Comparison of FDG-PET and 99mTc-MIBI scintigraphy in detecting metastatic well differentiated thyroid carcinoma with negative 131I-whole body scan
6
0
0
全文
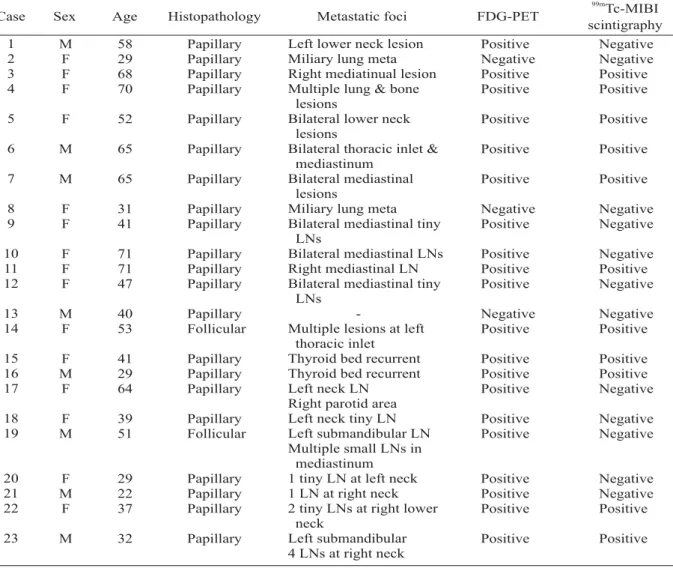
(2) Te-Chun Hsieh, et al.. 45. Table 1. FDG-PET and 99mTc MIBI scintigraphy results 99m. Case. Sex. Age. Histopathology. Metastatic foci. FDG-PET. 1 2 3 4. M F F F. 58 29 68 70. Papillary Papillary Papillary Papillary. Positive Negative Positive Positive. 5. F. 52. Papillary. Positive. Positive. 6. M. 65. Papillary. Positive. Positive. 7. M. 65. Papillary. Positive. Positive. 8 9. F F. 31 41. Papillary Papillary. Negative Positive. Negative Negative. 10 11 12. F F F. 71 71 47. Papillary Papillary Papillary. Positive Positive Positive. Negative Positive Negative. 13 14. M F. 40 53. Papillary Follicular. Negative Positive. Negative Positive. 15 16 17. F M F. 41 29 64. Papillary Papillary Papillary. Positive Positive Positive. Positive Positive Negative. 18 19. F M. 39 51. Papillary Follicular. Positive Positive. Negative Negative. 20 21 22. F M F. 29 22 37. Papillary Papillary Papillary. Positive Positive Positive. Negative Negative Positive. 23. M. 32. Papillary. Left lower neck lesion Miliary lung meta Right mediatinual lesion Multiple lung & bone lesions Bilateral lower neck lesions Bilateral thoracic inlet & mediastinum Bilateral mediastinal lesions Miliary lung meta Bilateral mediastinal tiny LNs Bilateral mediastinal LNs Right mediastinal LN Bilateral mediastinal tiny LNs Multiple lesions at left thoracic inlet Thyroid bed recurrent Thyroid bed recurrent Left neck LN Right parotid area Left neck tiny LN Left submandibular LN Multiple small LNs in mediastinum 1 tiny LN at left neck 1 LN at right neck 2 tiny LNs at right lower neck Left submandibular 4 LNs at right neck. Tc-MIBI scintigraphy Negative Negative Positive Positive. Positive. Positive. (WBS) have been widely used for follow-up of patients with well differentiated thyroid carcinoma (DTC) after nearly total thyroidectomy and 131I treatment [1-4]. Although 131I WBS has a very high specificity of 99% to 100%, 131 I recurrences in WBS-positive cases is about 50% to 60% in papillary and 64% to 67% in follicular thyroid cancer [2,5-6]. Patients with elevated hTg levels but negative 131I WBS, are not usually treated with high-dose 131I. Accurate localization of metastatic lesions is therefore very important since they need to be removed surgically or treated with external radiotherapy. Non-specific radiopharmaceuticals, such as 201Tl chloride, 99mTc methoxysiobutyl isonitrile ( 99mTc MIBI) and. positron emission tomography (PET) with 2[18F]fluoro-2-deoxy-D-glucose (FDG) have been shown to be valuable [7-19]. This study was designed to assess the clinical usefulness of 99mTc MIBI scintigraphy and FDG-PET in the followup of patients with differentiated thyroid cancer who present with increased hTg levels and negative 131I scans. PATIENTS AND METHODS. Patients. The study group was composed of 23 patients (15 women, 8 men; age 22-71, median 47 years) with DTC (20 papillary-type and 3 follicular-type) who underwent nearly total.
