前十字韌帶損傷患者之動態功能表現變化; Changes of Dynamic Functional Performance in Patients with Anterior Cruciate Ligament Injury
95
0
0
全文
(2) 中 文 摘 要. 前十字韌帶是膝關節中最常受傷害的組織之ㄧ,前十字韌帶的缺損會造成膝 關節結構上與功能上的不穩定。因此膝關節鬆弛度檢測與功能性表現是兩個最常 用於評估十字韌帶損傷病人復健進度與預後狀態的方式。過去文獻中,很少針對 功能性損傷做量化的評估,大多所使用的方式為針對接受重建手術後期的病患做 單腳跳躍測試。因此本研究目的在於利用動態平衡測量儀的測試來量化前十字韌 帶損傷之病患其動態功能性表現,並了解在不同復健階段的表現變化與相對關係 本計畫收取四組受測者,分別為:健康受測者 20 位、前十字韌帶缺損患者 20 位、前十字韌帶重建術後初期患者 15 位及前十字韌帶重建術後後期患者 15 位。每位受測者都必須在動態平衡測量儀上進行四項的功能性活動,此四項功能 性活動分別為:負重蹲立(weight bearing/squat)、前跨(forward lunge)、跨步上 下(step up/over)及快步轉身(step/quick turn)。並以 SPSS 統計軟體進行分析。 結果顯示功能動作測試可以用來評估不同時期之前十字韌帶患者的動作變化及 表現,前十字韌帶缺損患者在膝關節趨近於伸直的角度下會減少股四肌的收縮, 而術後初期的患者其功能性表現為最差,術後後期的患者其功能性表現為最接近 健康受試者的狀況。因此,動態平衡測量儀的功能性測試為一評估之良好工具, 用以了解不同時期的前十字韌帶損傷患者其動態功能表現的變化及回復。. i.
(3) Abstract. Anterior cruciate ligament (ACL) is one of the most frequently injured structures of the knee which commonly results in structural and functional instability. Therefore, knee laxity and functional performance of ACL patients are two criteria frequently used in evaluating rehabilitation progress and long-term recovery outcome. However, there are fewer methods to quantify functional impairment.. Hop testing is. commonly used to measure function after ACL reconstruction (ACLR) but it would not appropriate for all patients of ACL deficiency.. Therefore, the purpose of this. study was to investigate the changes in dynamic functional performance with different rehabilitation stage of ACL injured patients. Twenty healthy subjects, twenty patients with unilateral ACL deficient, fifteen patients in the early stage of post-reconstruction and fifteen patients in the late stage of post-reconstruction participated in this study. tests were performed on the long force plateform.. Four functional movement. The functional movement tests. include weight bearing/squat, forward lunge, step up/over and step/quick turn. SPSS software was used to analyze the data.. The results indicated that the dynamic. functional performance tests were sensitive to detect changes of movement strategies following ACL injury and surgical reconstruction.. ii. The ACLD patients would.
(4) reduce quadriceps contraction in the knee terminal extension.. The functional. abilities were significantly decreased in the early ACLR subject, and were gradually recovered in the late stage of ACLR close to the normal.. Therefore, examing these. moderate functional tests using computerized dynamic postruogram system could be a good rehabilitative and evaluative tool.. iii.
(5) Acknowledge. 本論文得以順利完成首先要感謝我的指導教授許弘昌老師這兩年來的細心 教導,林秀真老師在整個實驗過程中的指導與協助,吳鴻文老師的鼓勵以及口試 委員羅世忠老師的不吝指導、提供意見,使得本論文能更臻完整,以最佳方式呈 現。 此外還要感謝學弟妹家銘、榮鏗、一涵、芳儀、柏瑞、立勛的協助,才得以 圓滿的完成實驗。同時感謝怡柔學姊、沛怡、瑀揚、斐文、世倫和致凱等人在精 神上給予的支持,有了你們的鼓勵及陪伴,才能讓我在一次次的難關中持續堅持 努力。 最後感謝全力支持我的雙親與家人,在求學的過程中給我支持和照顧,讓我 可以全心全力的致力於課業上。在此僅將本論文獻給支持我、幫助我的所有人!. iv.
(6) Contents Chinese Abstract‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧i Abstract ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧ii Acknowledge‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧iv Contents‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧v List of Tables ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧ix List of Figures ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧x. ChapterⅠ Introduction‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧1 1.1. Background‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧3 1.1.1. Anatomy ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧3. 1.1.2. Effect of muscle contraction to ACL‧‧‧‧‧‧‧‧‧‧‧‧4. 1.1.3. Diagnosis and clinical examination after ACL injury‧‧‧‧‧‧5 1.1.3.1. Clinical diagnosis‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧6. 1.1.3.2. Physical examination‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧6. 1.1.4. Treatment of ACL injury‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧11. 1.1.4.1. Conservative treatment‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧11. 1.1.4.2. ACL surgical reconstruction‧‧‧‧‧‧‧‧‧‧‧‧‧12. 1.1.4.3. Rehabilitation program following ACL reconstructive surgery‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧14. v.
(7) 1.2 Literature review ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧17 1.2.1. Functional assessment in ACL injured patients‧‧‧‧‧‧‧‧17. 1.3 Purpose‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧22. ChapterⅡ Methods‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧23 2.1 Participants‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧23 2.2 Instrument‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧24 2.2.1. Force plateform‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧25. 2.2.1.1. Calculating surface force characteristics‧‧‧‧‧‧‧‧‧26. 2.3 Experiment protocol‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧28 2.3.1. Experimental procedure‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧28. 2.3.1.1. Dynamic functional performance test ‧‧‧‧‧‧‧‧‧‧30. 2.4 Data analysis‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧36 2.4.1. Weight bearing/squat (WBS)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧36. 2.4.2. Forward lunge (FL)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧37. 2.4.3. 2.4.2.1. Distance‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧37. 2.4.2.2. Impact index‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧37. 2.4.2.3. Contact time‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧38. 2.4.2.4. Force impulse‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧38. Step up/over (SUO)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧39. vi.
(8) 2.4.3.1. Lift-Up index and percentage of lift-up index exerted by leading leg‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧39. 2.4.3.2. Movement time‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧41. 2.4.3.3. Impact index and percentage of impact index exerted by trailing leg‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧41. 2.4.4. Step/quick turn (SQT)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧43 2.4.4.1. Turn sway‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧43. 2.4.4.2. Initial weight shift‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧43. 2.4.4.3. Turn width‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧44. 2.4.4.4. Turn time‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧44. 2.4.4.5. Velocity of stepping forward and velocity of stepping backward‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧44. 2.5 Statistical analysis‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧46. ChapterⅢ Results‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧47 3.1 Demography of the participants‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧47 3.1.1. Basic data‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧47. 3.1.2. Activity level and knee scoring scale‧‧‧‧‧‧‧‧‧‧‧‧48. 3.2 Dynamic functional performance test‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧49 3.2.1. Weight bearing/squat (WBS)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧49. vii.
(9) 3.2.2. Forward lunge (FL)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧50. 3.2.3. Step up/over (SUO)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧53. 3.2.4. Step/quick turn (SQT)‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧57. ChapterⅣ Discussion ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧ 5 9 4.1 Dyna mi c func t i ona l pe r for ma nc e‧‧‧‧‧‧‧‧‧‧‧‧‧ 61 4.1.1. Weight bearing/squat‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧61. 4.1.2. Forward lunge‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧62. 4.1.3. Step up/over‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧65. 4.1.4. Step/quick turn‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧69. 4.2 Clinical relavance‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧72 4.3 Limitation‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧73. ChapterⅤ Conclusion‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧74 Reference‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧75. viii.
(10) List of Tables. Table 2-1: The questionnaire of activity level ‧‧‧‧‧‧‧‧‧‧‧‧‧‧29 Table 2-2: The Lysholm knee scoring scale ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧30 Table 3-1: The basic data of ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧48 Table 3-2: Lysholm knee scoring scale and activity level of ACLD, early stage of post-ACLR and late stage of post-ACLR groups‧‧‧‧‧‧‧‧‧48 Table 3-3: The weight bearing score of each side in ACLD, early stage of post-ACLR, Late stage of post-ACLR‧‧‧‧‧‧‧‧‧‧‧‧‧50 Table 3-4: The percentage of impact index in ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧56. ix.
