The Design and Development of a Physician-Oriented Information
Infrastructure for the Enhancement of e-Hospital Facilities.
Hsu-Hua Ho
1, Tzu-Yi Yu
2, Hung-Pin Hou
3, Wen-Yung Wu
4Director of Internal Medicine Department, Puli Christian Hospital
1Assistant Professor, National Chi Nan University
2Director of Administrative Department, Puli Christian Hospital
3Director of Radiological Department, Puli Christian Hospital
4[email protected]
1, [email protected]
2, [email protected]
3Abstract
Recent advancements in modern medical diagnoses have necessitated a huge increase in the frequency of the use of equipment such as CT and ultrasound machines. Correspondingly, the storage and dissemination of these medical images have become an important issue to medical professionals. Management of these images has traditionally been slow and cumbersome. With the prevalence of the personal computer, however, along with increased network bandwidth, it is now possible to handle this information electronically as well as wirelessly. The Picture Archiving and Communication System (PACS) is at the forefront of this revolution. Yet, commercially available PACS software is generally very expensive and hard to afford for hospitals with limited financial resources. A dilemma among many hospitals is deciding how to acquire and implement the proper PACS system without unduly affecting the budget. In this paper, a full-function, efficient, and economical PACS system is presented as a viable, non-compromising option for many small and medium-sized hospitals. This system, designed and developed mainly by the physicians and technicians of the Puli Christian Hospital (PCH), with the cooperation from academics, allows for customization to fit the needs of the individual hospital. This system can be used as the foundation of the health information infrastructure and to enhance e-Hospital service.
1. Introduction
There are always unexpected catastrophes or severe infectious diseases which might occur from time to time. Unforgettable experiences such as the 911 attack in New York, the SARS epidemic in Taiwan during 2003, and the hurricane Katrina in New Orleans Louisiana and Mississippi in 2005 have been very prominent news items. These incidents not only created unimaginable chaos, but it also impacted against the local Medical and Medicare systems. From reading the review reports of these tragedies, one of the important conclusions that can be reached is that if the documentation/information is not stored electronically, it can be destroyed by these unexpected events (such as by explosion or flood) and cannot be recovered or can be recovered only with the
expenditure of much time and effort. This conclusion actually agrees with one of the major goals of the “National Health Information Infrastructure” (NHII) project presented by the US Department of Health and Human Services [1]. It hopes to reach the “Paperless Healthcare” by the year of 2010. Similar to this project, the National Health Service (NHS) of the Great Britain has the “National Program for IT” project [2], and the Department of Health of Canada also has the “Electronic Health Record (EHR)” program which tries to promote the digitalization of patient records [3] to create a paperless environment. The goal of the EHR is not only to save and store patients’ information more securely, but also to transfer electronic more easily when patients are referred to another hospital. These electronic records will give the doctors a better picture of their patients’ medical history, reduce the waste associated with unnecessarily repeated examinations. Furthermore, with electronic health records, hospitals can easily provide useful statistical reports to the Health Department.
In light of these global tendencies, the Department of Health (DoH), Executive Yuan, R.O.C. (Taiwan) is sponsoring the “National Health Information Infrastructure” (NHII) project which focus is on the integration and extension of some original carry on projects [4, 5, 6, 7]. The main visions of this NHII project is to “establish a national-wide e-Health environment and to build-up new information sharing model for Healthcare and Medicare services”. The DoH is also trying to encourage medical facilities to utilize emerging internet and computer technology to develop and enhance in-house computer infrastructures. This is the basis of the motivation for the Puli Christian Hospital to design the “Picture Archiving and Communication System” (PACS). PACS was first announced in 1980s, and its intent was to achieve a paperless/filmless environment for the hospitals and clinics. This goal actually matches the objective of the NHII project. As a matter of fact, the PACS not only digitalizes the patients’ personal information and their medical histories, but it also stores and retrieves medical images obtained from any medical examination electronically. Even though controversy has followed the use and developments of the PACS [8, 9, 10, 12, 13], the Taichung Veterans General Hospital first presented their PACS system in 1999 [11]. The PCH was inspired
and motivated by this successful experience, but it came to the conclusion that most commercial PACS are not only prohibitively expensive, but they lack the customization feature required for each hospital. Furthermore, one of the important missions for PCH is to provide healthcare services for the surrounding mountainous region and remote areas where medical resources are severely lacking. Only by developing an in-house PACS can costs be greatly reduced while still providing exemplary health care for the patients and the community around the Nantou, Puli County – a region that is far removed from the nearest metropolitan city.
