The Effectiveness of Video-Telemedicine for
Screening of Patients Requesting Emergency Air
Medical Transport (EAMT)
Shin-Han Tsai, MD, PhD, Jess Kraus, PhD, Hsueh-Ru Wu, MSN, Wan-Lin Chen, MD,
Ming-Fu Chiang, MD, PhD, Li-Hua Lu, MD, MMS, Chia-En Chang, MS, and Wen-Ta Chiu, MD, PhD Background:Demand for emergency
air medical transport (EAMT) services have increased in recent years. However, the high costs of these services have raised questions on the benefit to patient outcomes. In this study, we evaluate the effectiveness of video-telemedicine for the preflight screening of patients for air medical transports.
Method:A prospective cohort study. Medical records of patients transported from the Penghu Islands to Taiwan were retrospectively collected from November 1999 to October 2002 (stage 1). In addi-tion, we collected medical records of pa-tients who were preflight-screened by physicians using video Web cameras from November 1, 2002 through August 30, 2003 (stage 2). The intervention in stage 2 included a set of protocols and screening
criteria for EAMT implemented by the Na-tional Aeromedical Consultation Center (NACC). In stage 1, there were no standard-ized protocols or screening guidelines for EAMT. The EAMT system before imple-menting preflight screening and telemedi-cine was mostly based on patient’s requests and their health condition determined by the treating medical officers (TMO).
Results:A total of 822 transfers were included in this study. Patient demographic backgrounds in the two groups were similar on gender, age, disease classification, and types of illnesses. Patients in stage 2 were significantly older than those in stage 1. In a comparison of flight frequencies between the two stages, the results revealed a 36.2% reduction of EAMT applications in stage 2. The flight approval rate was 91.2%. The
intervention in stage 2 also presented a sig-nificant reduction in cross-zone transport (16.1% to 0.1% to the northern Taiwan re-gion). Within-zone transfers increased from 74.9% to 88.3%. Cost analysis showed that physician triage in stage 2 resulted in a total annual savings on EAMTs of US$ 448,986.
Conclusions:This study demonstrates the physician-assisted preflight screening using video-telemedicine significantly re-duced the frequency of unnecessary air medical transports and consequently led to reduced costs. Video-telemedicine can be an essential tool to support physicians in decision-making for patient screening.
Key Words: Emergency air medical transport, Remote island, Physician triage, Telemedicine, Helicopter, Cost analysis.
J Trauma. 2007;62:504 –511.
T
he demand for emergency air medical transport (EAMT) services has increased in recent years. There are increasing numbers of EAMT programs supported by trauma centers to provide efficient management of emergency medical care andbetter patient outcomes.1– 4However, there are growing num-bers of studies questioning the cost-effectiveness of EAMT services.5–10Attempts to reduce costs have been a major con-cern for hospital administrators as well as the third-party payers.11A well-defined and integrated triage system has been widely suggested for cost-effective management of emergency air medical transport.3,9,11–15
IMPORTANCE
Previous studies have shown cost effectiveness of tele-medicine in emergency care.14,16 –22Because of advances in computer technology, video telemedicine has become popu-lar and available. The use of telemedicine has been widely accepted as a cost-effective option in health care, especially in remote areas.18,19Moreover, in a study on the use of tele-medicine, Roth et al. (1998) concluded that prehospital transtele-phonic triage can effectively reduce costs of medical care and the number of hospital emergency department visits.11 In a similar study, Haskins and colleagues (2002) reported that tele-medicine resulted in an approximately 15% decrease in ambu-lance transport.23In the United Kingdom, the first telemedicine link in Northern Ireland showed a dramatic reduction of patients referred to their General Practitioners (GPs) and accident and emergency (A&E) departments.24 A study in Aberdeen also Submitted for publication June 15, 2005.
Accepted for publication February 22, 2006.
Copyright © 2007 by Lippincott Williams & Wilkins, Inc.
From the Institute of Injury Prevention and Control (S.-H.T., H.-R.W., W.-L.C., C.-E.C., W.-T.C.), Department of Neurological Surgery (S.-H.T., W.-T.C.), and Department of Emergency Medicine (S.-H.T.), Taipei Medical University-Wan Fang Hospital, Taipei, Taiwan; Injury Prevention Research Center (J.F.K.), University of California Los Angeles, Los Angeles, CA; Division of Neurological Surgery (W.-L.C.), St. Mary’s Hospital, Ilan, Tai-wan; Division of Neurological Surgery (M.-F.C.), Mackay Memorial Hos-pital, Taipei, Taiwan; Department of Emergency Medicine (W.-M.C.), Mackay Memorial Hospital Hsinchu Branch, Hsinchu, Taiwan; and Depart-ment of Emergency Medicine (L.-H.L.), Tong’s MetroHarbor Hospital, Taichung, Taiwan.
