Chin J Radiol 2004; 29: 349-352 349
It is difficult to manage arteriovenous malforma-tions or fistulas of the face because of the abundant vascular network in this region. They are commonly manifest in childhood or adolescence and often pre-sent with significant hemorrhage or cosmetic defects. We report a one-year-old infant with a facial arteriovenous fistula. It is successfully treated by transarterial embolization with metallic coils, resulting in clinical and angiographical improve-ment.
Key words: Arteriovenous malformation, therapeutic embolization; Face
Arteriovenous malformations (AVMs) or arteri-ovenous fistulas (AVFs) of the head and neck are quite rare in contrast to low-flow vascular malformations. They are 20 times more common in the intracranial vasculature than in that served by the external carotid arteries [1]. Cervicofacial involvement is most common in the cheeks, ears, nose, and forehead, in descending order of prevalence. The primary pathology occurs at the capillary level, where arteri-ovenous shunting occurs. Engorged feeding arteries and drainage veins result from uncontrolled shunting through these channels. They are rarely symptomatic in the neonatal or infant period, but most commonly discovered in late childhood, adolescence, or early adulthood. AVMs / AVFs manifest as warm, firm masses with thrills, bruits, and pulsatility.
Treatment of these high-flow vascular anomalies is complex and has a predictably high incidence of recurrence if not managed correctly. Intervention is indicated for complications such as pain, haemorrhage, pressure symptoms, ischaemic ulceration and even congestive cardiac failure.
CASE REPORT
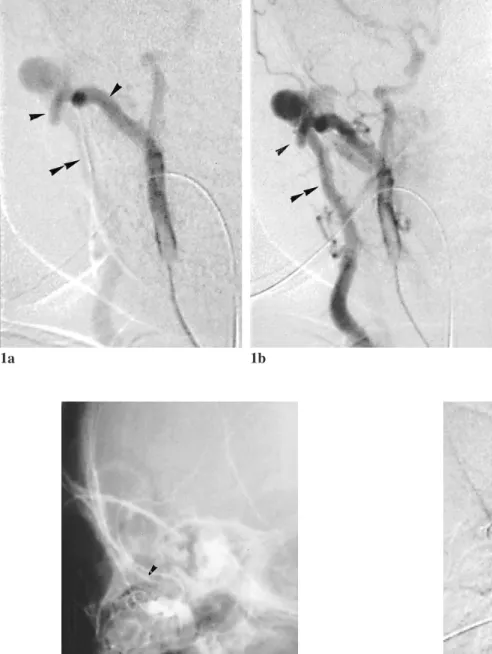
A 1-year-old infant had suffered from a pulsatile lesion over right preauricular area for several months. There was an erythematous blush of the skin overlying the lesion. Physical examination revealed a remark-ablely palpable thrill with continuous murmur at right preauricular area. Digital subtraction angiography with selective right external carotid arteriography revealed arteriovenous fistula between right internal maxillary artery and right external jugular vein (Fig. 1). After the feeding arteries were identified, transarterial emboliza-tion with two 5mm spring coils was performed to embolize the fistula (Fig. 2). The thrill in preauricular region disappeared immediately. Post-embolization angiogram showed complete disappearance of the
Reprint requests to: Dr. Yung- Fang Chen
Department of Radiology, China Medical University Hospital.
No. 2, Yuh Der Road, Taichung 404, Taiwan, R.O.C.
Congenital Facial Arteriovenous Fistula
Successfully Treated by Tranarterial
Embolization: a case report
HUI-YICHEN1 YUNG- FANGCHEN1 HSEIN- JARCHIANG2 MING- TSEHUNG1 WU -CHUNGSHEN1 Department of Radiology1, China Medical University Hospital
fistula (Fig. 3). The patient recovered without compli-cation. No recurrence of the lesion was seen on subse-quent clinical examination.
DISCUSSION
AVFs occur most often in the carotid cavernous
fistula and vertebral fistula, rarely in external carotid fistula. AVMs / AVFs of the face or neck are high-flow vascular malformations and have a rich arterial network fed by branches of the external carotid artery. There are two types of arteriovenous fistulas, congen-ital and acquired. A congencongen-ital arteriovenous fistula is uncommon and one that formed during fetal develop-Congenital AVF treated by TAE
350
Figure 3. Lateral projection of right external carotid
angiogram after embolization shows complete occlusion of the fistula.
Figure 1. a. Arterial, and b. capillary
phase of lateral projection digital subtraction images from right external carotid angiogram show arteriovenous fistula (white arrow) between the internal maxillary artery (black arrow) and external jugular vein (double black arrow).
