systemic lupus erythematosus in Taiwan
Y.-J. Lin
1,2,3, L. Wan
1,2,3, C.-M. Huang
4, J. J.-C. Sheu
1,2, S.-Y. Chen
1,2, T.-H. Lin
1,
D.-Y. Chen
1, K.-C. Hsueh
5, C.-C. Lai
6, F.-J. Tsai
1,2,3,5*1
Department of Medical Research,
2Graduate Institute of Chinese Medical Science,
4Division of
Immunology and Rheumatology, and
5Department of Pediatrics, China Medical University, Taichung,
Taiwan;
3Department of Biotechnology and Bioinformatics, Asia University, Taichung, Taiwan;
6The Institute of Molecular Biology, National Chung Hsing University, Taichung, Taiwan.
Abstract
The genetic control of Interleukin-10 (IL-10) and Tumour necrosis factor-α (TNF-α) production and the possible
interaction between the two cytokines in influencing SLE susceptibility as well as clinical features has not been completely
evaluated in the Taiwanese population. We investigated the association of IL-10 and TNF-α promoter polymorphisms
(-1082, -819 and -592 for IL-10 gene; -308 for TNF-α gene) with SLE in a total of 172 Taiwanese patients and 215
controls. Our results indicate that IL-10 A/T/A-A/T/A genotype was associated with Taiwanese SLE, whereas no
significance was observed between TNF-α genotype and SLE. Furthermore, the TNF-α G allele frequency of the
polymorphism at -308 was significantly decreased in patients with oral ulcers. The combined frequencies of IL-10 A/T/A
haplotype and TNF-α G-G genotype were significantly increased in SLE patients. In addition, the combined frequencies
of IL-10 A/T/A haplotype and TNF-α G-G genotype were significantly decreased in patients with oral ulcers. These results
suggest a significant correlation of the combined IL-10 and TNF-α genetic polymorphisms contribute to SLE susceptibility
and clinical features in the Taiwanese population.
Key words
Y-J Lin, L Wan, C-M Huang, J J-C Sheu, S-Y Chen, T-H Lin, D-Y Chen, K-C Hsueh, C-C Lai, Fuu-Jen Tsai
This work was supported by China Medical University (CMU97-CMC-005), China Medical University Hospital (DMR-97-102) and the National Science Council in Taiwan (NSC97-2320-B-039-023-MY3).
Please address correspondence and reprints requests to:
Fuu-Jen Tsai,
Department of Medical Research, China Medical University Hospital, No. 2 Yuh Der Road,
Taichung, Taiwan.
E-mail: [email protected] Received on August 3, 2009; accepted in revised form on December 4, 2009. © Copyright CLINICALAND
EXPERIMENTAL RHEUMATOLOGY 2010.
Competing interests: none declared.
Introduction
Systemic lupus erythematosus (SLE),
is a systemic autoimmune disorder,
characterised by distinct clinical
mani-festations (1-4). Although the exact
eti-ology and pathogenesis of SLE are
un-known, it is believed that the disease is
genetic in origin (2). Cytokines are
po-tent immunomodulatory molecules that
mediate immune response and
inflam-mation. Investigators have explored
the role of several cytokines involved
in pathogenesis of SLE (5-7).
Interleukin-10 (IL-10), produced by
monocytes and lymphocytes, is a
po-tent cytokine that has pleiotropic
ef-fects in immunoregulation and
inflam-mation (8, 9). It has been reported that
the serum levels of IL-10 are elevated
in the case of SLE patients (5, 10).
IL-10 production appears to be influenced
by the polymorphisms in the IL-10
promoter region (11, 12). In addition,
the three IL-10 promoter SNPs are
strongly associated with the
pathogen-esis of SLE (13-18). Tumour necrosis
factor-α (TNF-α), an important
proin-flammatory cytokine, exerts a variety
of physiologic and pathogenic effects,
including the activation of a cascade of
inflammatory events, which lead to
tis-sue destruction in autoimmune
diseas-es (19-21). Levels of TNF-α have been
reported in SLE patients and have been
shown to correlate with SLE disease
activity (22-24). Nevertheless, studies
on TNF-α genetic polymorphisms in
SLE patients have yielded
inconclu-sive results (25-31). The production of
these two regulators of the
inflammato-ry reactions-IL-10 and TNF-α has been
found to be deeply deregulated in SLE,
suggesting that these regulators may be
involved in the pathogenesis of SLE.
The genetic control of IL-10 and TNF-α
production and the possible interaction
between the two cytokines in
influenc-ing SLE susceptibility as well as
clini-cal features has not been completely
evaluated in the Taiwanese population.
