Characterization of the Muscle Electrical Properties in Low Back Pain
Patients by Electrical Impedance Myography
Congo Tak-Shing Chinga,b,c,*, Yueh-Chi Chend, Li-Hua Lud,
Chin-Sung Hsiaoc, Tai-Ping Suna,b,*, Hsiu-Li Shieha, Kang-Ming Changc,e,*
a Department of Electrical Engineering,
National Chi Nan University, Nantou, Taiwan, ROC
b Department of Applied Materials and Optoelectronic Engineering
National Chi Nan University, Nantou, Taiwan, ROC
c Department of Photonics and Communication Engineering,
Asia University, Taichung County, Taiwan, ROC
d Physical Therapy Room,,
Chung Shan Medical University Hospital, Taichung, Taiwan, ROC
e Graduate Institute of Clinical Medical Science
China Medical University, Taichung, Taiwan, ROC
*Corresponding Authors
Name: Tai-Ping Sun and Congo Tak-Shing Ching
Address: Department of Electrical Engineering, National Chi Nan University, No. 1, University Rd., Puli, Nantou County 54561, Taiwan, ROC
e-mail: tps@ncnu.edu.tw and tsching@ncnu.edu.tw *Corresponding Authors
Name: Kang-Ming Chang
Address: Department of Photonics and Communication Engineering, Asia University, No. 500, Lioufeng Rd., Wufeng, Taichung 41354, Taiwan, ROC
Abstract
Objectives. The aim of this study is to investigate the electrical properties of
lumbar paraspinal muscles (LPM) of patients with acute lower back pain (LBP) and to study a new approach, namely Electrical Impedance Myography (EIM), for reliable, low-cost, non-invasive, and real-time assessment of muscle-strained acute LBP.
Design. Patients with muscle-strained acute LBP (n = 30) are compared to a
healthy reference group (n = 30). Electrical properties of LPM are studied.
Background. EIM is a novel technique under development for the assessment of
neuromuscular disease. Therefore, it is speculated that EIM can be employed for the assessment of muscle-strained acute LBP.
Methods. Disposable surface electromyographic electrodes, in bipolar electrode
configurations, was used to measure the electrical properties of patient’s and healthy subject’s LPM at six different frequencies (0.02, 25.02, 50.02, 1000.02, 3000.02 and 5000.02 kHz), with the amplitude of the applied voltage limited to 200mV. Four studying parameters of impedance (Z), extracellular resistance (Re), intracellular resistance (Ri), and the ratio of extracellular resistance to intracellular resistance (Re/Ri) of LBP patient’s and healthy subject’s LPM were assessed to see if significant difference in values obtained in muscle-strained acute LBP patients existed.
(ICC>0.96 for all studying parameters: Z, Re, Ri and Re/Ri) had good reliability and validity. Significant differences were found on Z between LBP patient’s and healthy subject’s LPM at all studying frequencies, with p<0.05 for all frequencies. It was also found that Re (p<0.05) and Re/Ri (p<0.05) of LBP patient’s LPM was significant smaller than that of healthy subjects while Ri (p<0.05) of LBP patient’s LPM was significant greater than that of healthy subjects. Moreover, no statistical significant difference was found between the left and right LPM of LBP patients and healthy subjects on the four studying parameters.
Conclusion. EIM is a promising technique for assessing muscle-strained acute
LBP.
Keywords: Electrical Impedance Myography; Lower Back Pain; Noninvasive; Acute;
1. Introduction
Lower back pain (LBP) is common in the general population, affecting 60–80% of all adults at some point in their life [1,2]. In the United States and United Kingdom between 70% and 80% of the adult population have suffered from LBP at some time and have contacted a general practitioner [3-5]. LBP is one of the most common symptoms reported by Taiwan people [6,7]. The life and 12-month incidence rate of LBP among Taiwan people was 37.0% and 18.9%, respectively [6]. LBP is a common reason for patients to seek medical care. In Taiwan alone more than 2.14 million patients sought medical care for back pain in 1998 and that medical cost alone exceeded 3 billion New Taiwan Dollars [8]. The possible consequences of unmanaged LBP are well documented, e.g. depression [9,10] and functional disability [11]. LBP is costly in terms of treatment, individual suffering and work absenteeism [12].
