Uterine artery ligation for treatment of pregnant
women with uterine leiomyomas who are undergoing
cesarean section
Wei-Min Liu, M.D.,aPeng-Hui Wang, M.D., Ph.D.,bWun-Long Tang, M.D.,aI-Te Wang, M.D.,a and Chii-Reuy Tzeng, M.D.a
aDepartment of Obstetrics and Gynecology, Taipei Medical University Hospital and Taipei Medical University andbDepartment of Obstetrics and Gynecology, Taipei Veterans General Hospital and Institute of Emergency Medicine and Critical Care, National Yang-Ming University School of Medicine, Taipei, Taiwan
Objective: To evaluate the therapeutic effects of uterine artery ligation for pregnant women with uterine leiomyomas, who are undergoing cesarean section.
Design: Prospective clinical study without randomization. Setting: University-affiliated tertiary referral center.
Patient(s): Forty-eight women with uterine leiomyomas undergoing cesarean section for obstetric reasons were enrolled into the study. Diagnosis was established with ultrasound before or during early pregnancy.
Intervention(s): Ligation of the bilateral uterine arteries was performed immediately after closure of the uterine incision wound.
Main Outcome Measure(s): Blood loss during cesarean section, dominant leiomyoma size, and future surgical intervention for symptomatic leiomyoma.
Result(s): Twenty-six (54%) of 48 patients underwent uterine artery ligation during cesarean section (group I), and 22 (46%) received cesarean section only (group II). The average follow-up time was 38.5 months. The average blood loss during surgery was 254⫾ 92.3 mL for group I and 278 ⫾ 160.5 mL for group II. Hemoglobin on the first postoperative day was 11.2⫾ 0.9 g/dL for group I and 10.4 ⫾ 1.1 g/dL for group II. One patient in group II required blood transfusion due to hemorrhage. Two patients (7.7%) in group I and 9 (40.9%) in group II underwent myomectomy or hysterectomy for symptomatic leiomyomas within 6 –38 months after cesarean section. Reductions in the dominant myoma size (average: 45%) were demonstrated in group I patients postoperatively. Four patients (15.4%) in group I and three (13.6%) in group II had a repeat cesarean section during the follow-up period.
Conclusion(s): Uterine artery ligation appears to be a promising method for treating pregnant women with uterine leiomyomas, who are undergoing cesarean section, because it is able to reduce postpartum blood loss and minimize the necessity of future surgery. Fertility is apparently not compromised by this treatment, which offers obstetricians with another choice between observation and myomectomy for pregnant women with leiomyomas who are undergoing cesarean section. (Fertil Steril威 2006;86:423–8. ©2006 by American Society for Repro-ductive Medicine.)
Key Words: Cesarean section, myomectomy, uterine artery ligation, uterine leiomyoma
The probability of the occurrence of uterine leiomyomas during pregnancy is reported to be 2% (1). With the increas-ing age of obstetric patients, obstetricians generally encoun-ter more cases of uencoun-terine leiomyomas. Although most leiomyomas remain asymptomatic, they may still complicate the course of the pregnancy to a certain degree. Myomec-tomy during cesarean section has traditionally been discour-aged because of the risk of intractable intrapartum hemor-rhage. Some obstetricians believe that with careful case selection, myomectomy at cesarean section may be safe
(2–5). However, the management of uterine leiomyomas encountered during cesarean delivery still poses a therapeu-tic dilemma for today’s obstetricians.
Since the introduction in 2000 of uterine artery occlu-sion for treating uterine leiomyomas (6), many studies have shown this procedure to be efficacious (7–10). In an attempt to evaluate the benefits of uterine artery ligation during cesarean section for women with uterine leiomyo-mas, we kept a detailed record of these patients for a period of approximately 6 years. Our objectives were threefold: [1] to evaluate whether uterine artery ligation at time of cesarean delivery leads to a reduction of intraop-erative or postopintraop-erative hemorrhage; [2] to determine whether uterine artery ligation can decrease the necessity of future surgical treatment; and [3] to measure the re-duction percentage of the dominant uterine myomas in
Received September 15, 2005; revised and accepted January 3, 2006. Partly supported grants from Taipei Veterans General Hospital and Taipei
Medical School University.
Reprint requests: Wei-Min Liu, M.D., Department of Obstetrics and Gy-necology, Taipei Medical University Hospital and Taipei Medical Uni-versity, No.252, Wusing St., Sinyi District, Taipei 110, Taiwan (FAX: 886-2-2735-8406; E-mail: [email protected]).
