Title: Effects of Stroke Rehabilitation on Incidence of Post-stroke Depression: A Population-based Cohort Study
Running title: Stroke Rehabilitation and Post-stroke Depression Authors’ names and affiliations:
Wen-Hsuan Hou, MD, MSc, PhD1,2; Huey-Wen Liang, MD, PhD3 ; Ching-Lin Hsieh, PhD4; Chieh-Yi Hou, MSc5; Pei-Chun Wen, DDSc6,7; Chung-Yi Li, PhD7,8
1. Department of Physical Medicine and Rehabilitation, Taipei Medical University -
Shuang Ho Hospital, New Taipei City, TAIWAN
2. School of Gerontology Health Management, College of Nursing, Taipei Medical
University, Taipei, TAIWAN
3. Department of Physical Medicine and Rehabilitation, National Taiwan University
Hospital, Taipei, TAIWAN
4. School of Occupational Therapy, College of Medicine, National Taiwan
University, Taipei, TAIWAN
5. Department of Physical Medicine and Rehabilitation, E-Da Hospital, Yan-Chau
District, Kaohsiung, TAIWAN
6. Department of Dentistry, Buddhist Dalin Tzu Chi General Hospital, Chia-Yi City,
TAIWAN
7. Department and Graduate Institute of Public Health, College of Medicine,
National Cheng Kung University, Tainan, TAIWAN
8. Department of Public Health, College of Public Health, China Medical University,
Taichung, TAIWAN
Pei-Chun Wen and Chung-Yi Li contributed to this article equally
Corresponding author:
Department of Dentistry, Buddhist Dalin Tzu Chi General Hospital No. 2. Min-Sheng Road, Dalin Town, Chia-Yi 622, TAIWAN TEL: +886-5-2648000; FAX: +886-5- 2648999
E-mail: [email protected] OR
Chung-Yi Li
Department of Public Health, College of Medicine National Cheng Kung University
No. 1, University Rd., Tainan 701, TAIWAN TEL: +886-6-2353535, FAX: +886-6-2359033 E-mail: [email protected]
Title: Effects of stroke rehabilitation on incidence of post-stroke depression: A population-based cohort study
Abstract
Objectives:
To investigate the effects of rehabilitation intervention provided within the first 3 months following stroke admission on the incidence of post-stroke depression (PSD,
ICD-9-CM code: 296, 309, 311 or A-code: A212, A219 ).
Methods:
This population-based cohort study examined medical claim data of a random sample of 1 million insured people registered in 2000 in Taiwan. Between 2000 and 2005, there were 7,677 patients admitted as first-time stroke patients. Of these patients ,
1,285 (16.7%) received a rehabilitation regimen within the first 3 months of stroke admission. The other 83.3% of patients belonged to the control group. All study subjects were followed to the end of 2009 to identify any ambulatory treatment for depression as the endpoint. The incidence density (ID) of PSD was calculated assuming a Poisson process. A Cox proportional hazard model was used to estimate the relative risk of PSD in relation to the receipt of rehabilitation.
Results: Over a 10-year follow-up, 75 (5.8%) patients with rehabilitation and 566 (8.7%) controls developed PSD, representing IDs of 11.3 and 18.5 per 1,000 person-years, respectively. After controlling for potential confounders, rehabilitation was found to significantly reduce the risk of PSD with a hazard ratio (HR) of 0.57 (95% confidence interval (CI)=0.45-0.73). The effect was greater for men (HR=0.52, 95% CI=0.37-0.71), especially for elderly men (HR=0.45), than for women (HR=0.69,
95% CI=0.47-1.02).
Conclusion: Stroke rehabilitation intervention in the first 3 months of stroke
admission may significantly reduce the risk of PSD. Although such beneficial effect appears to be greater for men than for women , c linicians should also be alert for PSD occurring in women.
Keywords:
Stroke, Rehabilitation, Post-stroke depression, Cohort study
Abbreviations:
PSD: post-stroke depression ADL: activities of daily living
NHIRD: National Health Insurance Research Database BNHI: Bureau of National Health Insurance
ACVC: ambulatory care visit claims
IEA: Inpatient Expenditures by Admissions RB: Registry for Beneficiaries
NHI: National Health Insurance
COPD: chronic obstructive pulmonary disease LOS: length of hospital stay
HR: hazard ratio
Introduction
Depression is common in stroke survivors.1 Previous studies have reported that
the prevalence of post-stroke depression (PSD) ranges from 20 to 80%, depending on the time (i.e., more prevalent within 3 months post stroke) and method of depression ascertainment,2 as well as on the levels of family functioning and social support of the
patients.3 It has been well documented that PSD may deter stroke patients from social
participation and limit their activities of daily living (ADL), leading to poor
rehabilitation outcomes, which may in turn cause poor quality of life and increase the risk of mortality in stroke survivors. Thus, in managing the recovery of stroke
survivors, it is crucial to prevent or treat depression.