Several diagnostic methods are available to diagnose the cause of LBP so as to give an appropriate treatment: x-ray imaging, discography, computerized tomography, magnetic resonance imaging, electrodiagnostic procedures (electromyography, nerve conduction studies, and evoked potential studies), bone scans, and ultrasound imaging. However, most LBP mainly arises from the problem of low back muscles [13-17] and therefore some of these diagnostic methods are ineffective on diagnosing muscle-strained acute LBP. For example, x-ray imaging and computerized tomography are
good for bone diagnosis but not ideal for the diagnosis of muscle problem. On the other hands, some of these diagnostic methods are either invasive or costly. For instance, discography and bone scans are invasive methods, as they involve the injection of a special contrast dye and a radioactive material respectively for diagnosis, and they are also not the methods for the diagnosis of muscle problem. Although magnetic resonance imaging is the best way to obtain a definitive diagnosis of muscle-strained acute LBP, it is costly. The drawbacks of electrodiagnostic procedures and ultrasound imaging are that they cannot give information about electrochemical processes and physiological changes in the muscle.
Electrical Impedance Myography (EIM) is a bioimpedance-based technique. It is the measurement of the bioimpedance signal, which is obtained by injecting low-level sinusoidal current in the tissue and measuring the voltage drop generated by the tissue impedance. Bioimpedance signal gives information about electrochemical processes in the tissue and can hence be used for characterizing the tissue or for monitoring physiological changes. EIM is well established. It has been used for investigating the physiological properties of muscles [18-24] and has been effective in the assessment of neuromuscular diseases [22-24]. The basic concept underlying the use of EIM as a clinical tool is that pathological muscle changes such as muscle fiber atrophy and loss, tissue edema, and fatty replacement alter impedance signatures in consistent ways. For
example, Aaron et al. in 2006 [21] used EIM for the assessment of quadriceps and tibialis anterior muscles to the effects of normal aging and they found that there are muscle reductions, in terms of the spatially averaged phase angle, with increasing age. Other works have been demonstrated that the phase angle decreases in generalized neuromuscular diseases including myopathy and motor neuron disease, as well as in more focal disorders, such as radiculopathy [22-24]. At present, no studies using EIM for the investigation of muscle-strained acute LBP are reported in the literature. Muscle changes which occur in muscle-strained acute LBP are expected to affect EIM outcome parameters much as they do in disease, including changes in the membrane properties and the composition of the intra-cellular and extra-cellular matrices. Earlier EIM studies have shown that its principal outcome variable, the spatially averaged phase angle, rapidly drops with increasing severity in generalized disorders such as inflammatory myositis and amyotropic lateral sclerosis [22,24,25]. Therefore, the aim of this study is to study the electrical properties of lumbar paraspinal muscles (LPM) of patients with LBP and to investigate the EIM approach for reliable, low-cost, non-invasive, and real-time assessment of muscle-strained acute LBP.
2. Materials and Methods
Thirty patients (14 men and 16 women; age: 45 7 year; weight: 61 ± 9 kg) diagnosed with muscle-strained acute LBP by rehabilitation medical doctor and another
thirty healthy subjects (15 men and 15 women; age: 48 10 year; weight: 67 ± 13 kg) without LBP in the past 6 months were recruited in this study. The study was approved by the Asia University Medical Research Ethics Committee. Each participant provided his/her written informed consent to participate in this study.
Four electrical properties of LPM were investigated: impedance (Z), extracellular resistance (Re), intracellular resistance (Ri), and the ratio of extracellular resistance to intracellular resistance (Re/Ri).
