國立臺灣大學公共衛生學院職業醫學與工業衛生研究所 碩士論文
Graduate Institute of Occupational Medicine and Industrial Hygiene College of Public Health
National Taiwan University Master Thesis
從文獻回顧探究職業傷病監測系統的低報與選擇性偏誤 Under-reporting and Selection Bias in Occupational Injury and
Illness Surveillance System, A Literature review
陳秉暉 Ping Hui Chen
指導教授:陳保中 博士
Advisor: Pau-Chung Chen, MD. Ph.D.
誌謝
在職衛所的這段時間,能順利完成這篇論文,實在有太多要感謝的人。
最感謝的是指導老師保中老師,作為在職衛所比較少見的質性研究,很感謝 保中老師一路上放手讓我自己在這個題目上探索,又能在有疑問時隨時和老師討 論、向老師請教,能擁有研究上的自由摸索空間,又能同時得到老師寶貴的經驗 與提點,學生真的是獲得了太多;感謝生殖危害實驗室的學長姐和同學夥伴們,
謝謝亮瑜學長的牽線,讓我有機會負責這個研究計畫,也才有機會接觸這個重要 的議題,謝謝靜君學姊在研究計畫上的種種幫忙,讓我在計劃期間可以專心處裡 研究的內容,沒有後顧之憂;感謝所有對這篇論文給過寶貴意見的專家學者,無 論是當初研究計畫進行時參與專家會議的國內專家學者,或是去 ICOH 口頭報告 時給予寶貴意見的國外專家學者,這些建議都擴展了我褊狹的視野,也充實了這 篇論文的內容;最後,也感謝職衛所的師長和同學們,一路上對於這篇論文的討 論和建議,很珍惜也很感謝那些寶貴的交流,和那難得的緣分。;最後,感謝勞 動部勞動及職業安全衛生研究所 ILOSH105-A302 號研究「職業災害通報及職業傷 病鑑定制度研究」對我研究上的啟發與支持。
感謝台大醫院環職部的師長與同仁的支持與包容,謝謝當初一起協助這個計 畫的亮瑜學長、維安學長、志阜學長、鈺潔和昆暉,謝謝你們在工作之餘努力抽 空協助這個計畫的進行,讓我能更全面且快速地掌握這九個國家的狀況,也謝謝 科部師長一路上的包容與配合,讓我能在工作的同時,順利完成研究所的課程與 這篇論文。
最後感謝總是在我身邊給予支持的,我親愛的家人和親愛的瑋菁,謝謝你們 願意包容工作狂的我,當我把自己的時間都投注在研究和工作上時,除了肯認我 的目標和價值外,也不吝於在旁邊給予我最大的支持與鼓勵,對於你們,我總是 付出的太少,卻得到了太多。
謝謝所有一路上給予我各種協助的人,是因為有你們才有這篇論文的產出,
我也會繼續努力堅持到底,希望能聊以回報你們給予我的協助。
中文摘要
研究背景:職業傷病的低報與伴隨而來的選擇性偏誤,始終是一個艱難的挑 戰,許多國家都因此使用各種通報機制從不同資料來源取得可信的資料。雖然過 去的研究曾經討論個別通報機制的運作、通報機制的分類或職業傷病的低報來 源,但沒有已知的研究曾經系統性地討論不同種類通報機制中職業傷病的低報來 源,以及這些通報機制如何交互作用並共同建構一個理想的職業傷病監測系統。
研究方法:包含臺灣、日本、韓國、新加坡、澳洲、美國、英國、德國和法 國的九個國家被選為研究對象,根據可搜尋到的網路資料,我們將這幾個國家運 作中的通報機制辨識出來,之後將這些通報機制進行分類,並根據 Webb 所提出的 濾篩模型(Filter model),將這些通報機制拆解為五種濾篩,後續的討論就著重在這 五種濾篩如何在各種通報機制中導致職業傷病的低報與選擇性偏誤,以及這九個 國家如何克服這些濾篩。
結果與討論:我們辨識出 17 個通報機制,包含 7 個補償為基礎的通報機制、
6 個職業安全法為基礎的通報機制與 4 個醫療行為為基礎的通報機制,且超過半數 的國家,9 個國家中有 6 個,有超過兩種以上的通報機制。
在各種通報機制中,這五種濾篩有不同的濾篩效果,且各國都有許多可以解 決低報的有效手段,並有職業傷病統計資料跨國或跨年的比較可以驗證其效果。
尤其那些職業傷病發生率較高、可合理解釋為較少低報問題的歐洲國家,他們克 服低報問題並得到精確統計資料的方法,無疑十分值得學習,特別是對於職業傷 病發生率最低的亞洲國家來說。
結論:共有三種通報機制,包含補償為基礎、職業安全法為基礎和醫療行為 為基礎的通報制度,且各種機制都有其自身的濾篩,與因能涵蓋不同職業傷病而 在職業傷病監測系統中不可取代的腳色。對於主管機關來說,要建構一個理想的
ABSTRACT
Introduction: Under-reporting of occupational injury and illness(OII) and accompanied selection bias have always been a difficult challenge, and each country has come up with various reporting mechanisms to obtain reliable data from different sources. Although operation of individual reporting mechanism, categorization of reporting mechanisms and sources of under-reporting have been discussed by previous studies, no searchable study has systematically discussed sources of under-reporting in different types of reporting mechanisms and how these reporting mechanisms interact and all together construct an ideal OII surveillance system.
Methods: Nine countries, including Taiwan, Japan, Korea, Singapore, Australia, the United States(US), the United Kingdom(UK), Germany, and France, were chosen as study targets. Based on searchable online information, we identified all active reporting mechanisms among these countries. We then carried out categorization of reporting mechanism and broke it down into five types of filters, according to modified filter model of Webb et al. Discussion is then focused on how these five types of filters lead to under-reporting and accompanied selection bias in each type of reporting mechanism and how these nine countries overcome them.
Results: 17 reporting mechanisms, including 7 compensation-based reporting mechanisms (CBRM), 6 OSH-Act-based reporting mechanism (OBRM), and 4 medical-practice-based reporting mechanisms (MBRM), are identified, and over half countries, six of nine, have more than two types of reporting mechanism.
Five types of filters have different filtering effects in each type of reporting mechanism, and there are many effective practices to overcome under-reporting, supported by temporal or international comparison of yearly statistics on OII.