(11) List of Figures. Figure 1-1: The knee joint ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧3 Figure 1-2: Hand position for the Lachamn test ‧‧‧‧‧‧‧‧‧‧‧‧‧‧7 Figure 1-3: The anterior drawer test ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧7 Figure 1-4: Knee ligament arthrometer KT-2000‧‧‧‧‧‧‧‧‧‧‧‧‧‧8 Figure 2-1: PRO Balance Master® ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧25 Figure 2-2: The force plateform PRO Balance Master® ‧‧‧‧‧‧‧‧‧25 Figure 2-3: The position and foot position in weight bearing/squat test‧‧‧‧‧31 Figure 2-4: The forward lunge test‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧32 Figure 2-5: The step up/over test‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧33 Figure 2-6: The step/quick turn test ‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧34 Figure 2-7: Vertical ground reaction force of summation of both legs, the leading leg and trailing leg in step up/over test‧‧‧‧‧‧‧‧‧‧‧‧‧‧40 Figure 2-8: Vertical ground reaction force of summation of both legs and the leading leg in step up/over test‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧40 Figure 2-9: Vertical force in step up/over test‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧41 Figure 2-10: Vertical ground reaction force of summation of both legs and the trialing leg in step up/over test‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧42. x.
(12) Figure 2-11: Medial-latera displacement of COP in step/quick turn test‧‧‧‧44 Figure 2-12: Anteroposterior displacement of COP in step/quick turn test‧‧‧45 Figure 3-1: The lunge distance of ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧‧51 Figure 3-2: The impact index of ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧‧51 Figure 3-3: The contact time of ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧52 Figure 3-4: The impulse index in ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧53 Figure 3-5: The lift-up index in ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧‧54 Figure 3-6: The percentage of lift-up index in ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧55 Figure 3-7: Movement time in ACLD, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧‧55 Figure 3-8: The impact force index in ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧‧56. xi.
(13) Figure 3-9: The turn time of ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧‧‧‧‧57 Figure 3-10: The stepping back velocity of ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control groups‧‧‧‧‧‧‧‧‧58. xii.
(14) Chapter 1. Introduction. Knee joint is the largest joint in the body. joint and is able to move in six degrees of freedom.. It is considered as a condylar The knee joint provides a large. degree of range of motion (ROM). However, because of the bony congruency little inherent knee stability, the joint greatly depends on muscular and ligamentous structures for stability and strength. The most common injured ligament in the knee joint is anterior cruciate ligament (ACL) injury. It will significantly increase the anterior laxity of knee joint 20,78. , deficient muscle strength. 21,41. , decrease proprioception. 27. and alter muscle. activity pattern 2 and thus lead to difficult to return to full function of individuals after injury. 28. . These residual functional deficits were reported resulted from decreased. muscle strength in patients after ACL injury.. In order to restore stability and. function of the knee, ligaments reconstruction surgery is considered. Although the structural stability can be rebuilt 5,6. 1,9. , deficits in muscle strength. 16,49,56. , proprioception. in patients after ACL surgical reconstruction have been widely reported. These. impairments would affect the functional performance in different extent in these patients. 16,25,41,58,60,75. . An appropriate rehabilitation program for these patients after. 1.
(15) injury or reconstruction will help to restore their impairment and thus promote their functional abilities.. Therefore, monitoring the dynamic functional performance. during their rehabilitation provide insight to the recovery of their impairments.. 2.
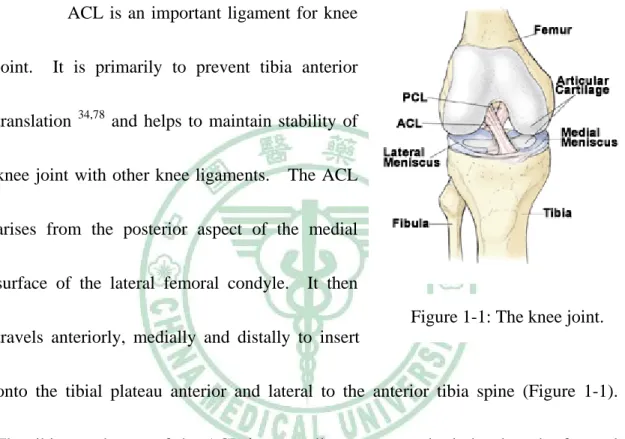
(16) 1.1. Background. 1.1.1. Anatomy. ACL is an important ligament for knee joint.. It is primarily to prevent tibia anterior. translation. 34,78. and helps to maintain stability of. knee joint with other knee ligaments.. The ACL. arises from the posterior aspect of the medial surface of the lateral femoral condyle.. It then Figure 1-1: The knee joint.. travels anteriorly, medially and distally to insert onto the tibial plateau anterior and lateral to the anterior tibia spine (Figure 1-1). The tibia attachment of the ACL is generally stronger and winder than the femoral attachment and the ligament has a tendency to “fan out” as it proceeds distally.. The. ACL may be divided into two separate bands: the anteromedial and the posterolateral. The orientation of the two bands furnishes a general ideal of the dynamics of the ACL to remain tight throughout the ROM of the knee. Scientists typically report both a linear stiffness and ultimate tensile load to evaluate biomechanical properties of ligaments.. 3. Trent et al.. 73. tested the ACL with.
(17) bone blocks of the femur ACL tibial complex (FATC) of cadavers between the ages of 29 and 55 years. A linear of 141 N/mm and ultimate tensile load of 633 N were reported.. Changes in the length of the ACL during extension-flexion,. internal–external and varus-valgus rotations have both surgical and rehabilitative connotations.. Literature has documented the effect of knee motion on the length and. orientation of the human ACL. 29,70,79. .. Because of the broad attachments of ACL,. some collagenous bundles experience heightened tension whereas others carry less load based on range of motion and rotational orientation. In generally, orientation of the ACL anteromedial band is taut in flexion and lax in extension, whereas the posterolateral bundle of ACL is taut in extension and lax in flexion 29,70.. 1.1.2 Effects of Muscle Contraction to ACL. Hamstring muscles have been recognized as an important element in compensating for the loss of stability in the ACL-deficient knee whereas quadriceps contraction is considered to induce anterior instability.. Therefore, the strain. behavior of the ACL under quadriceps and hamstring contraction have studied and described with several different approaches, including anatomical observation mathematical modeling. 12. , ACL force measurement. 4. 47,48. 30. ,. and tibial displacement.
(18) measurement 7,11. The ACL was found to be unstrained or have lower loads during hamstring isometric contraction 8.. The effects would remain even incorporate with the. contraction of the quadriceps muscle.. Isolated quadriceps contraction would have. the peak anterior tibial translation in the last 25 to 30 degree of knee extension. 8,69. .. The ACL graft load and anterior tibial translation would decrease with quadriceps contraction while knee flexion more.. The contraction force of the quadriceps would. become even the opposite that pulled the tibia posteriorly when knee flexion more than 70 degrees 69.. Study investigated the ACL strain value in closed-kinetic chain. exercises showed the similar behavior to those during performing open-kinetic chain exercises 10.. 1.1.3. Diagnosis and Clinical Examination after ACL Injury. A comprehensive examination of an individual with suspected injury to the ligamentous structures of the knee joint is the first step in a complete treatment and rehabilitation process.. 5.
(19) 1.1.3.1. Clinical Diagnosis The clinical diagnostic tools include x-ray, magnetic resonance imaging. (MRI) and arthroscopy.. X-rays of the knee joint was taken first to assess for any. possible bony structural problems.. MRI is a diagnostic invasive procedure, which. help assessing the damage present to the soft tissues inside and around the knee joint. The accuracy of MRI in clinical diagnosis for ACL tear was 90% 72, but it is unable to distinguish the degree of tear. If physical exam and diagnostic imaging studies have been performed and the definite diagnosis remains in doubt, a diagnostic arthroscopy may be recommended. During this invasive procedure, a tiny fiber optic lens connected to a video system is able to view all of the structures directly through a 4-millimeter incision.. The arthroscopy allows the surgeon to directly examine and assess the. damages inside the knee joint and to repair many of them surgically.. 1.1.3.2. Physical Examination. Stability Testing ACL rupture will result in anterior tibiofemoral laxity which is considered to lead structural and functional instability.. 6. The stability of knee joint is measured.
(20) by a manual special test or by an instrumented arthrometer.. The most common physical. examinations for patients of ACL injury are Lachman test and anterior drawer test.. The. Lachman test has been reported to be the best test. for. assessing. the. integrity. of. the. Figure 1-2: Hand position for the Lachman Test 45.. posterolateral band of the ACL and is a test for one-plane anterior instability. Performing the Lachman test is illustrated in Figure 1-2.. The patient lies supine and. places the knee in approximately 20 to 30 degree of flexion as recommended.. This. position is close to the functional position of the knee, in which the ACL plays a major role. A positive sign is indicated by a mushy or soft end feel when the tibia is moved forward on the femur and disappearance of the infra-patellar tendon slop. The Lachman test was found to be 95% sensitive and was the single best clinical test for diagnosing complete ACL tears 40. Another manual special test to assess anterior stability of the knee joint is the anterior drawer test.. This test. involves flexing the knee to 90° and the Figure 1-3: The Anterior drawer test 24.. hip to 45°. The examiner is seated and. 7.