EIM measurements of the LPM were made with LBP patients and healthy subjects lying on a bed in the prone position. Disposable surface electromyographic electrodes (3M red. dotTM 2258T AglAgCl) were used and positioned at a bipolar electrode configuration (Figure 1). In brief, two electrodes were positioned along the left LPM region of the LBP patients and healthy subjects, with the center of the distal electrode 5 cm below the fifth lumbar vertebra and the center of the two electrodes was 5 cm apart. Another two electrodes were positioned in the same manner at the right LPM region of the LBP patients and healthy subjects. Prior to the electrodes attachment, the areas of skin where the electrodes to be located were prepared by briskly rubbing the areas for 8 seconds with alcohol prep pads to remove dry skin, oils and other contaminants. The areas were then allowed to dry thoroughly.
2.1 Measurement procedures
Electrodes at each side (left and right side) were separately connected to an impedance analyzer (Precision Impedance Analyzer WK6420C, Wayne Kerr Electronics Ltd, United Kingdom) for each LBP patient and healthy subject measurement. At each side, EIM measurements were made at six frequencies (0.02, 25.02, 50.02, 1000.02, 3000.02 and 5000.02 kHz), with the amplitude of the applied voltage limited to 200 mV. In all cases, three separate sets of measurement of each side were made in succession in order to check reliability of the EIM measurements.
Before and after each LBP patient and healthy subject measurement, their lower back skin-surface temperatures (LBSSTemp) were measured using infrared thermometer (TemporalScannerTM 2000C, Exergen Corporation, USA).
2.2 Data Processing
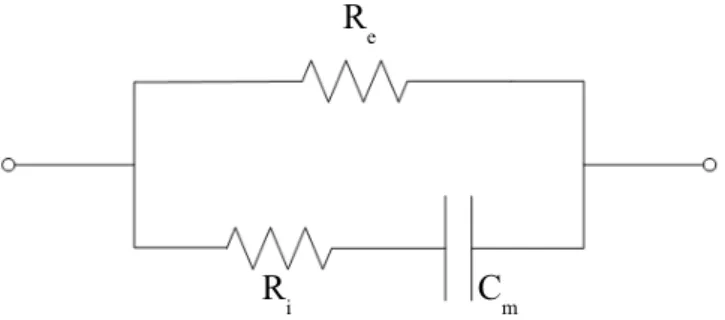
Yamamoto and Yamamoto suggested that a tissue can be electrically represented in impedance terms as a combination of a resistor placed in parallel with another resistor and a capacitor in series [26], an equivalent circuit of the impedance of the LPM can be established as shown in Figure 2, with impedance Z:
i m e R fC R Z 2 1 1 1 1 [1]
where Re and Ri are the resistance of the extracellular and intracellular medium of the LPM respectively, Cm is the capacitance of the cell membrane, and f is the frequency.
When the frequency approaches zero, Equation 1 can be rewritten:
e
f R
Z 0 [2]
where Zf→0 is the impedance of the LPM as frequency closed to zero (0.02 kHz in this study).
When the frequency approaches infinity, Equation 1 can be rewritten:
i e i e f R R R R Z [3]
study).
Electrical properties Re, Ri, and Re/Ri of the LPM can thus be determined from Equations 2 and 3.
2.3 Statistical analysis
Intraclass correlation coefficient (ICC) was used to evaluate intrarater reliability (ICC 3,1) for the measurement of Z, Re, Ri, and Re/Ri. Paired-sample t test (within group) and independent-samples t test (between groups) were used to determine whether there were significant differences between LBP patient’s and healthy subject’s LPM for the studying parameters of Z, Re, Ri, and Re/Ri at each frequency and their LBSSTemp. All statistical analyses were carried out using SPSS software with the level of statistical significance set at 0.05.