While European countries have much higher incidence rate of OII, which is more reasonably explained by less under-reporting, how do they get accurate statistics and overcome under-reporting is worth learning, especially for Eastern Asian countries with lowest incidence.
Conclusions: There are three types of reporting mechanism, CBRM, OBRM, and MBRM, and each has its own filters and irreplaceable role in OII surveillance system due to different coverage of OII. For authorities concerned, to construct an ideal surveillance system, establishing other well-functioned complementary reporting mechanisms is as important as enhancing permeability of each reporting mechanism’s filters. For researchers, it is important to get familiar with OII coverage of certain reporting mechanism before utilization of its reported statistics, and pooling data from more than one reporting mechanisms may be necessary for a more comprehensive picture.
Keywords Occupational injury and illness, Surveillance, Reporting
CONTENTS
口試委員會審定書 ... #
誌謝 ...i
中文摘要 ... ii
ABSTRACT ... iii
CONTENTS ... v
LIST OF FIGURES ...vi
LIST OF TABLES ... vii
Chapter 1 Introduction ... 1
Chapter 2 Methods ... 2
2.1 Study targets and Literature review ... 2
2.2 Filter model to under-reporting of reporting mechanism ... 2
2.3 Filters in each type of reporting mechanism ... 3
Chapter 3 Results and Discussion ... 4
3.1 Identified reporting mechanisms and yearly statistics ... 4
3.2 Compensation-based reporting mechanism(CBRM) ... 4
3.3 OSH-Act-based reporting mechanism(OBRM) ... 11
3.4 Medical-practice-based reporting mechanism(MBRM) ... 13
3.5 Design of two-way reporting ... 16
3.6 Limitations ... 17
Chapter 4 Conclusions ... 18
Chapter 5 Tables and Figures ... 19
REFERENCE ... 27
LIST OF FIGURES
Figure 5-1. Cases of Compensated/Reported Occupational Injury per Million and Proportion of Death in Compensated/Reported Injury in Eight Countries in 2016.………24
Figure 5-2. The coverage of compensation insurance of OII in six countries from 2005 to 2016……….………25
LIST OF TABLES
Table 5-1. List of 17 Identified Active Reporting Mechanisms in Nine countries.…….18 Table 5-2. Cases of Compensated/Reported Occupational Illness per Million in Nine Countries by Disease Category in 2015……….. ………..….21 Table 5-3 The unshared employer responsibility for compensation of OII during temporary disability in six countries………...………23
Chapter 1 Introduction
Under-reporting of occupational injury and illness(OII) and accompanied selection bias have always been a difficult challenge for policy making and epidemiological studies in many countries, and each country has come up with various reporting mechanisms to obtain reliable data from different sources.
Many studies have reviewed operation and performance of reporting mechanisms, including multiple reporting mechanisms in European countries 1 2, single new-developing reporting mechanism, like RNV3P in France 3, THOR in the United Kingdom 4, NODIS in In Taiwan 5, single OII surveillance system in one country, like Singapore 6 and Korea 7 8, and worldwide reporting mechanisms suitable for reporting of new-emerging occupational illness 9. To discuss these reporting mechanism more precisely, categorization of reporting mechanism has also been adopted by many studies
2 9.
Only few studies have systematically reviewed sources of under-reporting, especially limited to reporting of occupational injury 10 or the United States 11 12, and no searchable study has systematically discussed sources of under-reporting in different types of reporting mechanisms and how these reporting mechanisms interact and all together construct an ideal OII surveillance system.
Chapter 2 Methods
2.1 Study targets and Literature review
Nine countries, including Taiwan, Japan, Korea, Singapore, Australia, the United States(US), the United Kingdom(UK), Germany, and France, were chosen as study targets. Based on searchable online information, including statutory laws, official webpages, government documents and journal articles, we identified all active reporting mechanisms among these countries with its qualitative reporting process and quantitative reporting performance.
2.2 Filter model to under-reporting of reporting mechanism
Filter model was first proposed by Webb et al in 1989 to systematically discuss sources of under-reporting in reporting occupational injuries, and then adopted by other studies to compare different OII data sources in US 13, explain under-reporting of Hispanic construction workers’ injuries 14, and discuss under-reporting of injury of occupational light-vehicle user 15, alcohol-related accidents and injuries 16 17, sharp injury of healthcare workers 18, and OII in US 12. The concept of filter model has also been introduced by National Institute for Occupational Safety and Health (NIOSH) as a method to discuss validity and reliability of injury statistics in their Guide to Evaluating the Effectiveness of Strategies for Preventing Work Injuries 1920.
To examine the process of each reporting mechanism and its association with under-reporting, we adopted and modified Filter model of Webb et al. to break these reporting mechanisms down into a series of filters 10 12, including awareness of reporting initiator, effective coverage of reporting mechanism, characteristics of reportable OII,
reporting incentive / disincentive, and determination of work-relatedness. Reporting initiators must pass all the filters in path to complete reporting, and these filters are thus obstacles causing under-reporting and focus of our study.
2.3 Filters in each type of reporting mechanism
According to types of reporting initiators and their incentive, reporting mechanisms were categorized into three types, including OSH-Act-based reporting mechanism (OBRM), compensation-based reporting mechanism (CBRM), and medical-practice-based reporting mechanism (MBRM). We then discussed how these five types of filters lead to under-reporting and accompanied selection bias in each type of reporting mechanism and how these nine countries overcome them, along with temporal or international comparison of yearly statistics on OII as a supportive evidence.
Although these filers may have similar filtering effect on occupational injury and occupational illness, however, because the definition of occupational injury’s work-relatedness is relatively clear-cut and needs little awareness or further determination, “awareness of reporting initiator” and “determination of work-relatedness” have little filtering effect and thus not discussed in reporting occupational injury.
Chapter 3 Results and Discussion
3.1 Identified reporting mechanisms and yearly statistics
Among these nine countries, 17 reporting mechanisms, including 7 CBRMs, 6 OBRMs, and 4 MBRMs, are identified, and over half countries, six of nine, have more than two types of reporting mechanism. Two countries, UK and Taiwan, have all three types of reporting mechanisms. All 17 reporting mechanisms are listed in Table 5-1.