Many studies have explored ways to effectively treat PSD.6-8One study
investigated whether pharmacological therapy or psychotherapy can prevent PSD.2 Despite a recent study supporting the preventive effect of antidepressants for PSD, evidence has been inconsistent with respect to the effectiveness of antidepressant
medication use and psychotherapy to improve mood and to prevent PSD. Presently, little is known about the effectiveness of stroke rehabilitation in preventing the incidence of depression in stroke survivors.
Stroke rehabilitation, defined as any treatment or exercise with the aims of facilitating neurological recovery, achieving functional recovery, minimizing daily disability, and reintegrating back in family and community,9 has been proposed as an
effective therapeutic approach for PSD in patients with stroke.10 Previous studies have
for PSD,11 suggesting that stroke rehabilitation could prevent PSD by minimizing functional impairments and enhancing participation in ADL.
The purpose of this study was to conduct a population-based cohort study to investigate the association between stroke rehabilitation and the risk of PSD onset among first-time stroke patients. In addition to assessing the overall effectiveness of stroke rehabilitation to prevent PSD onset, we also aimed to explore the age and sex-specific relationships between stroke rehabilitation and risk of depression onset in patients with stroke.
Methods
Source of data
The data were collected from the claims of 1 million beneficiaries randomly selected from all beneficiaries insured in 2000, with age and sex distributions nearly identical to the entire insured population of Taiwan.12 The claims were retrieved from
the National Health Insurance Research Database (NHIRD) of the Bureau of National Health Insurance (BNHI). The NHIRD provides all inpatient and ambulatory medical claims for around 99% of the Taiwanese people.13 To ensure the accuracy of the claim
files, the BNHI performs quarterly expert reviews on a random sample for every 50 to 100 ambulatory and inpatient claims.14 Therefore, information obtained from the
NHIRD is considered to be complete and accurate.15 We used several NHIRD datasets
in this study, including ambulatory care visit claims (ACVC), Inpatient Expenditures by Admissions (IEA), and the Registry for Beneficiaries (RB). Access to the research data was approved by the Review Committee of the National Health Research
Institutes.
Study subjects and end-points
The IEA claims showed that between 2000 and 2005, a total of 15,580 patients were admitted for a principal or secondary diagnosis of stroke (ICD-9-CM code: 430-434, 436-437). After the exclusion of 1,930 patients who were admitted or had sought ambulatory service for stroke in 1997-1999, the remaining 13,650 patients were considered as the incident cases of stroke for the years 2000-2005. We further excluded 2,086 patients who had ambulatory care visits for depression (ICD-9-CM code: 296, 309, 311 or A-code: A212, A219) between January 1st 1997 and date of
admission for first-time stroke attack (i.e., the index date ) . There were 2,222 patients who sought ambulatory care for depression within the first 3 months of stroke attack, and there were 1,575 patients who died in hospital or withdrew (including death) from the National Health Insurance (NHI) program within the first 3 months after stroke attack. These patients were also excluded, leaving 7,767 patients in the study. Patients who were not followed for a full 3 months after discharge were excluded because the stroke rehabilitation program is considered most effective within the first 3 months after the stroke attack.16 The annual numbers of stroke incident cases from 2000 to
2005 were 1,401, 1,338, 1,348, 1,165, 1,305, and 1,210, respectively.
We linked the cohort of stroke patients to the ACVC and searched for their rehabilitation visits within the 3-month period following the stroke attack, finding a total of 8,288 rehabilitation visits by 1,285 stroke patients. Information on receipt of stroke rehabilitation was based on the treatment code of NHI claims. Fundamentally, the r ehabilitation orders include facilitation of hemiplegic limbs, muscle
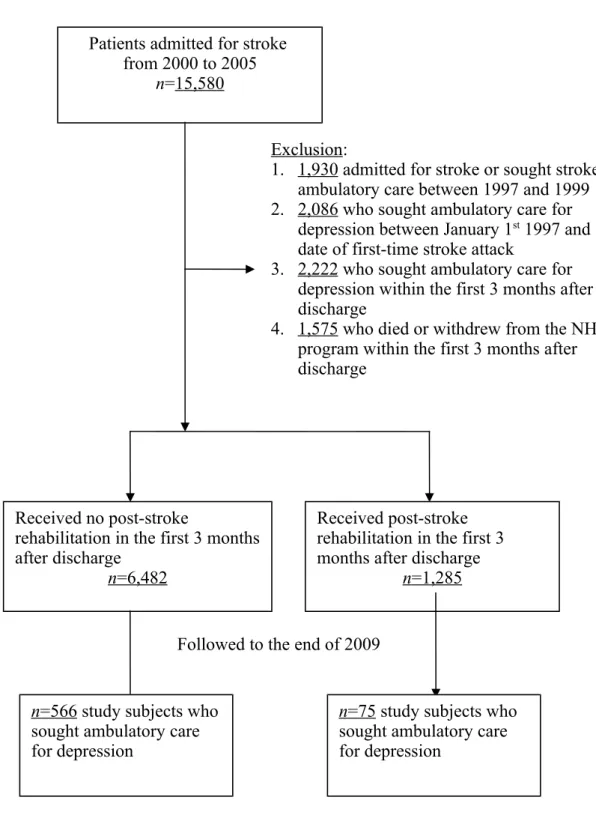
strengthening, moving, activities of daily living, ambulation, and balance training to achieve functional improvement. 17 It was found that 83% (n=6,482) of the patients received no post-stroke rehabilitation. The patients of both groups (i.e., rehabilitation and non-rehabilitation) were linked to the ACVC and IEA in the years 2000-2009 to identify possible treatment for depression. A flow chart showing the study criteria, the exclusion criteria, and the follow-up procedure is presented in Figure 1.
