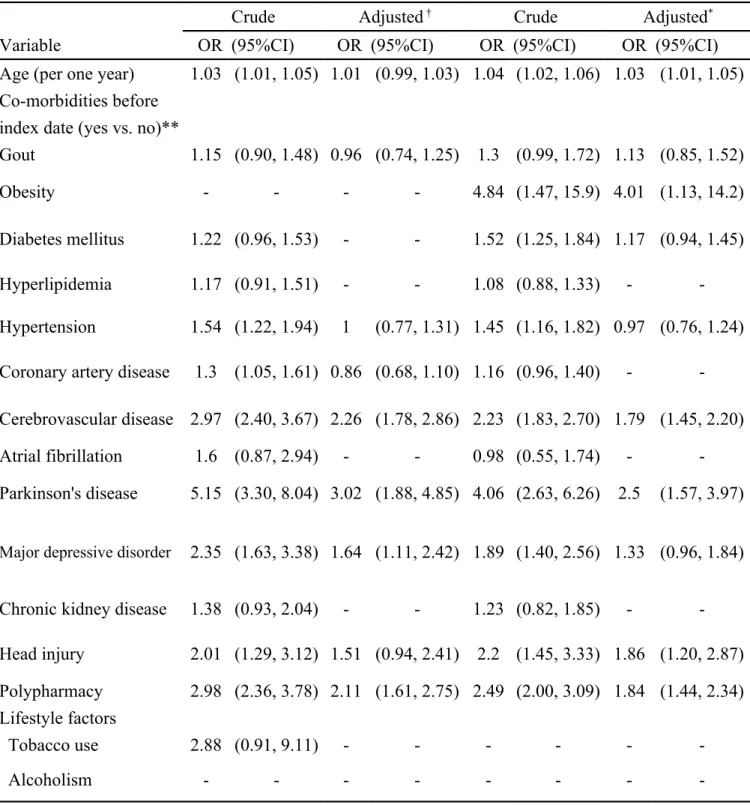
In men, there were 104 subjects with gout among Alzheimer's disease cases (23.1%) and 373 subjects with gout among control subjects (20.7%) (P = 0.27). In women, there were 75 subjects with gout among Alzheimer's disease cases (13.9%) and 238 subjects with gout among control subjects (11.1%) (P = 0.06). After controlling for the covariates, multivariate logistic regression analysis showed that no association was detected between gout and Alzheimer's disease in both gender (OR 0.96, 95% CI 0.74-1.25 and OR 1.13, 95% CI 0.85-1.52, respectively)(Table 1). As a reference of non-gout group, the sub-analysis displayed that the ORs of Alzheimer's disease were 1.07 (95% CI 0.77-1.47) in male gouty subjects without using urate-lowering drugs and 0.82 (95% CI 0.55-1.21) in male gouty subjects s with using urate-lowering drugs. The ORs of Alzheimer's disease were 1.24 (95% CI 0.87-1.76) in female gouty subjects without using urate-lowering drugs and 0.98 (95% CI 0.62-1.56) in female gouty subjects with using urate-lowering drugs (Table not shown).
A cross-sectional study by Ruggiero et al in Italy , patients with dementia had higher level of uric acid (P = 0.001). Another case-control study by Cascalheira et al in Portugal , higher level of uric acid was associated with Alzheimer’s disease (OR 2.42,
P < 0.02). Both studies have conveyed the message that high level of uric acid may
increase the risk of Alzheimer’s disease. In this present study, we found that no association is detected between gout and Alzheimer's disease in both gender, whether
gouty patients had ever used urate-lowering drugs or not. Because conflicting results exist, further studies are required to confirm the association between gout and Alzheimer’s disease.
Some limitations should be addressed. First, because of the nature of this database, no data of uric acid could be used. Therefore, the uric acid level can not be linked with Alzheimer’s disease in this present study. This indicates a study direction in the future for measuring uric acid when diagnosing Alzheimer’s disease. Second, we did not know what criteria were used to diagnose Alzheimer’s disease. Thus, we could not clarify the stage of Alzheimer’s disease in each patient.
Funding
This study was supported in part by Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH102-TD-B-111-004).The funding agency did not influence the study design, data collection and analysis, decision to publish, or
preparation of the manuscript.
Conflict of Interest None declared.
References
Cascalheira JF, Joao SS, Pinhancos SS, et al. 2009. Serum homocysteine: interplay with other circulating and genetic factors in association to Alzheimer's type dementia. Clin Biochem 42: 783-790.