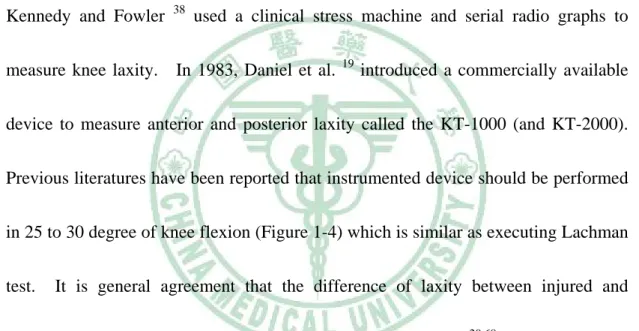
(21) places the forefoot of the tested extremity under his or her buttock to stabilize the distal portion of extremity (Figure 1-3). The examiner’s hands are placed around the tibia, palpating the hamstring tendons medially and laterally to confirm a relax state of these muscle-tendon units.. If the tibia moves forward more than 6 mm on the femur,. it is a positive sign for this test. Instrumented testing using knee ligament arthrometers began in 1971 when Kennedy and Fowler. 38. measure knee laxity.. In 1983, Daniel et al.. used a clinical stress machine and serial radio graphs to 19. introduced a commercially available. device to measure anterior and posterior laxity called the KT-1000 (and KT-2000). Previous literatures have been reported that instrumented device should be performed in 25 to 30 degree of knee flexion (Figure 1-4) which is similar as executing Lachman test.. It is general agreement that the difference of laxity between injured and. non-injured knee greater than 3mm is indicative of an ACL tear 20,68. In addition, the reliability and validity of KT arthrometer have been confirmed 19.. Figure 1-4. Knee ligament arthrometer KT-2000 18.. 8.
(22) Muscular Strength Testing The use of manual muscle testing (MMT) has become a clinical standard for muscular strength assessment.. MMT is an inexpensive and quick assessment. technique that ultimately depends on the subjective rating of muscular strength by the examiner.. It is the primary initial examination method used clinically to quickly. discern the strength of the musculature surrounding the knee joint. In addition to MMT, individuals with higher levels of function require more advanced methods of muscular assessment. Isokinetic testing and exercise is the most common used by clinicians for assessment and training.. Through isokinetic. evaluation and exercise, the limb keeps at a constant, predetermined angular velocity through the dynamometer’s application of accommodating resistance. Hence using an isokinetic device is able to loaded the tested muscle to its maximum capability through its entire ROM, thereby allowing a more efficient and effective form of evaluation and exercise.. Functional Testing Functional testing is an important element in every musculoskeletal examination.. Hopping tests were wildly used to evaluate the functional performance. of the lower extremity in the ACL injured patients. 9. 4,50,57,63,75. and found to have high.
(23) discrimination 32,36.. The one-leg hop test involves jumping off and landing upon the. same limb, and the results of the involved limb would be compared to those of the uninvolved limb. 90%. 37. .. It has been suggested that the normal ratio is greater than 85% 4 or. A study investigated the changes in impairments and disabilities of the. ACL-reconstructed (ACLR) patients found triple-jump and stair-hop tests were two of the most significant predictors of disability in the follow-up period from 3 months to 2 years post-operation 61.. Knee Rating or Scoring Scales Subjective rating scales are used for quantify the patient’s perception of function and pain levels, to serve as a baseline following injury or surgery and during serial evaluations and follow-up. The simplest form of subject rating scale is the visual analog pain scale.. With this scale, the patient is asked to quantify the pain. with rest or certain activities using the scale from 0 (no pain) to 10 (worst pain ever experienced).. Knee questionnaire is also mostly common used, such as Lysholm. questionnaire, Knee Outcome Survey (KOS) and International Knee Documentation Committee (IKDC).. These questionnaires provide the quantitative information. about the patient’s satisfaction of functional ability after reconstruction and can be used in research when comparing rehabilitation or surgical methods 17.. 10.
(24) 1.1.4 Treatment of ACL Injury. The initial treatment of an ACL injury is based on reducing pain and swelling and restoring full ROM of knee joint.. There are two treatment manners. following a quiescent state: conservative and ACL surgical reconstruction. Some patients who experience ACL tears are able to resume normal daily activities without surgical reconstruction while some patients are unable. 23,64. . Making the decision as. to whether or not operative treatment of an ACL tear is needed to consider some important factors.. These factors include the age, activity level (recreational and. occupational), the ability and willingness of the patient to participate in post-operative rehabilitation, the degree of instability of the joint, and other associated injuries to the knee (e.g. other ligamentous or meniscal problems).. Regardless of the decision of. surgical reconstruction, the injured knee needs to be rehabilitated beginning immediately after ACL injury.. 1.1.4.1. Conservative Treatment Conservative treatment involves the re-education of the quadriceps,. hamstring and other lower extremity muscles with an emphasis placed on the hamstrings which can restrict the amount of forward tibial translation relative to the. 11.
(25) femur.. Re-establishment of neuromuscular control of the lower extremity has. recently been considered as one of the keys to restoring dynamic joint stability and functional movement patterns subluxation. 14. 15,64. . Neuromuscular control results in avoidance of. , with the sequent reduced risk of further injuries.. Activities of daily. living and sport activities require coordination neuromuscular control and muscle strength sufficient to perform these movements and activities.. Therefore, the aim of. the conservation treatment programs for ACL injury is to normalize dynamic knee joint stability and muscle strength of the lower extremity 59. If the patients could not manage their daily activities after conservation treatment programs, difficulties will arise when the athlete return to strenuous physical activities and lead to the athletes who continue sports have a very high rate of meniscal and chondral injuries.. Therefore, the treatment of surgical. reconstruction is suggested.. 1.1.4.2. ACL Surgical Reconstruction In order to restore stability and function of the knee with ACL-deficiency. (ACLD), ligament reconstruction surgery is considered. graft replacement of a torn ACL. graft that is used.. Reconstruction is surgical. The types of surgery differ mainly in the type of. The two most commonly used grafts are the patella tendon and. 12.
(26) hamstring tendon autografts.. Patella Tendon The patellar tendon connects the patella to the tibia.. The graft is taken. from the central third of the patellar tendon and including its bone insertion sites. Thus the attachments of the tendon to the bone are not disturbed (bone-patellar tendon bone or BTB).. Then the graft is threaded through holes drilled in the tibia and femur,. and finally screwed into place. When the graft is placed into the knee, this allows for bone to bone healing. graft choice.. The patella tendon graft has been considered the ideal. It is accessible, has good structural and fixation properties and a. predictable success rate in the restoration of knee stability 1,31,39.. Hamstring Tendon The semitendinosus (ST) or ST/gracilis tendons from the hamstring are used to graft.. The tendon segments are folded and braided together to form a. quadruple thickness strand for the replacement graft.. The braided segment is. threaded through the heads of tibia and femur and its ends fixated with screws on the opposite sides of the two bones. Previous studies showed that there was no significant difference between. 13.
(27) the two grafts in terms of ligament stability, ROM, and general symptom. 9,17,39,46. .. Therefore, hamstring tendon graft does as well as the patellar tendon graft 39.. 1.1.4.3. Rehabilitation Program Following ACL Reconstructive Surgery The primary goals of ACL reconstruction (ACLR) and rehabilitation. include restoring the knee stability and returning to normal or sports activities safely and expediently.. The rehabilitation program of post-ACL reconstruction is divided. into three phases.. Phase Ⅰ - Immediate to 3 months post-reconstruction The clinical goals of phase Ⅰ initial stage include decreasing swelling and obtaining full passive knee extension and flexion to 110 degrees.. Continuous. passive motion (CPM) and rehabilitation exercises are started upon the patient’s arrival to the hospital room after surgery. degrees.. The machine of CPM is set to 10-0-30. And quadriceps muscle contraction and full knee extension exercises are. performed to promote leg control and to minimize the potential for a patella contracture. The clinical goals of phase Ⅰ late stage include controlling swelling and obtaining full knee extension and flexion to 130 degrees. At this time, patient can. 14.
(28) also start the early strengthening exercise.. During this phase, the patient is remain. reclining as much as possible to control swelling and weight bearing as tolerated with crutches is encourage.. Phase Ⅱ -. Three to six months post-reconstruction. The emphasis in this phase is on gaining full ROM of knee flexion, return to normal daily activities and moderate strengthening exercise to regain strength to 80%. At this time, the patient should have nearly full ROM and normal gait without assistive devices. Functional strengthening is initiated in this phase, including knee bend, step-up, leg press, squat and using a stationary bicycle. Closed kinetic chain (CKC) exercises are preferred for functional strengthening of the lower extremity.. This. form of exercise has been shown to reduce shear force across the tibiofemoral joint 8 whereas open kinetic chain (OKC) exercises facilitate isolated quadriceps muscle strengthening and owing compression force to tibiofemoral joint. must be performed with caution.. So OKC exercises. These exercises are started with lower weight and. gradually progressed to higher weight.. 15.