423
comparison with their initial size. This report summarizes our findings.
MATERIALS AND METHODS Patients and Indications
Between March 1999 and March 2004, 65 patients were enrolled into this prospective clinical study. To make this study even more uniform and consistent, the following pa-tients of the original 65 were excluded: 3 with placenta previa, 1 with abruptio placentae, 4 with preterm labor, 6 patients with a dominant leiomyoma less than 5 cm in size, and 3 who were lost to follow-up. We recruited the remain-ing 48 patients, aged 26 to 41 years (mean: 32.8 years), each of whom had a documented dominant myoma larger than 5 cm, using an antepartum or the first intrapartum ultrasound examination, and no co-morbid conditions with evidence of coagulopathy. Multiple myomas were present in 29 (60.4%) cases.
Because uterine artery ligation in the treatment of uterine leiomyomas is a novel technique, the outcome of uterine and ovarian function and fertility outcome after surgery are not well known. After our patients had received clear explana-tions, those willing to undergo uterine artery ligation during cesarean section were placed in the study group (group I; n⫽ 26), and those unwilling to try this new technique, but who would undergo cesarean section only with postpartum follow-up of myomas, were placed in a control group (group II; n⫽ 22). The patients were all extensively counseled regard-ing possible surgical risks, current and future benefits, and curative nature and fertility issues related to uterine artery ligation. Institutional Review Board approval was obtained by the Department of Obstetrics and Gynecology, Taipei Medical University Hospital. Written informed consent was obtained from all patients enrolled into this study.
All patients in group I were counseled, and each gave their consent for possible surgical intervention if uterine artery ligation failed to resolve the leiomyoma-related symptoms after delivery. All cesarean sections were indicated as per-formed for standard obstetric reasons.
Operative Procedures
Laparatomy was performed with a Pfannenstiel incision. In the group I patients, a lower uterine segment transverse cesarean section was first completed. Then, bilateral uterine arteries were double-ligated with silks, as described by Liu et al. (11) in the treatment of symptomatic uterine leiomas, combining the uterine depletion procedure and myo-mectomy. A vertical incision of 3 cm was made on the triangular area enclosed by the round ligament, external iliac artery, and infundibulopelvic ligament. With the aid of a retractor (Courtesy of Zinnati Surgical Instruments, Chats-worth, CA), the ureter was medially compressed, isolating the uterine artery from the ureter and the internal iliac artery. This procedure is easily accomplished during cesarean
sec-tion because the retroperitoneal avascular space between the broad ligaments is more visible and loose during pregnancy. In the control group II patients, a lower uterine segment transverse cesarean section was completed in the same way as with the group I patients, except for one patient who had an anterior low segment myoma measuring 7 cm in size. For this case, we performed a vertical incision to deliver the baby, and left the myoma in situ without removing it.
In each patient, after delivery of the baby and placenta, 30 IU of oxytocin in a 500-mL dextrose solution was infused at a rate of 60 U/min in both groups. Bimanual uterine massage was performed on some patients in both groups to promote uterine contraction.
Assessments
Intraoperative blood loss was estimated by calculating the blood volume of the suction machine and the weight change of the gauze used during surgery (12). Preoperative basal and postop-erative first day hemoglobin levels were recorded in all patients. All patients underwent postoperative monthly evaluations of leiomyoma size measurements for 3 months after cesarean section, then evaluations every 3 months for at least 1 year, followed by evaluations every 6 months for an average of 38.5 months. Longitudinal, anteroposterior, and transverse measure-ments of the dominant leiomyoma were obtained for all pa-tients. The volume of the dominant leiomyoma was calculated by using a sector scanner (GateWay; Diasonics, Milpitas, CA) to measure the three largest dimensions (A, B, and C) and applying the formula for a prolate ellipsoid (0.5233 by A by B by C), as described elsewhere (13, 14). The volume reduction percentage of the dominant leiomyoma was calculated for each patient. The follow-up time was at least 1 year, averaging 38.5 months after cesarean section.
Statistical Analysis
The SPSS (version 11.5; SPSS Inc., Chicago, IL) statistical software was used for analyzing the patient data. Data were presented with a mean⫾ standard deviation. A parametric-independent samples t test was used to compare differences between the two groups, and2analysis was used for cate-gorical variables. The level of statistical significance was set at a P⬍.05.
