Effects of glutamine-containing total parenteral nutrition on phagocytic activity and anabolic hormone response in rats undergoing gastrectomy
Running title: Effect of glutamine in rats with gastrectomy
Chen-Hsien Lee, Wan-Chun Chiu, Soul-Chin Chen, Chih-Hsiung Wu, Sung-Ling Yeh
Chen-Hsien Lee, Wan-Chun Chiu, Sung-Ling Yeh, Institute of Nutrition and Health Sciences, Taipei Medical University, Taipei, Taiwan
Soul-Chin Chen, Chih-Hsiung Wu, Department of Surgery, Taipei Medical University Hospital, Taipei, Taiwan
Supported by research grant from the National Science Council, Taipei, Taiwan, No.
91-2815-C-038-007-B
Correspondence to: Sung-Ling Yeh, PhD, Institute of Nutrition and Health Sciences, Taipei Medical University
250 Wu-Hsing Street, Taipei, Taiwan 110. [email protected] Telephone: +88-62-27361661 ext. 6551-115 Fax: +88-62-27373112 Received: 2004-03-16 Accepted: 2004-05-13
Abstract
AIM: To investigate the effect of glutamine (Gln)-containing parenteral nutrition on phagocytic activity and to elucidate the possible roles of Gln in the secretion of anabolic hormones and nitrogen balance in rats undergoing a gastrectomy.
METHODS: Rats with an internal jugular catheter were divided into 2 experimental groups and received total parenteral nutrition (TPN). The TPN solutions were isonitrogenous and identical in nutrient compositions except for differences in amino acid content. One group received conventional TPN (control), and in the other group, 25% of the total amino acid nitrogen was replaced with Gln. After receiving TPN for 3 d, one-third of the rats in each experimental group were sacrificed as the baseline group. The remaining rats underwent a partial gastrectomy and were sacrificed 1 and 3 d, respectively, after surgery. Plasma, peritoneal lavage fluid (PLF), and urine samples were collected for further analysis.
RESULTS: The Gln group had lower nitrogen losses 1 and 2 d after surgery (d1, 16.6242.5 vs -233.4205.9 mg/d, d2, 31.8238.8 vs -253.4184.6 mg/d, P<0.05).
There were no differences in plasma growth hormone (GH) and insulin-like growth factor-1 levels between the 2 groups before or after surgery. The phagocytic activity of peritoneal macrophages, was higher in the Gln group than in the control group 1 d after surgery (OD 1185931 vs 323201, P<0.05). There were no differences in the phagocytic activities of blood polymorphonuclear neutrophils between the 2 groups at the baseline or on the postoperative days. No significant differences in interleukin-1 or interleukin-6 concentrations in PLF were observed between the 2 groups. However, tumor necrosis factor- level in PLF was significantly lower in the Gln group than in the control group on postoperative day 3.
CONCLUSIONS: TPN supplemented with Gln can improve the nitrogen balance, and enhance macrophage phagocytic activity at the site of injury. However, Gln
supplementation has no effect on phagocytic cell activity in the systemic circulation, GH and insulin-like growth factor-1 might not be responsible for attenuating nitrogen losses in rats with a partial gastrectomy.
Chen-Hsien Lee, Wan-Chun Chiu, Soul-Chin Chen, Chih-Hsiung Wu, Sung-Ling Yeh. Effects of glutamine-containing total parenteral nutrition on phagocytic activity and anabolic hormone response in rats undergoing gastrectomy.
World J Gastroenterol 2004;
INTRODUCTION
Surgeries of the upper gastrointestinal tract usually produce a moderate degree of metabolic stress. Altered protein metabolism characterized by a negative nitrogen balance and changes in plasma free amino acid pattern were often observed in surgical traumas[1,2]. For most gastrectomized patients with gastric diseases, preoperative protein-energy malnutrition was often present, and adequate oral intake after surgery was achieved late[3,4]. Artificial nutritional support is essential for these patients. Most surgeons use the parenteral route to administer nutrients before and after a gastrectomy. However, the optimal formulation of TPN for patients with gastrectomy is still unknown.