1a 1b
Figure 2. Unsubtracted lateral radiograph obtained after
embolization of the feeding artery with two pieces of 5mm spring coils (arrow).
ment. In congenital fistulas, blood vessels of the lower extremity are more frequently involved than other areas of the body. Spontaneous development of AVF occurs in neurofibromatosis 1 and fibromuscular disease, as well as without specific underlying disease [2, 3]. An acquired arteriovenous fistula may cause by iatrogenic reasons or more commonly, traumatic in origin. It is rare of our case, a congenital arteriovenous fistula of the external carotid artery, which is sympto-matic in such a little baby.
Our Case is a stage II arteriovenous fistula, which displays bruit and thrill. In early stage, AVM may manifest only cutaneous warmth or blush. When the extensive lesion causes increased shunting of blood and decreased nutritive blood flow to the skin, the symptoms and signs include pain, ulceration, bleeding, audible bruits, palpable thrills, and pulsatility [4]. Factors associated with expansion include trauma, infection, incomplete resection, and hormonal changes occurring during pregnancy, puberty.
Symptomatic or complicated lesions may necessi-tate an attempt at surgical excision or selective embolization. In the past, treatment of AVM/ AVF of the face was primarily reliant on surgical excision or ligation of the feeding arteries [5, 6, 7]. For small lesions, excision alone may be possible. For more extensive lesions, the treatment of choice is combina-tion therapy that consists of preoperative angiography with selective embolization followed by definitive resection within 24- 48 hours. Excision was often associated with extensive blood loss and the need for skin reconstruction procedures. Surgical ligations of the feeding vessels proximal to the fistula are sometimes ineffective because of the recruitment of a collateral vessel supply and the loss of access to the fistula for further embolization [8].
Embolization as the sole treatment of AVM/ AVF can be either curative or palliative for symptoms such as pain or mass effect [9, 10, 11]. When used embolization immediately prior to resection, it reduces intraoperative blood loss, shortens surgical time, and decreases surgical morbidity and mortality [9]. Embolization may use PVA, balloons, coils or NBCA [12]. Small diameter coils are especially useful when it is impossible to pass a balloon through the narrow orifice of the fistula, or when the venous portion of the fistula is not large enough to inflate the balloon.
Congenital arteriovenous fistula of the internal maxillary artery in a infant is rare. Early recognition and proper treatment are essential for an acceptable long term outcome. The case we present here demon-strates a quick and successful method of closing an AVF by the transvascular embolization with coils.
REFERENCES
1. Kohout MP, Hansen M, Pribaz JJ, Mulliken JB: Arteriovenous malformations of the head and neck: nat-ural history and management. Plast Reconstr Surg 1998 Sep; 102: 643-654
2. Markham JW. Spontaneous arteriovenous fistula of the vertebral artery and vein (case report). J Neurosurgery 1969; 31: 220-223
3. Deans Wr, Bloch S, Leibrock L, et al. Arteriovenous fistula in patient with neurofibromatosis. Radiology 1982; 144: 103-107
4. Bartlett JA, Riding KH, Solkeld LJ. Management of hemangiomas of the head and neck in children. J Otolaryngol 1988; 17: 11-20
5. Nagasaka S, Fukushima T, Goto K, Ohijimi H, Iwabuchi S, Maehara F. Treatment of scalp arteriove-nous malformation. Neurosurgery 1996; 38: 671-677 6. Stillman RM, Powers JC, Fitzgerald JF. Cosmetic
exci-sion of an isolated extracranial arteriovenous malforma-tion using Gelfoam embolizamalforma-tion. Br J Surg 1977; 64: 784-785
7. Marotta TR, Berenstein A, Zide B. The role of embolization and tissue expanders in the management of arteriovenous malformations of the scalp. AJNR 1994; 15: 1240-1246
8. Berenstein A, Scott J, Choi IS, Persky M. Percutaneous embolization of arteriovenous fistulas of the carotid artery. AJNR 1986; 7: 937-942
9. Han MH, Seong SO, Kim HD, Chang KH, Yeon KM, Han MC. Craniofacial arteriovenous malformation: pre-operative embolization with direct puncture and injec-tion of n-butyl cyanoacrylate. Radiology 1999; 211: 661-666
10. Gobin YP, Garcia-de-la-Fuente JA, Herbreteau D, Houdart E, Merland JJ. Endovascular treatment of external carotid-jugular fistulae in the parotid region. Neurosurgery 1993; 33: 812-816
11. Herbreteau D, Aymard A, Jhaveri HS, et al. Current management of cervicofacial superficial vascular mal-formations and hemangiomas. Interventional neuroradi-ology. Philadelphia, Pa: Saunders, 1999; 317-327 12. Towbin RB, Ball WS Tr. Pediatric interventional
radiol-ogy. Radiol Clin North Am 1988; 26: 419
Congenital AVF treated by TAE 352