(29) Phase Ⅲ - More than six months post-reconstruction The emphases in phase Ⅲ are on advanced strengthening and return to sports.. To advance into the final phase of the rehabilitation program, the patient. needs to have nearly full ROM.. It is now customary to allow a return to full sports. activities 6 months after surgery 43,67.. Patients are encouraged to progress from high. repetition/ low weights to low repetition/ high weights. In this phase, agility activities could also be started. include lateral shuffles, cross-over drills and backward running. begin solo sports activities.. These activities Patients may also. These early agility activities promote patient confidence,. facilitate moderate-speed strength and redevelop quickness, agility and sport-specific skills.. As the patient progresses, agility workouts become more vigorous, to include. activities such as figure-of-eights and half- to full-speed running.. 16.
(30) 1.2. Literature Review. 1.2.1 Functional Assessment in ACL Injured Patients. ACL rupture would increase the anterior laxity of knee joint 20,78 knee stability.. and alter. In addition, muscle strength deficit, diminished proprioception (or. joint awareness) and lack of neuromuscular control following ACL injury were also wildly reported. 13,27,62,76. and related to causing dynamic instability of the knee joint.. Therefore, the aim of rehabilitation programs for patients with ACL injury is to normalize dynamic knee joint stability and muscle strength of the lower extremity and subsequence reduce risk of further injuries. Patients with ACL rupture accepted reconstructive surgery for restoring stability and function of the knee and returning to full function of activities. Although the ligamentous structures for knee stability was rebuilt by surgery proprioception and neuromuscular control diminished after ACL injury and may not recover after surgical reconstruction. 26,44,76. .. 1,9. , the. 13,26,27,44,62,76. The surgeons would. attempt to reconstruct the disruption to surrounding soft tissue during surgery, but the implantation of a substitute for the ACL could not restore the sensorimotor system, and which may result in a compromised afferent neural system. 17. 53,55. .. These.
(31) neuromuscular deficits in ACLR patients were different from ACL-deficient (ACLD) patients 6,77 and have been reported persisting from 6 weeks to 9 years postoperative 15. These impairments would affect the functional performance in different extent in ACLR patients. 16,25,41,58,60,75. . Therefore, the poor relationship between knee laxity. and its functional performance has been reported 23,66,71. Several methods have been reported to follow up the functional status of the ACL injured patients. Knee questionnaire is mostly common used in longitudinal follow up study, such as Lysholm questionnaire. 42. , Knee Outcome Survey (KOS). 35. and International Knee Documentation Committee (IKDC) 33. These questionnaires provide the quantitative information about the patient’s satisfaction (subjective data) of functional ability after reconstruction and can be used as a bridge that connected to the objective parameters measured from other equipments. Although those clinical methods exist for subjectively evaluating functional status, there are fewer methods to objectively quantify functional impairment. Hopping test is a wildly used method to evaluate the functional performance of the lower extremity in the patients after ACL injury or reconstructive surgery. 4,50,57,63,75. .. Hop test is a valid and reliable method of measuring function and has high discrimination 32,36.. A study investigated the changes in impairments and disabilities. of the ACLR patients found triple-jump and stair-hop tests were two of the most. 18.
(32) significant predictors of disability in the follow-up period from 3 months to 2 years post-operation. 60. . However, the hopping test, which is a maximal test, can only be. performed on the patients in the late stage of post-operative and not appropriate for all patients with ACLD 4,63. Alternative methods to measure function are therefore needed for clinical decision-making, especially for the patients in early stage of post-operative ACL reconstruction.. Using motion analysis system to observe the change of movements. was well investigation. It is a valuable tool for monitoring the rehabilitation process after ACL injury 2,15,52,64.. However, the time consuming, complex of procedure and. calculation of the motion analysis system are not easily to application for clinician. On the other hand, the computerized dynamic posturogram system (NeuroCom® International Inc.) was also used to evaluate the functional performance in ACL injured and ACL reconstruction patients quantitatively. 16,49. .. The functional. activities of computerized dynamic posturogram system are moderately challenging test for strength and sensorimotor control which was suitable to application for most ACL injured patients. And the convenient and friendly operation of this system was to be a good rehabilitative and evaluative tool for clinician. Chmielewski TL et al. (2002) used the weight bearing squat, unilateral stance, sit to stand and step up over tests to compare the difference between healthy. 19.
(33) individuals, ACLD patients and ACLR patients and follow up the outcome of ACLR patient at early stage (1, 6 and 12 weeks) after reconstruction.. The results showed. that weight bearing squat test could detect the altered weight bearing in ACLD and ACLR group.. The unilateral stance and sit to stand tests revealed that ACLD. patients had a larger body sway.. And the step up over test was correlated with KOS. score and sensitive to disability.. Mattacola et al. (2004) also used step up over and. forward lunge to assess the difference between healthy individuals and patients at least 6 months after ACLR (late stage of post-reconstruction).. The results showed. that affected limb took longer time to complete the step up over test and less force was produced in forward lunge. In these studies, the investigators suggested that the assessment by using the computerized dynamic posturogram system could provide insight into disability in ACL injured patients. Nevertheless, the information from the objective functional assessment using computerized dynamic posturogram system was not completed in various phase of ACL injured patients. In addition, all movements of the evaluated functional performance test are mainly in sagittal plane.. ACL contributes stability of. knee joint not only in the anteroposterior but also in the other two directions and assists in controlling the normal rolling and gliding movements of the knee. Therefore, investigating the functional activities required movements in frontal and. 20.
(34) transverse planes is also necessary for ACL reconstruction patients.. But, there are. limited studies had ever investigated the functional tasks involve tibia rotation.. 21.
(35) 1.3. Purposes. The purpose of this study was to investigate the changes of dynamic functional performance in ACLD patients, early and late stages of post-operative ACLR patients. Four activities were selected to perform on the long forceplate (NeuroCom® International Inc.) to evaluate their dynamic functional performance.. These. functional performance tests were (1) weight bearing/squat; (2) forward lunge; (3) step up/over; and (4) step/quick turn. The hypothesis of this study was that the performance of the functional tests on the force plateform would be affected after ACL injury and reconstruction compared to the healthy control population.. 22.
(36) Chapter Ⅱ. 2.1. Methods. Participants. There were four study groups recruited in this study.. These groups were. healthy individuals, patients with complete ACL rupture (ACLD), patients at early-stage. post-ACL. reconstruction. and. patients. at. late-stage. post-ACL. reconstruction. Twenty young healthy subjects were included as the control group. All subjects were firstly submitted to physical examination, including the Lachman test, reverse Lachman test, valgus stress test, varus stress and McMurry test, to ensure the sound structures around the knee joints.. The exclusive criteria included that subjects. who had neuromuscular disorders in the lower limb, pain or injury to the ligaments of knee were excluded from this study. The ACLD group consisted of twenty patients with unilateral ACL injury. All of these patients had a positive Lachman’s test and bilateral difference exceed 3mm in anterio-posterior laxity measured by arthrometer (KT-2000, MEDmetric, San Diego, USA).. Patients who had other neuromuscular disorders of lower limb,. 23.
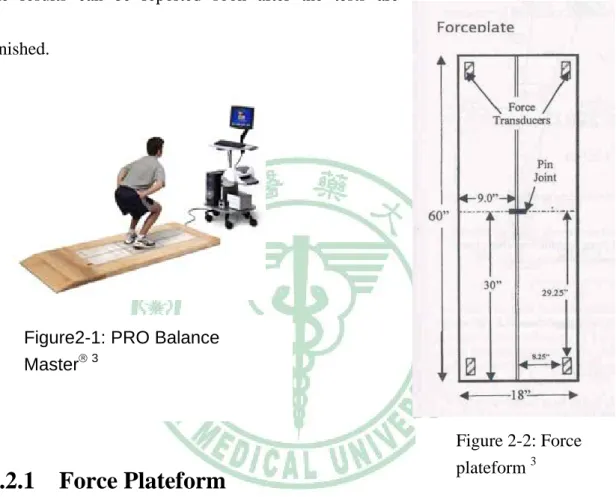
(37) acute pain or swelling of the knee and surgical procedure in either leg were excluded from this study. Fifteen patients post ACL reconstructive surgery for 3 to 4 months as early stage of post-ACLR (early ACLR group) and fifteen patients post ACL reconstructive for at least 6 month surgery as late stage (late ACLR group) were enrolled in this study.. All these patients had received the unilateral ACL reconstruction with BTB. graft.. Patients who had other neuromuscular disorders of lower limb, acute pain or. swelling of the knee and surgical procedure in either leg were excluded from this study. All the ACL patients were recruited from the Department of Orthopedics of China Medical University Hospital. Before the experiment, every subject signed the consent forms that were approved by the Ethics Committee of China Medical University Hospital.. 2.2. Instrument. The functional movements were tested by using a computerized dynamic posturogram, PRO Balance Master® (NeuroCom® International, Inc.) (Figure 2-1). The PRO Balance Master® system consists of a dual force platform and the computer.. 24.