Statistical analysis
The index date for each stroke patient was the date of discharge after his/her first stroke attack. The 10-year follow-up period began as early as on January 1, 2000, and ended on December 31, 2009. The age of each patient was calculated as the difference
in time between the index date and the date of birth. The insurance premium for each beneficiary with the NHI was proportional to his/her wages. A higher premium is indicative of higher wages. For those who were not actively employed or were self-employed, the insurance premium was zero. We grouped the patients’ residential areas into three urbanization levels (i.e., urban area, satellite city, and rural area) according to the National Statistics of Regional Standard Classification.18 The
information on insurance premiums and residential areas was obtained from the RB.
The age- and sex-specific hazard rates were determined with person-years as the denominator under the Poisson assumption. To assess the independent effects of stroke rehabilitation on the risk of depression, we conducted a Cox proportional hazard regression analysis with age, sex, insurance premium, urbanization level, and selected comorbidities adjusted simultaneously in the model. We adjusted the urbanization level for the presence of an urban-rural difference in accessibility to medical care in Taiwan.19 The comorbidities considered in our analysis included a
number of major illnesses, including cancer (ICD-9-CM code: 140-208), arthritis or rheumatism (ICD-9-CM code: 714.0, 729.0), chronic obstructive pulmonary disease (COPD) (ICD-9-CM code: 490-496), peripheral arterial disease (ICD-9-CM code: 440-449), and diabetes mellitus (ICD-9-CM code: 250), which were found to pose a significantly increased risk of depressive symptoms.20 The above comorbidities were
identified from the study subject’s AVCV or IEA claims in the one-year period prior to the stroke attack. Type of stroke (i.e., ischemic or hemorrhagic stroke) and length of hospital stay (LOS) associated with the index stroke admission were also
considered as covariates. The follow-up ended on the date of diagnosis of depression in either inpatient or outpatient care, or on the date of censoring, which was the either date of withdrawal (including death) from the NHI program or date of
end-of-follow-up, i.e., December, 31st, 2009. All statistical analyses were performed using SAS
(version 9.3; SAS Institute, Cary, NC) and Stata/SE 12.0 for Windows (StataCorp, College Station, TX). A P-value <0.05 was considered statistically significant.
Results
The stroke patients who received rehabilitation were more likely (63.3%) to be male and, on average, 2.3 years younger than those without rehabilitation. Both groups were comparable with respect to insurance premium and residential