3. Results
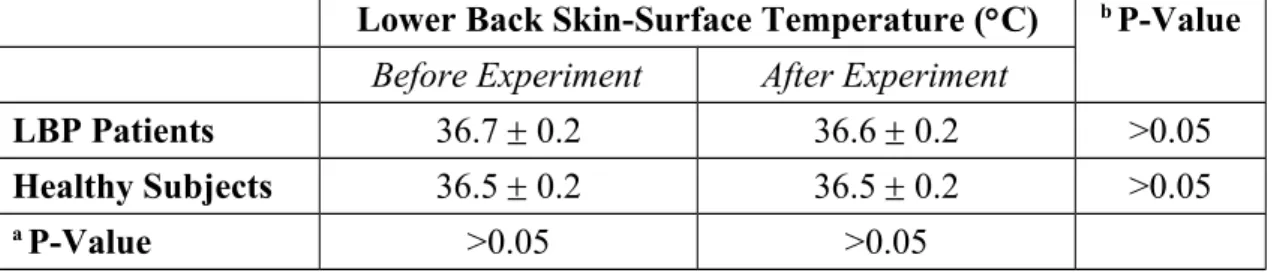
Thirty patients with muscle-strained acute LBP and thirty healthy subjects with no LBP in the past 6 months participated in this study. Their LBSSTemp before and after experiment were recorded and summarized in Table 1. No statistical significant difference was found on LBP patients’ pre- and post-experimental LBSSTemp as well as on healthy subjects’ pre- and post-experimental LBSSTemp. Also, no statistical
significant difference was found between the pre-experimental LBSSTemp of LBP patients and that of healthy subjects as well as between the post-experimental LBSSTemp of LBP patients and that of healthy subjects.
ICC for the intrarater reliability (ICC 3,1) for the measurement of electrical parameters (Z, Re, Ri, and Re/Ri) of LPM were summarized in Table 2. All electrical parameter measurements for the LPM of LBP patients and healthy subjects had ICC value ranging from 0.96 to 0.99.
The electrical properties (Z, Re, Ri, and Re/Ri) of LPM were summarized in Figures 3, 4, 5 and 6. No statistical significant difference was found between the left side and right side LPM of LBP patients and healthy subjects on the four studying parameters (Z, Re, Ri, and Re/Ri).
As shown in Figure 3, it was observed that Z of LBP patient’s and healthy subject’s LPM decreased as the measurement frequency increasing. Moreover, Z of LBP patient’s LPM was found to be significantly (p<0.05, about 0.9-fold) smaller than that of healthy subject’s LPM at 0.02 kHz. However, Z of LBP patient’s LPM was found to be significantly (p<0.05, about 1.1-fold) higher than that of healthy subject’s LPM at 25.02, 50.02, 1000.02, 3000.02 and 5000.02 kHz.
It was found that Re of LPM of LBP patient was significantly smaller (p<0.05, about 0.4-fold) than that of healthy subjects (Figure 4). The Re/Ri ratio of LPM of LBP
patient was also found to be significantly smaller (p<0.05, about 0.3-fold) than that of healthy subjects (Figure 6). However, Ri of LPM of LBP patient was found to be significantly greater (p<0.05, about 1.3-fold) than that of healthy subjects (Figure 5).
4. Discussion
The LPM plays an important role as stabilizers and therefore has been a focus of active research. For example, in patients with LBP, medical imaging studies of the paraspinal muscles consistently show a decrease in cross-sectional areas [27,28]. Therefore, this study focuses on the LPM in order to study the electrical properties difference between LBP patients and healthy subjects.
In this study, before and after each participator (LBP patient and healthy subject) measurement, his/her LBSSTemp was measured. This is because that impedance of tissue varies with temperature [29]. Some participators were found to have 0.1C change in their LBSSTemp whereas the rest of the participators had no change in their LBSSTemp. Participators’ actual skin-surface temperature change might be the source of such temperature changes. Another possible reason for such temperature changes might be due to the instrumentation error during measurement as the infrared thermometer has the accuracy of 0.2C. Participators’ skin-surface temperature ranged from 36.5C to 36.7C. The effect of temperature on participators’ impedance was
assumed to be negligible in this study for the reason that the skin-surface temperature difference among participators was very small.
The ICC is a measure that can be used to quantify the reproducibility of a variable. It is also a measure of the homogeneity within groups of replicate measurements relative to the total variation between groups. It is suggested that ICC values above 0.75 are indicative of good reliability [30]. Moreover, for many clinical measurements, reliability should exceed 0.90 to ensure reasonable validity [30]. In this study all the ICC(3,1) measurements exceeded 0.90. This suggests they have exceeded the threshold for both good reliability and reasonable validity.