Except for the number of compensated occupational injury of Japan’s CBRM is available only in 2012 and 2015, yearly statistics on OII are available for all 17 reporting mechanisms. Because there is little difference between different years’
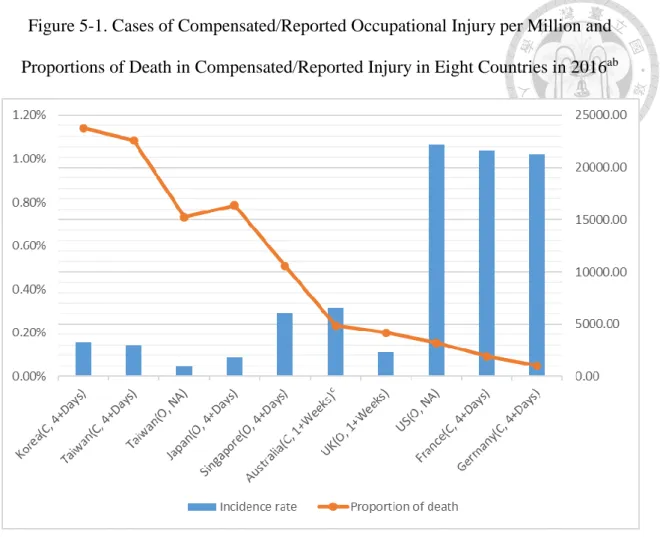
statistics on OII, year 2016 and 2015 were chosen as representative for international comparison of occupational injury and occupational illness, respectively. The numbers of compensated or reported occupational injury and illness per million in 2016 and 2015 are shown in Figure 5-1 and Table 5-2. Number of cases varies greatly between different countries, which is less likely to be merely explained by different industrial characteristics. Under-reporting is a much more reasonable explanation, especially in Eastern Asian countries with lowest incidence.
3.2 Compensation-based reporting mechanism(CBRM)
Seven countries (Taiwan, Japan, Korea, Australia, Germany, France, and UK) adopt CBRM. In CBRM, the major reporting initiator is workers, who voluntarily report to CBRM for claiming insurance benefits. Employers in France and Germany and physicians in Germany are also required to report all compensable occupational injury and listed compensable occupational illness, respectively, to their compensation
insurances. In UK, CBRM is more like allowance than social insurance and applies to all workers suffering from occupational illness with long-term disability.
There are five filters in CBRM.
1. Awareness of reporting initiator
For occupational illness, without awareness of the possibility of work-relatedness, workers as reporting initiator, would not try to claim benefits from compensation insurance 1. The awareness of workers may come from occupational safety and health education, which could only be enhanced by providing on-job education or raising social campaign. In 2007, Germany launched a campaign focusing on skin diseases, which had a huge social impact and successfully raised the awareness of workers about occupational skin diseases, and the notified case of suspected occupational skin diseases went from 15543 in 2006 to 18348 in 2007, while the number of compensated occupational skin diseases remained unchanged 1.
2. Effective coverage of reporting mechanism
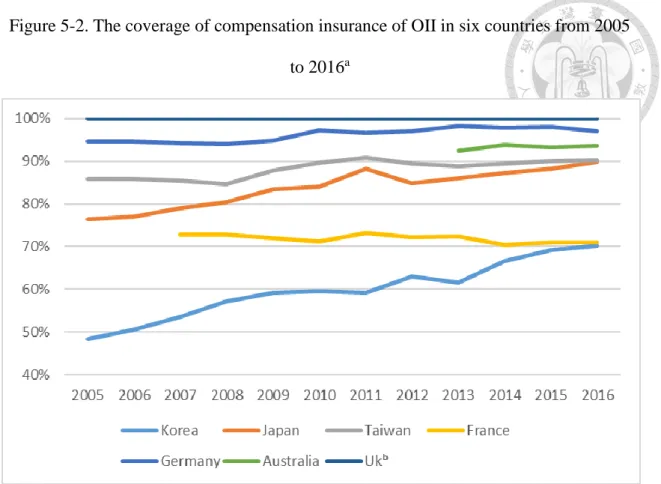
As shown in Figure 5-2, CBRMs in these seven countries have covered over half of employed persons. UK and Germany has the highest coverage rates (all workers/100% and over 97%), Taiwan, Japan, and Australia have acceptable coverage rates (around 90%), while France and Korea have poor coverage rates (around 70%). In contrast to relatively stable coverage rate in UK, France, Germany, and Australia, insurance coverage in Taiwan, Japan, and Korea has gradually expanded since 2005, especially in Korea, whose coverage rate went from 59.24% in 2011 to 70.26% in 2016.
covers employed person from specific industry, like agriculture or public sectors, and atypical employed person, like self-employee, dispatch worker, or contract worker.
These workers may be insured by other individual compensation insurance or totally not insured. Good practices like system integration (Germany merging BGs and UKs in 2007) 22 or data integration (Safe Work Australia collecting insurance data from each state) 23 of different compensation insurances, and voluntary participation in compensation insurance (Korea, Taiwan and Japan) are possible solutions to expand effective coverage of compensation insurance.
3. Characteristics of reportable OII
Compensation insurances in four countries (Taiwan, Japan, Korea, and Germany) require 4 or more days of incapability to claim benefits, while 1 or more days in France and 1 or more weeks in Australia.
According to statistic from France’s CBRM in 2015 and UK’s OBRM in 2012 and 2013, cases of occupational injury with 1 to 3 days and 4 to 6 days of incapability account for around 10% and 25% of total cases, which is a convenient way to evaluate filtering effect of 4 days and 7 days of incapability.4 days of incapability (losing only 10% cases), rather than 7 days of incapability (losing 35% cases), is a better balance between reporting burden and loss of cases.
Furthermore, considering difference in working days between part-time and full-time workers, it is much harder for part-time workers to fulfil the same incapability threshold. For example, 4 days of incapability actually means 4 weeks of incapability for part-time workers who work only one day per week. Thus, to avoid extra under-reporting and selection bias, it is necessary to adjust incapability threshold for part-time workers. In Australia, the threshold is adjusted proportionally to working day for part-time workers 24. If part-time workers only work one day per week, one day of
incapability would be viewed as one week, which is reportable and compensable in Australia’s CBRM.
For occupational illness, incapability threshold may have more complicated filtering effect than the above situation. Workers with certain kinds of occupational illness, like hearing loss and skin diseases, are usually still capable of working, and workers suffering from these diseases could hardly claim benefits from compensation insurance. In contrast, some occupational illness, like respiratory disease, usually leads to severe incapability, and more likely to be reportable and compensable 1. As shown in Table 5-2, in most countries, numbers of compensated occupational skin diseases and hearing loss are much lower than reported ones in MBRM, while numbers of compensated occupational respiratory diseases are much higher.