Our aim in the present study was to
in-vestigate the influence of cytokine
ge-netic variants and their interactions in
Taiwanese SLE population.
Patients and methods
Study population
The study subjects including a total of
172 patients with SLE and 215 healthy
subjects were recruited from China
Medical University Hospital in Taiwan.
However, the total numbers for SLE
patients or controls illustrated in Table
I do not agree with each other for the
IL-10 and TNF-α may due to the poor
quality of the genomic DNA of SLE
patients or controls. The poor quality
of the genomic DNA may lead to PCR
failure. Therefore, the total numbers
for SLE patients or controls in Table I
mean the success in PCR reaction
num-bers. Furthermore, due to insufficient
information of SLE clinical features,
some patients may only have
genotyp-ing results without clinical features; the
numbers of SLE patients with various
clinical features regarding genetic
hap-lotypes may be inconsistent. All of the
patients met American Rheumatism
As-sociation criteria for SLE classification
(32). The healthy individuals from the
general population were also enrolled.
Informed consent was obtained from
each patient and control subjects
in-volved. DNA collection was approved
by China Medical University
Hospi-tal’s Ethics Board.
IL-10 and TNF-α promoter
polymorphisms genotyping
Genomic DNA was extracted from
pe-ripheral blood leukocytes according to
standard protocols (Roche Genomic
DNA kit). The 3 biallelic IL-10
pro-moter polymorphisms were detected by
TaqMan(R) Genotyping Assays
(Ap-plied Biosystems) (Supplemental Table
I). The TNF-α genetic polymorphism
(-308) were detected by PCR using
primers that amplified a short fragment
of DNA containing the polymorphism
(Supplemental Table II). Polymorphic
site identification was performed by
incubating the PCR products with a
re-striction enzyme chosen to cut 1 of the
2 alleles, followed by electrophoresis
on 3% agarose gels. All samples were
amplified and digested in parallel with
3 samples of a known genotype.
Statistical analysis
Polymorphism genotype frequencies
and allelic frequency distributions in
SLE patients and control individuals
were analysed with chi-square tests
(SPSS Version 10.0). Statistical
signifi-cance was assumed at p<0.05. Allelic
frequencies were expressed as
percent-ages of total allele numbers. Odds ratios
(OR) were calculated from genotype
frequencies and allelic frequencies at
a 95% confidence interval (CI).
Hap-lotypes were inferred from unphased
genotype data with Bayesian statistics
(Phase 2.1 software) (33, 34).
Adher-ence to the Hardy-Weinberg
equilib-rium constant was examined using a χ
2test with one degree of freedom. The
corrected P (Pc) values were adjusted
by using Bonferroni’s correction for
multiple comparisons. Statistical
sig-nificance was considered as Pc-value
<0.0045 (0.05/11 clinical features).
Results
IL-10 and TNF-α promoter
polymorphisms
The promoter genotype frequencies of
IL-10 and TNF-α promoter
polymor-phisms are shown in Table I. Nine
IL-10 promoter haplotypes were present
in both SLE patients and controls. No
statistically significant differences were
observed in IL-10 promoter haplotypes
between these two groups with two
ex-ceptions: A/T/A-A/T/A and A/T/C-A/C/
C. In SLE patients, A/T/A-A/T/A
geno-type frequency was significantly higher
(p<0.001; OR=2.22, 95%
CI=1.47-3.34) and A/T/C-A/C/C frequency was
significantly lower (p=0.004; OR=0.15,
95% CI=0.03-0.65). Observed
frequen-cies for individuals carrying the A/T/
A haplotype were 97.1% in SLE
pa-tients and 79.1% in controls (p<0.001;
OR=8.83, 95% CI=3.42-22.76). No
sig-nificant difference in the allele and
gen-otype frequencies of the -308 position
of TNF-α promoter gene was observed
between SLE patients and controls.
IL-10, TNF-α promoter polymorphisms
and clinical features of SLE
The association between the clinical
feature profile of SLE patients with
Table I. Distribution of IL-10 and TNF-α promoter genotype in Taiwanese SLE patientsand controls.