In recent years, glutamine (Gln) has elicited great attention for its therapeutic role in the treatment of diseases. Gln has traditionally been considered as a nonessential amino acid, but laboratory and clinical data suggest that it may become essential during certain catabolic conditions[5,6], because studies have shown that hypercatabolic states are associated with significantly depressed plasma Gln levels[7-9]. A number of studies have demonstrated the beneficial effects of supplying exogenous Gln in the diet for metabolic-stressed conditions. These effects include increasing
permeability, maintaining immunologic function, and reducing infections[5,6,10,11]. Parry-Billings et al[6]. demopnstrated that depressed Gln concentrations were associated with depressed phagocytosis by peritoneal macrophages in normal mice.
Ogle et al [12].also reported that Gln improved the bactericidal ability of abnormal neutrophils from pediatric patients after burns. Furukawa et al[13].revealed that supplemental Gln enhances phagocytosis by neutrophils from postoperative patients in vitro. Although Parry-Billings et al [6]. and Ogle et al [12]. suggested the efficacy of Gln supplementation, they did not supply Gln to their patients. The beneficial effect of Gln on phagocytosis in in vitro studies might not reflect in vivo situations. To our knowledge, no study has been carried out to date to investigate the effect of Gln supplementation on phagocytic activity after gastrectomy. Therefore, in this study, we infused Gln-containing parenteral nutrition before and after gastrectomy to investigate the effect of Gln on phagocytic activity at the site of injury and systemic circulation. Growth hormone (GH) is an anabolic hormone that can reduce whole- body nitrogen loss after surgery[14,15]. A study showed that low-dose Gln supplementation was also capable of elevating plasma GH[16]. We analyzed plasma GH and insulin-like growth factor (IGF)-1 to elucidate whether Gln supplementation could enhance the secretion of anabolic hormones thus attenuating the nitrogen losses after gastrectomy.
MATERIALS AND METHODS Animals
Male 7-week-old Wistar rats weighing 170 to 210 g at the beginning of the experiment were used. All rats were housed in temperature- and humidity-controlled rooms, and allowed free access to a standard rat chow for 7 d prior to the experiment.
The care of the animals followed the standard experimental animal care procedures.
This study was approved by the Taipei Medical University Animal Care Committee.
Study protocol and operation procedures
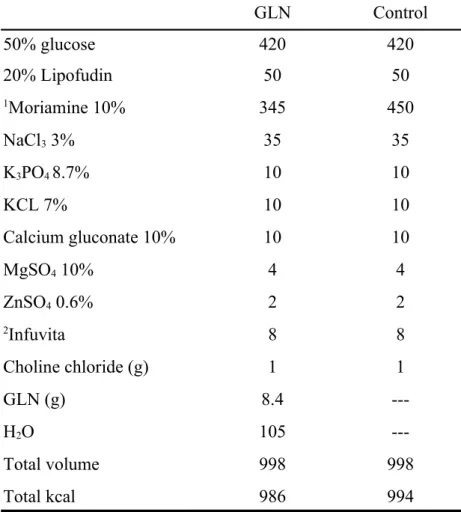
Rats were randomly assigned to 2 experimental groups, 30 rats in each group. The average weight between the groups was adjusted as similar as possible. After an overnight fasting, rats were anesthetized with intraperitoneal pentobarbital (50 mg/kg), and the right internal jugular vein was cannulated with a silastic catheter (Dow Corning, Midland, MI, USA) under sterile conditions. The catheter was tunneled subcutaneously to the back of neck and exited through a coil spring that was attached to a swivel, allowing free mobility of animals inside individual metabolic cages. All animals were allowed to drink water during the experimental period. TPN provided 270 kcal/kg body weight, this level of energy was slightly higher than weight maintenance for normal TPN rats[17]. The kcal/nitrogen ratio in the TPN solution was 145:1. The calorie density was almost 1 kcal/ml. The TPN solutions were isonitrogenous (6.84 mg/mL) and identical in nutrient compositions except for the difference in amino acid content. One group received conventional TPN (control), the other group replaced 25% of the total amino acid