(3) 46. FDG-PET and. 99m. Tc-MIBI Scintigraphy in Detecting Metastatic DTC. Table 2. Diagnostic values of FDG-PET and 99mTc-MIBI scintigraphy. Sensitivity (%). Specificity (%). Accuracy (%). 90.9 50.0. 100 100. 91.3 52.2. FDG-PET 99m Tc-MIBI scintigraphy. thyroidectomy and radioiodine ablation therapy. All had negative 131I WBS scans and elevated hTg levels (hTg ≥ 2.0 ng/mL) under thyroidstimulating hormone (TSH) stimulation (TSH ≥ 30 µgIU/mL). 99m. Tc MIBI Scan and FDG-PET. Ten minutes after a bolus injection of 740 MBq (20 mCi) 99mTc MIBI, whole body scan and SPECT of the head and chest were performed. The images were recorded by a dual-head gamma camera and a low-energy high-resolution collimator appropriate for low (less than 180 keV) energy levels. All patients fasted for at least 6 hours prior to the whole-body FDG-PET study. The FDG-PET study was performed 45 minutes after a bolus injection of 370 MBq (10 mCi) of FDG by either a Siemens-CTI EXACT HR + PET scanner (Siemens Medical systems, Iselin, NJ, USA; CTI Knoxville, TN, USA) or a GE Advance PET system (General Electric, Milwaukii, WI, USA). Interpretation of FDG-PET and 99mTc MIBI scans was based on visual analysis by two experienced nuclear medicine physicians without prior knowledge of the results of the other examinations. Lesions showing 99mTc MIBI uptake or FDG metabolism greater than the radioactivity of the neighboring background were considered to be positive. RESULTS 99m. FDG-PET and Tc MIBI scintigraphy results and the patients' characteristics are summarized in Table 1. FDG-PET detected abnormal hypermetabolic lesions in 20 patients. In 11 patients, all of the lesions detected by 99mTc MIBI had also been detected by FDG-PET. There were 9 patients whose FDG-PET scans were positive but whose 99mTc MIBI scintigraphy scans were negative. However, in one patient (patient 17) 99mTc MIBI scintigraphy demonstrated a lesion. on the left side of the neck but missed the lesion in the right parotid region. Both FDG-PET and 99m Tc MIBI scintigraphy failed to demonstrate any lesion in 3 patients. However, X-ray computed tomography (CT) showed miliary pulmonary nodules in two of these patients (patient 2 and patient 8). No lesions were detected by chest CT or any other imaging studying in the other patient (patient 13). Close follow-up over the past 10 months has shown that the patient has remained disease free. The diagnostic values of these two imaging modalities are listed in Table 2. DISCUSSION 131. A combination of I WBS and the determination of serum hTg levels has been suggested for the follow up care of differentiated thyroid carcinoma patients treated by total or nearly total thyroidectomy followed by 131I plus thyroid hormone therapy [1-4]. A positive 131I scintigraphy also indicates that 131I is useful in the treatment of recurrent or metastatic lesions. However, for those patients with elevated hTg levels but negative 131 I scintigraphy, early determination of metastatic lesions is difficult, but very important. Radical surgery, external radiotherapy or redifferentiation therapy can be performed if the lesions can be identified. In these cases, the metastatic foci lose the ability to take up 131I because of dedifferentiation of the cancer cells. Both 99mTc MIBI scintigraphy and FDG-PET have been demonstrated to be useful in these situations. 99m Tc MIBI has been found to accumulate in various tumor cell types, including DTC. The cationic charge and lipophilicity of 99mTc MIBI, the mitochondrial and plasma membrane potentials of the tumor cells, and the cellular mitiochondrial content are all considered to play significant roles in the mechanism of tumor.