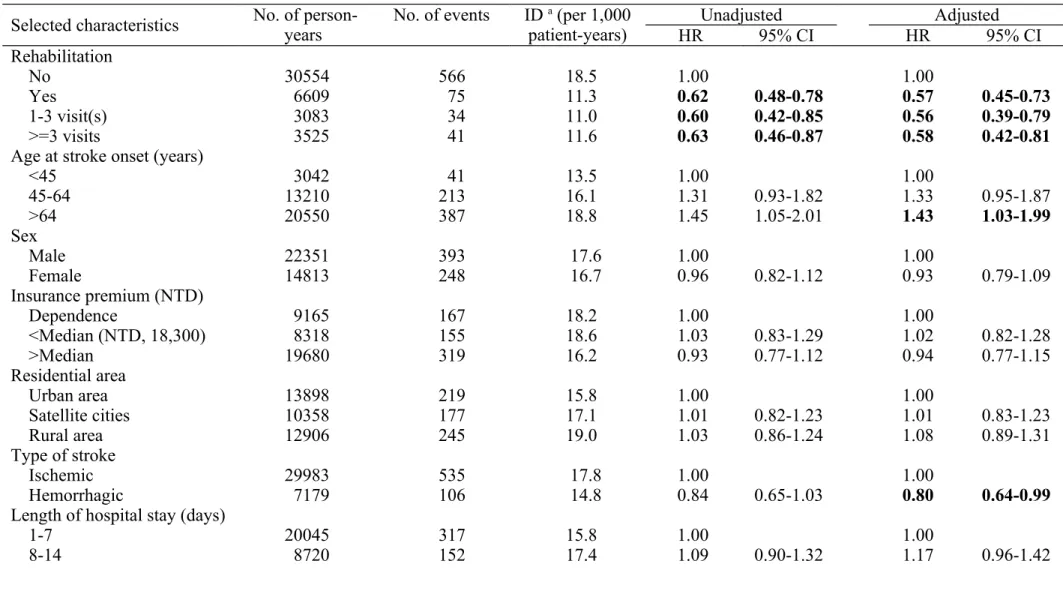
urbanization level. The patients with stroke rehabilitation tended to suffer from lesser major illnesses prior to the stroke attack (Table 1). After controlling for potential confounders (e.g., age, sex, insurance premium, residential area, type of stroke, length of hospital stay, and major illness related depression), stroke rehabilitation
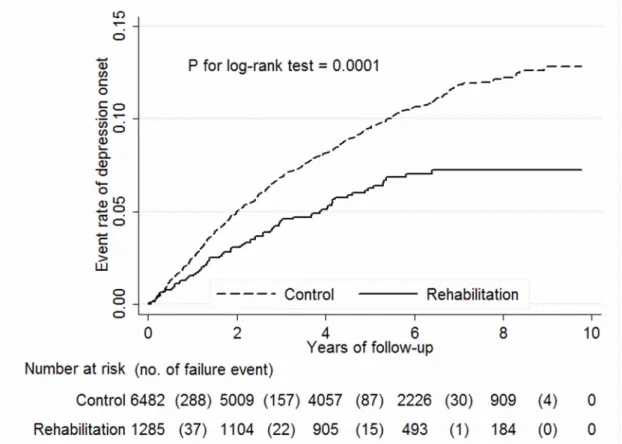
significantly and substantially reduced the risk of depression, with a hazard ratio (HR) of 0.57 (95% confidence interval (CI) of 0.45-0.73). The HRs remained unchanged when frequency of rehabilitation was taken into account. The multivariate analysis also showed that older stroke patients tended to be at significantly greater risk of depression after stroke rehabilitation (HR=1.43, 95% CI=1.03-1.99) than younger patients. Additionally, stroke patients with an LOS of 22-28 days and those with an LOS of >28 days had significantly higher HRs, 1.64 (95% CI=1.17-2.28) and 1.56 (95% CI=1.19-2.04), respectively (Table 2), than did those with an LOS of 1-7 days. Figure 2 compares the cumulative failure (event) rates of depression for the group receiving rehabilitation and the group without intervention, respectively. The patients receiving stroke rehabilitation had a significantly lower event rate over the study period (p-value for log-rank test=0.0001).
The sex- and age-specific analyses showed that men who received stroke rehabilitation had a lower incidence density of PSD than their non-rehabilitation counterparts (10.5 vs 19.2 per 1,000 person-years), representing a covariate adjusted HR of 0.52 (95% CI=0.37-0.71). A reduced HR was observed in elderly patients
(>=65 years) (HR=0.45, 95% CI=0.28-0.71) from the age-stratified analysis. On the other hand, the beneficial effect of stroke rehabilitation on PSD was less clear for female patients. Stroke rehabilitation was also associated with a reduced though statistically insignificant HR (0.69, 95% CI=0.47-1.02) in female patients, and the corresponding HR estimates for younger and elderly women were also insignificantly reduced at 0.64 (95% CI=0.33-1.23) and 0.70 (95% CI=0.43-1.13), respectively (Table 3).
Discussion
This 10-year follow-up, population-based cohort study examined whether early stroke rehabilitation could lower the risk of PSD onset in first-attack stroke patients. The magnitude of overall risk reduction was estimated at about 43%, higher for men (48%) than for women (31%). For male patients, the study found a more noticeable beneficial effect in elderly patients (55%) than in younger ones (40%). The
corresponding estimates for females were 36% and 30%, respectively.