(38) The dual force plateform can measure the forces exerted under subject’s feet.. The. computer received force measurements from the dual force plateform at 100 Hz, and processed with its own software to analyze the performance in each tested task and the results can be reported soon after the tests are finished.. Figure2-1: PRO Balance Master® 3. Figure 2-2: Force plateform 3. 2.2.1 Force Plateform. The force plateform includes two 9-inch by 60-inch foot-plates.. There is a. pin joint between the two plates, 30 inches from the rear border of the plates.. The. axis along the pin joint constitutes the X (mediolateral or ML) axis. The pin joint also intersects the Y (anteroposterior or AP) axis.. Each foot-plate rests on two. single-axis force transducers, which measure force by using variable inductance. 25.
(39) compression loadcells, with the sensitive axes oriented vertically.. The transducers. are mounted along the front-to-back center line of each plate (one 29.25 inches behind and the other 29.25 inches in front of the pin joint).. The lateral distance between left. and right plate transducers and center is 8.25 inches (Figure 2-2).. 2.2.1.1. Calculating Surface Force Characteristics. Total Vertical Forces The total vertical force exerted on the two foot-plates (equal to subject’s weight) is calculated by summing the four vertical force signals: FV(total vertical)= LR+LF+RR+RF. (2-1). Whereas LR represent the vertical force is detected by loadcell at left-rear and LF represent the vertical force is detected by loadcell at left-front. RR represent the vertical force is detected by loadcell at right-rear and RF represent the vertical force is detected by loadcell at right-front.. 26.
(40) X Axis Center of Vertical Force The X (lateral) axis position of the total vertical force center is calculated as follows:. PX (total X axis ) =. (RR + RF ) − (LR + LF ) × 8.25in RR + RF + LR + LF. (2-2). Where 8.25 inches is lateral distance between the foot-plate transducers and the boundary (X axis zero position) of the two foot-plates. For example, when all vertical forces are carried by the two right plate transducers, the X axis center of force position is a positive 8.25 inches.. When the center of vertical force is at the. boundary, the vertical forces carried by the two left transducers are equal to those carried by the two right transducers and the X axis center of force position is zero.. Y Axis Center of Vertical Force. The Y (anteroposterior) axis position of the total vertical force on the two foot-plates is calculated with the following formula: PY (total Y axis ) =. (LF + RF ) − (LR + RR ) × 29.25in LF + RF + LR + RR. (2-3). For example, when the vertical forces on the forceplate are carried only by the front transducers, the Y axis Center of force position is a positive 29.25 inches. When the vertical force is carried equally by the front and rear transducers, the Y axis force position is zero.. 27.
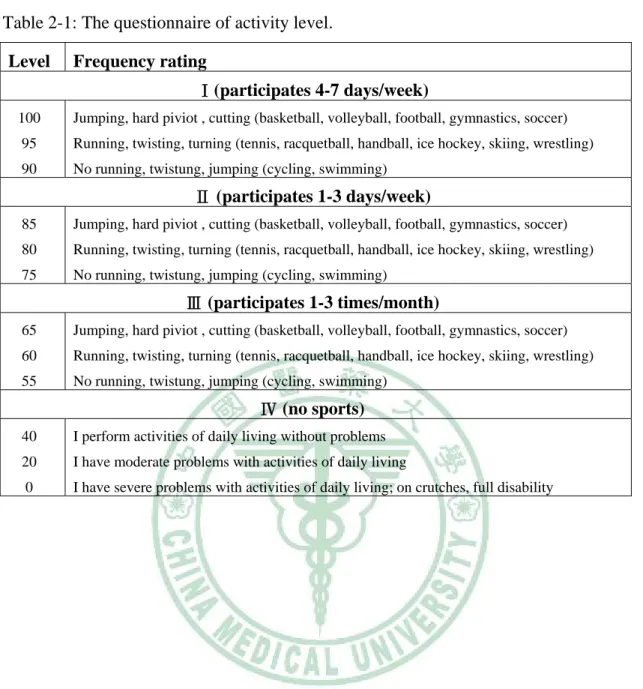
(41) 2.3. Experiment Protocol. The experiment included basic data collection, the pre-test examnination and the dynamic functional performance tests.. The dynamic functional. performance tests consisted of (1) weight bearing/squat test, (2) forward lunge test, (3) step up/over test and (4) step/quick turn test.. 2.3.1 Experimental Procedure. All subjects were firstly consented with the study aim, the procedure, the potential risks, and the benefits of this experiment. Basic data of each subject, such as age, body height, body weight and activity level (Table 2-1) was collected. Subjects then were asked to fill the Lysholm knee scoring scale (Table 2-2), which is a subjective rating scale, as a record of present general knee condition. Physical examination was then performed to ensure the other structure of the subjects’ knee joints. The examination included Lachman test, posterior drawer test, valgus stress test, varus stress and McMurry test.. 28.
(42) Table 2-1: The questionnaire of activity level. Level. Frequency rating Ⅰ(participates 4-7 days/week). 100. Jumping, hard piviot , cutting (basketball, volleyball, football, gymnastics, soccer). 95. Running, twisting, turning (tennis, racquetball, handball, ice hockey, skiing, wrestling). 90. No running, twistung, jumping (cycling, swimming). Ⅱ (participates 1-3 days/week) 85. Jumping, hard piviot , cutting (basketball, volleyball, football, gymnastics, soccer). 80. Running, twisting, turning (tennis, racquetball, handball, ice hockey, skiing, wrestling). 75. No running, twistung, jumping (cycling, swimming). Ⅲ (participates 1-3 times/month) 65. Jumping, hard piviot , cutting (basketball, volleyball, football, gymnastics, soccer). 60. Running, twisting, turning (tennis, racquetball, handball, ice hockey, skiing, wrestling). 55. No running, twistung, jumping (cycling, swimming). Ⅳ (no sports) 40. I perform activities of daily living without problems. 20. I have moderate problems with activities of daily living. 0. I have severe problems with activities of daily living; on crutches, full disability. 29.
(43) Table 2-2: The Lysholm knee scoring scale. Pain. Limp □ None (5). □ None (25). □ Slight or periodical (3). □. □ Severe and constant (0). Inconstant and slight during severe exertion (20). □ Marked during severe exertion (15). Support. □ Marked on or after walking more than 2 km (10). □ None (5) □ Stick or crutch (2). □ Marked on or after walking less than 2 km (5). □ Weight-bearing impossible (0). □ Constant (0). Locking. Swelling. □ No locking and no catching sensations (15). □ None (10). □ Catching sensation but no locking (10). □ On severe exertion (6). Locking □ Occasionally (6). □ On ordinary exertion (2). □ Frequently (2). □ Constant (0). □ Locked joint on examination (0). Stair-climbing □ No problems (10). Instability □ Never giving way (25). □ Slightly impaired (6). □ Rearly during athletics or other severe exertion (20). □ One step at a time(2) □ Impossible (0). □ Frequently during athletics or other severe exertion (or incapacible of participation) (15). Squatting □ No problems (5). □ Occasionally in daily activities (10). □ Slightly impaired (4). □ Often in daily activities (5). □ Not beyond 90 degrees (2). □ Every step (0). □ Impossible (0). 2.3.1.1. Dynamic Functional Performance Test. All the four dynamic functional performance tests were performed on the long dual force platform system of the PRO Balance Master®.. These tests. included wight bearing/squat, step/quick turn, step up/over and forward lunge. Each subject performed each task for three times on each leg and having at least 10. 30.
