I
NTERESTING
I
MAGE
Feasible Method to Successfully Uncover a Urothelial Carcinoma
in the Urinary Bladder on the FDG PET/CT Scan Masked by
Physiological Urine Radioactivity
Yeh-You Shen, MD,*† Chia-Hung Kao, MD,‡§ Li-Hao Yeh, MD,* Guang-Dar Juang, MD,†¶ Ji-An Liang, MD,
储
and Te-Chun Hsieh, MD**‡
Abstract: A 71-year-old man asked for a F-18 fluorodeoxyglucose positron
emission tomography/computed tomography (FDG PET/CT) scan for fol-low-up of the renal cell carcinoma of right kidney after nephrectomy 2 years ago. Except for normal radioactivity outside the urinary system, however, a CT abnormality in the urinary bladder was noted but its character of metabolic activity was interfered with by the abundant physiological urine FDG radioactivity. After a simple procedure with intravenous administration of diuretics and asking the patient to hold his urine, the lesion emerged as an area of focal intense radioactivity after the dilute effect of the urine. The subsequent histologic examination via the cystoscopic biopsy revealed pap-illary urothelial carcinoma.
Key Words: FDG PET, urothelial carcinoma, diuresis, hold urine,
dilution
(Clin Nucl Med 2010;35: 464 – 466)
REFERENCES
1. Kosuda S, Kison PV, Greenough R, et al. Preliminary assessment of fluo-rine-18 fluorodeoxyglucose positron emission tomography in patients with bladder cancer. Eur J Nucl Med. 1997;24:615– 620.
2. Lin WY, Wang KB, Tsai SC, et al. Unexpected accumulation of F-18 FDG in the urinary bladder after bladder irrigation and retrograde filling with sterile saline: a possible pitfall in PET examination. Clin Nucl Med. 2009;34:560 – 563.
3. Leisure GP, Vesselle HJ, Faulhaber PF, et al. Technical improvements in fluorine-18-FDG PET imaging of the abdomen and pelvis. J Nucl Med Technol. 1997;25:115–119.
4. Vesselle HJ, Miraldi FD. FDG PET of the retroperitoneum: normal anatomy, variants, pathologic conditions, and strategies to avoid diagnostic pitfalls. Radiographics. 1998;18:805– 823; discussion 823– 824.
5. Kibel AS, Dehdashti F, Katz MD, et al. Prospective study of关18F兴 fluorodeoxy-glucose positron emission tomography/computed tomography for staging of muscle-invasive bladder carcinoma. J Clin Oncol. 2009;27:4314 – 4320. 6. Kamel EM, Jichlinski P, Prior JO, et al. Forced diuresis improves the
diag-nostic accuracy of 18F-FDG PET in abdominopelvic malignancies. J Nucl Med. 2006;47:1803–1807.
7. Anjos DA, Etchebehere EC, Ramos CD, et al. 18F-FDG PET/CT delayed images after diuretic for restaging invasive bladder cancer. J Nucl Med. 2007;48:764 –770.
8. Wang KB, Tu DG, Huang SS. The identification of a tumor of the cervix on PET/CT with bladder filling and emptying. Clin Nucl Med. 2009;34:296 –297. 9. Sun SS, Chang CH, Ding HJ, et al. Preliminary study of detecting urothelial malignancy with FDG PET in Taiwanese ESRD patients. Anticancer Res. 2009;29:3459 –3463.
Received for publication December 20, 2009; revision accepted February 16, 2010.
From the *Department of Nuclear Medicine, Shin Kong Wu Ho-Su Hospital, Taipei, Taiwan; †School of Medicine, College of Medicine, FuJen Catholic University, HsinChung, Taipei, Taiwan; ‡Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung, Taiwan; §School of Medicine, China Medical University, Taichung, Taiwan; ¶Depart-ment of Urology, Shin Kong Wu Ho-Su Hospital, Taipei, Taiwan; 㛳Depart-ment of Radiation Therapy and Oncology, China Medical University Hospital, Taichung, Taiwan; and **Department of Biomedical Imaging and Radiolog-ical Science, China MedRadiolog-ical University, Taichung, Taiwan.
Reprints: Te-Chun Hsieh, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2, Yuh-Der Rd, Taichung 404, Taiwan. E-mail: [email protected].