(4) Te-Chun Hsieh, et al.. uptake of this agent [20]. FDG-PET has also been found to be a valuable imaging modality in detecting metastatic lesions in patients with DTC who present with elevated hTG and negative 131I WBS levels [11,13,21]. For the detection of metastatic DTC, studies have found that 99mTc MIBI [7] and FDG [11,21] accumulated more often in lesions in which 131I had failed to accumulate. It was suggested that FDG uptake and concomitant loss of 131I uptake is a sign of dedifferentiation of the cancer cells [11,15,21,22]. In this study, we observed that FDG-PET was more sensitive than 99mTc MIBI scintigraphy in these cases. The FDGpositive/MIBI-negative lesions tended to be small-sized including tiny lesions in the mediastinum in 4 patients. Our results are understandable since PET scanners have a higher spatial resolution than SPECT images from a dual-head gamma camera. Moreover, 99mTc MIBI scintigraphy missed 2 lesions (patient 17 at right parotid and patient 19 at left submandibular) close to the salivary glands. This could have been due to interference by the physiological uptake of 99m Tc MIBI in these glands. Both 99mTc MIBI scintigraphy and FDGPET were performed in this study without TSH stimulation. Although the influence of TSH on 99m Tc MIBI and FDG uptake in DTC cells remains to be determined, Mueller et al [23] reported that the uptake of 99mTc MIBI in thyroid carcinoma was independent of TSH stimulation while higher sensitivity of FDG-PET under high TSH levels was not observed [18,21]. In our study, 2 patients with miliary pulmonary metastases were verified by spiral CT. Neither FDG-PET nor 99mTc MIBI SPECT were able to differentiate the region of elevated uptake from normal lung background. In these circumstances, spiral CT should be included in the follow-up protocol. This study showed that FDG-PET is more sensitive than 99m Tc MIBI scintigarphy in detecting metastatic lesions in DTC patients with elevated hTg but negative 131I WBS. FDG-PET can detect smaller-sized lesions than 99mTc MIBI. 47. sintigarphy can, especially in the mediastinal lymph nodes; however, both modalities may miss miliary pulmonary metastasis. REFERENCES. 1. Ronga G, Fiorentino A, Paserio E, et al. Can iodine131 whole-body scan be replaced by thyroglobulin measurement in the post-surgical follow-up of differentiated thyroid carcinoma? J Nucl Med 1990; 31:1766-71. 2. Lubin E, Mechlis-Frish S, Zatz S, et al. Serum thyroglobulin and iodine-131 whole-body scan in the diagnosis and assessment of treatment for metastatic differentiated thyroid carcinoma. J Nucl Med 1994; 35:257-62. 3. Roelants V, Nayer PD, Bouckaert A, et al. The predictive value of serum thyroglobulin in the follow-up of differentiated thyroid cancer. Eur J Nucl Med 1997; 24:722-7. 4. Filesi M, Signore A, Ventroni G, et al. Role of initial iodine-131 whole body scan and serum thyroglobulin in differentiated thyroid carcinoma metastases. J Nucl Med 1998;39:1542-6. 5. Galloway RJ, Smallridge RC. Imaging in thyroid cancer. [Review] Endocrinol Metab Clin North Am 1996;25: 93-113. 6. Samaan NA, Schultz PN, Haynie TP, et al. Pulmonary metastasis of differentiated thyroid carcinoma: treatment results in 101 patients. J Clin Endocrinol Metab 1985;60: 376-80. 7. Miylamoto S, Kasagi K, Misaki T, et al. Evaluation of techentium-99m-MIBI scintigraphy in metastatic differentiated thyroid carcinoma. J Nucl Med 1997; 38:352-6. 8. Ng DC, Sundram FX, Sin AE. 99mTc-sestamibi and 131 I whole-body scintigraphy and initial serum thyroglobulin in the management of differentiated thyroid carcinoma. J Nucl Med 2000;41:631-5. 9. Seabold JE, Gurll N, Schurrer ME, et al. Comparison of 99m Tc-methoxyisobutyl isonitrile and 201 Tl scintigraphy for detection of residual thyroid cancer after 131I ablative therapy. J Nucl Med 1999;40:143440. 10.Rubello D, Mazzarotto R, Casara D. The role of techentium-99m methoxyisobutylisonitrile scintigraphy in the planning of therapy and follow-up of patients with differentiated thyroid carcinoma after surgery. Eur J Nucl Med 2000;27:431-40. 11. Grunwald F, Schomburg A, Bender H, et al. Fluorine-.
