中華放射醫誌Chin J Radiol 2010; 35: 57-60 57
Reprint requests to: Dr. Shaw-Nan Jean
Department of Radiology, Dachien General Hospital. No. 6, Shinguang Street, Miaoli 360, Taiwan, R.O.C.
Venous aneurysms are uncommon in clinical practice. Idiopathic aneurysms of the superior mesenteric vein are rare. The etiology of these aneurysms is unclear, as they are found in both asymptomatic individuals and in those with concurrent disease. Herein we discuss a case of superior mesenteric vein aneurysm in a patient with colon cancer diagnosed with MDCT.
Aneurysms of the superior mesenteric vein are rare; the first case was reported by Barzilai and Kleckner in 1956. Many aneurysms are asymptom-atic, and the diagnosis is established from radiologic findings. Others are diagnosed after complications such as gastrointestinal bleeding or thrombosis with associated abdominal pain. Because imaging of the abdomen is performed more frequently than ever, such aneurysms may be more common than previ-ously recognized. Herein we present a case with no predisposing factor.
CASE REPORT
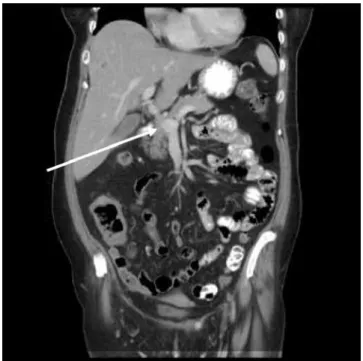
A 64-year-old woman presented with inter-mittent right lower quadrant pain of one month. Laboratory analysis revealed an elevation of CEA. An abdominal sonogram showed target-sign in the right lower quadrant. Unenhanced and enhanced CT scans demonstrated a mass-like lesion in the right ascending colon and the coronal and the axial section of CT scan showed a dilated (1.8 cm AP) diameter superior mesenteric vein (Fig. 1) without internal thrombosis near the level of the portal confluence (Fig. 2). Surgical intervention was performed for the colon, and the pathology was confirmed as colon cancer. Since the time of diagnosis of the aneurysm, the patient’s condition has remained stable and continues to be followed clinically.
DISCCUSSION
The portal vein is created by the confluence of the SMV and splenic veins at the level of the pancreatic neck. It extends into the hepato-duodenal ligament and is divided into the right and left branches to supply both lobes of the liver. Its trunk measures 5 to 7 cm in length. Characteristically, the SMV is located anterior right to the superior mesen-teric artery and posterior medial to the head of the pancreas. The SMV tributaries are the ileocolonic, pancreatoduodenal, & gatroepiploic veins. Normally,
Aneurysm of the Superior Mesenteric Vein:
case report
Shaw-NaN JeaN1 XiaN-Jia JiaNg1 YuNg-FaNg CheN2 Jui-FeN CheN2
Department of Radiology1, Dachien General Hospital Department of Radiology2, China Medical University Hospital
Aneurysm of the superior mesenteric vein 58
the SMV measures 1.2 cm in diameter [1]. Its size was reported as abnormal if it measured > 1.4 to 1.6 cm in transverse diameter or showed abrupt change of the caliber it courses.
Aneurysms of the superior mesenteric vein are rare; the first case was reported by Barzilai and Kleckner in 1956 [2]. Schill et al offered a possible explanation of the congenital basis of a superior mesenteric vein aneurysm [3]. The portal vein is formed from portions of the right and left vitelline omphalomesenteric vein. Very early in development, the two vitelline veins are connected by bridging channels or anastomosis, which are named according to their relation with that portion of the foregut they surround, namely the future duodenum. Regression of the cranial component of the left vitelline vein, the central-ventral intervitelline anastomosis, and the caudal component of the right vitelline vein allows for a normal extrahepatic portal vein [4]. Schild et al proposed that if the right vitelline vein is not obliter-ated completely to the level of the caudal-ventral intervitelline anastomosis, a small diverticulum may persist that eventually develops into an aneurysm of the superior mesenteric vein.