Presented, in part, at the 14th World Congress for Disaster and Emer-gency Medicine, May 16 –20, 2005, Edinburgh, United Kingdom.
Supported by research funding from the Department of Health, Taiwan for NACC project (DOH93-TD-M-113-010) and a grant from the National Health Research Institute (NHRI-EX94-9106PN).
Address for reprints: Wen-Ta Chiu, PhD, MD, 250 Wu-Shin Street, Taipei 110, Taiwan; email: [email protected].
demonstrated that 58% of patient transfers can be avoided after the use of telemedical link.20,24Other studies have also reported the reliability and feasibility of telemedicine in emergency care, especially in rural areas.21,25–27
The geographical limitations in Taiwan and unequal de-velopment of medical manpower and facilities on remote islands have resulted in a growing need of medical transfers to the main island of Taiwan. A lack of a preflight screening system has resulted in rapid growth of unnecessary flights, which caused increased government expenditures of up to NT $200,000,000 (US$ 6,250,000) each year. The rapid growth of EAMTs and the high costs caused Taiwanese healthcare authorities to establish a National Aeromedical Consultation Center (NACC), a physician-based helicopter control center for the preflight screening of patients requesting EAMT services.28
GOAL OF INVESTIGATION
Although there is increasing awareness on cost effective use of telemedicine in emergency care, little is published about the use of telemedicine in reducing unnecessary air medical transport. The increase in the use of EAMT programs as well as its high costs has prompted a need to investigate the real benefit on EAMT. This is the first report to examine the effectiveness of video-telemedicine to reduce costs by pre-flight screening of EAMT. Our research question is ‘would preflight screening using telemedicine result in the reduction of EAMT and enhance the safety of patient transfers’?
MATERIALS AND METHODS
Study Design and the Selection of Patients
This is a prospective cohort study, which comprised two groups of research subjects; a historical group before the intervention (stage 1) and a second group who received a screening protocol, defined as stage 2. Patients in the control group (stage 1) were defined as patients who were air trans-ported from a remote island of Taiwan to the mainland without receiving preflight screening. The patients in the intervention group were those who receive preflight screen-ing by physicians usscreen-ing a protocol containscreen-ing screenscreen-ing cri-teria, and video-telemedical devices. The study period began on November 1, 2002 and ran to August 30, 2003.
Participants included patients from Penghu Islands who received EAMT services during the study period. Patients who took commercial flights to Taiwan without preflight screening were excluded. Participants who did not meet the transport criteria were included in the study.
Settings
The research settings include four sites of wireless local area network (LAN) located in the emergency departments on the Penghu Islands connected to one control center located in the headquarters of National Rescue Command Center in Taipei. The four sites included two district hospitals, Penghu
Military Hospital and Penghu County Hospital, and two re-mote clinics located in two of the outer islands of Penghu. Definitions
Penghu Islands
The Penghu Islands comprise archipelago located off the southwest coast of Taiwan in the Taiwan Strait. The flying distance between the Penghu Islands and Taiwan is approx-imately 200 miles. There were no changes regarding popu-lation, manpower, or medical facilities available in Penghu Islands during the study period.
The National Aeromedical Consultation Center
The National Aeromedical Consultation Center (NACC) was established on October 1, 2002. It is a physician-based 24-hour control center that coordinates the transport of in-jured or critically ill patients between Taiwan and its sur-rounding islands.28 The main objective of the NACC is to provide criteria-based preflight screening of patients who required air transport from 18 locations nationwide. Currently there are 10 senior consultant physicians and a medical di-rector who participate in consultation. All have backgrounds in emergency medicine, neurologic surgery, critical care medicine, aviation medicine, and “flying doctors” who have participated in EAMT for at least 2 years.