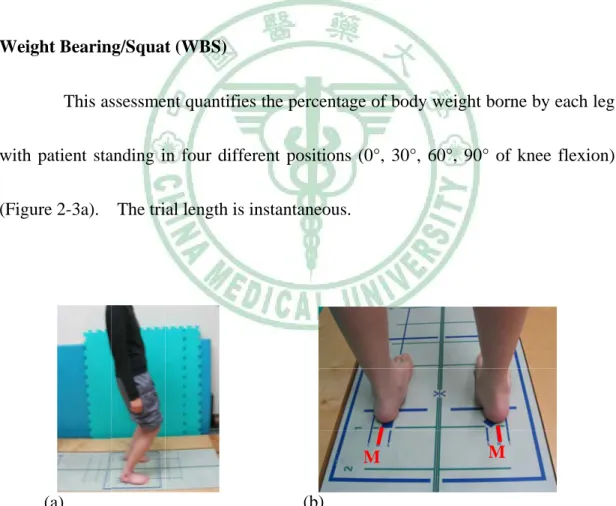
(44) seconds resting between each trial. Although the test order of the four functional tests is radomized, the patients of ACLD and ACLR group executed the tests with sound side first at each testing session.. Subjects were given the same verbal. description of each test followed by the video demonstration before performing the test. The detailed procedures of these dynamic functional performance tests were described as below.. Weight Bearing/Squat (WBS). This assessment quantifies the percentage of body weight borne by each leg with patient standing in four different positions (0°, 30°, 60°, 90° of knee flexion) (Figure 2-3a). The trial length is instantaneous.. M. (a). M. (b). Figure 2-3: The position (a) and foot position (b) in weight bearing/squat test.. During the test, the patient standed with keeping feet parallel and positioned feet to align each medial mallelous with the wide blue line and the center 31.
(45) of each heel with the “M” line (Figure.2-3b). Then the tester gived the commands: “look straight ahead. Stand with your hands on your side. Hold this position until I say stop”.. Forward Lunge (FL). The forward lunge test was used to measure the movement characterics as the individual started in a standing psition, lunge forward with one leg and then return to the original standing position (Figure 2-4).. Figure 2-4: The forward lunge test.. Each subject was given the commands: “When the assessment begin you will see a yellow square at the top of screen. Stand up right at the start of the force plateform.. When you see the green square, lunge forward with your left (right) foot. as far and as fast as you can, bending the forward knee, then return to the start. 32.
(46) position as fast as possible and hold steady”.. This action requires not only adquate strength and good inter-limb coordination, but also the ability to change the muscle activation from concentric to eccentric which related to the impact force.. Step Up /Over (SUO). The step up and over test was performed using a 30 cm wooden step placed on the center of the force plateform.. Subjects stood a comfortable distance behind. the step, determined during a practice trial. Then subject was asked to step up test leg (leading leg) onto the curb, lift the other leg (trailing leg) over the curb and down onto the floor, and step down the test leg (Figure 2-5) .. Figure 2-5 The step up/over test. Each subject was given the commands: “When the assessment begin you will see a yellow square at the top of screen. Stand up right at the start of the force plateform.. When you see the green square,quickly step up with your left (right). 33.
(47) foot, swing your other leg up and over the curb, the step down with your test leg. Hold that position as steady sa possible until I say stop” .. This movement requires strength, balance and coordination to perform properly. The concentric and eccentric contraction force of testing leg are both tested during the movement.. Step/Quick Turn (SQT). This assessment quantifies two movement characteristics as the subject takes two forward steps, quickly turn 180 degree, and step back to the start location (Figure 2-6) .. Figure 2-6: The step/quick turn test.. 34.
(48) Each subject was given the commands: ”When the assessment begin you will see a yellow square at the top of screen. Stand up right at the start of the force plateform.. When you see the green square, start with your left (right) foot and take. two steps forward turn around quickly to your left (right) and return to the end of the force plateform where you started”. And all of the subjects were asked to use the pivot pattern when turning.. 35.
(49) 2.4. Data Analysis. The vertical component of the ground reaction force was measured by the four loadcells under each corners of the force plateform and then the PRO Balance Master® system calculated the instantaneous position of center of pressure (COP) and other parameters. Because of the limited outcome measures in step /quick turn and step up/over tests were provided from the PRO Balance Master®, the raw data from the loadcells were also exported and then analyzed with a self-design MATLAB program (MathWorks, USA) for further analysis.. 2.4.1 Weight Bearing/Squat (WBS). The parameter measured of WBS test was the percentage of weight borne by each leg in each angle of knee flexion (0°, 30°, 60° and 90°). It was expressed as percentage of body weight (%BW).. 36.
(50) 2.4.2 Forward Lunge (FL). Four parameters were measured of forward lunge test were distance, contact time, impact index and force impulse.. 2.4.2.1. Distance. Distance is the length of the forward step, expressed as a percentage of body height (%BH). For this assessment, the patient was asked to lunge as far and as fast as possible.. 2.4.2.2. Impact Index. Impact index is the amount of the maximum vertical force exceeded the body weight through the lunge leg as it lands on the surface, expressed as a percentage of body weight (%BW). Impact index =. The formula of impact index as follows:. maximal impact force - body weight × 100 % body weight. (2-4). The lunge foot must rapidly accept the body weight and stop the forward progression of the center of gravity (COG). 37. The lunge leg must switch from.
(51) concentric control (advance the limb) to eccentric control (place the foot and accept weight loadiong) as the COG passage over the foot. The amount of impact force transmitted through the lunge leg as it lands is an indication of its eccentric control.. 2.4.2.3. Contact Time. Contact time is the duration that the lunge is in contact with the surface, expressed in seconds. Scoring starts with the first impact of the lunge foot, and stops when the foot leaves the surface to step backward. For this assessment, the patient is asked to lunge as far and as fast as possible.. Contact time will be. extended if it takes the lunge leg longer to accept the body weight and brake the COG momentum (eccentric deficit) and/or to recruit the muscle forces necessary to reverse the direction of COG travel and push the body weight backward (conccentric deficit).. 2.4.2.4 Force Impulse. The impulse is defined as the amount of work performed by the lunge leg during the whole landing and thrusting phases of the movement, expressed in percent body weight (force) and second (time). To compared between subjects, the impulse. 38.
(52) is further divided by contact time, the equation for calculating force impulse is showed as followed. Good performance is considered that doing a lot of work in a short period of time.. Force impulse =. ∫. t = contact time. t =0. Vertical force/BW. Contact time. (2-5). 2.4.3 Step Up /Over (SUO). Five measured parameters of this test were amalyzed: the lift-up index, percentage of lift-up index exerted by leading leg, movement time, impact index and percentage of impact index exerted by lagging leg.. 2.4.3.1. Lift-Up Index and Percentage of Lift-up Index Exerted by Leading Leg. The lift-up index, which is provided from the PRO Balance Master®, quantifies the amount of the maximum vertical force exceeded the body weight during liftting and is expressed as a percentage of the individual’s body weight. The formula of impact index as follows:. 39.
(53) Lift - up index =. maximal vertical force - body weight × 100 % body weight. (2-5). These values indicate wheather or not sufficient force can be generated by each leg to quickly and effectively move the body over the step.. Because the lift-up. force is the summation of the lift-up force exerted by the leading leg and the push-off force exerted by the trailing leg (Figure 2-7), the percentage of exerted by leading leg was also calculated to reveal the contribution of the leading leg (Figure 2-8).. 100 90. Vertical GRF (kg). 80 70 60 50 40 Leading Leg. 30. Trailing Leg 20 10. 0. 1. 2. 3. 4. 5. 6. 7. Figure 2-7: Vertical ground reaction force of summation of both legs (solid line), the leading leg (dot-dash line) and trailing leg (dot line) in step up/over test.. Time (sec). 100 90. Total Lift-up Force. Vertical GRF (kg). 80 70 60 50. Figure 2-8: Vertical ground reaction force of summation of both legs (solid line) and the leading leg (dot-dash line) in step up/over test.. Lift-up Force on the Leading Leg. 40 30 20 10 0. 1. 2. 3. 4. 5. 6. Time (sec). 40. 7.
(54) 2.4.3.2. Movement Time. The movement time is the amount of time to complete the step over, expressed in seconds. Scoring begins with the lifting phase and ends with the impact of trailing leg onto the surface (Figure 2-9) .. Movement Time. 100. Vertical GRF (kg). 90 80 70 60 50 40 30. 0. 1. 2. 3. 4. 5. 6. 7. Figure 2-9: Vertical force in step up/over test.. Time (sec). 2.4.3.3. Impact Index and Percentage of Impact Index Exerted by Trailing Leg. Impact index, which is supplyed from the PRO Balance Master®, is the amount of the maximum vertical force exceeded body weight while the trailinging leg landing on the foot-plate, expressed as a percentage of body weight (%BW). The calculation was showed as formula 2-4. The leading leg has to switch from concentric control (lift the body) to eccentric control (lower the body) as the COG passes toward the forward limit of stability boundary while moving over the step. The amount of impact force on the trailing leg indicate the eccentric control of the 41.