However, in Germany, workers with occupational skin diseases could still claim additional insurance benefits for individual prevention, medical rehabilitation and health education, and most workers with occupational hearing loss could claim pension benefits for permanent disability 1. Thus, numbers of compensated occupational hearing loss and skin diseases in Germany are much higher than other countries.
4. Reporting incentive / disincentive
Workers often encounter economic loss due to medical expense and incapability to work, and have to claim insurance benefits to maintain their daily life, especially for economically disadvantaged workers 12, which makes CBRM an effective reporting mechanism. If the economic loss could be covered by other funding, like National
injury and occupational illness, from 15251 and 603 per million in 2008 to 16850 and 691 per million in 2009, for enterprises with less than 5 workers.
However, once workers file a claim, employers may also encounter direct (unshared employer responsibility for OII compensation) or indirect economic loss (elevated insurance premium, labor inspection, and further civil lawsuit) 12. These pressure, coming from employers, is an noteworthy disincentive for workers to claim benefits 26, especially in Eastern Asian countries, where workers are less unionized and empowered 12.
For cases of permanent disability or death, faced with serious incapability and burdensome economic loss, workers’ incentive to claim benefits is usually strong enough, regardless of how much pressure employers may put on them. However, for cases of temporary disability, consisting of most compensated OII, whether to claim benefits may be impeded by pressure from employers 7. Thus, pressure from employers, especially direct economic loss employers have to bear immediately, is an important consideration for workers to claim benefits or not.
As showed in Table 5-3, compensation insurances in most countries (Japan, Korea, Australia, Germany, and France) almost share all the compensation responsibility during temporary disability, except for partial wage replacement during first 3 days to first 6 weeks 25 27-31. However, compensation insurance in Taiwan apparently fails to share employers’ responsibility. Employers in Taiwan have to bear 30-50% wage at least for two years, which would definitely become a huge disincentive for workers to claim benefits and account for under-reporting in Taiwan’s CBRM.
Due to the above difference in reporting incentive between OII of different severity, proportion of death in compensated injury could reflect filtering effect of “reporting incentive / disincentive”, though the proportion may be affected by other factors, like
industrial characteristics causing more death than minor injury. As shown in Figure 5-1, the proportion is much higher in Eastern Asian countries, like Taiwan and Korea (around 1.00%) than in other countries, like Australia (around 0.25%), Germany, and France (around 0.10%).
In Taiwan, due to relative poor payment from National Health Insurance, physicians also have incentive to claim medical expense from compensation insurance.
Some medical facilities systematically identify cases of occupational injury by asking simple screening questions in department like emergency medicine or orthopaedics, and become another important reporting initiator, yet only for occupational injury whose work-relatedness is much more clear-cut.
5. Determination of work-relatedness
In CBRM, workers encounter great difficulties in proving work-relatedness, which requires rigorous exposure assessment and solid epidemiologic evidences. There must be a group of specialists, usually occupational specialists, whose profession is causal relationship between occupation and illness, helping workers prepare necessary documents to claim benefits from compensation insurance.
In US, several occupational health clinical centres provide diagnosis and treatment of occupational disease, and a network of clinical centres even get funded by compensation insurance to help recognize cases of occupational illness systematically 26
32. In Taiwan, Ministry of Labor also funds the establishment of Network of Occupational Diseases and Injuries Service, and thus 81 hospitals have department of
2008 to 87.07 in 2015.
For occupational specialists, occupational exposure is indispensable in evaluating work-relatedness, yet specialists usually have to take great efforts to obtain reliable information via history taking, workplace visiting or environmental measurements, especially without full co-operation from employers 1. On one hand, obligatory workplace monitoring and local epidemiological studies focusing on high-risk workplace could provide some information in advance 1 8 33; on the other hand, all countries also have a prescribed list of occupational illness, to spare efforts in determination of work-relatedness. Workers with listed diagnosis and associated occupational exposure are generally viewed as cases of occupational illness, and the listed diagnosis is far more likely to be recognized than the unlisted one 1. Thus, how many diseases is included in one country’s prescribed list is an important filter, even in countries where unlisted diagnosis could be recognized case by case. According to the statistic from Germany’s CBRM, cases of compensated occupational skin diseases went from 646 in 2014 to 2151 in 2015, which could be explained by inclusion of UV-radiation-related occupational skin cancer into prescribed list of occupational illness in 2015.
Furthermore, France also set well-defined recognition criteria for the listed diseases, and workers fulfilling these criteria would even be automatically recognized as occupational illness by compensation insurance, especially for musculoskeletal diseases
1. Similarly, to facilitate early treatment and intervention, Australia also waives off some strict recognition process in evaluating work-relatedness of musculoskeletal diseases.
Additionally, Korea also set well-defined recognition criteria for occupational vascular diseases, to facilitate recognition of Karoshi 21. As shown in Table 5-2, this may explain why France and Australia have most compensated musculoskeletal diseases and Korea
has far more compensated vascular diseases than Japan and Taiwan.
3.3 OSH-Act-based reporting mechanism(OBRM)
Six countries (Taiwan, Japan, Singapore, Australia, US and UK) adopt OBRM. In OBRM, the major reporting initiator is employers, who obligatorily report to OBRM for fulfilling statutory reporting duty.
Among these six countries, most countries mandate employers to report only occupational injury, yet employers in Japan and US are still required to report all reportable OII in OBRM. However, employers’ poor incentive to fulfil reporting duty and inability to identify work-relatedness of workers’ illness both lead to under-reporting of occupational illness 11. In Japan, number of reported occupational illness in OBRM is only half of the number in CBRM. In US, OBRM adopts sampling and estimation to compromise employers’ weak incentive by relieving their reporting burden, yet only gross incidence of four types of illness, including skin diseases, respiratory diseases, chemical agents, and hearing loss, could be obtained 34. Considering these limitations, UK concludes that OBRM is not suitable for surveillance of occupational illness, and revised its OSH Act and largely narrowed down employers’
reporting duty in 2012. Meanwhile, they sought alternative data source and replaced OBRM with MBRM 35. Thus, the following discussion would be focused on OBRM in reporting occupational injury.