Promoter genotypes SLE Controls p-value Odds ratio (95% CI) IL-10 (-1082/-819/-592) Number (%) Number (%)
A/C/C-A/C/C 1 (0.6) 7 (3.3) 0.066 0.17 (0.02–1.43) A/C/C-G/C/C 0 (0.0) 3 (1.4) 0.120 ND A/T/A-A/C/C 56 (32.6) 84 (39.1) 0.185 0.75 (0.49–1.15) A/T/A-A/T/A 96 (55.8) 78 (36.3) <0.001* 2.22 (1.47–3.34) A/T/A-A/T/C 2 (1.2) 8 (3.7) 0.115 0.30 (0.06–1.45) A/T/A-G/C/C 13 (7.6) 13 (6.0) 0.555 1.27 (0.57–2.82) A/T/C-A/C/C 2 (1.2) 16 (7.4) 0.004* 0.15 (0.03–0.65) A/T/C-A/T/C 1 (0.6) 1 (0.5) 0.874 1.25 (0.08–20.15) A/T/C-G/C/C 1 (0.6) 5 (2.3) 0.168 0.25 (0.03–2.12) A/T/A 167 (97.1) 174 (80.9) <0.001* 7.87 (3.04–12.00) Non A/T/A 5 (2.9) 41 (19.1) 1.00 TNF-α (-308) A-A 3 (1.9) 2 (0.9) 0.747 1.98 (0.33–12.00) G-A 26 (16.1) 35 (16.6) 0.98 (0.56-1.71) G-G 132 (82.0) 174 (82.5) 1.00 -308 A allele 32 (9.9) 39 (9.2) 0.749 1.08 (0.66–1.77) -308 G allele 290 (90.1) 383 (90.8) 1.00 G-G 132 (82.0) 174 (82.5) 0.905 1.03 (0.60–1.77) Non G-G 29 (18.0) 37 (17.5) 1.00
The significance was evaluated by χ2 test or two-tailed Fisher’s exact test.
IL-10: interleukin-10; TNF-α: tumour necrosis factor-α; SLE: systemic lupus erythematosus; 95% CI: 95% confidence intervals; ND: not determined.
Table II. IL-10 haplotype frequencies of Taiwanese SLE patients with various clinical features.
Clinical features Allele (n=264) Genotype (n=132)
Ht1, Non-Ht1, Pc value Ht1/Ht1, Ht1/Non-Ht1, Non-Ht1/Non-Ht1, Pc-value
n=196 n=68 n=69 n=58 n=5
Number (%) Number (%) Number (%) Number (%) Number (%)
ANA 192 (98.0) 66 (97.1) 0.668 68 (98.6) 56 (96.6) 5 (100.0) 0.709 Immunologic disorder 150 (76.5) 56 (82.4) 0.318 50 (72.5) 50 (86.2) 3 (60.0) 0.108 Hematological disorder 99 (50.5) 33 (48.5) 0.778 35 (50.7) 29 (50.0) 2 (40.0) 0.898 CNS disorder 23 (11.7) 11 (16.2) 0.346 8 (11.6) 7 (12.1) 2 (40.0) 0.181 Renal disorder 81 (41.3) 29 (42.6) 0.849 29 (42.0) 23 (39.7) 3 (60.0) 0.673 Serositis 40 (20.4) 14 (20.6) 0.975 14 (20.3) 12 (20.7) 1 (20.0) 0.998 Arthritis 105 (53.6) 41 (60.3) 0.337 35 (50.7) 35 (60.3) 3 (60.0) 0.542 Oral ulcers 50 (25.5) 26 (38.2) 0.046 20 (34.5) 20 (34.5) 3 (60.0) 0.083 Photoseneitivity 87 (44.4) 35 (51.5) 0.313 27 (46.6) 27 (46.6) 4 (80.0) 0.286 Discoid rash 27 (13.8) 13 (19.1) 0.290 9 (15.5) 9 (15.5) 2 (40.0) 0.266 Malar rash 99 (50.5) 39 (57.4) 0.330 31 (53.4) 31 (53.4) 4 (80.0) 0.402 Ht1: A/T/A; N: number of SLE patients in genotype analysis; NS: not signifificant; ANA: anti-nuclear antibodies.
The chi-square test (2x2 table for haplotype; 2x3 table for genotype) was performed to obtain the p-value. SLE patients with ht1 were compared with SLE patients without ht1 after stratification by clinical features. The corrected P (Pc) values were adjusted by using Bonferroni’s correction for multiple compari-sons. Statistical significance was considered as Pc-value <0.0045 (0.05/11 clinical features).