P revious studies have documented that various types of phamarcotherapy ( e.g., antidepressants, psychostimulants, and microcirculation improvers), psychotherapy, electroconvulsive therapy, or repetitive transcranial magnetic stimulation could be effective for treating PSD.21More recently the therapeutic effects of exercise training
and rehabilitation programs for PSD have been reported. One systematic review concluded that physical exercise reduces depressive mood status, that community-based rehabilitation programs enhance health-related quality of life (HRQoL), a broad multidimensional concept that usually includes self-reported measures of physical and mental health , 23 and that leisure rehabilitation may improve HRQoL and/or
participation. Unfortunately, there were numerous inconsistencies in the protocols, types, durations, frequencies, and intensities of the rehabilitation programs.23 To the
best of our knowledge, our study is the first to examine the effect of stroke
rehabilitation within 3 months post admission in preventing the occurrence of PSD. Several mechanisms have been proposed to explain the positive link between physical exercise, an integral part of rehabilitation programs, and well-being, a subjectively perceived quality of one ’ s live including both emotional reactions and cognitive judgments . 28-29 Physiological explanations include an increase in the
concentrations of circulating beta-endophins and monoamines, and an increase in body temperature and fitness level.24 Psychological benefits were achieved after a
short period of time and even after aerobic or Tai-Chi training, suggesting that increases in fitness level may improve psychological well-being. Biological changes, together with the relief of somatic symptoms, may also lead to better physical
function and HRQoL. As for the social aspect, rehabilitation could directly improve physical function and reduce the likelihood of disability, which may adversely affect mood. Therefore, rehabilitation may delay or prevent the onset of depression by improving physical function and imparting independence.26 Previous studies have also
reported that both aerobic and anaerobic exercise may be used to treat depression.27
Others have addressed a dose-gradient effect (e.g., high-intensity vs. lower intensity) of physical activities on outcomes of depression. Furthermore, frequent and regular, but not too frequent, daily exercise has been found to be associated with low
depression scores.30
Our study results supported previous findings that a higher prevalence of PSD is associated with older age,31 longer hospital stays,32 poorer physical function, and
increased stroke severity.35 Our data showed that patients with ischemic stroke are
more prone to PSD, mainly due to the fact that ischemic insults can directly and heavily damage cortical and subcortical circuits.36 Contrary to a systematic review
indicating that PSD appears to be slightly more common in women than in men,32 our
data showed the reverse to be true, but the difference was not statistically significant. Although the age- and sex-specific differences in PSD incidence or prevalence have been frequently documented in previous studies, there is limited information on age- and sex-specific differences for stroke patients in response to prevention or treatment of PSD.32 Our study showed that elderly men benefited the most from stroke
rehabilitation in preventing PSD onset. Similar findings were also noted in a
community-based study that also noted that men and elderly (aged > 75 y/o) patients had fewer poor outcomes during treatment and rehabilitation in stroke units.37
Explanations for the age difference in the response to the preventive effect of rehabilitation could be that younger patients were relatively few in number and that their rates of developing adverse outcomes were somewhat lower than those of elderly patients.37 Additionally, some evidence supports the notion that the beneficial effect of
rehabilitation on reduced PSD is inter-mediated by the increasing physical independence and decreasing emotional distress or the social isolation of stroke patients. Previous studies found that the male gender and older age were associated with an increased risk of loss on ADL.38 In addition, Neri et al., who surveyed 176
elderly people who had cared for a spouse and/or parents in the past 5 years, found that being male is a risk factor for social isolation indicated by discontinuity of activities and social roles.39 It is likely that elderly men with stroke are more
vulnerable than other stroke patients to an increased risk of ADL disability and limited social participation. This may explain why the elderly male stroke patients benefited the most from rehabilitation, which may effectively have increased their physical independence and lifted barriers to social participation.
This study had the following strengths. First, it was a population-based study including a highly representative sample of stroke patients admitted to hospitals in Taiwan in the year 2000. Therefore, the data allow little room for selection bias. Second, the advantage of using insurance claim datasets in clinical research is that doing so provides easy access to longitudinal records for a large sample of
demographically disperse patients. The size of the dataset made it possible to conduct stratified analyses according to certain variables of interest, such as age and sex.
Third, this stroke cohort was collected from the NHI database, and all the research information was retrieved from the NHI claims, which entails little likelihood of non-response or loss to follow-up of the cohort members. Fourth, we managed to adjust, in multivariate regression models, for a number of socio-demographic variables, several major co-morbidities, and stroke severity indicators (i.e., stroke type and LOS) that are considered to be potential confounders. This approach may help elucidate the independent effect of stroke rehabilitation on the risk of depression onset.
Several limitations of our study should be noted. First, exclusive reliance on claim data may have resulted in a potential disease misclassification bias. The incidence of depression estimated from claim data could be biased estimated because some people who suffer from depression seek no ambulatory care. Similarly, some people might erroneously receive a depression diagnosis simply because of their increased
interaction with the healthcare system due to their stroke condition, i.e., surveillance bias
. To address this concern, we calculated the number of outpatient visit within the period between index date (i.e., date of stroke admission) and date of depression diagnosis or date of end-of-follow-up for each study participant . The mean+/-SD number of ambulatory care visit for rehabilitation and non-rehabilitation group was 18.48+/-29.64 per person-year (range: 1-120) and 19.42+/-31.97 per person-year (range: 0-92), respectively. We further included the number of ambulatory care visit in the multivariate Cox regression model to assess whether it poses influence on the relative risk estimates of depression in relation to rehabilitation . The re-analytical results are shown below. It is expected to find that a greater number of ambulatory care visit is positively and significantly associated with an increased risk of
depression (adjusted HR=1.09, 95% CI=1.08-1.09). However, adjustment for number of ambulatory care visit does not alter the strength of association between
rehabilitation and risk of depression.Second, because the validity of depression diagnosis is essential to the study results, w e performed a sensitivity analysis that limited the depressive subjects diagnosed by psychiatrists. We noted that 65 (86.7%) out of 75 depressive subjects from rehabilitation group were diagnosed by
psychiatrists while only 68.4% (387/566) of the depressive subjects from non-rehabilitation group fit the same criteria. The re-analytical results indicated that the protective effect of rehabilitation somewhat attenuated but still statistically significant (HR=0.72, 95% CI=0.55-0.95). The rehabilitation intensity specific HRs were also attenuated at 0.76 (95% CI=0.54-1.07) (1-3 visits) and 0.69 (95% CI=0.46-1.01) (>=3 visits), which were became insignificant partly because of reduced sample size of patients with depression.