In OBRM, employers have to report occupational injury in a short time, and
OBRM in these two countries more like sampling and estimation, rather than counting every cases.
There are three filters in OBRM, and filtering effect of “effective coverage of reporting mechanism” and “characteristics of reportable OII” is quiet similar to CBRM.
Generally, effective coverage of OSH Act is slightly larger than compensation insurance, and only special workplace, like army (Singapore and Australia), household worker (Japan), and offshore worker (Australia) are excluded. Incapability thresholds in different countries’ OBRM also range from 1 or more days (Taiwan and US), to 4 or more days (Japan and Singapore), to 7 or more days (UK).
As for “reporting incentive / disincentive”, compared with employees actively reporting their OII for claiming benefits in CBRM, employers passively report employee’s OII for fulfilling reporting duties, only if breach of reporting duty would be uncovered by labor inspection or supervision from unionized workers and leads to serious punishment. Thus, employers’ poor reporting incentive leads to serious under-reporting in OBRM, especially minor injury which is less inspected. For example, Eurostat has concluded that insurance based systems (namely CBRM) have higher reporting level than systems based on the legal obligation of the employer to notify the accidents (namely OBRM) due to poor reporting incentive 36. Based on Eurostat’s metadata on accidents at work, compared with estimated reporting level of 100% in Germany and almost 100% in France except some industries, estimated reporting level of UK’s OBRM is only 47%, and minor injuries are especially under-reported 37. As shown in Figure 5-1, proportion of death in reported injury also reflects filtering effect of “reporting incentive / disincentive” in OBRM, and the proportion is much higher in UK (around 0.20%) than in France (0.09%) and Germany (0.05%).
In addition, electronic system has been adopted to reduce reporting burden.
Singapore’s iReport, encompassing all reporting mechanism for all kinds of reporting initiators in a user-friendly one-stop system, is a good example. Cases reported via iReport had rapidly increased from 50% of total cases in 2006 to 90% in 2009. Right now, iReport is the sole reporting channel, which has greatly reduced reporting burden.
Similar electronic system has also been adopted by many countries (Taiwan, UK, Germany, and France) in various types of reporting mechanisms 1 6 9 38 39.
3.4 Medical-practice-based reporting mechanism(MBRM)
Four countries (Taiwan, Singapore, France and UK) adopt MBRM. The major reporting initiator is physicians, who may voluntarily or obligatorily report their patients’ occupational illness for fulfilling statutory reporting duty(Singapore) 6 40 3933, fulfilling administrative reporting duty(Taiwan), or seeking information feedback for clinical decision-making (France and UK) 3. There are three filters in MBRM.
1. Awareness of reporting initiator
Similar to workers’ awareness in CBRM, the awareness of physicians also plays an important role in MBRM 33 1. One meta-analysis in 2016 found moderate-quality evidence that a reminder message of legal obligation, rather than reporting bonus, could significantly encourage physician reporting (RR: 1.32, 1.05-1.66) 41. Another intervention study in 2008 shows that educational programme could enhance physicians’ incentive to report occupational illness 42.
work-relatedness sometimes becomes part of medical practice, like recognition of occupational illness for claiming benefits or filing civil lawsuits, seeking medical advices on prevention and control of occupational illness, and taking statutory health examination for special occupational exposure. When motivated or required to report occupational illness, physician may report these handy cases39 40 43.
In France, general physicians can consult occupational specialists in university hospital to make clinical decisions, which becomes reported cases in MBRM at the same time 3. The reasons for consultation in 2012 and 2013 included occupational diagnosis (around 50% of total consultation), opinion on fitness for work, career guidance or reclassification (around 20%), occupational diseases monitoring (12%). In UK, to eradicate causative agents or risk factors, including occupational aetiologies, specialists are interested in information about work-relatedness between exposure and diseases, like material and asthma/dermatitis, movement and musculoskeletal diseases, or event and mental diseases, provided by database of UK’s MBRM 44. Different from traditional incentive, these information feedbacks further encourage physician reporting by helping their clinical decision-making, which is itself a part of medical practice.
However, in UK, even with information feedback, there is still a sign of reporter fatigue 12. Core reporters, who must report all the reportable occupational illness in the whole year, tend to report fewer cases than sample reporters, who just report in one month, and the reported cases also become fewer over years of participation 4 9. To compromise physicians’ weak incentive, UK’s MBRM adopts sampling and estimation to reduce reporting burden. Although the problem of under-reporting may be corrected by precise estimation, however, only gross incidence of four types of diseases, including skin diseases, respiratory diseases, musculoskeletal diseases, and mental diseases, could be obtained through sampling and estimation 45, which is much less informative than
counting every cases.
Although MBRM does not exclude any workers, how many physicians are motivated to report actually determines MBRM’s effective coverage 46. Considering limited number of occupational specialists and patients they visit, cooperation between different specialties is necessary in MBRM. In UK’s MBRM, occupational specialists reported 404 cases of skin diseases and 158 cases of respiratory diseases in 2010, while dermatologists reported 1789 cases of skin diseases and chest physicians reported 1811 cases of respiratory diseases. Thus, inclusion of physicians other than occupational specialists, via direct participation of other specialists (UK), referral (Singapore), or consultation (France), may be an important element to expand effective coverage of MBRM.
3. Determination of work-relatedness
The major strength of MBRM is relatively flexible scheme for determination of work-relatedness. Contrary to CBRM, whose determination of work-relatedness is closely related to compensation responsibility and insurance requirement, specialists in MBRM can freely report all the suspected cases without filters mentioned in CBRM 4.
As shown in Table 5-2, compared with CBRM, more cases of hearing loss, skin diseases, and mental diseases are reported in MBRM without the filtering effect of
“characteristics of reportable OII” and “determination of work-relatedness”, and less cases of respiratory diseases and musculoskeletal disease, which is often compensated in CBRM, is reported in MBRM. As a complementary reporting mechanism to CBPM 4,
largely limited and could hardly cover non-compensable cases, and highly overlapping between MBRM and CBRM becomes unnecessary reporting burden and brings little benefit.