LBP is often caused by muscle inflammation and strain. It can be marked by localized swelling in the immediate area. Our findings showed that the four studying parameters (Z, Re, Ri, and Re/Ri) have the ability to distinguish the LPM of LBP patients and healthy subjects. Results showed that Z of LBP patient’s LPM was significantly smaller (p<0.05) than that of healthy subject’s LPM at 0.02 kHz. Also, Re of LBP patient’s LPM was significantly smaller (p<0.05) than that of healthy subjects. The relatively lower Z and Re in LBP patient’s LPM might be due to the muscle inflammation which commonly results in local swelling (i.e. more blood and interstitial fluid at that region for the facilitation of muscle repair). A possible explanation for the changes observed is as follows. As shown in Equation 2, current at low frequency (<1
kHz) primarily flows around the muscle cell without being able to directly go through the muscle cell (Figure 7). For healthy subjects, their muscle cells are well packed and closed to each other. Hence, low frequency (0.02 kHz in this study) current has very restricted intercellular pathways to run and this result in a high resistance. But, for acute LBP patients, their muscles normally have a phenomenon of inflammation and strain, which have adverse effects on resistance. Inflamed/strained muscles have enlarged extracellular gaps because of the local swelling and this would be expected to decrease resistance. Therefore, acute LBP patients normally have a relatively lower Z and Re in their LPM. On the other hand, current at high frequency (>1 kHz) flows around and penetrates the muscle cell at the same time (Figure 7). For acute LBP patients, their inflamed/strained muscles are under repair and hence many repairing proteins are synthesized inside the muscle cells. This results in a dramatically increase of intracellular resistance and this phenomenon has been further proved in Figure 5. Owing to the increase of intracellular resistance of inflamed/strained muscles and based on Equation 3, inflamed/strained muscles will have a higher Z as compared to healthy muscles if the Z is measured at high frequency (>1 kHz). Therefore, as shown in Figure 3, Z of LBP patient’s LPM was found to be significantly (p<0.05) higher than that of healthy subject’s LPM at 25.02, 50.02, 1000.02, 3000.02 and 5000.02 kHz. Also, Ri of
subjects (Figure 5).
Self-normalization idea has been utilized in the studying parameter of Re/Ri. The use of self-normalization aims to keep away from the large subject-to-subject differences in LPM during data analysis. Therefore, this allows the electrical properties of LPM to be studied without the nonuniformities introduced by patient-to-patient variation. Hence, Re/Ri is more independent and trustable on distinguishing the LPM of LBP patients and healthy subjects. As shown in Figure 6, it was observed that Re/Ri of LBP patient’s LPM was significantly smaller (p<0.05) than that of healthy subjects.
EIM have several advantages such as low-cost, providing instant result, and little training requirement. Besides, provision of instant assessment results can be able to repeat inadequate assessment immediately. Therefore EIM can be easily used in primary care.
5. Conclusion
Significant separation of LPM of LBP patients and healthy subjects could be attained using the measurement parameter of Z, Re, Ri and Re/Ri. The ratio Re/Ri is an independent and trustable measurement parameter for distinguishing the LPM of LBP patients and healthy subjects. All measurements had good reliability with ICC>0.95. This method can be used as a potential screening test with the advantage of providing an
immediate result. Also, this method may be used by those with minimal training in the setting of primary care or in the developing countries.
Acknowledgement
The authors wish to thank the participators who participated in this study. This work was supported in part by grants (NSC 101-2221-E-260-001- and NSC 98-2221-E-260-024-MY3) from National Science Council, Taiwan, Republic of China. And, no additional external funding received for this study.
Conflict of Interest Statement None declared.
Reference
1. Heliovaara M, Makela M, Knekt P, Impivaara O, Aromaa A (1991) Determination of sciatica and low back pain. Spine 16: 608-614.
2. Nurminen M (1997) Reanalysis of the occurrence of back pain among construction workers: modelling for the interdependent effects of heavy physical work, earlier back accidents, and aging. Occup Environ Med 54: 807-811.
3. Patel AT, Ogle AA (2007) Diagnosis and Management of Acute Low Back Pain. American Academy of Family Physicians. Retrieved March 12, 2007.
