•
BRIEF REPORTS•
Post-radiation survival time in hepatocellular carcinoma based
on predictors for CT-determined, transarterial embolization and
various other parameters
Ting-Kai Leung, Chi-Ming Lee, Li-Kuo Shen, Hsi-Chi Chen, Yu-Cheng Kuo, Jeng-Fong Chiou E L S E V I E R
PO Box 2345, Beijing 100023, China World J Gastroenterol 2005;11(11):1697-1699 www.wjgnet.com World Journal of Gastroenterology ISSN 1007-9327 wjg@wjgnet.com © 2005 The WJG Press and Elsevier Inc. All rights reserved.
Ting-Kai Leung, Chi-Ming Lee, Li-Kuo Shen, Hsi-Chi Chen,
Department of Diagnostic Radiology, Taipei Medical University Hospital, Taipei, Taiwan, China
Yu-Cheng Kuo, Jeng-Fong Chiou,Department of Radiation Oncology, Taipei Medical University Hospital and Wan Fang Hospital, Taipei, Taiwan, China
Correspondence to: Chi-Ming Lee, M.D., Department of Diagnostic
Radiology, Taipei Medical University Hospital, Wu-Hsin Street 250, Taipei, Taiwan, China. vd142098@yahoo.com.tw
Telephone: +886-2-27372181-1131 Fax: +886-2-23780943 Received: 2004-08-13 Accepted: 2004-09-30 A b s t r a c t A b s t r a c t A b s t r a c t A b s t r a c t A b s t r a c t
AIM: In this retrospective study of unresectable hepatocellular carcinoma (HCC), we have investigated the efficacy of CT-derived parameters, laboratory measurements, clinical assessment and associated transarterial embolization (TAE) as predictors of post-radiotherapy survival time. METHODS: Sixty-six patients diagnosed with unresectable HCC that had undergone radiotherapy at two medical university hospitals in Taipei were enrolled in the study. Using multivariant analysis, pre-treatment parameters including tumor number and CT confirmation of PVT and ascites were compared. Multivariant analysis was also used for comparison of the mean pretreatment values for laboratory measurements, including alpha-fetoprotein, direct/total bilirubin and GOT/GPT levels, and clinical history of chronic hepatitis across the three survival-time categories. The χ2 was used to test the significance of the relationship between survival time and TAE procedure. The P values for the above tests were deemed statistically significant where P<0.05.
RESULTS: Portal vein thrombosis (P = 0.032) and ascites (P<0.05) were negative predictors of post-radiation survival time. Low-grade liver cirrhosis (A or B), lower tumor volume and low levels of AFT, GOT/GPT, and total bilirubin were predictors of longer post-radiation survival time (P<0.05).
CONCLUSION: The CT and clinical and laboratory assessment provide a reference for, and enable estimation of, probable survival times in HCC patients after radiotherapy. Tumor volume, severity of liver cirrhosis, status with respect to portal vein thrombosis and ascites and AFT, GOT/GPT and total bilirubin values were significant predictors of survival in this study.
© 2005 The WJG Press and Elsevier Inc. All rights reserved.
Key words: Hepatocellular carcinoma; HCC; Radiotherapy; CT-determined parameters; Transarterial embolization; Post-radiation survival time
Leung TK, Lee CM, Shen LK, Chen HC, Kuo YC, Chiou JF. Post-radiation survival time in hepatocellular carcinoma based on predictors for CT-determined, transarterial embolization and various other parameters. World J Gastroenterol 2005; 11(11): 1697-1699 http://www.wjgnet.com/1007-9327/11/1697.asp INTRODUCTION INTRODUCTION INTRODUCTION INTRODUCTION INTRODUCTION
Radiotherapy treatment for hepatocellular carcinoma (HCC)[1] is still considered unorthodox in Taiwan. However, there has been a trend towards increased utilization in unresectable and TAE-nonsusceptible cases.
In this study, we share our experience over the past six years with HCC irradiation to provide a reference for prediction of survival time based on clinical, laboratory, and image-derived information[2], and particularly to discuss the value of pre-TAE treatment.
We also compared our results with those of other analogous research[1].
MA MA MA MA
MATERIALS AND METHODSTERIALS AND METHODSTERIALS AND METHODSTERIALS AND METHODSTERIALS AND METHODS
Patients
From June 1998 to June 2004, radiotherapy for a total of 66 patients diagnosed with unresectable HCC was performed at Taipei Medical University Hospital (TMUH) and Taipei Wan-Fang Hospital (TWH).
The mean age for the 35 male (53%) and 31 female (47%) patients was 58 years. Diagnosis was based on cytology, high serum alpha-fetoprotein and image findings characteristic of malignancy (including angiography and CT follow-up).
Various factors were considered, including: laboratory data for alpha-fetoprotein, total bilirubin, and GOT/GPT; tumor number and volume and existence of portal vein thrombosis (PVT) and ascites, based on pre-treatment CT; clinical grade of liver cirrhosis (Child’s A, B, C); history of chronic hepatitis; and status for the associated therapeutic factor, transarterial embolization (TAE).