Before the NACC was established, all EAMT services were dispatched without criteria for patients’ qualification. Physicians in referring hospitals made requests to helicopters for urgent transport, if, in their opinion, a patient’s conditions required it. Once requested, the helicopter was dispatched in all cases except in extreme nonflying weather conditions. Safety
Cross-strait transport exceeding 250 miles is considered high risk and unsafe. In some cases, cross-zone flights were considered unnecessary if medical centers within the respon-sible zones had the ability to manage the medical condition. Unnecessary Flights
For purposes of this study, unnecessary flight is defined by the urgency of the patient’s condition. If alternative means of transport, such as transported by ferry or commercial flights is suitable for transport, the EAMT applications would be rejected. Standard Operation Procedures for Medical Transports
The standard operation procedures (SOPs) were de-signed by a joint committee comprised of a group of experts including representatives from the National Fire Administra-tion (NFA), senior officers from the Department of Health (DOH), and Civil Aeronautics Administration (CAA), as well as physicians who specialize in emergency medicine, critical care, and aviation medicine. Requests for EAMT must be made by the treating medical officers (TMO) from an island hospital to the NACC. Physicians communicate using the tele-video system. Furthermore, physicians at the NACC
evaluate patients directly through a desktop computer for the initial assessment. Once the application forms are received by the physicians at the NACC, a decision must be made within 15 minutes on whether the patient is fit to fly. Patients in a stable condition or those who do not meet the criteria for transport remain on the island. However, they will receive the same level of care by the TMO, and they are monitored constantly by the NACC.29Patients in a stable condition but who still need to be transported to major hospitals for further evaluation will travel by ferry or commercial flights to Tai-wan. The transport is free of charge, as the health authorities cover transportation cost.
The Video System
The video system is located at the NACC. The system includes receiving terminals that connect 18 remote hospitals with the control center and are connected to a Web cam in the emergency rooms. Physicians at the control center can closely evaluate a patient’s condition and his or her medical records including X-ray films and echocardiogram reports through the desktop computer. In case of an emergency, the TMO in the referring hospital can initiate an urgent consultation with the NACC. Once the alarm is given, consultants in the NACC are alerted.
Criteria for Emergency Transport
The criteria were originally adapted from various resources including the American College of Emergency Physicians (Guidelines for Trauma Care Systems12,13), Air Medical Ser-vices Committee of the National Association of EMS Physi-cians (Prehospital Air Medical Transport: Non-Trauma and
Pediatric Consideration30), transport guidelines from the As-sociation of Air Medical Services29, and regional criteria from Australia.31The criteria were summarized in Table 1. Data Collection
Data collection comprised chart review at two different times. Stage 1 consisted of EAMT services on the Penghu Islands before the NACC was established when all EAMTs were activated without preflight screening from November 1999 to September 30, 2002.
In stage 2, all EAMT services received preflight screen-ing and involved physicians who were on call at the NACC using video Web-cameras for cross-strait consultation. Med-ical record data were collected from October 1, 2002 until August 30, 2003.
Data collection included two abstractors who received training on the use of computer software ‘SPSS 11.0’. The database was reviewed by the two abstractors for validity and reliability. All data in both stages included patient demo-graphics, disease classification, average flights per months, the frequencies of cross-zone transports, and costs were en-tered into SPSS for coding and statistical analyses. The re-search associate in charge of the study developed the data
codebook, and the abstractors were blinded to the research questions being tested.
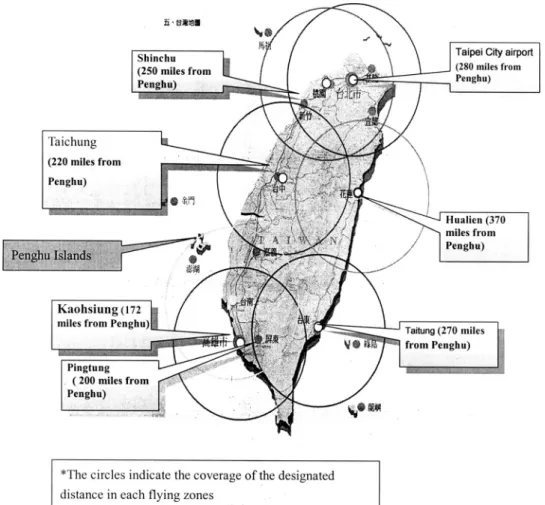
Zones of Responsibility and Flying Distances
There are seven major responsible zones (Fig. 1). The Penghu Islands are included in the southern region, and the flying distance between Penghu Islands and the nearest city (Kaoshiung) in Taiwan is 172 miles. When EAMT is acti-vated, all helicopters take off from the bases in Taiwan to the remote islands and transfer patients back that doubles the flying distances. Flying distances between Penghu and major cities in Taiwan are shown in Figure 1.
Statistical Analysis
The results are evaluated by frequency in each stage. Categorical variables in two groups are compared by 2
analysis. All p values were two tailed, and a p value⬍0.05 was considered statistically significant.