nitrogen as Gln. Although the amount of essential amino acids (EAA) was lower in the Gln group than in the control group, the EAA was adequate for maintenance according to the reported EAA requirements for rats[18]. The energy distribution of the TPN solutions in the experimental groups was 72% from glucose, 18% from protein, and 10% from fat (Table 1). Gln was dissolved and sterilized by passage through a 0.2-um Minisart NML filter (Sartorius, Goettingen, Germany) and stored at 4 oC until being used. Gln solution was stable at room temperature for at least 2 d as previously described[17]. The TPN solution was refilled daily and infused for 24 h at room temperature. Two
milliliters per hour was administered on the first day, and then the rats received 48-57 kcal/d according to their body weight. The infusion rate was maintained with a Terufusion pump (model STC-503, Terumo, Tokyo, Japan). The TPN solution without fat was prepared every other day in a laminar flow hood, and the fat emulsion was added daily just before use. After receiving TPN for 3 d, one-third of the rats (n
= 10) in each experimental group were sacrificed as the baseline group. The remaining rats underwent a partial gastrectomy on the 4th day of TPN, and were sacrificed 1 or 3 d, respectively, after surgery. Partial gastrectomy was performed using the same method as in our previous study[19]. TPN was maintained for 3, 5, or 7 days according to the sacrifice schedule of the rats.
Measurements and analytical procedure
Rats in the respective groups were sacrificed before or 1 or 3 d after surgery. The animals were anesthetized with intraperitoneal pentobarbital (50mg/kg BW). A middle abdominal incision was made, and 10 mL of phosphate-buffered saline (PBS) was intraperitoneally injected to elute the peritoneal cells. After the peritoneal lavage fluid (PLF) was harvested, rats were exsanguinated by drawing arterial blood from the aorta. Blood samples were collected in tubes containing heparin and immediately centrifuged. Plasma amino acids were analyzed by the standard ninhydrin technology (Beckman Instruments, model 6300, Palo Alto, CA, USA), after deproteinization of the plasma with 5% salicylic acid[20]. Plasma GH (Cayman Chemical, Ann Arbor, MI, USA) and insulin-like growth factor (IGF)-1 (Diagnostic Systems, Webster, TX, USA) were determined by using commercially available enzyme-linked immunosorbent assay (ELISA) kits. Interleukin (IL)-1, IL-6, and tumor necrosis factor (TNF)- levels in plasma and peritoneal lavage fluid (PLF) were measured using commercial ELISA microtiter plates, with antibodies specific for rat IL-1, IL-
6, and TNF- coated onto wells of the microtiter strips provided (Amersham Pharmacia Biotech, Buckinghamshire, UK).
Flow cytometric phagocytosis test was used to evaluate the phagocytic activity of blood polymorphonuclear neutrophils[21,22]. One hundred microliters of heparinized whole blood was aliquoted on the bottom of a 12mm x 75mm Falcon polystyrene tube (Becton Dickinson) and placed in an ice-water bath. Twenty microliters of precooled opsonized FITC-labeled E. coli (Molecular Probes, Eugene, OR, USA.) was added to each tube. Control tubes remained on ice, and assay samples were incubated for precisely 10 min at 37 ℃ in a shaking water bath. After incubation, samples were immediately placed in ice water, and 100 L of a precooled trypan blue (Sigma, St.
Louis, MO, USA) solution (0.25 mg/ml in citrate salt buffer pH 4.4) was added to quench the fluorescence of the bacteria merely adhering to the surface of
phagocytosing cells. Cells were washed twice in Hank’s buffered saline (HBSS), and erythrocytes were lysed by the addition of FACS lysing solution (Becton Dickinson).