2. System Architecture
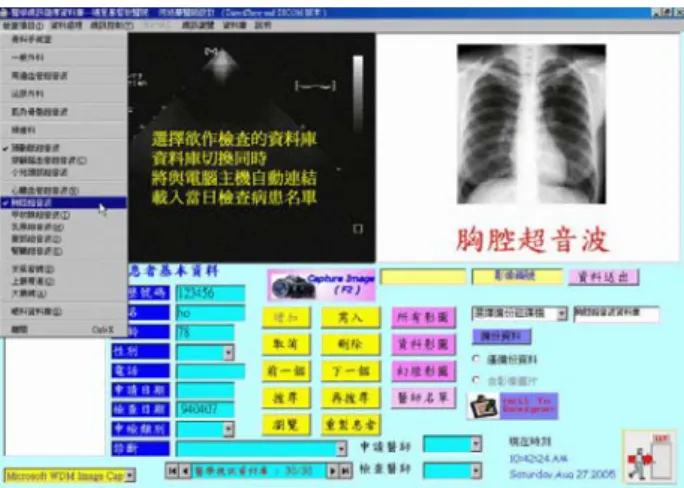
As is the case with many other regional hospitals, Puli Christian Hospital lacks the financial resources to purchase expensive PACS facilities. In order to reduce costs and use the current available resource, and also because of the availability of the personal computer, this PCH-PACS system is developed based on the PC-Windows platform. One immediate and obvious advantage to this is that there is virtually no training expenses involved since the Windows-based operating system is very popular in this country. Basically, this system can be divided into two parts: database design and image processing (including acquisition and retrieval). This system evolved in several distinct stages. Originally it was built under Visual Basic and Access databases. Later, the VBA (Visual Basic Applications) embedded with the Access component was used as the front end program, and the SQL server was used as the back end database. After the Microsoft Company came out with their new Operating System and software, this system incorporated the advantage of the continuous update feature, giving it better stability under the Microsoft XP .NET framework. Figure 1 shows this in-house self-made software system.
Figure 1 The self-made PACS system used in PCH.
2.1. Medical Database Design
In order to synchronize the PACS system with the original Healthcare Information System (HIS) and to reduce the development costs, the minimum requirement for the database is that the PACS system database schema should be designed to fit for implementation in a relational database. In addition, the medical database management systems and applications developed to manipulate data stored in databases should provide reporting functions easily and communicating with other packages effortlessly. The Access and SQL database were chosen because of these flexibilities. Access is embedded with VBA as the front end program, and the SQL server is used as the back end database server. The SQL server is a robust database; it can handle huge dataset even if they are located on different hard drives. They are Microsoft software and can embed other Microsoft components. Their statistical functions are useful and can be adopted for medical statistical reports. The data integrity features allow them to maintain consistent medical data constraint when new records are added to the database. The data security feature is capable of protecting sensitive information with varying levels of access privileges. The concurrency control allows different physicians to access, manipulate and update this database simultaneous at the same time in different locations. Automatic periodically backup is performed to protect this medical database. Either from the viewing workstation or from the server, the strong backup system protects the electronic health records and the medical images well. After years of operations under real-life situations, it has been determined that a robust database is the foundation of a successful PACS system. This medical database not only may be used to store the information securely, but it can also function as a communication channel to provide fast and accurate data retrieval and display.
2.2. Medical Images Processing
Most of the available PACS systems in medical facilities today are used to acquire, retrieve, and store the medical images. This information is generally in the form of still images (not the dynamical image such as the Audio Video Interactive (avi) file). They are obtained from various sources, such as from the Computed Tomography (CT), Magnetic Resonance Imaging (MRI), Breast Ultrasound, Echocardiography and Cardiac Doppler Ultrasound and from Transcranial Color-Coded Sonography, … etc. Therefore, the major concerns are how to obtain high quality images with affordable devices and how to configure the system to retrieve images instantaneously from the database and then display them fluently throughout the intranet. Thanks fully the notable progress in hardware development, spurred on by market competition, has resulted in graphics and acquisition cards that are not only more affordable, but has much better quality than
ever before. This in-house PACS system adopts a PCI (Peripheral Component Interconnect)-based acquisition card to capture most of the images. Most images are stored as still images, i.e., the single image format in the medical database. However, a Cardiac Ultrasound is much more useful if it can display how the blood flow moves between the atrium and ventricle of the heart. Hence, the dynamical image (also known as animation pictures) file format is needed. Based on different requirements, this system can store images in still or animated formats. In other words, when the images are being acquired, the system can store them into BMP, JEP or DICOM (Digital Imaging and Communication in Medicine) files format (still image file format) or AVI, WMV or MOTION_JPEG (the animated file format).