4. Frymoyer JW, Cats-Baril WL (1991) An overview of the incidences and costs of low back pain. Orthop Clin N Am 22: 263-271.
5. Walsh K, Cruddas M, Coggon D (1992) Low back pain in eight areas of Britain. J Epidemiol Commun H 46: 227-230.
6. Guo HR, Chang YC, Yen WY, Chen CW, Guo YL (2004) Prevalence of musculoskeletal disorder among workers in Taiwa: A national stdy. J Occup Health 46: 26-36.
7. Lee JH, Hoshino Y, Kariya Y, Chen CL, et al. (1998) Epidemiological comparison of low back pain in three Asian countries. Journal of Orthopaedic Surgery.
http://findarticles.com/p/articles/mi_qa3794/is_199812/ai_n8814144/print
8. Wei HH (2000) Health Insurance compensation exceeded 3 billion dollars in 1998 for upper and lower back pain. United Daily News, May 3.
9. Cohen-Mansfield J, Marx MS (1993) Pain and depression in the nursing home: collaborating results. J Gerontol Psychol Sci 48: 96–97.
10. Parmelee PA, Katz IR, Powell Lawton M (1991) The relation of pain to depression among institutionalized aged. J Gerontol 46: 15-21.
11. Ferrell BA, Ferell BR, Osterweil D (1990) Pain in the nursing home. J Am Geriatr Soc 38: 409-414.
12. Chiu TTW, Lam TH, Hedley AJ (2001) Subjective health measure used on Chinese patients with neck pain in Hong Kong. Spine 26: 1884-1889.
13. Sihvonen T, Partanen J, Hanninen O, Soimakallio S (1991) Electric behavior of low back muscles during lumbar pelvic rythm in low back pain patients and healthy control. Arch Phys Med Rehabil 72: 1080-1087.
14. Konno S, Kikuchi S, Nagaosa Y (1994) The relationship between intramuscular pressure of the paraspinal muscles and low back pain. Spine 19: 2186-2189. 15. Waddell G (1998) The back pain revolution, Churchill Livingstone, Edinburgh. 16. Van Dieen JH, Selen LP, Cholewicki J (2003) Trunk muscle activation in
low-back pain patients, an analysis of the literature. J Electromyogr Kines 13: 333-351. 17. Radebold A, Cholewicki J, Polzhofer GK, Greene HS (2001) Impaired postural
control of the lumbar spine is associated with delayed muscle response times in patients with chronic idiopathic low back pain. Spine 26: 724-730.]
18. Elleby B, Knudsen LF, Brown BH, Crofts CE, Woods MJ, Trowbridge EA (1990) Electrical impedance assessment of muscle changes following exercise. Clin Phys Physiol Meas 11: 159-166.
19. Aaron R, Huangy M, Shiffman CA (1997) Anisotropy of human muscle via non-invasive impedance measurements. Phys Med Biol 42: 1245-1262.
20. Shiffman CA, Aaron R, Rutkove SB (2003) Electrical impedance of muscle during isometric contraction. Physiol Meas 24: 213-234.
21. Aaron R, Esper GJ, Shiffman CA, Bradonjic K, Lee KS, Rutkove SB (2006) Effects of age on muscle as measured by electrical impedance myography. Physiol
Meas 27: 953-959.
22. Rutkove SB, Aaron R, Shiffman CA (2002) Localized bioimpedance analysis in the evaluation of neuromuscular disease. Muscle Nerve 25: 390-397.
23. Rutkove SB, Esper GJ, Lee KS, Aaron R, Shiffman CA (2005) Electrical impedance myography in the detection of radiculopathy. Muscle Nerve 32: 335-341.
24. Tarulli A, Esper GJ, Lee KS, Aaron R, Shiffman CA, Rutkove SB (2005) Electrical impedance myography in the bedside assessment of inflammatory myopathy. Neurology 65: 451-452.
25. Aaron R, Shiffman CA (2000) Using localized impedance measurements to study muscle changes in injury and disease. Ann NY Acad Sci 904: 171-180.