RESULTS
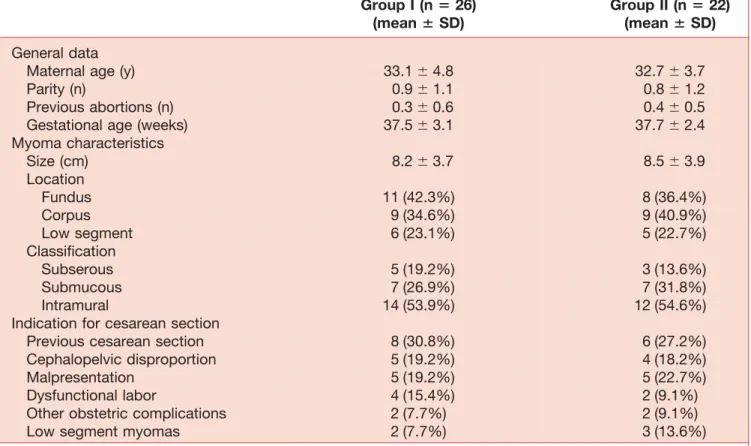
This research report involved 48 patients who were entered into our analysis during the study period. All underwent technically successful surgery and completed follow-up in-quiries during a period of 12– 60 months (average follow-up time: 38.5 months). Twenty-six (54%) of 48 patients under-went ligation of the bilateral uterine arteries during cesarean section (group I), and 22 (46%) received cesarean section only (group II). The mean ⫾ SD age of group I was 33.1 ⫾ 4.8 years and the mean ⫾ SD age of group II was 32.2 ⫾ 3.7 years (Table 1). Both groups were similar in terms of
mean age, parity, previous abortions, and gestational age. The mean size of the dominant myoma in group I was 8.2⫾ 3.7 cm (range: 5.0 –16.5 cm). In group II, the mean size was 8.5⫾ 3.9 cm (range: 5.0 –15.0 cm). The dominant myoma position and location were similar in both groups (Table 1). Indications for cesarean section in both groups are shown inTable 1, and included previous cesarean section, cephalopelvic dispropor-tion, malpresentadispropor-tion, dysfunctional labor, other obstetric complications, and large low-segment myomas.
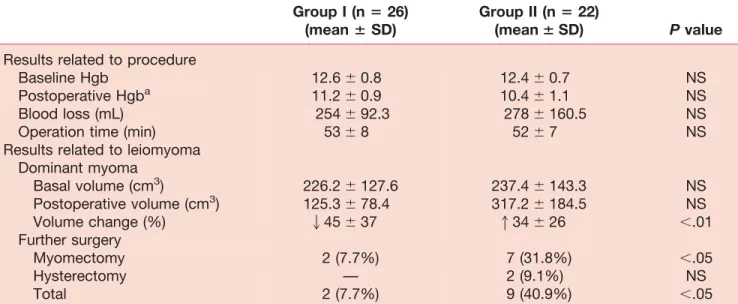
Preoperative baseline hemoglobin values measured on the first postoperative day showed no significant differences between the two groups (Table 2). In the group I patients, intraoperative blood loss was lower and the first postopera-tive hemoglobin level was higher, but without significant difference between the patients of both groups. The opera-tive time was a little longer for group I than for group II patients. However, this was also statistically insignificant. One patient in group II had an intraoperative blood loss of 1,650 mL and postpartum hemorrhage, she was given four units of packed red blood cells (RBCs) to restore blood volume.
The mean size of the first ultrasound examination of the dominant myoma was 8.2 cm by 7.8 cm by 6.8 cm
(calcu-lated volume: 226.2 cm3) for group I patients and 8.5 cm by 7.9 cm by 6.8 cm (calculated volume: 237.4 cm3) for the
group II patients. All patients received regular follow-up at our clinic for an average of 38.5 months (range: 12– 60 months). The mean volume of the dominant myomas was 6.7 cm by 6.2 cm by 5.8 cm (calculated volume: 125.3 cm3) in
the group I patients after treatment (Table 2). The average myoma volume reduction was 45%, with the most notable reduction being the disappearance of a 6-cm intramural myoma within 6 months. The mean volume of the dominant myoma was 9.2 cm by 8.5 cm by 7.8 cm (calculated volume: 317.2 cm3) in the group II patients postoperatively. The average myoma volume increase was 34%. During the follow-up time, two patients (7.7%) in group I underwent myomectomy, and nine patients (40.9%) in group II underwent myomectomy (n⫽ 7) or hysterectomy (n ⫽ 2), within 6–38 months for their symptomatic leiomyomas. Specimens of those removed leiomyomas showed marked degeneration in two patients (100%) in group I, and three patients (33.3%) in group II. Four patients (15.4%) in group I and three patients (13.6%) in group II had repeat cesarean sections after this study; of those three patients in group II, uterine artery ligation was performed simultaneously by patient request.