Lai SW, Lin CH, Liao KF, et al. 2012. Association between polypharmacy and dementia in older people: A population-based case-control study in Taiwan.
Geriatr Gerontol Int 12: 491-498.
Ruggiero C, Cherubini A, Lauretani F, et al. 2009. Uric acid and dementia in community-dwelling older persons. Dement Geriatr Cogn Disord 27: 382-389.
Sultana R, Butterfield D. 2010. Role of oxidative stress in the progression of Alzheimer's disease. J Alzheimers Dis 19: 341-353.
Waring WS, Convery A, MishraV, et al. 2003. Uric acid reduces exercise-induced oxidative stress in healthy adults. Clin Sci (Lond) 105: 425-430.
Table 1 Odds ratios and 95% confidence intervals of Alzheimer's disease associated with gout and other co-morbidities
Men Women
Crude Adjusted † Crude Adjusted*
Variable OR (95%CI) OR (95%CI) OR (95%CI) OR (95%CI)
Age (per one year) 1.03 (1.01, 1.05) 1.01 (0.99, 1.03) 1.04 (1.02, 1.06) 1.03 (1.01, 1.05) Co-morbidities before
index date (yes vs. no)**
Gout 1.15 (0.90, 1.48) 0.96 (0.74, 1.25) 1.3 (0.99, 1.72) 1.13 (0.85, 1.52)
Obesity - - - - 4.84 (1.47, 15.9) 4.01 (1.13, 14.2)
Diabetes mellitus 1.22 (0.96, 1.53) - - 1.52 (1.25, 1.84) 1.17 (0.94, 1.45)
Hyperlipidemia 1.17 (0.91, 1.51) - - 1.08 (0.88, 1.33) -
-Hypertension 1.54 (1.22, 1.94) 1 (0.77, 1.31) 1.45 (1.16, 1.82) 0.97 (0.76, 1.24) Coronary artery disease 1.3 (1.05, 1.61) 0.86 (0.68, 1.10) 1.16 (0.96, 1.40) - -Cerebrovascular disease 2.97 (2.40, 3.67) 2.26 (1.78, 2.86) 2.23 (1.83, 2.70) 1.79 (1.45, 2.20)
Atrial fibrillation 1.6 (0.87, 2.94) - - 0.98 (0.55, 1.74) -
-Parkinson's disease 5.15 (3.30, 8.04) 3.02 (1.88, 4.85) 4.06 (2.63, 6.26) 2.5 (1.57, 3.97)
Major depressive disorder 2.35 (1.63, 3.38) 1.64 (1.11, 2.42) 1.89 (1.40, 2.56) 1.33 (0.96, 1.84)
Chronic kidney disease 1.38 (0.93, 2.04) - - 1.23 (0.82, 1.85) -
-Head injury 2.01 (1.29, 3.12) 1.51 (0.94, 2.41) 2.2 (1.45, 3.33) 1.86 (1.20, 2.87) Polypharmacy 2.98 (2.36, 3.78) 2.11 (1.61, 2.75) 2.49 (2.00, 3.09) 1.84 (1.44, 2.34) Lifestyle factors
Tobacco use 2.88 (0.91, 9.11) - - -
-Alcoholism - - -
-** Co-morbidities included before index date were as follows: gout (including gouty attack (ICD-9 codes 274) and hyperuricemia (ICD-9 codes 790.61)), obesity (ICD-9 codes 278.00 and 278.01), diabetes mellitus (ICD-9 codes 250), hyperlipidemia (ICD-9 codes 272.0, 272.1, 272.2, 272.3 and 272.4), hypertension (ICD-9 codes 401-405), coronary artery
Parkinson's disease (ICD-9 codes 332), major depressive disorder (ICD-9 codes 296.2, 296.3, 300.4 and 311), chronic kidney disease 9 codes 585, 586, 588.8 and 588.9), head injury 9 codes 850-854 and 959.01), tobacco use (ICD-9 codes 305.1) and alcoholism (ICD-(ICD-9 codes 303, 305.00, 305.01, 305.02, 305.03 and V11.3). Polypharmacy was defined as the daily average use of 5 or more drugs. The subject number of alcoholism in both gender, the subject number of obesity in men, and the subject number of tobacco use in women were too small to reach statistic significance.
†Adjusted OR in men: adjusted for age, hypertension, hypertension, coronary artery disease, cerebrovascular disease, Parkinson's disease, major depressive disorder, head injury and polypharmacy
*Adjusted OR in women: adjusted for age, obesity, diabetes mellitus, hypertension, cerebrovascular disease, Parkinson's disease, major depressive disorder, head injury and polypharmacy