26. Yamamoto T, Yamamoto Y (1976) Electrical properties of the epidermal stratum corneum. Med Biol Eng Comput 14: 151-158.
27. Danneels LA, Vanderstraeten GG, Cambier DC, Witvrouw EE, De Cuyper HJ (2000) CT imaging of trunk muscles in chronic low back pain patients and healthy control subjects. Eur Spine J 9: 266-272.
28. Gibbons LE, Videman T, Battie MC (1997) Isokinetic and psychophysical lifting strength, static back muscle endurance, and magnetic resonance imaging of the paraspinal muscles as predictors of low back pain in men. Scand J Rehabil Med 29: 187-191.
29. Rabbat A (1990) Tissue resistivity. In Electrical impedance tomography. Edited by Webster JG. Bristol and New York: IOP Publishing: 8-20.
30. Portney L (2000) Watkins M: Foundations of Clinical Research: applications to practice. 2nd edition. New Jersey: Prentice Hall Health.
Figure Legends
Figure 1 : Position of electrodes. All electrodes are positioned along the LPM. The center of both distal electrodes is 5 cm below the fifth lumbar vertebra and the center of the two electrodes on each side was 5 cm apart.
Figure 2: An equivalent circuit of LPM. Re and Ri are the resistance of the extracellular and intracellular medium of the LPM. Cm is the capacitance of the cell membrane
Figure 3: Impedance (Z) of LPM measured at different frequencies (n=30). Results were expressed as means and standard deviations. Z of LBP patient’s LPM was found to be significantly smaller (p<0.05) than that of healthy subject’s LPM at 0.02 kHz. However, Z of LBP patient’s LPM was found to be significantly higher (p<0.05) than that of healthy subject’s LPM at the remaining frequencies (25.02, 50.02, 1000.02, 3000.02 and 5000.02 kHz). No statistical significant difference was found between the left and right LPM of LBP patients and healthy subjects on Z.
Figure 4: Extracellular resistance (Re) of LPM (n=30). Results were expressed as means and standard deviations. Re of LBP patient’s LPM was found to be significant smaller (p<0.05) than that of healthy subjects. However, no statistical significant difference was found between the left and right LPM of LBP patients and healthy subjects on Re.
Figure 5: Intracellular resistance (Ri) of LPM (n=30). Results were expressed as means and standard deviations. Ri of LBP patient’s LPM was found to be significant higher (p<0.05) than that of healthy subjects. However, no statistical significant difference was found between the left and right LPM of LBP patients and healthy subjects on Ri.
Figure 6: The ratio of extracellular resistance to intracellular resistance (Re/Ri) of LPM (n=30). Results were expressed as means and standard deviations. Re/Ri of LBP patient’s LPM was found to be significant smaller (p<0.05) than that of healthy subjects. However, no statistical significant difference was found between the left and right LPM of LBP patients and healthy subjects on Re/Ri.
Figure 7: Schematic diagram shows the route of low and high frequency currents running through a healthy and an inflamed/strained muscle. According to Equation 2, the impedance of a muscle as frequency closed to zero is equal to its extracellular resistance (Re). This means that low frequency current primarily runs through the extracellular medium but not the intracellular medium. For inflamed/strained muscle, it has enlarged extracellular gaps because of the local swelling. Therefore, low frequency current has a wider extracellular gap to flow and this result in the reduction in the Re.
Table 1: The lower back skin-surface temperature of LBP patients and healthy subjects before and after experiment.
Lower Back Skin-Surface Temperature (C) b P-Value
Before Experiment After Experiment
LBP Patients 36.7 0.2 36.6 0.2 >0.05
Healthy Subjects 36.5 0.2 36.5 0.2 >0.05
a P-Value >0.05 >0.05
a Independent-samples t test. b Paired-sample t test.
Table 2: Estimation of intrarater reliability (ICC 3,1) for the measurement of impedance (Z) extracellular resistance (Re), intracellular resistance (Ri), and the ratio of extracellular resistance to intracellular resistance (Re/Ri) of LPM.
ICC 3,1
Z Re Ri Re/Ri
LBP Patients 0.99 0.96 0.99 0.98
Figure 1
Figure 2 Re