3.5 Design of two-way reporting
For occupational injury, three countries (Japan, Germany and France) adopt design of two-way reporting, which means that CBRM and OBRM share similar filters and covering similar group of occupational injury. By adopting two-way reporting, in one hand, the authorities concerned could use data from CBRM to check whether employers comply with OSH Act and overcome employers’ poor reporting incentive; in the other hand, real-time data from OBRM could permit timely intervention and further pick up under-reported cases in CBRM. For example, the numbers of compensated/reported occupational injury in Japan are 119131/119576 and 116743/117910 in 2012 and 2015, proving that two-way reporting could overcome filters in both reporting mechanisms 38.
The design of two-way reporting is also adopted by the surveillance of occupational illness in Germany. CBRM in Germany also mandates physicians to report suspected cases of occupational illness, bringing features of MBRM. Physicians could not only fulfil his/her statutory obligation but also get reporting bonus per case reported.
In fact, most compensated cases are reported by physicians, followed by social organization (20%), workers (10%), and employers (3%) 1. The design of two-way reporting has both strengths of CBRM and MBRM. While workers still have strong incentive to claim benefits, physicians could still report relatively freely according to their own professional judgement 38.
3.6 Limitations
Although filter model of Webb et al. has been adopted and introduced by NIOSH and many other previous studies as methods to analyse and discuss sources of under-reporting, most study targets of these studies is injuries rather than illness 13-20, and only one study’s study target include occupational illness 12. Thus, some special filters, like stigma of occupational illness, may not be included in our modified filter model.
Besides, other databases, like occupational health examination database, death registry, and cancer registry, could also become important OII reporting mechanisms.
However, reported cases in these databases usually fail to meet the definition of occupational injury or illness, for example, abnormal health examination only stands for suboptimal health rather than illness, and lack of solid evaluation of work-relatedness in death/cancer registry, and thus not included in our study targets.
Finally, although we already include all the searchable online literature to identify and characterize all the active OII reporting mechanisms in these nine countries, language barrier and lack of other literature source may still be important limitations of our study.
Chapter 4 Conclusions
There are three types of reporting mechanism, CBRM, OBRM, and MBRM.
CBRM is the major reporting mechanism in most countries 38. However, the purpose of our study is not the comparison of generosity of compensation insurance. OBRM and MBRM, as complementary reporting mechanism, are also important data source. In fact, most countries adopt more than one type of reporting mechanism, and even in countries without reporting mechanism other than CBRM, like Germany, there are still features of OBRM or MBRM by adopting two-way reporting. Due to different filtering effects, each type of reporting mechanism covers different OII and has its own irreplaceable role in OII surveillance system.
For authorities concerned, to construct an ideal surveillance system, establishing other well-functioned complementary reporting mechanisms, which is the strategy adopted by UK 39, is as important as enhancing permeability of each reporting mechanism’s filters.
Researchers must bear in mind that each reporting mechanism has its own filters and accompanied selection bias. It is important to get familiar with OII coverage of certain reporting mechanism before utilization of reported statistics, and pooling data from more than one reporting mechanisms may be necessary for a more comprehensive picture of OII.
Chapter 5 Tables and Figures
Table 5-1. List of 17 Identified Active Reporting Mechanisms in Nine countries
Name Country Type Official websites and Data-releasing websites
Labor Insurance (勞工保險) Taiwan CBRM https://www.bli.gov.tw/
https://www.osha.gov.tw/1106/1164/1165/1168/
Occupational Injury (職業災害統計網 路填報系統)
Taiwan OBRM http://injury.osha.gov.tw/inj1005.aspx
https://www.osha.gov.tw/1106/1164/1165/1168/
Network of Occupational Diseases and Injuries Service (NODIS)
Taiwan MBRM https://tmsc.osha.gov.tw/
Industrial Accident Compensation Insurance (労働者災害補償保険)
Japan CBRM https://www.mhlw.go.jp/stf/seisakunitsuite/buny a/koyou_roudou/roudoukijun/hoken/980916_1.h tml
https://www.mhlw.go.jp/stf/seisakunitsuite/buny a/koyou_roudou/roudoukijun/gyoumu_00531.ht ml
Fatal Accidents Reports (死亡災害報 告), Workers’ Accidents Reports (労 働者死傷病報告), Reports of Occupational diseases (業務上疾病
Japan OBRM https://www.mhlw.go.jp/stf/seisakunitsuite/buny a/koyou_roudou/roudoukijun/anzen/toukei.html https://www.jisha.or.jp/english/statistics/index.ht ml
Work accident reporting – Employer / Workplace occupier (iReport)
Singapore OBRM https://www.mom.gov.sg/workplace-safety-and- health/work-accident-reporting
http://stats.mom.gov.sg/Pages/Workplace-Safety -and-Health-Tables2017.aspx
Work accident reporting - Treating doctor (iReport)
Singapore MBRM https://www.mom.gov.sg/workplace-safety-and- health/work-accident-reporting
http://stats.mom.gov.sg/Pages/Workplace-Safety -and-Health-Tables2017.aspx
Australian Workers’ Compensation Statistics
Australia CBRM https://www.safeworkaustralia.gov.au/collection /australian-workers-compensation-statistics Notifiable fatalities monthly report Australia OBRM https://www.safeworkaustralia.gov.au/collection
/notifiable-fatalities-monthly-report Injuries, Illnesses, and Fatalities (IIF) US OBRM https://www.bls.gov/iif/
The Health Insurance - Occupational Risks (L'Assurance Maladie – Risques professionnels)
France CBRM http://www.risquesprofessionnels.ameli.fr/accuei l.html
The National Occupational illness surveillance and Prevention Network (RNV3P)
France MBRM https://www.anses.fr/en/content/rnv3p-national- network-monitoring-and-prevention-occupationa l-diseases