After an additional wash in HBSS, 100 L of propidium iodide (PI) solution (1
g/mL in HBSS) was added to stain the nuclear DNA 10 min before the flow cytometric analysis. Flow cytometry was performed on a FACS CaliburTM flow cytometer (Becton Dickinson) equipped with a 488-nm argon laser. A live gate was set on the red (PI) fluorescence histogram during acquisition to include only those cells with a DNA content at least equal to human diploid cells. The number of cells with phagocytic activity did not exceed 6% at 0 oC.
A Vybrant TM phagocytosis assay kit (molecular probes) was used to evaluate the phagocytic activity of peritoneal macrophages. After the peritoneal macrophages was washed 3 times with HBSS, the cell concentration was counted, and the cell number was adjusted to 106 cells/mL with RPMI-1640 supplemented with 5% fetal bovine
serum and an adequate amount of antibiotics. After 100 l of diluted solutions was distributed into each well on 96-well microplates, it was transferred to a 37 ℃ CO2
incubator for 1 h to allow the cells to adhere to the microplate surface. The RPMI solution was removed from all microplate wells by vacuum aspiration, and then 100
l of the prepared FITC-labeled E. coli was added to each well for 2 h. Labeled bacteria were removed by vacuum aspiration, and 100 l of trypan blue suspension was added to all wells within 1 min. The excess trypan blue was immediately aspirated, and the experimental and control wells (without peritoneal macrophages) were read in the fluorescence plate reader using ~480 nm for excitation and ~520 nm for emission.
Twenty-four-hour urine specimens were collected during the 3 infusion days after surgery for determination of the nitrogen balance. Nonprotein nitrogen in urine was measured by a colorimetric method (Randox, Antrim, Ireland)
Statistical analysis
Data were expressed as mean ± SD. Differences among groups were analyzed by ANOVA using Duncan’s test. A p value less than 0.05 was considered statistically significant.
RESULTS
There were no differences in initial body weights between the 2 experimental groups at the beginning of TPN administration. All rats gained weight after TPN infusion, and weights were maintained postoperatively. No differences in body weights were seen between the 2 groups on postoperative days 1 and 3 (Figure 1). The Gln group had a higher plasma Gln level on postoperative day 1. No significant differences were observed before and 3 days after surgery (Figure 2).
Compared with the control group, the Gln group had less nitrogen loss 1 and 2 d
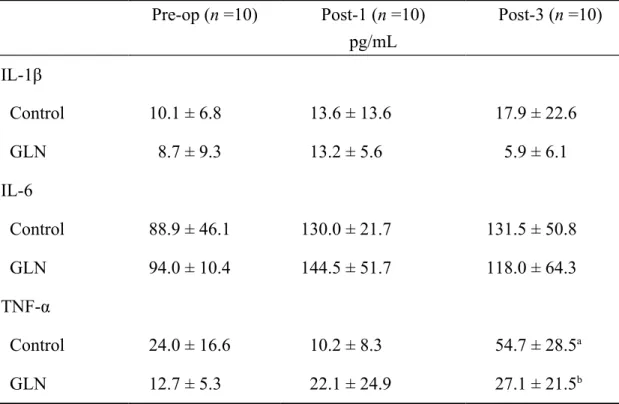
after surgery (Figure 3A). A significantly better cumulative nitrogen balance was observed in the Gln group on postoperative days (Figure 3B). Compared with the levels before surgery, plasma GH concentrations were significantly lower after surgery in the control group on both postoperative days 1 and 3, whereas there was only a difference on day 3 postoperatively in the GLN group. There were no differences in GH and IGF-1 levels between the 2 groups before or after surgery (Figure 4A, 4B). The phagocytic activity of peritoneal macrophages was higher in the Gln group than in the control group on postoperative day 1 (Figure 5A). The phagocytic activities of blood PMNs were significantly higher after surgery than the baseline, regardless of whether or not Gln was given. There were no significant differences in the phagocytic activities of blood PMNs between the 2 groups at various time points (Figure 5B). Plasma IL-1, IL-6, and TNF- levels were undetectable. No significant differences in concentrations of IL-1 and IL-6 in PLF were observed between the 2 groups at the time we took the measurements. However, TNF- levels in PLF were significantly lower in the Gln group than in the control group on postoperative day 3 (Table 2).