Third, we were unable to take into account a comprehensive list of potential confounders in the analysis, which might also have resulted in residual confounding in our study. The unadjusted potential confounders may include certain socio-economic factors (including family support and financial condition) and healthy lifestyles (such as physical and leisure time activities), since accessibility,42 financial
condition,43 family or friends support,44 socioeconomic status,45 and geographic
region46 cause variations in the utilization of rehabilitation services and the PSD
prevalence. Stroke severity is among the potential confounders strongly related to the risk of depression onset. Because information on stroke severity is not available from the NHI claims, we managed to adjust for it by using LOS associated with the first-time admission for stroke as a proxy. We also noted strong associations of LOS with drug and surgery fees. To address this concern, we adjusted for the urbanization level of each patient’s residential area. Fourth, our study might suffer from potential confounding by indication, indicating that stroke patients who received rehabilitation
were involved with certain indications related patients and hospitals. To address this potential problem, we calculated, for each study patient, t he propensity score based on the variables available from the NHI claims including a patient ’ s age, sex, insurance premium, residential area, type of stroke, and co-morbidity as well as hospital accreditation level. The mean+/- standard deviation (SD) propensity score calculated for the rehabilitation and non-rehabilitation group was 0.077+/-0.027 (range: 0.043-0.204) and 0.084+/-0.031 (range: 0.040-0.224), respectively. We further included the propensity score in the multivariate Cox regression model to adjust for such potential confounding by indication. The estimated HR associated with rehabilitation was slightly reduced (0.62, 95% CI=0.49-0.80) , but remained significant statistically. Fifth, our data showed that 965 control patients (14.8%) did receive rehabilitation after 3 months of stroke attack (i.e., late rehabilitation), suggesting a potential for exposure contamination. We conducted a sensitivity analysis by excluding the patients with late rehabilitation from the control group; and the re-analysis yielded essentially the same results. Sixth, we e xclud ed those who died early or withdrew from NHI within 3 months post stroke for analyses. Those who died early may accompany more severe comorbidities or with more severe neurologic complications. S
ince this study did not include those who died early after stroke, the beneficial effect of stroke rehabilitation for these patients could not be evaluated.
Seventh, this cohort study was involved with a long-term follow-up. It is likely that the stroke patients who died earlier may have smaller chance of developing depression. To address this potential source of bias, we treated “ mortality ” as a competing-risks event and performed survival analysis with competing-risks
regression model. We noted that 176 patients (176/1285=13.7%) from rehabilitation group who did not encounter any depression diagnosis and died during the follow-up
period. The corresponding figures for non-rehabilitation group was 1015
(1015/6483=15.7%). The re-analytical results that took into account mortality as a competing-risks event were essentially the same as those reported from the original analysis. Lastly , because we retrieved all patients who had visited rehabilitation within the 3-month period following the stroke attack from the NHI claim data, there was great diversity in the stroke rehabilitation techniques, protocols, durations, frequencies, and periods between different therapists, clinics or hospitals, which led to heterogeneous effects of stroke rehabilitation. Therefore, further studies to quantify and qualify the dose-response effects and causal relationships of stroke rehabilitation to prevent PSD are needed.
In conclusion, this large cohort study demonstrated a beneficial effect of rehabilitation on the risk of depression onset in patients with stroke. Findings from this study may have important clinical implications because comprehensive evidence has shown that patients with stroke may be at higher risk of depression, a debilitating illness that can lead to early death.41 We recommend that clinicians inform stroke
patients and their families or care givers of the effectiveness of timely rehabilitation programs, and that health policy makers consider setting clinical guidelines that make rehabilitation mandatory. Another limitation is that although the NHI coverage may successfully remove financial barriers of access to treatment for patients who suffer from stroke, future studies should be conducted to further identify the non-financial factors that prevent stroke patients from receiving rehabilitation. Meanwhile,
clinicians should also pay additional attention to the mental health of stroke patients who are unable to receive rehabilitation.
Acknowledgment:
This study was supported by research grants from the National Scientific Council (grant number: 101-2314-B-006 -076 -MY3), Taipei Medical University (grant number: TMU101-AE1-B21), and The E-Da Hospital (grant number: EDAHT-101010).
Clinical Points
-
Post-stroke depression increased morbidity and mortality in stroke survivors. -
This study provides evidence that best supports the protective effect of stroke rehabilitation intervention on depression incidence.
-
The stroke rehabilitation intervention appears to be effective in patients with all age and sex stratifications, with stronger protective effect noted in male patients.