RESULTS
General Information
In total, 822 transfers were included in the study. The number of uses of EAMT in stage 1 was 685 (84%) and 137 Table 1 Criteria of EAMT
1. Penetrating injury anywhere on the body between the mid-thigh and the head
2. Amputation or near amputation and required timely evaluation for possible replantation
3. Severe hemorrhage. Included are those patients with a systolic blood pressure of⬍90 mm Hg after initial volume resuscitation and those requiring ongoing blood transfusions to maintain a stable blood pressure
4. Burns of the skin;⬎10% of the body surface; or major burns of the face, hands, feet, or perineum; or associated with an airway or inhalation injury
5. Injury to the spinal cord, spinal column, or neurologic deficit 6. Trauma Score⬍12 or Glasgow Coma Scale score ⬍10 at the
scene of the accident or at the referring hospital’s emergency department that indicated a severe injury
7. Less than 5 years of age with multiple traumatic injuries 8. Adult with a respiratory rate of⬍10 or ⬎30 breaths per minute,
or a heart rate of⬍60 or ⬎120 beats per minute
9. Requires mechanical ventilator support or is at risk of having an unstable airway
10. Requires immediate invasive therapy for hypothermia
11. Respiratory rate of⬍10 or ⬎30, or a heart rate of ⬍50 or ⬎150 per minute
12. Requires immediate transport in a critical care environment to a medical center that can perform organ transplantation or procurement
13. Seizures that cannot be controlled at the referring hospital 14. Acute respiratory failure or respiratory arrest and is not
responsive to initial therapy 15. Unstable vital signs
Respiratory rate⬍10 or ⬎60 breaths per minute Systolic blood pressure⬍60 mm Hg in a neonate
Systolic blood pressure⬍70 mm Hg in a child 2 to 5 years old or systolic blood pressure⬍80 mm Hg in a child 6 to 12 years
(16%) in stage 2. Patient demographic data for the two cohorts were similar regarding gender, age, disease classifi-cation, and types of illnesses (trauma, disease) (Table 2). The
majority of patients were male (65.6%). Over 28% of patients were between 61 and 75 years of age or between 0 and 15 years (18.9%) (Table 3).
The mean age of the total sample group was 47.15⫾ SD 27.53. Patient mean age significantly differed between the groups. Patient mean age in stage 2 was older (51.7⫾ 23.47) than those in stage 1 (46.23⫾ SD 28.21, t ⫽ ⫺2.135, p ⫽ 0.033) (Table 3). The majority of patients had major illnesses (76.6%, n⫽ 630).
Frequencies of EAMTs
During stage one, 685 flights were activated representing an average of 19.6 flights per month. In comparison, 137 flights were requested in stage two, but only 125 flights were approved representing an average of 12.5 flights per month, less than stage one. The reduction rate of flights between two stages was 36.3%.
Responsible Zones and Flight Distances
In the first stage of this study, about 74.9% of patients were within-zone transferred to the southern region (Table 4) and 16.1% were transferred to the northern region. We also found that one patient (0.1%) was inappropriately transferred to the eastern region, a remote region with limited medical
Fig. 1. EAMT responsible zones and average one-way flight distances to the Penghu Islands.
Table 2 Demographic Information of Subjects in the Two Stages Stage 1 N⫽ 685 (%) Stage 2 N⫽ 137 (%) Total N⫽ 822 (%) Gender Male 452 (66.0) 87 (63.5) 539 (65.6) Female 233 (34.0) 50 (36.5) 283 (34.4) Age 0–15 142 (20.7) 13 (9.5) 155 (18.9) 16–30 74 (10.8) 14 (10.2) 88 (10.7) 31–45 74 (10.8) 19 (13.9) 93 (11.3) 46–60 103 (15.0) 26 (19.0) 129 (15.7) 61–75 188 (27.4) 44 (32.1) 232 (28.2) ⬎76 104 (15.2) 21 (15.3) 125 (15.2) Illness category Trauma 161 (23.5) 31 (22.6) 192 (23.4) Major illnesses 524 (76.5) 106 (77.4) 630 (76.6) Disease classification Medical 363 (53) 80 (58) 443 (53.9) Surgical 171 (25) 39 (29) 210 (25.6) Pediatric 137 (20) 12(9) 149 (18.1) OBS/GYN 14 (2) 6 (4) 20 (2.4)
facilities; and the flying distance exceeded 370 miles. In stage 2, cross-zone transfers were mostly disapproved.
During stage 2, the percentage of patients transferred to the northern region had decreased (from 16.1% to 1.5%) and within-zone transfers to the southern region increased from 74.9% to 88.3%. This finding suggests that most patients were transported to the nearest major hospital within respon-sible zones.