1698 ISSN 1007-9327 CN 14-1219/ R World J Gastroenterol March 21, 2005 Volume 11 Number 11
performed, and the following parameters recorded: tumor number and volume (as described below), and presence of PVT or ascites.
VARIAN Eclipse 7.1.35.7 software (Integrated Treatment Planning System) was used for CT-based measurement of tumor volume, with the images made available on a large screen monitor. The distance-reference line on the CT images was used to calculate the pixel size. The tumor outlines were traced manually on the screen using a mouse-controlled cursor. Tumor volume was calculated by multiplying the sum of the traced areas by the image reconstruction interval (summation-of-areas technique). All three-dimensional reformation volumes were calculated in milliliters.
The patients were treated using limited-field radiotherapy mostly irradiated with daily fractions of 180/250 cGy to a total dose of 5 000 cGy.
Survival time after radiation was divided into three categories: (1) 6 mo; (2) 6-24 mo; (3) >24 mo; with these considered dependent variables. Other variables included PVT, ascites, hepatitis, liver cirrhosis (A, B or C) and tumor number (n = 1, 2, or >2) with multivariant analysis used to determine statistical significance as independent predictors where P<0.05. Mean AFP, tumor size, and GOT/GPT and total bilirubin [Bili(T)] levels were compared for each of the three survival categories, with multivariant analysis used to verify statistical significance as independent predictors where P<0.05.
Statistical significance was also determined for the associated therapeutic factor, TAE, for the three survival-time categories. The significance of the relationship between TAE and survival time was evaluated using the χ2 (P<0.05).
RESUL RESUL RESUL RESUL RESULTSTSTSTSTS
The overall survival rates for the 66 irradiation patients[3] for <6, 6-24 and >24 mo were 18%, 32% and 50% respectively. Of these 66 cases: 46 (70%) involved single lesions detected by pre-treatment spiral CT; 12 patients (18%) had two visible tumors; and, 8 individuals (12%) had multiple or diffuse lesions. Tumor volumes ranged from 4-1 948 mL. Pre-treatment CT scan was used for 16 (24%)
and 29 instances (44%) of portal vein thrombosis and ascites respectively (Table 1).
The clinical assessments and grading for the liver cirrhoses are presented in Table 2. A total of 40 cases (61%) were associated with TAE treatment[4] before or during radiation therapy[5].
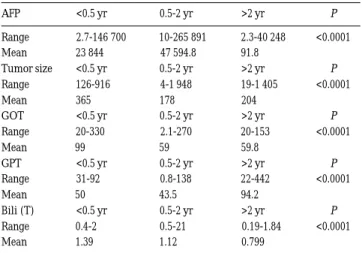
The pre-treatment laboratory data for alpha-fetoprotein, direct/total bilirubin, GOT/GPT and clinical history of chronic hepatitis are presented in Tables 2, 3.
We found that, for our sample, PVT[6] (P = 0.032) and ascites (P = 0.025) were predictors[7] of shorter survival time[8] after radiation therapy (Table 1). By contrast, the early stages of liver cirrhosis (A or B; P = 0.03 and 0.02 respectively) were predictors of longer survival time. The variant factors of chronic hepatitis and tumor numbers were, however, not significant predictors. Mean values for the study parameters were compared across the three survival times using multiple analysis (Tables 1, 2). It was demonstrated that AFP <91.8 ng/mL, tumor volume <178 mL; GOT <59 IU/L; GPT <43.5 IU/L, and total bilirubin <0.799 mg/dL were predictors of longer survival time post radiation therapy.
We found that the associated procedure for TAE did not predict survival time after radiation therapy (Table 4).
DISCUSSION DISCUSSION DISCUSSION DISCUSSION DISCUSSION
Our results may provide a reference for prediction of outcome after radiotherapy for HCC, based on CT and clinical and laboratory assessment.
In this retrospective study, the number of eligible cases from the radiation oncology departments at TMUH and TWH was scarcely sufficient. In comparison to the reference study of Guo and colleagues[1], high grade criteria were not set to exclude advanced or terminal-stage disease from our sample.