German Social Accident Insurance (DGUV))
Germany CBRM https://www.dguv.de/de/index.jsp
Industrial Injuries Disablement Benefit (IIDB)
UK CBRM https://www.gov.uk/industrial-injuries-disablem ent-benefit
http://www.hse.gov.uk/statistics/tables/#iidb
Reporting of Injuries, Diseases and Dangerous Occurrences (RIDDOR)
UK OBRM http://www.hse.gov.uk/riddor/index.htm http://www.hse.gov.uk/statistics/tables/#iidb The Health and Occupation Research
Network (THOR)
UK MBRM http://research.bmh.manchester.ac.uk/epidemiol ogy/COEH/research/thor/
http://www.hse.gov.uk/statistics/tables/#iidb
Table 5-2. Cases of Compensated/Reported Occupational Illness per Million in Nine Countries by Disease Category in 2015ab
Chem ical Agent s
Musculo -Skeletal Diseases
Phys ical Age nts
Hearing Loss
Infecti ous Disea ses
Respira tory Disease s
Skin Disease s
Vascu lar Disea ses
Mental Diseases
Total (others included)
Taiwan(C) 0.71 50.19 0.00 0.18 0.36 12.50 0.63 7.41 0.27 87.07 Taiwan(M) 2.68 54.47 1.61 115.56 0.27 8.31 10.45 1.70 0.54 200.21 Japan(C) 1.51 20.75 6.29 4.56 2.92 20.64 0.25 3.94 7.40 68.54
Japan(O) 3.92 6.57
10.7 9
0.11 3.15 3.94 NA 1.14 0.89 31.82
Korea(C) 1.97 128.39 7.56 14.34 2.97 43.53 0.69 24.44 2.43 232.73
Singapore(M) 0.93 141.53 11.6
4
231.84 NA 2.33 41.43 NA NA 435.29
Germany(C) 14.90 29.72 1.04 154.58 24.10 134.54 53.49 NA NA 417.85 Germany(C+) 15.24 33.45 1.04 154.58 24.10 134.54 547.85 NA NA 923.85 France(C) 17.60 1672.84 6.55 30.24 6.77 157.74 10.94 NA NA 1928.55 France(M)c NA 68.54 NA NA 1.76 44.12 26.61 5.03 81.23 367.28 Australia(C) 44.54 1456.57 NA 12.30 24.60 17.81 36.48 8.06 520.02 2363.00
UK(C) NA 36.87
20.3 6
3.21 NA 142.34 1.44 NA NA 205.49
UK(M)d NA 9260.00 NA NA NA 640.00 560.00 NA 5020.00 16330.00
US(O)d 16.80 NA NA 131.02 NA 115.56 190.14 NA NA 417.85
a. The abbreviations used are: C, compensation-based reporting mechanism (CBRM); C+,
compensation-based reporting mechanism with additional insurance benefit for individual prevention, medical rehabilitation and health education; M, medical-practice-based reporting mechanism
(MBRM); O, OSH-Act-based reporting mechanism (OBRM)
b. The number of compensated/reported occupational illness comes from yearly statistics on OII of each reporting mechanism. The detailed data-releasing websites are listed in Table 5-1. The number of employed persons comes from labour statistics of ILO. Due to inconsistent disease categorization in the released data, there may be minor misclassification between disease categories
c. Due to data limitation, the number in each disease category is approximated by multiplying total number of confirmed cases with disease distribution of suspected cases
d. MBRM in UK and OBRM in US rely on sampling and estimation, rather than counting all the cases
Table 5-3. The unshared employer responsibility for compensation of OII during temporary disability in six countries 25 27-31
Duration of Temporary Disability
Employer responsibility in labor law
Insurance
benefit for
temporal disability
Unshared employer responsibility
Taiwan
First 3 days 100% Wage NA 100% Wage
1st Year 100% Wage 70% Wage 30% Wage
2nd Year 100% Wage 50% Wage 50% Wage
Japan
First 3 days 60% Wage NA 60% Wage
1.5 Years 60% Wage 80% Wage 0%
Korea
First 3 days 60% Wage NA 60% Wage
2 Years 60% Wage 70% Wage 0%
Australia
First 1-2 weeks
1/2 100% Wage NA 100%
1/2 NA 100% Wage 0%
2nd Year NA 75-80% Wage 0%
France
First 28 days NA 60% Wage 0%
MMI NA 80% Wage 0%
Germany
First 6 weeks 100% Wage 80% Wage 20% Wage
1.5 Years or MMI NA 80% Wage 0%
Figure 5-1. Cases of Compensated/Reported Occupational Injury per Million and Proportions of Death in Compensated/Reported Injury in Eight Countries in 2016ab
a. The abbreviations used are: C, compensation-based reporting mechanism (CBRM); M,
medical-practice-based reporting mechanism (MBRM); O, OSH-Act-based reporting mechanism (OBRM); 4+ Days/1+Weeks, 4+ Days/1+Weeks incapability threshold; NA, incapability threshold not defined as days
b. The number of compensated/reported occupational injury comes from yearly statistics on OII of each reporting mechanism. The detailed data-releasing websites are listed in Table 5-1. The number of employed persons comes from labour statistics of ILO. Statistics on occupational injury from Japan’s CBRM is only available in 2012 and 2015.
c. OBRM in Australia is limited to reporting of occupational fatalities
Figure 5-2. The coverage of compensation insurance of OII in six countries from 2005 to 2016a
a. The number of insured persons comes from yearly statistics on OII of each reporting mechanism. The detailed data-releasing websites are listed in Table 5-1. The number of employed persons comes from labour statistics of ILO
b. CBRM in UK is more like allowance and applies to all workers
REFERENCE
1. EUROGIP. Reporting of Occupational Diseases Issues and Good Practices in Five European Countries. Eurogip 2015;102/E
2. Carder M, Bensefa-Colas L, Mattioli S, et al. A review of occupational disease surveillance systems in Modernet countries. Occup Med (Lond)
2015;65(8):615-25. doi: 10.1093/occmed/kqv081 [published Online First:
2015/10/09]
3. Bonneterre V, Faisandier L, Bicout D, et al. Programmed health surveillance and detection of emerging diseases in occupational health: contribution of the French national occupational disease surveillance and prevention network (RNV3P).
Occup Environ Med 2010;67(3):178-86. doi: 10.1136/oem.2008.044610
4. Carder M, Hussey L, Money A, et al. The Health and Occupation Research Network:
An Evolving Surveillance System. Saf Health Work 2017;8(3):231-36. doi:
10.1016/j.shaw.2016.12.003
5. Chu PC, Fuh HR, Luo JC, et al. The impact of occupational health service network and reporting system in Taiwan. Int J Occup Environ Health 2013;19(4):352-62.
doi: 10.1179/2049396713Y.0000000043
6. Siang LH, Tan A. Singapore’s Framework for Reporting Occupational Accidents, Injuries and Diseases. Asian-Pacific newslett on Occup Health and Safety 2010;17:28-31.
7. Kim EA, Kang S-K. Reporting System for Occupational Injuries and Illness in Korea.
Asian-Pacific newslett on Occup Health and Safety 2010;17:32-34.