In addition, there were 12 patients who did not meet the criteria for transfer, including four patients who remained on the island who received the same level of care by the TMO and were constantly monitored. In addition, eight patients were in a stable condition and were transported by scheduled commercial flights or regular shuttle ferries between remote islands and major cities in Taiwan. None of these 12 patients developed any medical complications. The rationale for dis-approval is shown in Table 5.
Cost Analysis
Cost analysis is based on the sum of the reduced expen-diture for the decreased flights in stage 2. The average cost
for each repatriation was NT $200,000 (US$ 6,250); There-fore, the sum of the reduced cost of EAMTs each month was $6,250⫻ (19.6 ⫺ 12.5/mo) ⫽ US$ 44,375/mo or
US$ 532,500 per year. Direct Costs
The fee for physician manpower in Taiwan is not as good as it is in the United States. However, the cost of air trans-portation is very similar with that in every country. The annual budget of NACC including physician manpower is 13,000,000 NTD (US$ 406,250). This study collected data from Penghu Islands with four remote locations and NACC takes care of 18 remote locations nationwide. The cost of set up of the telemedicine system including the equipment of 18 locations is 6,500,000 NTD (US$ 203,125) and the system is estimated to be functional for 5 years (60 months). In this study we have used telemedicine equipment for 10 months. The cost of transport by scheduled commercial flight ($120 for round trip) and regular shuttle ferry ($70 for round trip) is quite inexpensive. There are 21 daily regular flights from Taiwan mainland to Penghu Island and 1 to the other 2 small islands. Therefore, the saving of cost in total has to deduct the above cost and is
$532,500⫺ ($406,250 ⫻ 4/18 ⫻ 10/12) ⫺ ($203,125 ⫻ 4/18 ⫻ 10/60) ⫺ ($120 ⫻ 4) ⫺ ($70 ⫻ 4) ⫽ $448,986 Indirect Costs
The indirect cost includes (1) increasing cost of medical care in the mainland and (2) the saving cost of productivity Table 3 Results of Grouped Sample t Test on Mean Age
N Mean Standard Deviation Standard Error of the Mean Stage 1 685 46.2336 28.21660 1.07810 Stage 2 136 51.7426 23.47039 2.01257
t test for Equality of Means
t df Significance (two-tailed) Mean Difference Standard Error of the Difference
95% Confidence Interval of the Difference
Lower Upper
⫺2.135 819 0.033 ⫺5.5091 2.58073 ⫺10.57470 ⫺0.44344
Table 4 Distribution Differences of Receiving Hospitals
Receiving hospitals by regions Flying Distances to Penghu (miles)*
Stage 1
N⫽ 685 (%) N⫽ 137 (%)Stage 2 N⫽ 822 (%)Total (two-sided)p-Value
Northern region 280 110 (16.1) 2 (1.5) 112 (13.6) 0.0002test
Central region 220 42 (6.1) 12 (8.8) 54 (6.6)
Southern region (responsible zone) 172 513 (74.9) 121 (88.3) 634 (77.1)
Eastern region 370 1 (.1) 0. (0) 1 (.1)
Within-island transfer 20 19 (2.7) 2 (1.5) 20 (2.4)
* The flying distances are calculated by one-way routes designated by CAA in Taiwan.
Table 5 Rationales for Disapproval of Flights
Rationale No. of Patients (n⫽ 12)
Condition stable, no need for immediate transfer
4 (33.3%) Transferred by scheduled commercial flight 4 (33.3%) Transferred by shuttle ferry 4 (33.3%)
loss because of disability from the patients and loss of future productivity because of premature death immediately repa-triated by this system. Both of them are very difficult to estimate.
Limitations
One of the limitations of this study was there was no information regarding patient follow-up in stage 1 because of a lack of protocols or monitoring of patient conditions during air transfer in stage 1. Although, in stage 2 of the study, physicians in the NACC provided records of patient moni-toring during and after the EAMT. Hence, it was impossible to compare patient outcomes between two stages. We also encountered a major difficulty in retrieving copies of medical records from more than 36 receiving hospitals in the 15 provinces of Taiwan. As in the first stage of the study, most patients were transferred to hospitals without proper selection or evaluation by the receiving hospitals.
DISCUSSION
Overview of the Findings
This study demonstrates several major findings. First, the intervention in stage 2 resulted in a significant (36.3%) re-duction in unnecessary air medical transport. Second, the reduced EAMT applications as a result of physician triage created a total government annual savings of up to US$ 448,986.