TABLE 1
Subject characteristics. Group I (n ⴝ 26) (mean ⴞ SD) Group II (nⴝ 22) (meanⴞ SD) General dataMaternal age (y) 33.1⫾ 4.8 32.7⫾ 3.7
Parity (n) 0.9⫾ 1.1 0.8⫾ 1.2
Previous abortions (n) 0.3⫾ 0.6 0.4⫾ 0.5
Gestational age (weeks) 37.5⫾ 3.1 37.7⫾ 2.4
Myoma characteristics Size (cm) 8.2⫾ 3.7 8.5⫾ 3.9 Location Fundus 11 (42.3%) 8 (36.4%) Corpus 9 (34.6%) 9 (40.9%) Low segment 6 (23.1%) 5 (22.7%) Classification Subserous 5 (19.2%) 3 (13.6%) Submucous 7 (26.9%) 7 (31.8%) Intramural 14 (53.9%) 12 (54.6%)
Indication for cesarean section
Previous cesarean section 8 (30.8%) 6 (27.2%)
Cephalopelvic disproportion 5 (19.2%) 4 (18.2%)
Malpresentation 5 (19.2%) 5 (22.7%)
Dysfunctional labor 4 (15.4%) 2 (9.1%)
Other obstetric complications 2 (7.7%) 2 (9.1%)
Low segment myomas 2 (7.7%) 3 (13.6%)
Note: P⫽not statistically significant.
DISCUSSION
The management of leiomyomas encountered during ce-sarean section poses a therapeutic dilemma for most ob-stetricians. Traditionally, most obstetricians do not sug-gest myomectomy during cesarean section unless the myoma is pedunculated (2). The main risk is intractable hemorrhage and possible postoperative morbidity. In this study, we demonstrated that uterine artery ligation per-formed during cesarean section may lead to a reduction of postpartum bleeding, a decreased necessity of future sur-gery, and a moderate reduction of the myoma volume postoperatively.
Bilateral ascending uterine artery ligation and tourni-quet have been used in cesarean myomectomy with sim-ilar efficacy in controlling intraoperative blood loss, but artery ligation is preferable to a tourniquet in preventing blood loss postoperatively (15). Because ligation is per-manent, it works from the intraoperative to the postoper-ative period. The tourniquet method is not effective with postoperative blood loss because it is removed at the end of the operation. In this study, no differences were shown between group I and group II patients in preoperative baseline hemoglobin levels; however, the average hemo-globin level of the first postoperative day was 11.2 g/dL in the group I patients and 10.4 g/dL in the group II patients. Although the uterine artery ligation performed after de-livery and the closure of the uterine wound could not effectively decrease blood loss during cesarean section, they exerted a hemostatic effect postoperatively. The use of bilateral uterine artery ligation in cases of postpartum
hemorrhage resulting from uterine atony was established long ago, without negative effects (16 –18). This explains why our group I study subjects had higher first postoper-ative day hemoglobin levels than the control group pa-tients, although intraoperative blood loss was comparable between the groups.
Since the introduction by Liu in 2000 of the uterine depletion procedure in treating uterine leiomyomas (6), various positive reports have addressed this issue (7–11). Symptomatic improvement was reported by Liu et al. (7) in 76 (89.4%) of 85 patients, including 18 (21.2%) with a complete resolution of symptoms. Significant reductions in the dominant myoma size (average 76%) were also demonstrated at a follow-up mean time of 10.2 months by using laparoscopic bipolar coagulation of the uterine ves-sels. The procedure involved double ligation of the bilat-eral uterine arteries with hemoclips, and coagulation of the anastomotic sites of the uterine arteries and the ovar-ian arteries with bipolar forceps. However, in this study, we performed double ligation on only the bilateral uterine arteries after cesarean delivery without ligating the anas-tomotic sites of the uterine arteries and ovarian arteries. This might explain why the average reduction percentage of the dominant myoma (45%) was lower than in previous reports (76%). In one study, the average reduction per-centage of the dominant myoma was reported to be 36% at the 6-month follow-up (10), after the patients were treated with a uterine depletion procedure similar to Liu’s laparoscopic bipolar coagulation of the uterine vessel procedure. In the present study, we followed up our
pa-TABLE 2
Outcome measurement. Group I (nⴝ 26) (mean ⴞ SD) Group II (nⴝ 22) (meanⴞ SD) P valueResults related to procedure
Baseline Hgb 12.6⫾ 0.8 12.4⫾ 0.7 NS
Postoperative Hgba 11.2⫾ 0.9 10.4⫾ 1.1 NS
Blood loss (mL) 254⫾ 92.3 278⫾ 160.5 NS
Operation time (min) 53⫾ 8 52⫾ 7 NS
Results related to leiomyoma Dominant myoma Basal volume (cm3) 226.2⫾ 127.6 237.4⫾ 143.3 NS Postoperative volume (cm3) 125.3⫾ 78.4 317.2⫾ 184.5 NS Volume change (%) 245⫾ 37 134⫾ 26 ⬍.01 Further surgery Myomectomy 2 (7.7%) 7 (31.8%) ⬍.05 Hysterectomy — 2 (9.1%) NS Total 2 (7.7%) 9 (40.9%) ⬍.05
Note: Hgb⫽ hemoglobin (g/dL). 2 ⫽ volume decrease; 1 ⫽ volume increase; NS ⫽ not statistically significant.