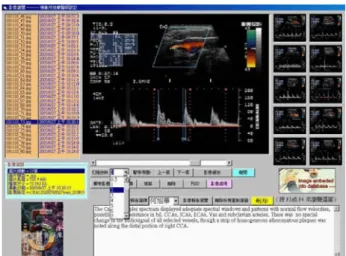
There are instances when physicians need to manipulate the acquired images. Editing functions such as the zooming in/out, brightness and contrast adjustments, local region enlargement for detail texture, distance or area measurement … etc., are all provided through a user-friendly interface. Another useful function is that all the images acquired or retrieved can be linked together into a slideshow for demonstration purposes. For those medical instruments (such as endoscope and ultrasound) that produce non-DICOM images, a special multimedia video card is used to digitize and capture the medical video image into dynamical or statical file format and then store them into the PACS image database. The related functionalities and the features will be discussed in the next section. Figure 2 shows the system architecture of the PACS used in PCH.
Figure 2 The PACS system Architecture in PCH.
3. System Features
As previously mentioned, this in-house software was primarily developed by the attending physicians of the PCH. The graphics user interface is very friendly and follows the conventional window software architecture. As Figure 1 shows, the GUI is displayed with Chinese characters, making it easy to manipulate even for the non-technical users. When a physician desires to access the system to obtain information on a patient, all the examination results completed the same day will be displayed, even if the patient had visited more than one
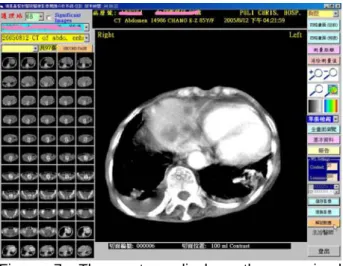
doctor in different departments. Data deserving of urgent or immediate attention will automatically be displayed in red. If any image-related tests were performed, those images can also be shown on a high resolution computer monitor. A complicated examination might be composed of more than one image. This system allows the physician to view pictures in either single image or multiple (4 or 16) image mode. If the same examination was performed previously, this system can also display these two sets of images together, allowing the doctor to track the patient’s prognosis and to follow the progress of the disease to determine if the patient is getting better or worse. Figure 3 demonstrates this functionality.
Figure 3 Multi-image display mode of the in-house PACS system.
Preparing the diagnostic reports with medical images is very tedious work. This new system allows the physicians to embed the medical images in the report by selecting the image and then clicking the “Report” option. The selected image(s) can be placed either vertically or horizontally. Text can easily be made to flow around the images. Since most patients’ symptoms can be classified, and some of them are either similar or the same, the physicians can use the system to pre-define these symptoms, along with their suggested method of treatment and/or comments. In specifying the parameters of the reports, these pre-defined items can be included to reduce the amount of typing. Furthermore, in order to take advantage of the electronic referral procedure, the physician (after inputting administrative permission and security clearance) can use this system to easily attach the medical images along with the diagnostic reports, and then utilize Microsoft email system (such as Outlook Express or Outlook) to disseminate the information to designated personal in other hospitals. Even though sending the information through the email system could cause the security concern, yet the encryption approach, request return receipt and the digital signature can be used to meet the authentication, integrity and nonrepudiation security purpose. These features are demonstrated in Figure 4 and Figure 5 respectively.
Figure 4. Easy report generation feature.
Figure 5. The software integrates email system for e-referral procedure.