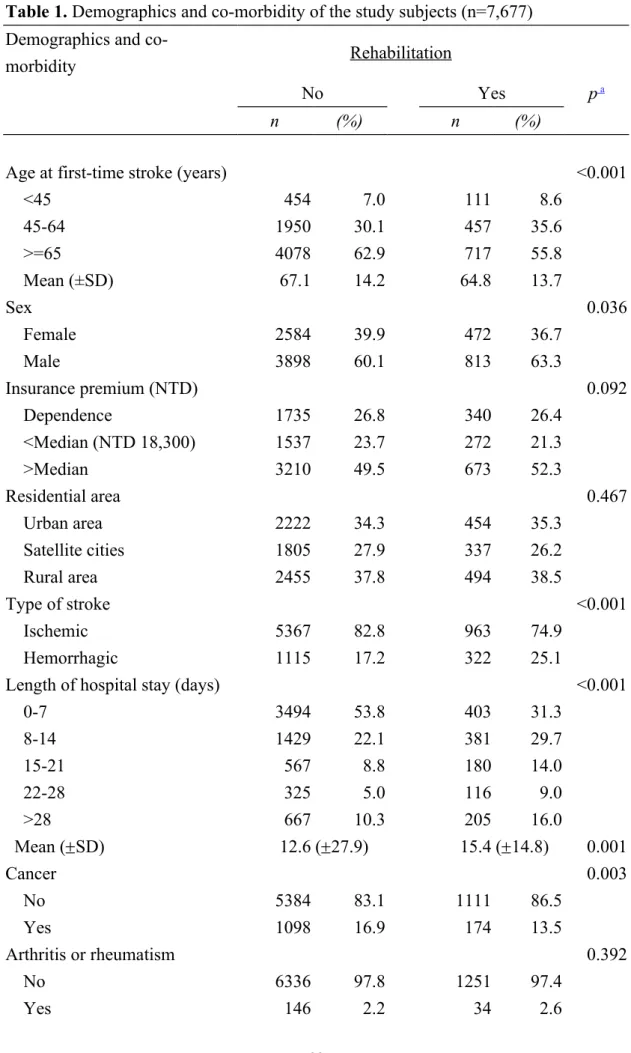
Table 1. Demographics and co-morbidity of the study subjects (n=7,677) Demographics and
co-morbidity Rehabilitation
No Yes p a
n (%) n (%)
Age at first-time stroke (years) <0.001
<45 454 7.0 111 8.6 45-64 1950 30.1 457 35.6 >=65 4078 62.9 717 55.8 Mean (±SD) 67.1 14.2 64.8 13.7 Sex 0.036 Female 2584 39.9 472 36.7 Male 3898 60.1 813 63.3 Insurance premium (NTD) 0.092 Dependence 1735 26.8 340 26.4 <Median (NTD 18,300) 1537 23.7 272 21.3 >Median 3210 49.5 673 52.3 Residential area 0.467 Urban area 2222 34.3 454 35.3 Satellite cities 1805 27.9 337 26.2 Rural area 2455 37.8 494 38.5 Type of stroke <0.001 Ischemic 5367 82.8 963 74.9 Hemorrhagic 1115 17.2 322 25.1
Length of hospital stay (days) <0.001
0-7 3494 53.8 403 31.3 8-14 1429 22.1 381 29.7 15-21 567 8.8 180 14.0 22-28 325 5.0 116 9.0 >28 667 10.3 205 16.0 Mean (SD) 12.6 (27.9) 15.4 (14.8) 0.001 Cancer 0.003 No 5384 83.1 1111 86.5 Yes 1098 16.9 174 13.5 Arthritis or rheumatism 0.392 No 6336 97.8 1251 97.4 Yes 146 2.2 34 2.6
COPD 0.051
No 4333 66.9 895 69.7
Yes 2149 33.1 390 30.3
Peripheral arterial disease 0.103
No 5880 90.7 1184 92.1 Yes 602 9.3 101 7.9 Diabetes 0.072 No 4035 62.25 834 64.90 Yes 2447 37.75 451 35.10 Total 6,482 (100%) 1,285 (100%)
Abbreviations: SD, standard deviation; NTD, New Taiwan Dollars (1 USD ≒ 30 NTD); COPD, chronic obstructive pulmonary disease
a
Table 2. Hazard ratio of depression in relation to post-stroke rehabilitation and selected covariates.