various alleles and genotypes of IL-10
promoter haplotypes was analysed, and
the results are shown in Table II. No
significant differences in the clinical
features between patients with various
genotypes/haplotypes could be
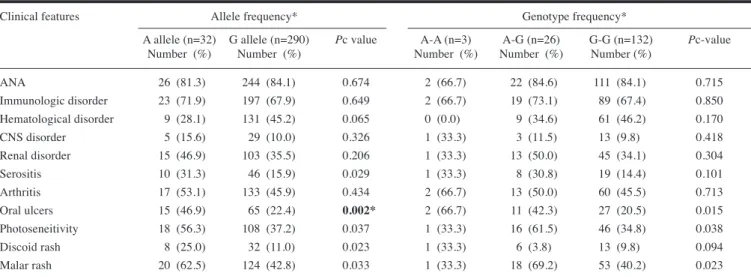
dem-onstrated. The association between the
clinical manifestations of SLE patients
with TNF-α genetic polymorphism was
also investigated. The allele and
geno-type frequencies of the polymorphisms
at -308 were significantly different in
patients with serositis, oral ulcers,
pho-tosensitivity, discoid rash and malar
rash (Table III). The G allele frequency
was significantly decreased in patients
with oral ulcers (Pc=0.002).
IL-10 and TNF-α genotypes in
Taiwanese SLE susceptibility and
clinical features
SLE patients were also classified into
the four possible combined genotypes
to investigate potential IL-10 and
TNF-α
interaction in SLE susceptibility
(Table IV). Analysis of the combined
IL-10 and TNF-α genotypes yielded
a significant different distribution in
patients and controls (p<0.001, 4x2
contingency table). The combined
frequencies of IL-10 A/T/A haplotype
and TNF-α G-G genotype were
sig-nificantly increased in SLE patients
(79.5% in SLE patients and 68.1% in
controls; p=0.012), whereas the
fre-Table III. TNF-α-308 genetic polymorphism of Taiwanese SLE patients with various clinical features.Clinical features Allele frequency* Genotype frequency*
A allele (n=32) G allele (n=290) Pc value A-A (n=3) A-G (n=26) G-G (n=132) Pc-value
Number (%) Number (%) Number (%) Number (%) Number (%)
ANA 26 (81.3) 244 (84.1) 0.674 2 (66.7) 22 (84.6) 111 (84.1) 0.715 Immunologic disorder 23 (71.9) 197 (67.9) 0.649 2 (66.7) 19 (73.1) 89 (67.4) 0.850 Hematological disorder 9 (28.1) 131 (45.2) 0.065 0 (0.0) 9 (34.6) 61 (46.2) 0.170 CNS disorder 5 (15.6) 29 (10.0) 0.326 1 (33.3) 3 (11.5) 13 (9.8) 0.418 Renal disorder 15 (46.9) 103 (35.5) 0.206 1 (33.3) 13 (50.0) 45 (34.1) 0.304 Serositis 10 (31.3) 46 (15.9) 0.029 1 (33.3) 8 (30.8) 19 (14.4) 0.101 Arthritis 17 (53.1) 133 (45.9) 0.434 2 (66.7) 13 (50.0) 60 (45.5) 0.713 Oral ulcers 15 (46.9) 65 (22.4) 0.002* 2 (66.7) 11 (42.3) 27 (20.5) 0.015 Photoseneitivity 18 (56.3) 108 (37.2) 0.037 1 (33.3) 16 (61.5) 46 (34.8) 0.038 Discoid rash 8 (25.0) 32 (11.0) 0.023 1 (33.3) 6 (3.8) 13 (9.8) 0.094 Malar rash 20 (62.5) 124 (42.8) 0.033 1 (33.3) 18 (69.2) 53 (40.2) 0.023 n: number of SLE patients in genotype analysis; NS: not significant; ANA: antinuclear antibodies.
χ2 test (2x2 table for allele frequency; 2x3 table for genotype frequency) were performed to obtain the p-value. The corrected P (Pc) values were adjusted by
using Bonferroni’s correction for multiple comparisons. Statistical significance was considered as Pc-value <0.0045 (0.05/11 clinical features).
*Pc-value was <0.0045.
Table IV. IL-10 and TNF-α genotypes in Taiwanese SLE susceptibility. SLE patients
Controls, n. (%) n. (%) p-value Odds ratio (95% CI)
Combined IL-10 and TNF-α n=211 n=161
A/T/A vs. G-G 143 (68.1) 128 (79.5) 0.012* 1.84 (1.14-2.98) A/T/A vs. non G-G 25 (11.9) 29 (18.0) 0.094 0.61 (0.34-1.09) Non A/T/A vs. G-G 30 (14.3) 4 (2.5) <0.001* 0.15 (0.05-0.45) Non A/T/A vs. non G-G 12 (5.7) 0 (0.0) 0.002* ND
Trend test <0.001*
IL-10: interleukin-10; TNF-α: tumour necrosis factor-α; SLE: systemic lupus erythematosus; 95% CI: 95% confidence intervals; ND: not determined. *p value was <0.05.