(55) leadimng leg (Figure 2-9). In other words, during the affected side trial (leading with affected side), the impact force is the maximal force while sound side landing, and the maximal force while affected side landing during the sound side trial (leading with sound side).. Because the impact index is the summation of the eccentric control force on the leading leg and the maximal landing force on the trailing leg (Figure 2-7), the percentage of contribution of real impact force by landind leg was also calculated to reveal the contribution of the trailing leg (Figure 2-10).. Vertical GRF (kg). 100 90. Total Impact Force. 80. Impact Force on the Trialing Leg. 70 60 50 40 30 20 10. 0. 1. 2. 3. 4. 5. 6. Time (sec). 42. 7. Figure 2-10: Vertical ground reaction force of summation of both legs (solid line) and the trailing leg (dot line) in step up/over test..
(56) 2.4.4 Step/Quick Turn (SQT). Six measured parameters of SQT test were turn sway, initial weight shift, turn width, turn time, velocity of stepping forward and velocity of stepping back.. 2.4.4.1. Turn Sway. Turn sway, which is provided from the PRO Balance Master®, is the distance traveled by the COG (path length) during the turn, expressed in degree. Scoring begin when the forward COG progression stops, and ends when COG progression in the opposite direction starts.. 2.4.4.2. Initial Weight Shift. Initial weight shift is the amount of shifting to the leading leg at the beginning of the test. When initiating the stepping, center of pressure (COP) travels from the center of base of support (BOS) to the leading leg first (Figure 2-11) and then to the support leg (trailing leg). This value indicates wheather or not sufficient weight shitting to leading limb.. 43.
(57) 100 80. Px of COP (mm). 60 40 20 0. Initial Weight Shift Initial Weight Shift. -20. Turn Width Turn Width. -40 -60 -80 -100. 0. 1. 2. 3. 4. 5. 6. 7. 8. Figure 2-11: Medial-lateral displacement (Px) of COP in step quick turn.. Time (sec). 2.4.4.3. Turn Width. Turn width is the maximun mediolateral displacement of the COP during the turn (Figure 2-11). The calculation begins at the step before turnning and ends at the other leg takes off.. 2.4.4.4. Turn Time. Turn time is the amount of time taken to complete the 180 degree turn, expressed in seconds. Scoring begins when the forward COG progression stops, and ends when COG progression in the opposite direction starts (Figure 2-12) .. 44.
(58) 2.2.4.5 Velocity of Stepping Forward and Velocity of Stepping Backward. The velocity of stepping forward and velocity of stepping backward is the slope of step before and after turning, respectively (Figure 2-11).. Therefore, in. affected side trial (leading with affected side), sound side stepping speed before and after turning is the vlocity of stepping forward and backward, repectively. And in sound side trial (leading with sound side), affected side stepping speed before and after turning is the vlocity of stepping forward and backward, repectively.. 600 Turn Time. Py of COP (mm). 400 Velocity of Stepping Forward. 200. Velocity of Stepping Back. 0 -200 -400. Figure 2-12: Anteroposterior placement (Py) of COP in step/quick turn test. -600 -800. 0. 1. 2. 3. 4. 5. 6. Time (sec). 45. 7. 8.
(59) 2.5. Statistical Analysis. Descriptive statistics was used to exam the homogeneity of the basic characteristics between the subjects in different groups, such as body height, age and activity level…etc. and analysis of variance (ANOVA) with Tukey post-hoc testing was used to reveal the difference of dynamic functional performance between groups. A paired t-test was used to determine the difference of functional performance between involved side and uninvolved side among each group.. The statistical. significance was set at 0.05. All statistical analysis were performed using SPSS 13.0 software (Chicago, IL, USA).. 46.
(60) ChapterⅢ. Results. 3.1. Demography of the Participants. 3.1.1. Basic Data. The descriptive data of each group is shown in Table 3-1. The normal group consisted of twenty healthy individuals, 14 males and 6 females with a mean age 21.8±3.8 years. The ACLD group consisted of twenty patients with unilateral ACL rupture, 16 males and 4 females with a mean age 26.3±8.0 years. An interval of 2-60 months (mean: 20.0±22.1 months) elapsed between the episode caused the ACL rupture and the examination.. The early stage of post-ACLR (early ACLR). group comprised fifteen patients, 9 males and 6 females with a mean age 26.1±6.0 years. An interval of 3.2 months (mean: 3.2±0.4 months) elapsed between the ACL reconstruction and the examination.. The late-stage of post-ACLR (late ACLR). group comprised fifteen patients, 9 males and 3 females with a mean age 38.73±7.6 years.. An interval of 6-72 months (mean: 21.5±22.3 months) elapsed between the. ACL reconstruction and the examination.. 47.
(61) Table 3-1: The basic data of ACLD, early stage of post-ACLR, late stage of post-ACLR and normal control group Group ACLD Early stage of post-ACLR Late stage of post-ACLR Normal control a. Height (cm) 174.3±8.7 169.4±7.8 168.2±8.7 167.0±6.9 b. Weight (kg) 72.5±13.6 72.5±13.7 70.6±9.8 65.5±12.0. : P < 0.05 between the normal control and the late ACLR groups.. b. 3.1.2. Age (y/o) 26.3±8.0 26.1±6.0 28.7±7.6 21.8±3.8a. : P < 0.05 between the normal control and the ACLD groups.. Activity Level and Knee Scoring Scale. The result of Lysholm knee scoring scale and the activity level in the ACLD, early post-ACLR and late ACLR groups were showen in Table 3-2. The Lysholm knee score in the late ACLR group was significant higher than the ACLD group (P = 0.014). Activity level before the injury showed no significant difference between groups. But the recent activity level in the early ACLR was singnificant lower than those in the ACLD (P = 0.048) and late ACLR groups (P = 0.001).. Table 3-2: Lysholm Knee Scoring Scale and activity level of ACLD, early stage of post-ACLR (early ACLR) and late stage of post-ACLR (late ACLR) groups.. ACLD. Lysholm score 67.0±16.1a. Activity level (pre-injury) 87.5±16.7. Activity level (recent) 61.3±24.1. Early ACLR. 69.4±19.8. 84.0±11.5. 42.0±25.1b,c. Late ACLR. 83.4±12.4. 81.3±15.1. 76.3±17.3. Group. a. P < 0.05 between the ACLD and the late ACLR groups. b. P < 0.05 between the ACLD and the early ACLR groups. c. P < 0.05 between the early and the late ACLR groups 48.
(62) 3.2. Dynamic Functional Performance Test. The comparison of all the measured parameters between sides of the normal subjects showed no significant difference, so we pooled the results from both limbs to represent the performance of the normal group.. 3.2.1. Weight Bearing/Squat (WBS). Comparing between groups, there was no significant difference in weight bearing score in the three ACL injured and normal groups at each knee flexion angle. However, there was a significant less weight-bearing score when compared the affected side to the sound side of the ACLD group at 30°of knee flexion (P = 0.008). In the early ACLR group, weight-bearing score of affected side was also significant less than sound side at 30° (P = 0.011), 60° (P = 0.005) and 90° (P < 0.001) of knee flexion. In the late ACLR group, similar result was found significant at 90°of knee flexion (P = 0.006). (Table 3-3). 49.
(63) Table 3-3: The weight bearing score of each side in normal control, ACLD, early stage of post-ACLR (early ACLR), and late stage of post-ACLR (late ACLR) groups 0°. 30°. 60°. 90°. Left Side. 50.8±2.5. 50.4±4.1. 50.8±4.1. 51.0±3.1. Right Side. 49.2±2.6. 49.6±4.2. 49.2±4.1. 49.1±3.1. Affected Side. 49.1±3.6. 46.0±6.1†. 47.5±6.1. 47.9±7.2. Sound Side. 51.0±3.6. 54.1±6.1. 52.5±6.1. 52.1±7.2. Early ACLR. Affected Side. 49.3±3.7. 46.2±5.0†. 45.5±5.3†. 44.1±4.6†. Sound Side. 50.7±3.7. 53.8±5.0. 54.5±5.3. 56.0±4.8. Late ACLR. Affected Side. 50.6±3.3. 50.1±6.3. 48.6±5.6. 44.3±6.8†. Sound Side. 49.4±3.3. 49.9±6.3. 51.4±5.6. 55.7±6.8. Normal Control ACLD. †. : p<0.05 between the sound side and affected side. 3.2.2. Forward Lunge (FL). The lunge distance of the sound limb was larger than that of the affected limb in the ACLD group (P = 0.032), early ACLR group (P = 0.002) and late ACLR group (P = 0.026). Compared between groups, the lunge distance of the affected limb in the early ACLR group showed significant smaller than in the control normal group (P = 0.021) (Figure 3-1).. 50.