DISCUSSION
In this study, 25% of total nitrogen in the TPN solution was supplied by Gln. This amount of Gln was previously found to enhance the immune response in rodents [23,24]. We administered TPN before and after gastrectomy, to mimic the usual treatment for patients who were scheduled to undergo gastrectomy. These patients were frequently malnourished, and perioperative TPN was essential for adequate nutritional support.
Since human studies may have wide variations owing to the age of patients, severity of disease, infected area of the stomach, and complications of other diseases, which
may make interpretation difficult of the data. We used an animal model with a partial gastrectomy to investigate the effect of Gln on the catabolic and immune responses after abdominal surgery.
Injury to the body could result in a negative nitrogen balance together with a progressive loss of body protein[1,2], possibly resulting from hormonal changes and cytokine secretion[25,26]. Many studies have shown that Gln supplementation could enhance skeletal muscle synthesis which might consequently improve nitrogen balance after elective surgery[5,27,28]. GH is known to exert many metabolic effects.
Among them are nitrogen retention and preservation of muscle protein mass[14,15]. IGF-1 is one of the major effectors of GH action. The effects of GH are mediated in part by IGF-1 that is produced in the liver and locally in GH target tissues[29]. A study by Welbourne et al [16]. reported that oral Gln load was capable of elevating plasma GH in healthy adults. Hammarqvist et al [30]. demonstrated that GH together with Gln-containing TPN reduced nitrogen losses compared with Gln alone. The nitrogen retention data in the present study are in good agreement with those of previous reports[5,29,30]. However, we did not find an association between plasma GH, IGF-1 levels and Gln supplementation before or after operation. This finding suggests that GH and IGF-1 might not be responsible for attenuating nitrogen losses under the present experimental conditions.
Previous reports have shown that parenterally or enterally administered Gln lowered the incidence of infection in patients with bone marrow transplantation and multiple traumas[31,32]. Supplemental Gln improved the survival in experimentally Escherichia coli-induced peritonitis in rodents[33,34]. Nevertheless, the mechanisms underlying the enhancing effect of Gln on bactericidal capacity have not been fully elucidated. Gln is an important fuel for immune cells[6]. Macrophages could use Gln
at a very high rate[35]. Some in vitro studies have shown that Gln is required for macrophage phagocytosis[6,12 13,36]. In this study, we found that the phagocytic activity of peritoneal macrophages was much higher in the Gln group after surgery compared to the control group, whereas no differences were found in the phagocytic activities of blood PMNs between the 2 groups. These findings indicate that Gln supplementation can enhance the macrophage phagocytic activity at the site of injury. The effect of Gln on phagocytic cells in the systemic circulation was not obvious. In this study, we did not observe reduced plasma Gln levels after surgery. This result was consistent with the report by Parry-Billings et al [37] that plasma Gln levels did not change after minor surgery. It is possible that partial gastrectomy performed in this study resulted in a minor metabolic stress. The rats were free of infection or other stresses that would cause a systemic response. Therefore, a tissue or an organ specific nutrient like Gln exerts its effects locally but not systemically.
Cytokines are peptides produced by cells of the immune system that act as a mediator of the immune response and the response of tissues to injury. Studies have proposed that alterations in TNF- and IL-6 can be used as biochemical markers of the stress response[27,28,38]. IL-6 has been considered as the most consistently identified cytokine mediator of postinjury infections[39]. High plasma concentrations of IL-1 and TNF- were associated with increased severity of inflammatory diseases [39]. These cytokines in plasma were not detectable at the time we took measurements. However, cytokines in PLF were measurable. Compared with the baseline, IL-1, and IL-6 levels did not change after surgery. This result may indicate that postinjury infection was not obvious in this study. We observed that TNF- was lower in the Gln group than in the control group on postoperative day 3. This might mean that TPN with Gln could reduce the production of inflammatory mediators at the site of injury. An in
vitro study by Rohde et al [40] showed that Gln had no effect on the production of IL- 1, IL-6, or TNF-. Since it was an in vitro study, and samples used for evaluation were derived from healthy volunteers, response to the stressed metabolic conditions observed in this study might differ and consequently lead to different immune responses.