Venous aneurysms are not common in clinical practice; most patients with intra-abdominal venous aneurysm seek medial assistance because of vague abdominal pain. Some patients may have gastrointes-tinal bleeding, acute venous occlusion, or pulmonary embolism [5]. The patient in our case presented with right lower quadrant abdominal pain related to colon cancer. The SMV aneurysm is an incidental finding.
Sonography was usually the first imaging technique performed, because it is noninvasive. The aneurysm appeared as an anechnoic structure near the head of the pancreas. Their vascular nature is confirmed with color Doppler and duplex sonography. Color Doppler sonography reveals that these aneurysms fill completely with color f low unless they contain thrombosis. Duplex Doppler sonography demonstrates a monophasic wave form characteristic of the superior mesenteric vein. Flow is hepatopedal in the portal vein unless there is asso-ciated portal hypertension. Flow within the superior mesenteric vein is directed toward the por tal confluence.
A CT scan revealed the size and extent of the lesion, and confirmed its vascular origin, but required the use of iodinated intravenous contrast medium [6]. However, an advantage of helical CT is the CT angiogram, which allows rendering of three-dimensional angiogram images by using helical
technology and computer software. The multiplanar capability of magnetic resonance imaging (MRI) along with the capacity to render angiogram-like images of vascular structures makes MRI well suited to the evaluation of such an aneurysm. In the past,
Figure 1. Axial section of CT scan shows a dilated (1.8
cm AP diameter) superior mesenteric vein without inter-nal thrombosis.
Figure 2. Coronal section of CT scan demonstrates a
dilated superior mesenteric vein near the level of the con-fluence.
Aneurysm of the superior mesenteric vein 59 venous phase mesenteric angiography and
spleno-portography were used to evaluate these aneurysms [7, 8]. However, due to invasiveness of angiographic procedure, sonography, CT and MRI are preferred in most instances.
As there are few documented cases of SMV aneurysms, the nature and history of the disease are not clear. First-line management has changed over time, with there being a shift from surgical to conservative management. Initially it was though that surgical intervention with either shunting or aneurysmorrhagphy procedure was the treatment of choice, particularly in cases with evidence of portal hypertension [9].However, instead of the surgical approach, it may now be appropriate to follow up patients conservatively with serial imaging [10]. Because an SMV aneurysm is a rare anomaly and its long-term evolution is not known, patients should be clearly informed of possible complications, including rupture and thrombosis.
REFERENCES
1. B o l o n d i L , G a n d o l f i L , A r i e n t i V, e t a l : Ultrasonography in diagnosis of portal hypertension: Diminished response of portal vessels to respiration. Radiology 1982; 142: 167-172
2. Barzilai R, Kleckner MS. Hemocholecyst following ruptured aneurysm of portal vein. Arch Surg 1956; 72: 725-727
3. Schild H, Schweden F, Braun B, et al. Aneurysm of the superior mesenteric vein. Radiology 1982; 145: 641-642 4. Marks C. surgical implications of portal venous system
malformation. Ann Coll Surg Eng 1974; 55: 299-306 5. Nishinari K, Wolosker N, Yazbek G, Nakagawa WT,
Lopes A. Idiopathic aneurysm of inferior vena cava associated with retroperitoneal ganglioneuroma: case report. J Vas Surg 2003; 37: 895-898
6. Seda J, Padovani B, chanalet S. aneurysm of the supe-rior mesenteric vein. AJR Am J Roentgenol 1993; 161: 903-904
7. Hagiwara H, Kasahara A, Kono M, et al. Extrahepatic portal vein aneurysm associated with a tortuous portal vein. Gastroenterology 1991; 100: 818-821
8. Itoh Y, Kawasaki T, Nishikawa H, et al. A case of extrahepatic portal vein aneurysm accompanying lupioid hepatitis. J Clin Ultrasound 1995; 23: 374-378 9. WL Perret, A de Silva, et al. Portal circulation
aneu-rysms: Two case reviews. Australasian Radiology 2007; 51: 87-90
10. Fulcher A, Tumer M. Aneurysm of the portal vein and superior mesenteric vein. Abdom Imaging 1997; 22: 287-289
Aneurysm of the superior mesenteric vein 60