Geographical Background
Emergency air medical transport in Taiwan has experi-enced increasing demand in recent years. The geographical limits between Taiwan and its surrounding islands have pushed the growing need for EAMT.28The situation is par-ticularly relevant in the Penghu Islands with 90,000 residents located off the southwestern coast of Taiwan. Expenditures for helicopter emergency air medical services (HEAMS) in Penghu have increased in recent years. For example, in 2002, more than 300 flights were activated from the Penghu Island resulting in an increase of government annual expenditure of up to NT $60 million (US$ 1,875,000). One reason for the increase in EAMT flights may have been because of its free charge paid by the Taiwanese Health Authority. Another reason might have been because of the increasing trend in lawsuits resulting from physician shortages. Consequently, transferring patients to the mainland might have been con-sidered a solution to the above problems as healthcare facil-ities are better developed on Taiwan.
Benefits of Telemedicine
There are an increasing number of studies focusing on the use of telemedicine for a wide range of emergency med-ical care situations including sea rescue,26,32 telephone-assisted cardiopulmonary resuscitation,33 management of acute stroke,25 as well as other areas of prehospital and hospital emergency medical care.15,27,34 Telemedicine is
thought to have the potential to improve patient care, espe-cially for those who reside in remote areas.22,35With the use of digital Web cameras and wireless LANs, physicians can interpret radiographs, electrocardiograms, and other labora-tory reports, which allow them to provide extra assistance to medical professionals in remote areas.
Cost Issues
The high cost of helicopter transfers presented in this study, as well as the extensive flying distance (200 – 400 miles) be-tween remote islands and mainland Taiwan add extra risks for air medical transport. In our study, the interventions in stage 2 resulted in a significant reduction of EAMT applications. The use of a cross-strait multi-telemedicine system for preflight screening significantly reduced the incidence of unnecessary transport. Our results of an approval rate of 91% and the 36.3% reduction in the rate of EAMT applications in this study are consistent with a report released by Haskins, who suggested that the use of telemedicine may result in a 15% reduction in ambu-lance transports.23
Before the establishment of NACC, almost all patients had been transported by air whenever local physicians re-quested. There had been no triage criteria. After the imple-mentation of NACC with a telemedicine system, primary care physicians on the remote islands have to perform basic triage. Doctors in NACC review the application document for EAMS and discuss with the local physician if the patient requires emergency chartered helicopter or if the patient can be scheduled for commercial flight or regular shuttle ferry. Crucial Roles of Physician Triage
The physicians in the NACC played crucial roles in this aspect. One of the major roles the physicians is being a gatekeeper for EAMT approval and transport quality. The system, including the protocols used, screening criteria, and the use of video telemedicine, is thought to have caused the reduction of EAMT applications. The video telemedicine system allows clear communications between physicians in the remote islands and the control center; hence physicians in the remote islands need to evaluate the necessity of urgent transfers before formal EAMT application.
Physicians in the NACC also provide support, guidance, and medical consultation to island-based physicians through our video system. The results of this study suggest that consultation with NACC physicians provides support to the already overburdened medical manpower on the remote is-lands. Sometimes physicians will suggest that the local phy-sician do some kind of intervention on patients, such as chest tapping for assisting in the decision-making process and eval-uating the adequacy of the management given or endotracheal intubation for safety of air transportation. Previous studies suggested that preflight medical screening of patients may assure both the patient and physician of the safety of air travel and prevent minimal complications such as in-flight morbid-ity and emergencies.36,37 On the other hand, patients in an
unstable condition being ground-transported by ambulance can minimize the chance of second problems such as hypox-emia and the consequent complications that might occur if they were transported by air.36
Difference Between NACC With Video-Telemedicine and Telephone With Fax Transmission
Patients who received treatment by physicians on the remote islands do not always have strong confidence. Most physicians on remote islands are in general practice and do not have specialized training, such as in neurologic surgery. For example, in the case of head injury, the local physician and the doctor in the NACC with video link can not only examine the patient simultaneously but also can interpret X ray, computed tomography scan, etc. This significantly enhanced the confidence of patients and the quality of man-agement. The present study demonstrates that the implemen-tation of this system is beneficial not only in medical care but also from an economic perspective. It overcomes the lack of emergent and critical care expertise by extending the avail-ability of physician expertise from Taiwan mainland. The patients may have confidence not only in the quality of care but also feel comfortable because they know that in any kind of situation they will be taken care continuously including EAMS.
Transferred by Fixed Wing or Ground and Sea Modalities
For the time being, the scheduled commercial flight and regular shuttle ferry do not accept any critical patient. The reasons are (1) the airlines and boat companies do not like to take the risk of medicolegal problems and (2) the cost of equip-ping aircraft and ferries with stretchers cannot be covered, even if the family were to buy 10 tickets for each patient.
Follow Up of the Patients
The eight patients who were transported by commercial airlines and shuttle ferries with their family had been followed up. All of them were in stable condition and came back to their home island and followed in outpatient department (OPD) by local physicians.