In summary, parenterally infused Gln can significantly enhance peritoneal macrophage phagocytic activity, and the nitrogen balance can be improved.
However, Gln supplementation has no effect on phagocytic cells in the systemic circulation, GH and IGF-1 might not be responsible for attenuating nitrogen losses in rats with a partial gastrectomy.
REFERENCES
1. Finley RJ, Inculet RI, Pace R, Holliday R, Rose C, Duff JH, Groves AC, Woolf LI. Major operation trauma increases peripheral amino acid release during the steady-state infusion of total parenteral nutrition in man. Surgery 1986; 99: 491- 499. [PMID: 3082029]
2. Tashiro T, Yamamori H, Takagi K, Morishima Y, Nakajima N. Increased contribution by myofibrillar protein to whole-body protein breakdown according to severity of surgical stress. Nutrition 1996; 12: 685-689. [PMID: 8936491]
3. Delany HM, Demetriou AA, Teh E, Levenson SM. Effect of early postoperative nutritional support on skin wound and colon anastomosis healing. J Parenter Enter Nutr 1990; 14: 357-361. [PMID: 2119442]
4. Bragelmann R, Armbrecht U, Rosemeyer D, Schneider B, Zilly W, Stockbrugger RW. Nutrient malassimilation following total gastrectomy. Scand J Gastroenterol
1996; 218: 26-33. [PMID: 8865447]
5. Willmore DW. The effects of glutamine supplementation in patients following elective surgery and accidental injury. J Nutr 2001; 131: 2543S-2549S. [PMID:
11533310]
6. Parry-Billings M, Evans J, Calder PC, Newsholme EA. Does glutamine contribute to immunosuppression after major burns? Lancet 1990; 336: 523-525.
[PMID: 1975037]
7. Hammarqvist F, Wernerman J, von der Decken A, Vinnars E. Alanyl-glutamine counteracts the depletion of free glutamine and the postoperative decline in protein synthesis in skeletal muscle. Ann Surg 1990; 212: 637-644. [PMID:
2122821]
8. Stehle P, Zander J, Mertes N, Albers S, Puchstein C, Lawin P, Furst P. Effect of parenteral glutamine peptide supplements on muscle glutamine loss and nitrogen balance after major surgery. Lancet 1989; i: 231-233. [PMID: 2563409]
9. Souba WW. Glutamine: a key substrate for the splanchnic bed. Annu Rev Nutr 1991; 11: 285-308. [PMID: 1892702]
10. van der Hulst RR, van Kreel BK, von Meyenfeldt MF, Brummer RJ, Arends JW, Deutz NE, Soeters PB. Glutamine and the preservation of gut integrity. Lancet 1993; 341: 1363-1365. [PMID: 8098788]
11. Ding LA, Li JS. Effects of glutamine on intestinal permeability and bacterial translocation in TPN-rats with endotoxemia. World J Gastroenterol 2003; 9:
1327-1332. [PMID: 12800250]
12. Ogle CK, Ogle JD, Mao JX, Simon J, Noel JG, Li BG, Alexander JW. Effect of
glutamine on phagocytosis and bacterial killing in normal and pediatric burn patient neutrophils. J Parenter Enter Nutr 1994; 18: 128-133. [PMID: 8201747]
13. Furukawa S, Saito H, Inoue T, Matsuda T, Fukatsu K, Han I, Ikeda S, Hidemura A. Supplemental glutamine augments phagocytosis and reactive oxygen intermediate production by neutrophils and monocytes from postoperative patients in vitro. Nutrition 2000; 16: 323-329. [PMID: 10793298]