aHemoglobin was checked on the first postoperative day. Liu. Uterine artery ligation during cesarean section. Fertil Steril 2006.
tients for an average of 38.5 months. Most patients in group I experienced a symptom-free life and moderate shrinkage of the myoma volume (average: 45%), except for two women who had large uterine myomas (16 cm and 11 cm) without significant volume reduction after surgery. Myomectomy was performed for these two women at 6 months and 9 months, respectively, after cesarean section. Both myoma specimens showed marked degeneration re-sulting from either uterine artery ligation or pregnancy itself. In our past experience treating leiomyomas using the uterine depletion procedure we also encountered a small number of cases where tumor shrinkage was not observed as expected, although myomas were actually denourished by uterine artery occlusion, and growth had evidently stopped. In these few cases, the degenerated myomas were eventually removed at the request of the patients (unpublished data).
Nine (40.9%) of 22 patients in the control group received further surgery for symptomatic leiomyomas, 7 by myomec-tomy and 2 by hysterecmyomec-tomy. Degeneration of the myoma specimens was found only in three (33.3%) women. The possible reason for the high incidence of further surgery in this group is perhaps that the myomas grew progressively larger, and then induced related symptoms postoperatively. The average dominant myoma increase was 34% in these group II patients.
Four (15.4%) of 26 patients in the study group and 3 (13.6%) of 22 patients in the control group received a repeat cesarean section during the follow-up period. Fecundity had apparently not been compromised by uterine artery ligation during cesar-ean section. Old data revealed that pregnancy remained a pos-sibility and has been reported even after surgical occlusion of both the internal iliac and ovarian arteries (17). Twelve suc-cessful pregnancies were also reported after bilateral uterine artery ligaton for post-cesarean section hemorrhage (19, 20). In our previous report, 49 women who received uterine artery ligation and myomectomy for treating symptomatic leiomyo-mas had at least one live birth after treatment (11). No evidence for intrauterine growth retardation or other maternal or fetal problems was found in any of these patients. However, in another one of our previous reports, the laparoscopic bipolar coagulation of the uterine vessels procedure was recommended only for women who do not desire additional children, because a relatively high rate (7/17, 41.2%) of early miscarriages was observed (21).
Before reaching conclusions in this study, some study limitations should be clarified. As shown inTable 1, the general characteristics of the patients in both groups were similar, using the limited number of evaluated items. However, there may have been some differences, for example, in the educational level, socioeconomic level, degree of preoperative symptoms with fibroids, or some other etiology, such as willing for future pregnancy, be-tween these individuals. Unfortunately, we did not include these items for analysis. Although we did not perform the
analysis of these item, we believed that the patients enrolled into group I might have suffered from more symptoms, or the patients enrolled into group II might have a strongly unwilling for future pregnancy. The reason included the information about this procedure, which may influence the function of the ovary and uterus, and possibly subsequent fertility. Finally, this study had a short-term follow-up period (average: 38.5 months); therefore, the long-term effect of this procedure needs further investigation.
In conclusion, uterine artery ligation may be a promis-ing method for obstetricians in treatpromis-ing most pregnant women with leiomyomas during cesarean section. The procedure may prevent postpartum bleeding in patients, except for those with very large myomas, and it may effectively reduce postoperative blood loss. The proce-dure minimizes the need for future surgical treatment, either myomectomy or hysterectomy. Although volume reduction of the myomas is only mild to moderate, a long symptom-free period could be expected. Fertility may be not compromised by this treatment method.