When the PACS was first announced, one of its goals was to create a paperless working environment. However, after several years of development, realistic expectations have been re-focused towards increasing the rate of correct diagnosis in order to diagnose and treat the patients as quickly as possible. The way this system is developing is in this direction. It possesses very useful and efficient manipulative functions when examining the desired images. For example, the physician can use the mouse to select the interested area, and then enlarge this region to view more detailed information. By using the scrolling function of the mouse wheel, various properties of the image, such as the brightness, contrast or quality, can be easily adjusted. In many cases, the distance or the size of particular image, such as the tumor size, means a lot to the medical treatment. This system also provides the flexibility to allow the doctor to measure the distance and area multiple times over the image directly. This distance information is also preserved when exported to the diagnostic report. In addition, if further image manipulation function is needed, this system can evoke other image manipulation software such as PhotoShop to perform the editing. The images can also be copied and
pasted into other software packages to make illustration material for training purposes. These functions are shown in Figure 6.
Even though this system was originally designed for the attending physician, resident physicians or any clinicians who are outside of their area of specialty can easily use this system. However, there is always the desire to increase the practicability and convenience for the PACS. As medical science becomes more diversified and specialized, even an experienced physician might have difficulty in making correct judgments when examining results from other specialties. To overcome this obstacle for physicians or other technicians using this software, when the user selects an image, the appropriate image database with related documentation will be displayed. The user can then compare the images in order to obtain necessary information relating to the image and/or to confirm the symptoms of a particular disease. This practical function is demonstrated in Figure 7 and Figure 8.
Figure 6. The system has strong image manipulation capability.
Figure 7. The system displays the examined images which are then compared with the appropriate medical images.
Figure 8. The system can bring in standard images with detail documentation for comparison so that the physicians can have better confirmation and understanding of patients’ conditions.
After several years of evolution, the internet activities have become an important part of people’s regular daily life. According to the recent statistical report, the time spent engaged in internet browsing activities for people in Taiwan ranks among the top five worldwide. The fact that the internet has been deeply embraced indicates that the web browser can be a very convenient tool for collecting the information needed. With this in mind, this PACS system allows the world wide web-based viewer to access the database server through the Local Area Network (LAN). This web-based viewing system allows physicians to check examination results and retrieve image archived through the hospital internet into the PACS servers. It is a design based on the DICOM 3.0 standard format over TCP/IP communications protocol. With tight security control (such as firewall and password protection and access privilege settings), the system provides a convenient way for the attending physician or any clinician to verify a patient’s condition at any time. The system also automatically tracks all activities when a physician uses this web-based viewing software, and saves the histories into the system log. The system administrator can monitor all accesses through this history log to prevent any illegal web actions. These functions are demonstrated in Figure 9 and Figure .
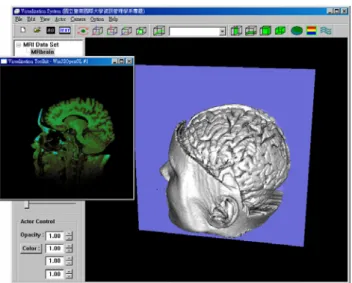
One of the on going projects is to integrate 3D medical database browsing into this system. Two major graphics libraries are used to develop this 3D browsing feature –the vtk [14, 15] and itk [16]. The vtk (Visualization ToolKit) and itk (National Library of Medicine Insight Segmentation and Registration Toolkit) are open-source, freely available software systems for computer graphics, image processing, and visualization. It supports hundreds of algorithms in visualization and image processing fields. These two libraries were designed primarily for medical research. They also support different computer language bindings, and are
available on different computer platforms such as Linux or Windows. The user can operate the arrow keys to move the sliding plane for the desired cutting plane or to rotate the mouse to visualize the entire medical object in three dimensions freely.
Figure 9. The login interface for the web-based viewing system.
Figure 10. Web-based viewing interface allows online browsing of patient examination results.
Figure 11. The interactive three dimensional browsing feature for medical data set.
4. System Performance
Puli Christian Hospital has in place a high speed internet and intranet communication system that has been in operation for a number of years. Recently, the 10/100/1000 Base-T Ethernet was installed. With this high speed communication capability, image retrieval and display processes can be carried out very smoothly at each viewing terminal. The average response time is 0.2 seconds for retrievalof a CT image and 0.08 seconds for retrieval of an ultrasound or endoscopic image. There are currently over 40 terminals that can access the medical database at the same time without notable lag. Since this PACS is an in-house developed software, the cost of the entire system is proportional to the hardware (mainly, the viewing terminals). For each single unit, the hardware is equipped with a PC (Cerelon CPU, 512 MB RAM) and one 19-inch LCD monitor with 1280 x 1024 resolution, with a cost of approximately $900 USD. The HP ProLiant, which is being used as the image server, is equipped with a 200 Gigabyte hard drive storage capacity. For data backup purposes, the RAID (Redundant Array of Independent Disks) system with four 300 Gigabyte hard drives is used.