14. Ponting GA, Halliday D, Teale JD, Sim AJ. Postoperative positive nitrogen balance with intravenous hyponutrition and growth hormone. Lancet 1988; i: 438- 440. PMID: 2893867
15. Jiang ZM, He GZ, Zhang SY, Wang XR, Yang NF, Zhu Y, Wilmore DW. Low dose growth hormone and hypocaloric nutrition attenuate the protein-caloric response after major operation. Ann Surg 1989; 210: 513-525. [PMID: 2802836]
16. Welbourne TC. Increased plasma bicarbonate and growth hormone after an oral glutamine load. Am J Clin Nutr 1995; 61: 1058-1061. [PMID: 7733028]
17. Yeh SL, Chen WJ, Huang PC. Effect of L-glutamine on hepatic lipids at different energy levels in rats receiving total parenteral nutrition. J Parenter Enter Nutr 1994; 18: 40-44. [PMID: 8164302]
18. National Research Council. Nutrient requirements of the laboratory rat. In Nutrient Requirements of Laboratory Animals, 3rd ed. National Academy of Sciences, Washington, DC, pp7-37, 1978
19. Lin MT, Yeh SL, Kuo ML, Liaw KY, Lee PH, Chang KJ, Chen WJ. Effects of medium-chain triglyceride in parenteral nutrition on rats undergoing gastrectomy.
Clin Nutr 2002; 21: 39-43. [PMID: 11884011]
20. Smith RJ, Panico K. Automated analysis of o-phthalaldehyde derivatives of amino acids in physiological fluids of reverse phase high performance liquid chromatography. J Liq Chromatogr 1985; 8: 1783-1795.
21. Böhmer RH, Trinkle LS, Staneck JL. Dose effects of LPS on neutrophils in a whole blood flow cytometric assay of phagocytosis and oxidative burst.
Cytometry 1992; 13: 525-531. [PMID: 1321708]
22. Schiffrin EJ, Rochat F, Aeschlimann JM, Donnet-Hughes A. Immunomodulation of human blood cells following ingestion of lactic acid bacteria. J Dairy Sci 1995;
78: 491-497. [PMID: 7782506]
23. Kew S, Wells SM, Yaqoob P, Wallace FA, Miles EA, Calder PC. Dietary glutamine enhances murine T-lymphocyte responsiveness. J Nutr 1999; 129:
1524-1531. [PMID: 10419985]
24. Wells SM, Kew S, Yaqoob P, Wallace FA, Calder PC. Dietary glutamine enhances cytokine production by murine macrophages. Nutrition 1999; 15: 881- 884. [PMID: 10575665]
25. Baigrie RJ, Lamont PM, Kwiatkowski D, Dallman MJ, Morris PJ. Systemic cytokine response after major surgery. Br J Surg 1992; 79: 757-760. [PMID:
1393463]
26. Fong Y, Moldawer LL, Shires GT, Lowry SF. The biological characteristics of cytokines and their implication in surgical injury. Surg Gynecol Obstect 1990;
170: 363-373. [PMID: 2108507]
27. Hammarqvist F, Wernerman J, Ali R, von der Decken A, Vinnars E. Addition of glutamine to total parenteral nutrition after elective abdominal surgery spares free
glutamine in muscle, counteracts the fall in muscle protein synthesis, and improves nitrogen balance. Ann Surg 1989; 209: 455-461. [PMID: 2494960]
28. Morlion BJ, Stehle P, Wachtler P, Siedhoff HP, Koller M, Konig W, Furst P, Puchstein C. Total parenteral nutrition with glutamine dipeptide after major abdominal surgery. Ann Surg 1998; 227: 302-3080. [PMID: 9488531]
29. Isgaard J, Nilsson A, Jansson OGP. Effects of local administration of GH and IGF-1 on longitudinal bone growth in rats. Am J Physiol 1986; 250: E367-E372.