8. Rhee KY, Choe SW. Management system of occupational diseases in Korea: statistics, report and monitoring system. J Korean Med Sci 2010;25(Suppl):S119-26. doi:
10.3346/jkms.2010.25.S.S119
9. Bakusic J, Lenderink A, Lambreghts C, et al. Methodologies to identify work-related diseases Review of sentinel and alert approaches. In: (EU-OSHA) EAfSaHaW, ed., 2017.
10. Webb GR, Redman S, Wilkinson C, et al. Filtering effects in reporting work injuries.
Accident Analysis & Prevention 1989;21(2):115-23. [published Online First:
1989/04/01]
11. Miller G. Hidden Tragedy: Underreporting of Workplace Injuries and Illness. In: The Committee on Education and Labor USHoR, ed., 2008.
12. Azaroff LS, Levenstein C, Wegman DH. Occupational Injury and Illness
Surveillance Conceptual Filters Explain Underreporting. American Journal of Public Health 2002;92(9):1421-29. [published Online First: 2002/08/29]
13. Murphy PL, Sorock GS, Courtney TK, et al. Injury and illness in the American workplace: a comparison of data sources. American journal of industrial medicine 1996;30(2):130-41. doi:
16. Webb GR. A filter model to describe bias in official statistics on alcohol-related injuries. Accident; analysis and prevention 1995;27(5):687-97. [published Online First: 1995/10/01]
17. Rehm J. Methodological approaches and problems in research into alcohol-related accidents and injuries. Addiction (Abingdon, England) 1993;88(7):885-96.
[published Online First: 1993/07/01]
18. Mahmood NHN, Hamzah NF. Factors influencing sharp injury reporting among healthcare workers in Hospital Melaka. Journal of Advanced Research Design 2017;34(1):8-18.
19. Robson LS, Shannon HS, Goldenhar LM, et al. Guide to Evaluating the
Effectiveness of Strategies for Preventing Work Injuries. In: Health NIfOSa, ed., 2001.
20. Moller J, Scott I. Guide to Evaluating the Effectiveness of Strategies for Preventing Work Injuries: How to show whether an intervention really works. Injury Prevention 2003;9(4):382-83. doi: 10.1136/ip.9.4.382-a
21. Kwon SC, Kim HR, Kwon YJ. The administrative process for recognition and compensation for occupational diseases in Korea. J Korean Med Sci 2014;29 Suppl:S3-11. doi: 10.3346/jkms.2014.29.S.S3
22. DGUV. DGUV Statistics 2016, 2017.
23. National Data Set for Compensation-based Statistics In: Commission NOHaS, ed., 2004.
24. Technical Manual for the National Data Set Compensation-Based Statistics. In:
Commission ASaC, ed., 2008.
25. Kim JG, Duk YJ. Development and Operation of Workers’ Compensation Insurance Scheme in S. Korea. In: Workers’ Compensation Research Center KWCWSC, ed., 2012.
26. Markowitz S. Occupational disease surveillance and reporting systems. In: Stellman JM, ed. Encyclopaedia of Occupational Health and Safety: International Labour Organization (ILO), 1998.
27. Comparison of workers’ compensation arrangements in Australia and New Zealand (2018). In: Australia SW, ed., 2018.
28. Your social security rights in France. In: Commission E, ed., 2013.
29. Your social security rights in Germany. In: Commission E, ed., 2011.
30. EUROGIP. Accidents at work and occupational diseases: flat rate or full reparation?
European survey on the conditions of compensation for the victims. Eurogip 2005;21/E
31. Industrial Accident Compensation Insurance Application Guidance for Foreign Workers. In: Compensation Division LSB, Ministry of Health Labour and Welfare, ed., 2018.
32. Welch L. The role of occupational health clinics in surveillance of occupational disease. American Journal of Public Health 1989;79 Suppl:58-60. [published Online First: 1989/12/01]
33. Improving Workplace Health Management in Singapore. In: Council WSaH, ed., 2018.
34. Survey of Occupational Injuries and Illness. In: Statistics BoL, ed., 2017.
35. Waclawski E. Disease reporting after the Reporting of Injuries, Diseases, and Dangerous Occurrence Regulations (1995) (RIDDOR) is revised. Occup Med (Lond) 2013;63(3):168-9. doi: 10.1093/occmed/kqs220
36. EUROSTAT. European Statistics on Accidents at Work(ESAW): Summary
methodology. In: Commission E, ed., 2013.
37. EUROSTAT. European Statistics on Accidents at Work(ESAW): Metadata. In:
Commission E, ed., 2016.
38. Ehnes H. Improvement of national reporting, data collection and analysis of
occupational accidents and diseases. In: International Labour Organization G, ed., 2012.
39. Choy K, Tan A, Soon LC, et al. Reporting of Occupational Diseases in Singapore.
The Singapore Family Physician 2011;37(25-30)
40. Choy K, Far HS. Workplace Safety and Health Guidelines Diagnosis and Management of Occupational Diseases. In: Council WSaH, ed., 2011.
41. Curti S, Sauni R, Spreeuwers D, et al. Interventions to increase the reporting of occupational diseases by physicians: a Cochrane systematic review. Occup Environ Med 2016;73(5):353-4. doi: 10.1136/oemed-2015-103209
42. Smits PB, de Boer AG, Kuijer PP, et al. The effectiveness of an educational programme on occupational disease reporting. Occup Med (Lond) 2008;58(5):373-5. doi: 10.1093/occmed/kqn061
43. Koh D, Chia K-S. Surveillance in developing countries. In: Stellman JM, ed.
Encyclopaedia of Occupational Health and Safety: International Labour Organization (ILO), 1998.
44. Money A, Carder M, Hussey L, et al. The utility of information collected by occupational disease surveillance systems. Occup Med (Lond)
2015;65(8):626-31. doi: 10.1093/occmed/kqv138
45. Hussey L. THOR-GP input to HSE Annual Statistics 2015/2016 - Note on methods used for calculating incidence rates and ‘caveats’ in interpretation. In: Centre for Occupational & Environmental Health (COEH) T, Manchester Uo, eds., 2016.
46. Delaunay M, Godard V, Le Barbier M, et al. Geographic dimensions of a health network dedicated to occupational and work related diseases. Int J Health Geogr 2016;15(1):34. doi: 10.1186/s12942-016-0063-7 [published Online First:
2016/09/30]