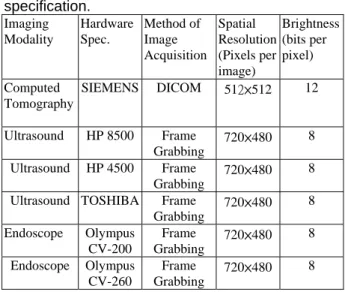
As it was mentioned previously, the image quality is of particular importance for the PACS system. For those images that are available in digital format (such as the Computed Tomography), there is no need to do any conversion. However, for those non-digital sources, there is a need to capture those images with a special graphical device. An “ASUS Extreme AX 700 PRO” acquisition card (also known as Frame Grabber) is used to obtain high quality images. The price for this card is around $250 USD each, and this device is currently installed for the following five procedures: the Cerebrovascular Ultrasound, Cardiac Ultrasound, Abdomen Ultrasound, Kidney Ultrasound, and the Upper and Lower alimentary endoscope. Because these five different departments have different hardware equipments, the organic interface necessary for these machines to capture images is very important. A user-friendly interface was designed for these non-DICOM apparatus to capture these images and store them in the medical database. When images from these sources are acquired, the system can convert them to JPG, BMP, DICOM or any animated formats (AVI or WMV). Table 1 shows the image quality and the hardware specification used, and Table 2 shows the number of patients and number of images acquired and processed in one month (March 01 to March 31, 2006).
Most commercial PACS systems are sold based on either the number of desired licenses or the “KeyPro” purchase which locks the view terminals. Hence, increasing the number of view station not only increases the hardware cost but also the software expense, resulting in a heavy financial load to the medical
facilities. For government-supported clinics or metropolitan hospitals, the financial pressure may not be a major concern. However, because regional medical facilities handles not only local residents’ medical problems but also has the responsibility to provide healthcare services for the mountainous area or remote communities, the in-house self-made PACS means a lot since it can be freely duplicated without incurring excessive hospital expenses.
Table 1. Image quality and the hardware specification. Imaging Modality Hardware Spec. Method of Image Acquisition Spatial Resolution (Pixels per image) Brightness (bits per pixel) Computed Tomography SIEMENS DICOM 512×512 12 Ultrasound HP 8500 Frame Grabbing 720×480 8 Ultrasound HP 4500 Frame Grabbing 720×480 8
Ultrasound TOSHIBA Frame
Grabbing 720×480 8 Endoscope Olympus CV-200 Frame Grabbing 720×480 8 Endoscope Olympus CV-260 Frame Grabbing 720×480 8
Table 2. Images acquired during March, 2006 Imaging Modality Number of Patients Number of Images Amount of storage used CT 221 7004 3820 Mbyte Ultrasound 460 2886 193 Mbyte Endoscope 120 1080 74 Mbyte Total 801 10970 4087 Mbyte 5.
Conclusion
When PACS was first announced in the 80s, many people, especially the radiologists, expressed high interest and expected that it could help the hospital achieve a filmless environment. Even though there were controversies during the development period, PACS has become an indispensable tool in hospital operations. However, the main obstacles preventing wide scale implementation of PACS among all the hospitals and clinics are its cost and lack of flexibility. Most PACSs were developed by vendors and software companies, and can generally be afforded only by metropolitan hospitals. In addition, because they were developed by software companies who were anticipating that they would be used by a full-service hospital, these PACSs may not completely fit the needs of diverse or smaller hospitals. For regional hospitals with limited budget, it has been even more difficult to promote the system in serving the needs of their patients. According to statistics reports from the Department of Health, Executive Yuan, R.O.C., only around 7% of hospitals in Taiwan utilize the PACS.