REFERENCES
1. Katz VL, Dotters DJ, Droegemueller W. Complications of uterine leiomyomas in pregnancy. Obstet Gynecol 1989;73:593– 6.
2. Burton CA, Grimes DA, March CM. Surgical management of leiomy-omata during pregnancy. Obstet Gynecol 1989;74:707–9.
3. Brown D, Myrie M. Cesarean myomectomy—a safe procedure. West Ind Med J 1997;46 (Suppl 2):45.
4. Ehigiegba AE, Ande AB, Ojobb SI. Myomectomy during Cesarean section. Int J Gynecol Obstet 2001;75:21–5.
5. Kaymak O, Ustunyurt E, Okyay RE, Kalyoncu S, Mollamahmutoglu L. Myomectomy during Cesarean section. Int J Gynecol Obstet 2005;89: 90 –3.
6. Liu WM. Laparoscopic bipolar coagulation of uterine vessels to treat symptomatic leiomyomas. J Am Assoc Gynecol Laparosc 2000;7:125–9. 7. Liu WM, Ng HT, Wu YC, Yen YK, Yuan CC. Laparoscopic bipolar coagulation of uterine vessels: a new method for treating symptomatic fibroids. Fertil Steril 2001;75:417–22.
8. Liu WM, Yen YK, Wu YC, Yuan CC, Ng HT. Vaginal expulsion of submucous myomas after laparoscopic-assisted uterine depletion of the myomas. J Am Assoc Gynecol Laparosc 2001;8:267–71.
9. Lichtinger M, Hallson L, Calvo P, Adeboyejo G. Laparoscopic uterine artery occlusion for symptomatic leiomyomas. J Am Assoc Gynecol Laparosc 2002;9:191– 8.
10. Hald K, Langebrekke A, Klow NE, Noreng HJ, Berge AB, Istre O. Laparoscopic occlusion of uterine vessels for the treatment of symp-tomatic fibroids: Initial experience and comparison to uterine artery embolization. Am J Obstet Gynecol 2004;190:37– 43.
11. Liu WM, Tzeng CR, Chen YJ, Wang PH. Combining the uterine depletion procedure and myomectomy may be useful for treating symptomatic fibroids. Fertil Steril 2004;82:205–10.
12. Teng SW, Tseng YU, Chang CK, Li CT, Chen YJ, Wang PH. Com-parison of laparoscopy and laparotomy in managing hemodynamic-stable patients having ruptured corpus luteum with hemoperitoneum. J Am Assoc Gynecol Laparoscopists 2003;10:474 –7.
13. Goldstein SR, Horii SC, Snyder JR, Raghavendra BN, Subramanyam B. Estimation of nongravid uterine volume based on a nomogram of gravid uterine volume: its value in gynecological abnormalities. Obstet Gynecol 1988;72:86 –90.
14. Lee WL, Liu RS, Yuan CC, Chao HT, Wang PH. The relationship between gonadotropin releasing hormone agonist and myoma cellular activity. Fertil Steril 2001;75:638 –9.
15. Sapmaz E, Celik H, Altungul A. Bilateral ascending uterine artery ligation vs. tourniquet use for hemostasis in Cesarean myomectomy. J Reprod Med 2003;48:950 – 4.
16. Mullins JH Jr, O’Leary JA, Aksel S. Uterine artery ligation for post-abortal hemorrhage. Obstet Gynecol 1979;54:383– 4.
17. O’Leary JL, O’Leary JA. Uterine artery ligation in the control of intrac-table postpartum hemorrhage. Am J Obstet Gynecol 1996;94:920 – 4. 18. O’Leary JA. Uterine artery ligation in the control of post-Cesarean
hemorrhage. J Reprod Med 1995;40:189 –93.
19. Mengert WF, Burchell RC, Blumstein RW. Pregnancy after bilateral ligation of the internal iliac and ovarian arteries. Obstet Gynecol 1969; 34:664 – 6.
20. O’Leary JA. Pregnancy following uterine artery ligation. Obstet Gy-necol 1980;55:112–3.
21. Chen YJ, Wang PH, Yuan CC, Yen YY, Yang MJ, Ng HT, et al. Pregnancy following treatment of symptomatic myomas with lapa-roscopic bipolar coagulation of uterine vessels. Hum Reprod 2003; 18:1077– 81.