(5) 48. FDG-PET and. 18 fluorodeoxyglucose positron emission tomography in the follow-up of differentiated thyroid cancer. Eur J Nucl Med 1996;23:312-9. 12. Dietlein M, Scheidhauer K, Voth E, et al. Fluorine-18 fluorodeoxyglucose positron emission tomography and iodine-131 whole-body scintigraphy in the followup of differentiated thyroid cancer. Eur J Nucl Med 1997;24:1342-8. 13. Chung JK, So Y, Lee JS, et al. Value of FDG-PET in 131 papillary thyroid carcinoma with negative I wholebody scan. J Nucl Med 1999;40:986-92. 14. Alnafisi NS, Driedger AA, Coates G, et al. FDG-PET of recurrent or metastatic 131I-negative papillary thyroid carcinoma. J Nucl Med 2000;41:1010-5. 15. Schluter B, Bohuslavizki KH, Beyer W, et al. Impact of FDG-PET on patients with differentiated thyroid cancer who present with elevated thyroglobulin and negative 131I scan. J Nucl Med 2001;42:71-6. 16. Grunwald F, Kalicke T, Feine U, et al. Fluorine-18 fluorodeoxyglucose positron emission tomography in thyroid cancer: results of a multicentre study. Eur J Ncul Med 1999;26:1547-52. 17. Dietlein M, Scheidhauer K, Voth E, et al. Fluorine-18 fluorodeoxyglucose positron emission tomography and iodine-131 whole-body scintigraphy in the follow-. 99m. Tc-MIBI Scintigraphy in Detecting Metastatic DTC. up of differentiated thyroid cancer. Eur J Ncul Med 1997;24:1342-8. 18. Grunwald F, Menzel C, Bender H, et al. Comparison of 18FDG-PET with 131Iodine and 99mTc-sestamibi scintigraphy in differentiated thyroid cancer. Thyroid 1997;7:327-35. 19. Fridrich L, Messa C, Landoni C, et al. Whole-body scintigraphy with 99Tc m-MIBi, 18F-FDG and 131I in patients with metastatic thyroid carcinoma. Nucl Med Commun 1997;18:3-9. 20. Chiu ML, Kronauge JF, Piwnica-Worms D. Effect of mitochondrial and plasma membrane potentials on accumulation of hexakis (2-methoxyisobutylisonitrile) technetium(I) in cultured mouse fibroblasts. J Nucl Med 1990;31:1646-53. 21. Feine U, Lietzenmayer R, Hanke JP, et al. Fluorine-18FDG and iodine-131-iodide uptake in thyroid cancer. J Nucl Med 1996;37:1468-72. 22. Joensuu H, Ahonen A. Imaging of metastases of thyroid carcinoma with fluorin-18 fluorodeoxyglucose. J Nucl Med 1987;28:910-4. 23. Mueller SP, Piotrowski B, Guth-Tougelides B, et al. Tc-99m MIBI and Tl-201 uptake in thyroid carcinoma. [Abstract] J Nucl Med 1988;29(supp):854..
(6) 49. -18. 131 1. 2. 1 2. 99m-MIBI. -18 -131. 23 71. 20. ( 3. 15. ). 131. 8. 22. 23 131. (TSH ≥ 30 µIU/mL) 2.0 µIU/mL). (hTg ≥. 99m-MIBI. -18. -18. 23. 99m-MIBI. 20. 11. 99m-MIBI. -18. 2 99m-MIBI. 23 -18 10. 131. -18 99m-MIBI. -18. 99m-MIBI 99m-MIBI. -18 2004;9:44-9. -18. 99m-MIBI. 404. 2. 2004. 1. 14. 2004. 3. 1. 2004. 2. 20.
(7)
數據
相關文件
The aim of this case report is to present the clinical and radiographic features of a 35-year-old female patient with autosomal dominant osteopetrosis type II who exhibited features
SUMMARY The purpose of this systematic review was to describe the prevalence of whiplash trauma in patients with temporomandibular disorders (TMDs) and to describe clinical signs
pylori in pathogenesis of oral mucosal lesions or ulcerations is still unclear, it seems that patients with oral lesions as leukoplakia and oral lichen planus, and concurrent
Lingual thyroid is defined as an ectopic thyroid gland tissue located in the midline of the tongue base and it is uncommonly observed in clinical practice and is rare in children..
To evaluate the clinicopathologic features, prognostic factors, and management of patients in the North Chinese population with head and neck squamous cell carcinoma (HNSCC)
E ffective utilization of dental and zygomatic implants may help to restore oral function in patients with severe maxillary defects.. This clinical report describes the management
Objectives This study investigated the clinical effectiveness of intervention with an open-mouth exercise device designed to facilitate maximal interincisal opening (MIO) and
A prospective study of magnetic resonance and radiographic imaging in relation to symptoms and clinical findings of the temporomandibular joint in children with juvenile