To overcome this restriction in Puli Christian Hospital, a customized PACS system has been developed by their in-hospital physicians and technicians from the Information Department. It is well known that in order to develop productive software, a good and thoughtful system analysis needs to be performed prior to building a PACS that will fit the needs of the hospital. In order to achieve this, the on-site physicians were deemed to be the best system analysts. This full-function PACS was initiated three years ago, and has achieved a relatively mature state in providing hospital-wide service. Because this system was developed and implemented by the PCH physicians, its maintenance and upgrade capabilities are much stronger than any commercially-developed PACS software. With regular feedbacks from the users (the clinicians, nurses, and technologist), modifications can be made quickly and easily. For the Puli Christian Hospital, this PACS not only saved considerable expense compared with purchasing commercial software, it has also provided the following contributions and
benefits to PCH:
z Instead of manually handling medical results, this PACS provides systematic access to the patient’s information on a hospital-wide basis. This has sped up the administrative process and medical treatments considerably.
z Medical information, examination results, and treatment histories have been stored electronically, thereby greatly reducing required physical storage space while increasing the capability of data preservation.
z Integration of the original Healthcare Information System (HIS) and the Radiology Information System (RIS) has increased hospital administrative efficiency; management abilities have improved enormously while reducing operation costs.
z This easily manipulated system has helped physicians/clinicians to make more accurate diagnosis, resulting in enhanced medical service. The ability to show medical results though the PACS has also earned the trust of patients.
z Simplification of the referral process for patients to transfer in or out of the hospital. Sharing the medical resources has also facilitated network treatments.
z The majority of PACS systems in Taiwan are commercially-developed products. In stark contrast, in developing this customized system, considerable valuable experience has been gained through designing the system analysis, software architecture design, debug process, system maintenance and developing updates, … etc. It is strongly believed these experiences can be used to
showcase and promote further hospital software development in Taiwan.
References
[1] U.S. Project of the National Health Information Infrastructure. http://aspe.hhs.gov/sp/NHII/
[2] Homepage of National Health Service of the Great Britian. http://www.nhs.uk/
[3] Homepage of Health of Canada. http://www.hc-
sc.gc.ca/hcs-sss/ehealth-esante/ehr-dse/biblio_can_e.html
[4] Homepage of Department of Health, Executive Yuan, Taiwan, ROC. http://www.doh.gov.tw/cht/index.aspx [5] Technical Report, National Science Council (NSC), Taiwan, ROC. http://www.nsc.gov.tw/pub/yearbook/ yearbook93/main/4/4-2.htm
[6] Fu-Zhong Wang, “The Study of National Health Information Infrastructure in Taiwan.”, Technical Report, Bureau of National Health Insurance, Taiwan, R.O.C., Dec, 2005.
[7] Cheng-Hua Lee, “Health Care and Medical Insurance: The National Health Information Infrastructure.”, Technical Report, Bureau of National Health Insurance, Taiwan, R.O.C., Sep 20, 2003. [8] Steckel RJ, “The Current Application of PACS to Radiology Practice.”, Radiology 1994; vol. 190(3), pp 50A-52A.
[9] Friedenberg RM, “PACS in the Clinical Setting: Revisited.”, Radiology 1994; Vol 190(3): 53A-54A. [10] Davide Caramella, “Is PACS Research and Development Still Necessary?” International Congress Series 1281, 2005, pp. 11-14.
[11] Tain-Chen Wu, San-Kan Lee, Chen-Hsing Peng, Chia-Hsien Wen and Shu-Kun Huang, “An Economical, Personal Computer-based Picture Archiving and Communication System”, RadioGraphics, 1999, Vol. 19(2) , pp 523-530.
[12] I-Chiu Chang, Hsin-Ginn Hwang, David C. Yen, J.W. Lian, “Critical Factors for Adopting PACS in Taiwan: Views of Radiology Department Directors”, Journal of Decision Support System.
[13] Mervyn D. Cohen, MB, ChB, MD, Lori L. Rumreich, MBA, Kimberley M. Garriot, S. Gregory Jennings, MD “Planning for PACS: A Comprehensive Guide to Non-technical Considerations.”, Journal of the
American College of Radiology, April 2005, Vol. 2 No. 4, pp 327-337.
[14] William J. Schroeder, Kenneth M. Martin, and William E. Lorenson. “The Design and Implementation of an Object-Oriented Toolkit for 3D Graphics and Visualization”. In IEEE Visualization, pp. 93-100, 1996.
[15] vtk homepage, http://www.vtk.org/ [16] itk homepage, http://www.itk.org/