Table V. Influence of TNF-α-308 genotype on the clinical features of Taiwanese SLE pa-tients with IL-10 ATA genotype.
Clinical features TNF-α G-Gq TNF-α non G-G Pc-value
(total n=107) (total n=25) Number (%) Number (%) ANA 104 (97.2) 24 (96) 0.753 Immunologic disorder 86 (80.37) 20 (80) 0.966 Haematological disorder 58 (54.21) 8 (32) 0.046 CNS disorder 11 (10.28) 4 (16) 0.417 Renal disorder 43 (40.19) 14 (56) 0.151 Serositis 19 (17.76) 9 (36) 0.045 Arthritis 56 (52.34 14 (46) 0.741 Oral ulcers 25 (23.36) 13 (52) 0.004# Photoseneitivity 43 (40.19) 16 (64) 0.031 Discoid rash 12 (11.21) 7 (28) 0.031 Malar rash 50 (46.73) 18 (72) 0.023
χ2 test (2x2 table for allele frequency; 2x3 table for genotype frequency) were performed to obtain the p-value. The corrected P (Pc) values were adjusted by using Bonferroni’s correction for multiple
com-parisons. Statistical significance was considered as Pc-value <0.0045 (0.05/11 clinical features).
quencies of IL-10 non A/T/A haplotype
and TNF-α G-G genotype were
signifi-cantly decreased in SLE patients (2.5%
in SLE patients and 14.3% in controls;
p<0.001). The association between the
clinical manifestations of SLE patients
with the combined genotypes was also
investigated (Table V). The combined
frequencies of IL-10 A/T/A haplotype
and TNF-α G-G genotype were
sig-nificantly different in patients with
oral ulcers (Table V). The combined
frequencies of IL-10 A/T/A haplotype
and TNF-α G-G genotype were
signifi-cantly decreased in patients with oral
ulcers (Pc=0.004).
Discussion
We have found a relation between
pol-ymorphisms at the promoter region of
IL-10 and TNF-α genes and the SLE
susceptibility and a significant
correla-tion of the combined IL-10 and TNF-α
genetic polymorphisms contribute to
clinical features was also observed in
the Taiwanese population.
Our results showed that IL-10
A/T/A-A/T/A genotype was associated with
Taiwanese SLE, whereas, no
signifi-cant differences in the clinical
fea-tures between patients with various
genotypes/haplotypes could be
dem-onstrated. Many studies have shown
conflicting evidence for and against
association of SLE with various IL-10
genetic polymorphisms (13-17, 35-40).
Rood et al. reported that the ATA
hap-lotype is associated with
neuropsychi-atric manifestations of SLE among the
Dutch population,(15) while Mok et
al. indicated that this haplotype is not
associated with SLE susceptibility, but
is associated with renal involvement in
the SLE patients (16). However, Chong
et al. identified that the non-ATA
hap-lotype is associated with SLE patients
with serositis (17). These results
sug-gest that SLE is a complicated disease.
And the involvements of genetic
fac-tors as well as certain environmental
factors might also be essential in
dis-ease predisposition and progression.
The allele and genotype frequencies of
the polymorphism at -308 were not
sig-nificantly different in Taiwanese SLE
patients and controls. Many studies
have also shown conflicting evidence
for and against association of SLE with
various TNF locus polymorphisms
(25-31). A recent meta-analysis of the
TNF-α
-308G/A promoter polymorphism in
SLE revealed a significant association
found in European population, but not
in Asian or African populations (27).
Our results are in agreement with this
conclusion that there is no significant
association at the -308 position of
TNF-α promoter gene in our
Taiwan-ese population. However, the G allele
of the polymorphism at -308 was
sig-nificantly decreased in patients with
oral ulcers. The functional analysis of
polymorphism in the promoter region
of TNF-α -308 position yielded
con-flicting observations. Some studies
have suggested that the TNF-α -308 A
allele has higher transcriptional
activ-ity, while other studies showed that this
polymorphism appeared not to
influ-ence TNF-α production (41-44). The
association between the genetic
poly-morphism at -308 and TNF-α
produc-tion remains to be characterised.