Selected characteristics No. of person-years No. of events ID patient-years)a (per 1,000 HR Unadjusted95% CI HRAdjusted95% CI Rehabilitation
No 30554 566 18.5 1.00 1.00
Yes 6609 75 11.3 0.62 0.48-0.78 0.57 0.45-0.73
1-3 visit(s) 3083 34 11.0 0.60 0.42-0.85 0.56 0.39-0.79
>=3 visits 3525 41 11.6 0.63 0.46-0.87 0.58 0.42-0.81
Age at stroke onset (years)
<45 3042 41 13.5 1.00 1.00 45-64 13210 213 16.1 1.31 0.93-1.82 1.33 0.95-1.87 >64 20550 387 18.8 1.45 1.05-2.01 1.43 1.03-1.99 Sex Male 22351 393 17.6 1.00 1.00 Female 14813 248 16.7 0.96 0.82-1.12 0.93 0.79-1.09 Insurance premium (NTD) Dependence 9165 167 18.2 1.00 1.00 <Median (NTD, 18,300) 8318 155 18.6 1.03 0.83-1.29 1.02 0.82-1.28 >Median 19680 319 16.2 0.93 0.77-1.12 0.94 0.77-1.15 Residential area Urban area 13898 219 15.8 1.00 1.00 Satellite cities 10358 177 17.1 1.01 0.82-1.23 1.01 0.83-1.23 Rural area 12906 245 19.0 1.03 0.86-1.24 1.08 0.89-1.31 Type of stroke Ischemic 29983 535 17.8 1.00 1.00 Hemorrhagic 7179 106 14.8 0.84 0.65-1.03 0.80 0.64-0.99
Length of hospital stay (days)
1-7 20045 317 15.8 1.00 1.00
15-21 3257 60 18.4 1.13 0.86-1.49 1.30 0.98-1.72
22-28 1800 41 22.8 1.39 1.01-1.92 1.64 1.17-2.28
>28 3342 71 21.2 1.30 1.01-1.68 1.56 1.19-2.04
History of major illnesses Cancer No 31640 542 17.1 1.00 1.00 Yes 5524 99 17.9 1.04 0.84-1.29 1.01 0.82-1.26 Arthritis or rheumatism No 36356 621 17.1 1.00 1.00 Yes 807 20 24.8 1.44 0.92-2.25 1.44 0.92-2.25 COPD No 26406 452 17.1 1.00 1.00 Yes 10758 189 17.6 1.00 0.84-1.18 0.93 0.78-1.11
Peripheral arterial disease
No 34010 591 17.4 1.00 1.00 Yes 3154 50 15.9 0.91 0.68-1.21 0.93 0.78-1.11 Diabetes No 22769 411 18.1 1.00 1.00 Yes 14394 230 16.0 0.95 0.80-1.11 0.94 0.79-1.10 Overall 37163 641 17.2
Abbreviations : ID, incidence density ; HR, hazard ratio; CI, confidence interval; NTD, N ew Taiwan D ollars ; COPD, chronic obstructive pulmonary disease
a
Table 3. Overall and age- and sex-specific incidence densities and relative hazards of depression in stroke patients with and without rehabilitation
Variables Non-rehabilitation Rehabilitation HR (95% CI) in
association with rehabilitation AHR b (95% CI) in association with rehabilitation No. of
subjects No. ofevents patient-years)ID (per 1,000 subjectsNo. of No. ofevents ID
a (per 1,000 patient-years) Men <65 1,575 141 16.3 398 24 10.6 0.65 (0.42-1.01) 0.60 (0.38-0.93) >=65 2,323 208 21.8 415 20 10.4 0.48 (0.31-0.77) 0.45 (0.28-0.71) Total 3,898 349 19.2 813 44 10.5 0.55 (0.41-0.76) 0.52 (0.37-0.71) Women <65 829 78 16.5 170 11 11.3 0.67 (0.36-1.27) 0.64 (0.33-1.23) >=65 1,755 139 18.2 302 20 13.7 0.76 (0.47-1.21) 0.70 (0.43-1.13) Total 2,584 217 17.5 472 31 12.7 0.73 (0.50-1.06) 0.69 (0.47-1.02) Overall 6,482 566 18.5 1,285 75 11.3 0.62 (0.48-0.78) 0.57 (0.45-0.73)
Abbreviations : ID, incidence density; CI, confidence interval; HR, hazard ratio; AHR, adjusted hazard ratio.
a Based on Poisson assumption
b Based on Cox proportional hazard regression with adjustment for age, sex, insurance premium, residential area, type of stroke, length of
hospital stay, and selected major illnesses related depression including cancer, arthritis/rheumatism, COPD, peripheral arterial disease, and diabetes.
Figure 1. Flow chart of study subjects’ selection and follow-up Patients admitted for stroke
from 2000 to 2005 n=15,580
Exclusion:
1. 1,930 admitted for stroke or sought stroke ambulatory care between 1997 and 1999 2. 2,086 who sought ambulatory care for
depression between January 1st 1997 and
date of first-time stroke attack
3. 2,222 who sought ambulatory care for depression within the first 3 months after discharge
4. 1,575 who died or withdrew from the NHI program within the first 3 months after discharge
Received no post-stroke
rehabilitation in the first 3 months after discharge
n =6,482
Received post-stroke rehabilitation in the first 3 months after discharge
n =1,285
Followed to the end of 2009
n =566 study subjects who sought ambulatory care for depression
n =75 study subjects who sought ambulatory care for depression
Figure 2. Comparison of Kaplan-Meier failure estimates of depression onset between the two study groups