Table 1 Parameters of CT findings
Parameters Survival time <0.5 yr 0.5-2 yr >2 yr P Tumor number 1 2 4 9 0.31 2 2 6 4 0.38 Multiple or diffuse 1 4 3 0.24 PVT 7 8 1 0.032 Ascites 7 16 6 0.025
Table 2 Parameters of clinical assessment
Parameters Survival time <0.5 yr 0.5-2 yr >2 yr P
Hepatitis 8 11 14 0.37 Cirrhosis
A 3 5 22 0.03 B 5 13 6 0.02 C 1 0 0 0.28
Table 3 Parameters of laboratory data
AFP <0.5 yr 0.5-2 yr >2 yr P Range 2.7-146 700 10-265 891 2.3-40 248 <0.0001 Mean 23 844 47 594.8 91.8 Tumor size <0.5 yr 0.5-2 yr >2 yr P Range 126-916 4-1 948 19-1 405 <0.0001 Mean 365 178 204 GOT <0.5 yr 0.5-2 yr >2 yr P Range 20-330 2.1-270 20-153 <0.0001 Mean 99 59 59.8 GPT <0.5 yr 0.5-2 yr >2 yr P Range 31-92 0.8-138 22-442 <0.0001 Mean 50 43.5 94.2 Bili (T) <0.5 yr 0.5-2 yr >2 yr P Range 0.4-2 0.5-21 0.19-1.84 <0.0001 Mean 1.39 1.12 0.799
Table 4 Parameters of TAE treatment
Parameters Survival time <0.5 yr 0.5-2 yr >2 yr Total P TAE
Performance 9 13 18 40 0.47 Not performance 3 8 15 26
Leung TK et al. Parameters predicts outcome of HCC by radiotherapy 1699
The two studies differed in terms of overall survival rate, with markedly shorter post-RT survival time demonstrated for our sample population. Basically, this is due to fundamental differences in the two studies. In the above-mentioned study, the cases were first treated in the same hospital. By contrast, the source of our cases could be divided into two categories. The first consisted of referrals from other hospitals or medical units without initial treatment at our two institutions, such that, in most cases, we were not able to take advantage of the ‘golden period’ in terms of successful TAE treatment. Further, many patients had already undergone multiple sequential TAE procedures and as such, poor response to further TAE could be anticipated. Further, we also suggest that our cases were more severe and more advanced in terms of HCC stage as determined from CT and clinical and laboratory parameters. Our second category of patients were initially treated in the same hospital after HCC was proven, as in the study of Guo and colleagues[1], with some of these referred to diagnostic radiation departments for TAE. Unfortunately, the first group outnumbered the second by more than nine-fold in our study, resulting in a significant decrease in prediction of success rate for our TAE cases, as well as, shorter median survival time post-RT treatment, compared to the reference study. Therefore, it appears reasonable to assume that the difference in patient-selection criteria explains the disparity between these two otherwise similar studies.
In conclusion, we found that the presence of PVT (P = 0.032)[9] and ascites (P = 0.025) after radiation therapy were predictors of shorter survival time. By contrast, the early stages of liver cirrhosis (A and B; P = 0.03 and 0.02 respectively) were predictors of longer survival time[10].
REFERENCES REFERENCES REFERENCES REFERENCES REFERENCES
1 Guo WJ, Yu EX, Liu LM, Li J, Chen Z, Lin JH, Meng ZQ, Feng
Y. Comparsion between chemoembolization combined with radiotherapy and chemoembolization alone for large hepato-cellular carcinoma. World J Gastroenterol 2003; 9: 1697-1701
2 Hermans R, Op de beeck K, Van den Bogaert W, Rijnders
A, Staelens L, Feron M, Bellon E. The relation of CT-deter-mined tumor parameters and local and regional outcome of tonsillar cancer after definitive radiation treatment. Int J Radiat Oncol Biol Phys 2001; 50: 37-45
3 Tokuuye K, Sumi M, Kagami Y, Murayama S, Kawashima
M, Ikeda H, Ueno H, Okusaka T, Okada S. Radiotherapy for hepatocellular carcinoma. Strahlenther Onkol 2000; 176: 406-410
4 Yasuda S, Ito H, Yoshikawa M, Shinozaki M, Goto N,
Fujimoto H, Nasu K, Uno T, Itami J, Isobe K, Shigematsu N, Ebara M, Saisho H. Radiotherapy for large hepatocellular carcinoma combined with transcatheter arterial embolization and percutaneous ethanol injection therapy. Int J Oncol 1999;
15: 467-473
5 Le Pechoux C, Akine Y, Tokita N, Sumi M, Churei H,
Takayasu K, Muramatsu Y, Wakao F, Hasegawa H. Case report; hepatocellular carcinoma diagnosed radiologically, treated by transcatheter arterial embolization and limited-field radiotherapy. Br J Radiol 1994; 67: 591-595
6 Chen SC, Lian SL, Chang WY. The effect of external radio-therapy in treatment of portal vein invasion in hepatocellular carcinoma. Cancer Chemother Pharmacol 1994; 33: 124-127 7 Seong J, Park HC, Han KH, Chon CY. Clinical results and
prognostic factors in radiotherapy for unresectable hepato-cellular carcinoma:a retrospective study of 158 patients. Int J Radiat Oncol Biol Phys 2003; 55: 329-336
8 Guo W, Yu E, Yi C, Wu W, Lin J. Prognostic factors influenc-ing survival in patients with large hepatocellular carcinoma receiving combined transcatheter arterial chemoembolization and radiotherapy. Zhonghua GanzangbBing Zazhi 2002; 10: 167-169
9 Huang CJ, Lian SL, Chen SC, Wu DK, Wei SY, Huang MY,
Ho YH. External beam radiation therapy for inoperable heptocellular carcinoma with portal vein thrombosis. Kaohsiung J Med Sci 2001; 17: 610-614
1 0 Watanabe J, Kushihata F, Honda K, Sugita A, Tateishi N, Mominoki K, Matsuda S, Kodayashi N. Prognostic signifi-cance of Bcl-xL in human hepatocellular carcinoma. Surgery 2004; 135: 604-612