(64) Sound Side. Distance (% BH). 60. Affected Side * †. †. †. 40. 20. 0. ACLD. Early ACLR Late ACLR. N. Figure 3-1: The lunge distance of ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control (N) groups. †. : Significant difference between sides.. *: Significant difference between groups.. Significant difference for the impact index was found only in the affected side of the early ACLR group with smaller values than those of the control normal group (P = 0.021) (Figure 3-2).. ACLD. Early ACLR. Late ACLR. N. Impact index (% BW). *. 40 35 30 25 20 15 10 5 0 Sound Side. Affected Side. Figure 3-2: The impact index of ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control groups.. 51.
(65) The ACLD, early ACLR and late ACLR groups had larger lunge contact time than the normal control group regardless of the affected (P = 0.007; P = 0.001; P = 0.006, respectively) or sound side (P = 0.008; P < 0.001 and P = 0.004, respectively) (Figure 3-3).. ACLD. Contact Time (sec). 1.5. *. Early ACKR. Late ACLR *. N. 1.2 0.9 0.6 0.3 0. Sound Side Affected Side Figure 3-3: The contact time of ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control (N) groups.. The force impulse of the sound limb in the early ACLR group was significant smaller than in the normal control group (P = 0.004).. And the impulse. index of the affected side was smaller in the ACLD (P = 0.001) and early ACLR (P < 0.001) groups than in the normal control group (Figure 3-4).. 52.
(66) Force Impulse (% BW). ACLD 120. Early ACLR. Late ACLR. N. *. *. 115 110 105 100 95. Sound Side Affected Side Figure 3-4: The force impulse in ACLD, early stage of post-ACLR. (early ACLR), late stage of post- ACLR (late ACLR) and normal control (N) groups.. 3.2.3. Step Up/Over (SUO). Only seven patients in the early ACLR group could perform the step up over test with 30cm step. Six of them could only perform with 20cm step and two with 10cm in affected side trial (trial of affected side leading). Therefore, comparing the difference of the three measured parameters between groups would exclude the early stage of ACLR group. Lift-up index of the affected side trial was significant larger than the sound side trial in ACLD (P = 0.046), early ACLR (P = 0.01) and late ACLR groups (P <. 53.
(67) 0.001) (Figure 3-5). For the sound side trial, lift up index in the ACLD group was even smaller than normal control group (P = 0.006). For the affected side trial in the ACLD group, the lift up index was also smaller than the late ACLR group (P = 0.011). Sound Side. Affected Side * *. Lift-up Index (% BW). 180. †. †. †. 150 120 90 60 30 0. ACLD. Early ACLR Late ACLR. N. Figure 3-5: The lift up index of ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control groups (N). †: Significant difference between sides. *: Significant difference between groups.. In the percentage of lift-up index, the mean value in the normal control group was 37.4±3.3%.. No significant difference was found in the both ACLR. groups. In the ACLD group, the affected side trial showed significant increased compared to those in the sound side trial (p=0.046) and also to those in the normal control group (P = 0.012) (Figure 3-6).. 54.
(68) Sound Side. Percentage of Liftup Index (%). 60. Affected Side *. †. 40. 20. 0 ACLD. Early ACLR Late ACLR. N. Figure 3-6: The percentage of lift up index in ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control groups (N). †: Significant difference between sides. *: Significant difference between groups.. No significant difference in movement time was found in the comparison between sides of the late ACLR group as well as in the comparison with the other groups.. Movement time in the ACLD group was shorter than in normal control. regardless in the sound or affected side trial (P = 0.028 and P = 0.037, respectively) (Figure 3-7).. Movement Time (msec). ACLD 160. Late ACLR. N. *. *. Sound Side. Affected Side. 120 80 40 0. Figure 3-7: Movement time in ACLD, late stage of ACLR (Late ACLR) and normal control (N) groups.. 55.
(69) Impact index of the affected side trial, in which the landing leg was the sound limb, was larger than sound side trial in the early ACLR (P = 0.047) and late ACLR groups (P = 0.040). That of the affected side trial in the late ACLR group was larger than in the ACLD group (P = 0.045) (Figure 3-8). The percentage of impact index showed no significant difference between sides of each group and between groups with mean value of 62.6±4.0% in the normal control group (Table 3-4).. Impact Index (% BW). Sound Side. Affected Side. 100. * †. †. 80 60 40 20 0 ACLD. Early ACLR. Late ACLR. N. Figure 3-8: The impact force index of ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control groups. †: Significant difference between sides. *: Significant difference between groups.. Table 3-4: The percentage of impact index in ACLD, early stage of postACLR (early ACLR), late stage of post-ACLR (late ACLR) groups. ACLD Early ACLR Late ACLR Affected side trial 64.5±3.1 64.9±8.3 63.2±5.4 Sound side trial 62.2±5.9 55.6±6.9 61.2±5.3. 56.
(70) 3.2.4. Step/Quick Turn (SQT). There was no significant difference in each measured parameter between affected and sound sides of the ACL injured groups. Initial weight shift, turn width and turn sway also showed no significant difference in both limbs between groups. Turn time of the affected (P = 0.035) and sound (P = 0.026) side trials in the ACLD group were significant longer than that in the normal control group (Figure 3-9).. ACLD. Turn Time (msec). 120. Early Stage. Late Stage. N. *. *. Sound Side. Affected Side. 100 80 60 40 20 0. Figure 3-9: The turn time of ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control (N) groups.. 57.
(71) Stepping back velocity with sound side lead showed significant lower in the ACLD (P = 0.032) and early stage of ACLR (P = 0.047) groups than in the normal control group. And significant lower stepping back velocity with affected side lead showed only in ACLD (P = 0.016) group compared to the normal control group (Figure 3-10).. ACLD Step Back Velocity (m/sec). 3. Early Stage. Late Stage. N. *. *. Sound Side. Affected Side. 2.5 2 1.5 1 0.5 0. Figure 3-10: The stepping back velocity of ACLD, early stage of post-ACLR (early ACLR), late stage of post-ACLR (late ACLR) and normal control (N) groups.. 58.
(72) Chapter Ⅳ. Discussion. This study aimed to examine the changes of the dynamic functional performance in the ACLD patients, early and late stages of post-operative ACLR patients.. In the literature, the most common clinical parameter reported and. discussed after rupture or reconstruction of the ACL is the amount of tibial anterior translation. This is understandable since the ACL is the primary restrain to anterior tibial translation and the recovery of pathologic anterior tibial translation is the goal of ACL reconstructive procedures. However, the amount of anterior tibial translation after injury was not related well to the functional disability 23,66,71. Therefore, many authors assessed the functional ability in various aspects following ACL injury and reconstruction.. Two main focuses of functional assessment are on the. neuromuscular control and on the muscle strength. The ability of responding to an external disturbance with appropriate reactive forces in correct ways is important in the prevention of further injury. The functional performance tests in the present study are not the maximal tests, such as the single-hop for distance or vertical jump, and therefore could be used in the patients who are not able to perform the maximal tests. Previous studies have demonstrated that some ACLD patients can adapt well to the impairments and return. 59.
(73) to the same activity level as pre-injury (copers) while others can not (non-copers) 23,54,65. . Rudolf et al.. 63. and Barber et al.. 4. reported that the maximal tests were not. recommended in non-coper ACLD patients because the increased quadriceps activation during the tests would raise the possibility of increasing anterior tibial translation.. This same precaution must be adhered to in the early stage of. post-ACLR patients, as the excessive anterior translation can increase the stress on the fresh surgical graft and then cause damage. However, these patients would still be required to perform function tasks in their daily living, such as squat, stepping, stair climbing and turning.. 60.
數據



+7

相關文件
Late Qing Master Taixu, recognized as the leader of Buddhist reform movement, and several Buddhist intellectuals collaborated to remodel and revive Buddhist
Impact of Early Mobilization on Glycemic Control and ICU- Acquired Weakness in Critically Ill Patients Who Are Mechanically Ventilated. Am J Phys
pylori in pathogenesis of oral mucosal lesions or ulcerations is still unclear, it seems that patients with oral lesions as leukoplakia and oral lichen planus, and concurrent
Abu-Ghanem S, Yehuda M, Carmel NN, et al: Elective neck dissection vs observation in early-stage squamous cell carci- noma of the oral tongue with N0 clinically apparent lymph
However, in this case, the lesion was diagnosed as an early stage of PVL rather than linear gingival keratosis, due to the fact that it occurred in a female in the gingiva and also
These changes suggest a time-related progression of the crease-associated changes. Our data suggest a significant correlation between the morphological changes of the myocardium
The Government of Eswatini recognises that while the “big projects” will provide the much needed investment to stimulate economic activi- ties, the MSME sector has a critical role
Lemma 3 An American call or a European call on a non-dividend-paying stock is never worth less than its intrinsic value.. • An American call cannot be worth less than its