Copyright © 2010 by Lippincott Williams & Wilkins ISSN: 0363-9762/10/3506-0464
Clinical Nuclear Medicine • Volume 35, Number 6, June 2010 464 | www.nuclearmed.com
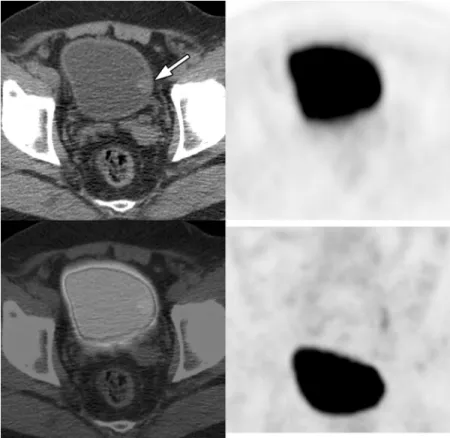
FIGURE 1. A 71-year-old man had undergone right nephrectomy for renal cell carcinoma about 2 years ago without
symp-toms and signs suggestive of recurrence during the regular follow-up. Recently, he asked for a FDG PET/CT scan for a com-prehensive survey and follow-up of the post-treatment condition of malignancy. The FDG PET/CT was performed 60 minutes after intravenous administration of FDG to the patient with a low radiation dose, freely breathing, noncontrast enhanced CT acquisition protocol. The whole body images revealed absence of the right kidney and no significant FDG-avid abnormality outside the urinary system. At first glance, the FDG radioactivity in the urinary bladder was intense and homogeneous (maxi-mum standardized uptake value, SUVmax⫽ 13), revealing a usual physiological pattern of urinary excretion. However, the CT component of the FDG PET/CT scan disclosed a focal hypodense (Hounsfield unit, HU⫽ 53) protuberance from the left inner wall of the urinary bladder (arrow), which was easily distinguished from the adjacent urine density (HU was about 0 –5). (The arrangement of the panels in Figures 1 and 2 are the same as follows: left upper panel indicates representative transaxial slice of CT scan; right upper panel, representative transaxial slice of FDG PET scan; left lower panel, representative transaxial slice of fused FDG PET/CT scan; right lower panel, maximum intensity projection of FDG PET scan).
Clinical Nuclear Medicine • Volume 35, Number 6, June 2010 Method to Uncover a Urothelial Carcinoma
FIGURE 2. For further discrimination of the CT finding with the assistance of reliable FDG metabolic activity, a delayed scan
was obtained 60 minutes after the bolus intravenous administration of the diuretic (20-mg furosemide). The time interval be-tween the initial and delayed scans was 75 minutes. No additional fluid was given either via the intravenous infusion or oral intake after the administration of the diuretics. The patient was also asked to void immediately after the initial scan and then hold the urine until the delayed scan was finished. The delayed scan showed much lowered intensity of the urine radioactivity (SUVmax⫽ 1.6) in contrast to the highlighted left bladder wall lesion (arrows; SUVmax ⫽ 8.0). The high FDG uptake strongly suggested its malignant origin. Further histologic examination of the lesion via cystoscopic biopsy proved a low-grade papil-lary urothelial carcinoma.
To correctly measure the actual metabolic activity of the intravesical or perivesical lesion is important for the differential diagnosis and depends on the capability of removing the influence of abundant physiological urinary FDG radioactivity. For this purpose, several methods have been advocated, including retrograde saline irrigation of the urinary bladder,1,2combined
use of diuretics, intravenous saline infusion and bladder catheters,3–5combined use of furosemide forced diuresis and
paren-teral hydration,6and combined use of furosemide forced diuresis, oral hydration and frequent voiding.7,8On the contrary, it
seems less problematic for anuric patients such as those with end-stage renal disease because of the better contrast of the tu-mor uptake and background radioactivity.9Although several methods to decrease the interference of urine radioactivity have
been proposed, they are either too invasive or labor intensive for the combination of multiple procedures to be routinely ap-plied. On the other hand, our patient only received additional diuretics after voiding immediately after the initial scan for eliminating the high concentrated radiopharmaceuticals, and then diluted the urine radioactivity with the subsequently physi-ologically produced low radioactive urine. The additional 1-step procedure is feasible and noninvasive, and may be more prac-tical for routine use of detecting an intravesical or perivesical lesion, especially in a busy nuclear medicine department. This case also highlights the need to carefully review the CT component of FDG PET/CT scan in case omission of morphologically evident lesions is masked by the abundant physiological FDG radioactivity.
Shen et al Clinical Nuclear Medicine • Volume 35, Number 6, June 2010
466 | www.nuclearmed.com © 2010 Lippincott Williams & Wilkins