Our results show that patients requiring EAMT services were mostly elderly with major illnesses. Another benefit of the preflight screening is, apart from the benefit of reducing unnecessary transports, every critical patient is ensured of receiving sound, efficient, safe, and quality transport to major tertiary hospitals in Taiwan. Physician triage in this study resulted in fewer cross-zone transfers, and most patients were transferred to major tertiary medical centers or teaching hospi-tals. Of those who did not meet the criteria for emergency transfer, alternative forms of transport were arranged. The above results indicate the achievement of safer and better quality EAMT services in the second stage of this study period.
Dilemmas of Decision Making
The majority of patients in this study were categorized as having major illnesses. In our experience, patients with a major illness, i.e. stroke, ischemia, heart attack, or major burns, need to be evacuated from the small islands at the earliest possible time. It might be difficult to determine whether a patient with a minor stroke can safely remain on the island or requires immediate transfer to more advanced facilities. This often causes dilemmas in decision making for emergency transfers. In this study, the majority of patients were aged 61 to 75 years and 0 to 15 years, which suggests extra caution for possible transfer risks. In addition, the TMO might insist on an urgent evacuation because of the family’s pressure or other factors such as medicolegal problems or personnel shortages.
The criteria for air medical transfers also have limita-tions. The American College of Surgeons (1993) states that 50% overtriage is necessary to allow 10% undertriage to avoid improper transport of seriously injured patients to hos-pitals other than major trauma centers.38The objectives of the criteria are mainly to assist physicians in critical evaluation for making decisions on patient transfer in a timely way.
In conclusion, physician triage with the use of telemedi-cine significantly reduced the frequency of air medical trans-port. We verified the benefit of telemedicine that permits physicians in the control center to make accurate assessments and decisions concerning emergency air transport. The results of this study further demonstrate the benefits of EAMT pro-tocol and the use of telemedicine for producing potential cost savings, as well as assisting physicians in performing pre-flight screening of patients for safer and much-needed EAMT services. The reduced costs as well as fewer cross-zone trans-ports suggest an improvement in better-directed transtrans-ports and effective management of EAMT services in Taiwan.
ACKNOWLEDGMENTS
Contributors: SHT and HRW initiated the study. SHT, MFC, WMC, CCC, and LHL initiate the SOPs and the Guidelines for NACC. SHT and HRW drafted the report. HRW analyzed the data. CEC collected data and data analysis. SHT, WLC, and WTC interpreted the results and completed the overall discussion of this study.
REFERENCES
1. Kerr W, Kerns T, Bissell R. Differences in mortality rates among trauma patients transported by helicopter and ambulance in Maryland. Prehospital Disaster Med. 1999;14:159 –164.
2. Bureney RE. Efficiency, cost and safety of hospital-based emergency aeromedical programs. Ann Emerg Med. 1987;16:133–135.
3. Wills VL, Eno L, Walker C, Gani JS. Use of an ambulance-based helicopter retrieval service. Aust N Z Surg. 2000;70:506 –510. 4. Dewhurst A, Farrar D, Walker C, Mason P, Beven P, Goldstone
J. Medical repatriation via fixed-wing air ambulance: a review of patient characteristics and adverse events. Anaesthesia. 2001;56:882– 887. 5. Schiller W, Knox R, Zinnecker H, et al. Effect of helicopter
transport of trauma victims on survival in an urban trauma center.
6. Chappell V, Mileski W, Wolf S, Gore D. Impact of discontinuing a hospital-based air ambulance service on trauma patient outcomes.
J Trauma. 2002;52:486 – 491.
7. Hotvedt R, Kristiansen I, Forde O, et al. Which groups of patients benefit from helicopter evacuation? Lancet. 1996;18:1362–1366. 8. Rosenberg BL, Butz DA, Comstock MC, Taheri PA. Aeromedical
service: how does it actually contribute to the mission? J Trauma. 2002;54:681– 688.
9. Shatney CH, Homan SJ, Sherck JP, Ho C-C. The utility of helicopter transport of trauma patients from the injury scene in an urban trauma system. J Trauma. 2002;53:817– 822.
10. Boyd C, Corse K, Campbell R. Emergency interhospital transport of the major trauma patients: air versus ground. J Trauma. 2002; 29:789 –793.
11. Roth A, Malov N, Carthy Z, et al. Potential reduction of costs and hospital emergency department visits resulting from prehospital transtelephonic triage: the Shahal experience in Israel. Clin Cardiol. 2000;3:271–276.