Since the two regulators of the
inflam-matory response- IL-10 and TNF-α
have been suggested for the
involve-ment of SLE pathogenesis, we have
also investigated the interaction
be-tween IL-10 and TNF-α in Taiwanese
SLE susceptibility as well as clinical
features. Our results showed that the
combined frequencies of IL-10 A/T/A
haplotype and TNF-α G-G genotype
were significantly increased in SLE
patients. In addition, the combined
frequencies of IL-10 A/T/A haplotype
and TNF-α G-G genotype were
signifi-cantly decreased in patients with oral
ulcers. The effects of cytokines may be
greatly conditioned by the presence of
other cytokines, particularly in the case
of IL-10 and TNF-α, which have
com-plex and predominantly opposing roles
in the systemic inflammatory
respons-es. Suarez et al. reported that in
Span-ish SLE patients, there was a strong
as-sociation between susceptibility to SLE
and the high TNF-α producer genotype,
Supplemental Table II. TNF-α polymorphism evaluated in SLE susceptibility and related clinical features.Gene name Primers PCR PCR conditions Restriction Alleles DNA Position
(Nucleotide change) product size (annealing enzyme site fragment
(SNP database ID) (bp) temperature) size (bp)
TNF-α-308 (A/G) Forward:5’-AGGCAATAGGTTTTGAGGGCCAT-3’ 117 ouchdown Nco I A 117 chr6:31,651,010
(rs1800629) Reverse:5’-ACACTCCCCATCCTCCCGGCT-3’ 60-50℃ G 97.20
Supplemental Table I. IL-10 promoter polymorphisms evaluated in Taiwanese SLE patients and controls. Gene name Report 1 Allele Report 1 Report 2 Allele Report 2 Context Sequence
(Nucleotide change) Dye Quencher Dye Quencher (SNP database ID)
IL-10 -1082 (A/G) VIC T NFQ FAM C NFQ TCCTCTTACCTATCCCTACTTCCCC[T/C]TCCCAAAGAAGCCTTAGTAGTGTTG
(rs1800896)
IL-10 -819 (C/T) VIC A NFQ FAM G NFQ AGTGAGCAAACTGAGGCACAGAGAT[A/G]TTACATCACCTGTACAAGGGTACAC
(rs1800871)
IL-10 -592 (C/A) VIC T NFQ FAM G NFQ CTTTCCAGAGACTGGCTTCCTACAG[T/G]ACAGGCGGGGTCACAGGATGTGTTC
(rs1800872)
independently of IL-10 production and
individuals harbouring high IL-10/low
TNF-α producer genotype tend to
de-velop DLE. These results suggest there
may be ethnic difference, genetic
fac-tors as well as certain environmental
factors involved in SLE disease
predis-position and progression.
In conclusion, our observations suggest
that the combined genotypes showed an
association with IL-10/ TNF-α genotype
in Taiwanese SLE patients and could
influence different SLE phenotypes.
References
1. KOTZIN BL: Systemic lupus erythematosus.
Cell 1996; 85: 303-6.
2. NATH SK, KILPATRICK J, HARLEY JB: Genet-ics of human systemic lupus erythematosus: the emerging picture. Curr Opin Immunol 2004; 16: 794-800.
3. ROBAK E, SYSA-JEDRZEJOWSKA A, ROBAK T, SMOLEWSKI P: Peripheral blood lym-phocyte apoptosis and circulating dendritic cells in patients with systemic lupus ery-thematosus: correlation with immunological status and disease-related symptoms. Clin
Rheumatol 2006; 25: 225-33.
4. KYTTARIS VC, KATSIARI CG, JUANG YT, TSOKOS GC: New insights into the pathogen-esis of systemic lupus erythematosus. Curr
Rheumatol Rep 2005; 7: 469-75.
5. GRONDAL G, GUNNARSSON I, RONNELID J, ROGBERG S, KLARESKOG L, LUNDBERG I: Cytokine production, serum levels and dis-ease activity in systemic lupus erythemato-sus. Clin Exp Rheumatol 2000; 18: 565-70. 6. AL-JANADI M, AL-BALLA S, AL-DALAAN A,
RAZIUDDIN S: Cytokine profile in systemic lupus erythematosus, rheumatoid arthritis, and other rheumatic diseases. J Clin
Immu-nol 1993; 13: 58-67.
7. CHUNG EY, LIU J, ZHANG Y, MA X: Differ-ential expression in lupus-associated IL-10 promoter single-nucleotide polymorphisms is mediated by poly(ADP-ribose) polymer-ase-1. Genes Immun 2007; 8: 577-89. 8. LALANI I, BHOL K, AHMED AR:
Interleukin-10: biology, role in inflammation and autoim-munity. Ann Allergy Asthma Immunol 1997; 79: 469-83.
9. ROUSSET F, GARCIA E, DEFRANCE T et al.: Interleukin 10 is a potent growth and differ-entiation factor for activated human B lym-phocytes. Proc Natl Acad Sci USA 1992; 89: 1890-3.
10. PARK YB, LEE SK, KIM DS, LEE J, LEE CH, SONG CH: Elevated interleukin-10 levels correlated with disease activity in systemic lupus erythematosus. Clin Exp Rheumatol 1998; 16: 283-8.
11. TURNER DM, WILLIAMS DM, SANKARAN D, LAZARUS M, SINNOTT PJ, HUTCHINSON IV: An investigation of polymorphism in the interleukin-10 gene promoter. Eur J
Immu-nogenet 1997; 24: 1-8.
12. EDWARDS-SMITH CJ, JONSSON JR, PURDIE DM, BANSAL A, SHORTHOUSE C, POWELL
EE: Interleukin-10 promoter polymorphism predicts initial response of chronic hepatitis C to interferon alfa. Hepatology 1999; 30: 526-30.
13. KHOA PD, SUGIYAMA T, YOKOCHI T: Poly-morphism of interleukin-10 promoter and tu-mor necrosis factor receptor II in Vietnamese patients with systemic lupus erythematosus.
Clin Rheumatol 2005; 24: 11-13.
14. LAZARUS M, HAJEER AH, TURNER D et al.:
Genetic variation in the interleukin 10 gene promoter and systemic lupus erythematosus.
J Rheumatol 1997; 24: 2314-7.
15. ROOD MJ, KEIJSERS V, VAN DER LINDEN MW et al.: Neuropsychiatric systemic lupus
erythematosus is associated with imbalance in interleukin 10 promoter haplotypes. Ann
Rheum Dis 1999; 58: 85-9.
16. MOK CC, LANCHBURY JS, CHAN DW, LAU CS: Interleukin-10 promoter polymorphisms in Southern Chinese patients with systemic lupus erythematosus. Arthritis Rheum 1998; 41 :1090-5.
17. CHONG WP, IP WK, WONG WH, LAU CS, CHAN TM, LAU YL: Association of inter-leukin-10 promoter polymorphisms with systemic lupus erythematosus. Genes Immun 2004; 5: 484-92.
18. LIN PW, HUANG CM, HUANG CC, TSAI CH, TSAI JJ, CHANG CP, TSAI FJ: The associa-tion of -627 interleukin-10 promoter poly-morphism in Chinese patients with systemic lupus erythematosus. Clin Rheumatol 2007; 26: 298-301.
19. SURYAPRASAD AG, PRINDIVILLE T: The biology of TNF blockade. Autoimmun Rev 2003; 2: 346-57.
20. KOLLIAS G, DOUNI E, KASSIOTIS G, KON-TOYIANNIS D: The function of tumour necro-sis factor and receptors in models of multi-organ inflammation, rheumatoid arthritis, multiple sclerosis and inflammatory bowel disease. Ann Rheum Dis 1999; 58 (Suppl. 1): I32-9.
21. SERRANO NC, MILLAN P, PAEZ MC: Non-HLA associations with autoimmune diseases.
Autoimmun Rev 2006; 5: 209-14.
22. ARINGER M, FEIERL E, STEINER G et al.:
Increased bioactive TNF in human systemic lupus erythematosus: associations with cell death. Lupus 2002; 11: 102-8.
23. MAURY CP, TEPPO AM: Tumor necrosis fac-tor in the serum of patients with systemic lupus erythematosus. Arthritis Rheum 1989; 32: 146-50.
24. GABAY C, CAKIR N, MORAL F et al.:
Circu-lating levels of tumor necrosis factor soluble receptors in systemic lupus erythematosus are significantly higher than in other rheu-matic diseases and correlate with disease activity. J Rheumatol 1997; 24: 303-8. 25. ROOD MJ, VAN KRUGTEN MV, ZANELLI E et
al.: TNF-308A and HLA-DR3 alleles
con-tribute independently to susceptibility to sys-temic lupus erythematosus. Arthritis Rheum 2000; 43: 129-34.
26. HIRANKARN N, AVIHINGSANON Y, WONGPI-YABOVORN J: Genetic susceptibility to SLE is associated with TNF-alpha gene polymor-phism -863, but not -308 and -238, in Thai population. Int J Immunogenet 2007; 34: 425-30.
27. LEE YH, HARLEY JB, NATH SK: Meta-analy-sis of TNF-alpha promoter -308 A/G poly-morphism and SLE susceptibility. Eur J
Hum Genet 2006; 14: 364-71.