12. American College of Emergency Physicians. Guidelines for trauma systems. Ann Emerg Med. 1987;16:459 – 463.
13. American College of Emergency Physicians. Guidelines for trauma care systems. Ann Emerg Med. 1993;22:1079 –1100.
14. Karlsen R, Sjoqvist B. Telemedicine and decision support in emergency ambulances in Uppsala. J Telemed Telecare. 2000; 6:1–7.
15. Plischke M, Wolf K, Lison T, Pretschner D. Telemedical support of prehospital emergency care in mass casualty incidents. Euro J Med
Res. 1999;4:394 –398.
16. Whitten PS, Mair FS, Haycox A, May CR, Wiliams TL, Hellmich S. Systematic review of cost effectiveness studies of telemedicine interventions. BMJ. 2002;324:1434 –1437.
17. Benger J. A review of telemedicine in accident and emergency: the story so far. Emerg Med J. 2000;17:157–164.
18. Debnath D. Activity analysis of telemedicine in the UK. Postgrad
Med J. 2004;80:335–338.
19. Benger J, Noble S, Coast J, Kendall J. The safety and effectiveness of minor injuries telemedicine. BMJ. 2004;21:438 – 445.
20. Armstrong IJ, Haston WS. Medical decision support for remote general practitioners using telemedicine. J Telemed Telecare. 1997; 2:27–34.
21. Meade B, Barnett P. Emergency care in a remote area using interactive video technology: a study in prehospital telemedicine.
J Telemed Telecare. 2002;8:115–117.
22. Saffle JR, Edelman L, Morris S. Regional air transport of burn patients: a case for telemedicine? J Trauma. 2004;57:57– 64.
23. Haskins P, Ellis D, Mayrose J. Predicted utilization of emergency medical services telemedicine in decreasing ambulance transports.
Prehosp Emerg Care. 2002;6:445– 448.
24. Armstrong I, Haston W. An evaluation of telemedical support for a minor treatment centre. J Telemed Telecare. 1996;2:93–99. 25. Handschu R, Littmann R, Reulbach U, et al. Telemedicine in
emergency evaluation of acute stroke: interrater agreement in remote video examination with a novel multimedia system. Stroke. 2003; 34:2842–2846.
26. Patel T. A cost-benefit analysis of the effect of shipboard telemedicine in a selected oceanic region. J Telemedicine Telecare. 2000;6:165–167. 27. Kofos D, Pitetti R, Orr R, Thompson A. Telemedicine in pediatric
transport: a feasibility study. Pediatrics. 1998;102:E58. 28. Tsai SH, Tsang C-M, Wu H-R, et al. Transporting patients with
suspected SARS. Emg Inf Dis. 2003;10:1325–1326. 29. Association of Air Medical Services. Medical Air Transport
Guidelines: Criteria for Emergency Air Medical Transport
Utilization. 1990[cited on February 22, 2000]. Available from: http://
www.providence.org/alaska/lifeguard/guidelines.htm.
30. Air Medical Services Committee of the National Association of EMS Physicians. Criteria for Prehospital Air Medical Transport: Non-Trauma and Pediatric Considerations. Prehospital Disaster Med. 1994;9:140–141. 31. Department of Human Services. Review of Trauma and Emergency
Services 1999: Final report.[cited on 2005 Feb 22]. Available from:
http://www.health.vic.gov.au/trauma/review99.
32. Prina L, Orzai U, Weber R. Evaluation of emergency air evacuation of critically ill patients from cruise ships. J Travel Med. 2002;8:285–292. 33. Hauff S, Rea T, Culley L, Kerry F, Becker L, Eisenbery M. Factors
impeding dispatcher-assisted telephone cardiopulmonary resuscitation. Ann Emerg Med. 2003;42:731–737.
34. Wang LM, Huang YT, Chern CH, et al. Tele-emergency medicine; the evaluation of Taipei veterans general hospital and Kinmen-granite hospital in Taiwan. Chinese Med J (Taipei). 2001;64:621– 628. 35. Hood M. Crisis in the countryside, networking and telemedicine are
crucial for health care facilities in rural America. Health Progress. 2004;85:16 –19.
36. Gong H, Mark JAL, Cowan MN. Preflight medical screening of patients: analysis of health and flight characteristics. Chest. 1993; 104:788 –794.
37. Lyznicki J, Williams M, Deitchman S, Howe JP Jr, Council on Scientific Affairs, American Medical Association. Inflight medical emergencies. Aviat Space Environ Med. 2000;71:832– 838. 38. American College of Surgeons. Resources for Optimal Care of the
Injured Patient. Chicago: Committee on Trauma, American College