28. ZUNIGA J, VARGAS-ALARCON G, HER-NANDEZ-PACHECO G, PORTAL-CELHAY C, YAMAMOTO-FURUSHO JK, GRANADOS J: Tumor necrosis factor-alpha promoter poly-morphisms in Mexican patients with system-ic lupus erythematosus (SLE). Genes Immun 2001; 2: 363-6.
29. PARKS CG, PANDEY JP, DOOLEY MA et al.:
Genetic polymorphisms in tumor necro-sis factor (TNF)-alpha and TNF-beta in a population-based study of systemic lupus erythematosus: associations and interaction with the interleukin-1alpha-889 C/T poly-morphism. Hum Immunol 2004; 65: 622-31. 30. TSUCHIYA N, KAWASAKI A, TSAO BP,
KOMA-TA T, GROSSMAN JM, TOKUNAGA K: Analy-sis of the association of HLA-DRB1, TN-Falpha promoter and TNFR2 (TNFRSF1B) polymorphisms with SLE using transmission disequilibrium test. Genes Immun 2001; 2: 317-22.
31. FERNANDO MM, STEVENS CR, SABETI PC et al.: Identification of two independent risk
factors for lupus within the MHC in United Kingdom families. PLoS Genet 2007; 3: e192.
32. HOCHBERG MC: Updating the American Col-lege of Rheumatology revised criteria for the classification of systemic lupus erythemato-sus. Arthritis Rheum 1997; 40: 1725. 33. STEPHENS M, DONNELLY P: A comparison
of bayesian methods for haplotype recon-struction from population genotype data. Am
J Hum Genet 2003; 73: 1162-9.
34. STEPHENS M, SMITH NJ, DONNELLY P: A new statistical method for haplotype recon-struction from population data. Am J Hum
Genet 2001; 68: 978-89.
35. CRAWLEY E, WOO P, ISENBERG DA: Single nucleotide polymorphic haplotypes of the interleukin-10 5’ flanking region are not as-sociated with renal disease or serology in Caucasian patients with systemic lupus ery-thematosus. Arthritis Rheum 1999; 42: 2017-8.
36. HIRANKARN N, WONGPIYABOVORN J, HAN-VIVATVONG O et al.: The synergistic effect
of FC gamma receptor IIa and interleukin-10 genes on the risk to develop systemic lupus erythematosus in Thai population. Tissue
An-tigens 2006; 68: 399-406.
37. ROSADO S, RUA-FIGUEROA I, VARGAS JA et al.: Interleukin-10 promoter polymorphisms
in patients with systemic lupus erythemato-sus from the Canary Islands. Int J
Immuno-genet 2008; 35: 235-42.
38. SOBKOWIAK A, LIANERI M, WUDARSKI M, LACKI JK, JAGODZINSKI PP: Genetic vari-ation in the interleukin-10 gene promoter in Polish patients with systemic lupus ery-thematosus. Rheumatol Int 2009; 29: 921-5. 39. SUAREZ A, LOPEZ P, MOZO L, GUTIERREZ C:
Differential effect of IL10 and TNF{alpha} genotypes on determining susceptibility to discoid and systemic lupus erythematosus.
Ann Rheum Dis 2005; 64: 1605-10.
40. VAN DER LINDEN MW, WESTENDORP RG, STURK A, BERGMAN W, HUIZINGA TW: High
interleukin-10 production in first-degree rel-atives of patients with generalized but not cu-taneous lupus erythematosus. J Investig Med 2000; 48: 327-34.
41. WILSON AG, SYMONS JA, MCDOWELL TL, MCDEVITT HO, DUFF GW: Effects of a poly-morphism in the human tumor necrosis factor alpha promoter on transcriptional activation.
Proc Natl Acad Sci USA 1997; 94: 3195-9.
42. KROEGER KM, CARVILLE KS, ABRAHAM LJ: The -308 tumor necrosis factor-alpha pro-moter polymorphism effects transcription.
Mol Immunol 1997; 34: 391-9.
43. HE B, NAVIKAS V, LUNDAHL J, SODER-STROM M, HILLERT J: Tumor necrosis factor alpha-308 alleles in multiple sclerosis and
optic neuritis. J Neuroimmunol 1995; 63: 143-7.
44. BAYLEY JP, DE ROOIJ H, VAN DEN ELSEN PJ, HUIZINGA TW, VERWEIJ CL: Functional analysis of linker-scan mutants spanning the -376, -308, -244, and -238 polymorphic sites of the TNF-alpha promoter. Cytokine 2001; 14: 316-23.