[PMID: 3963179]
30. Hammarqvist F, Sangren A, Andersson K, Essen P, McNurlan MA, Garlick PJ, Wernerman J. Growth hormone together with glutamine-containing total parenteral nutrition maintains muscle glutamine levels and results in a less negative nitrogen balance after surgical trauma. Surgery 2001; 129: 576-586.
[PMID: 11331450]
31. Ziegler TR, Young LS, Benfell K, Scheltinga M, Horto SK, Bye R, Morrow FD, Jacob DO, Smith RJ. Clinical and metabolic efficacy of glutamine-supplemented parenteral nutrition after bone transplantation. A randomized, double-blind, controlled study. Ann Intern Med 1992; 116: 821-828. [PMID: 1567096]
32. Houdijk AP, Rijinsburger ER, Jansen J, Wesdorp RIC, Weiss JK, McCamish MA, Teerlink T, Meuwissen SGM, Haarman HJM, Thijs LG, van Leeuwen PAM.
Randomized trial of glutamine-enriched enteral nutrition on infectious morbidity in patients with multiple trauma. Lancet 1998; 352: 772-776. [PMID: 9737282]
33. Gianotti L, Alexander JW, Gennari R, Pyles T, Babcock GF. Oral glutamine decreases bacterial translocation and improves survival in experimental gut-origin sepsis. J Parenter Enter Nutr 1995; 19: 69-74. [PMID: 7658604]
34. Inoue Y, Grant JP, Snyder PJ. Effect of glutamine-supplemented intravenous nutrition on survival after Escherichia coli-induced peritonitis. J Parenter Enter Nutr 1993; 17: 41-46. [PMID: 8437323]
35. Newsholme P, Gordon S, Newsholme EA. Rates of utilization and fates of glucose, glutamine, pyruvate, fatty acids and ketone bodies by mouse macrophages. Biochem J 1987; 242: 631-636
36. Wallace C, Keast D. Glutamine and macrophage function. Metabolism 1992; 41:
1016-1020. [PMID: 1381459]
37. Parry-Billings M, Baigrie RJ, Lamont PM, Morris PJ, Newsholme EA. Effects of major and minor surgery on plasma glutamine and cytokine levels. Arch Surg 1992; 127: 1237-1240. [PMID: 1358047]
38. Biffl WL, Moore EE, Moore FA, Peterson VM. Interleukin-6 in the injured patient. Marker of injury or mediator of inflammation? Ann Surg 1996; 224: 647- 664. [PMID: 8916880]
39. Foex BA, Shelly MP: The cytokine response to critical illness. J Accid Emerg Med 1996; 13:154-162. [PMID: 8733647]
40. Rohde T, Maclean DA, Pedersen BK: Glutamine, lymphocyte proliferation and cytokine production. Scand J Immunol 1996; 44: 648-650. [PMID: 8972749]
FIGURE LEGENDS
Figure 1. Body weights of experimental groups at the beginning of TPN administration and before sacrifice.
Figure 2. Plasma glutamine (Gln) levels of the 2 groups before and after surgery.
*P<0.05 vs control group on post-1.
Figure 3. Nitrogen balance and cumulative nitrogen balance between the 2 groups after operation. *P<0.05 vs control group on post-operative days.
A: Nitrogen balance between the 2 groups after operation.
B: Cumulative nitrogen balance between the 2 groups after operation
Figure 4. Plasma growth hormone (GH) and insulin-like growth factor-I (IGF-I) concentrations between the 2 groups before and after operation. *P<0.05 vs the corresponding group on post-operative days.
A: Plasma growth hormone concentrations between the 2 groups before and after operation.
B: Plasma insulin-like growth factor-1 concentrations between the 2 groups before and after operation
Figure 5. phagocytic activity of peritoneal macrophages and peripheral blood neutrophils.
A: Phagocytic activity of peritoneal macrophages measured by phagocytosis assay and read in the fluorescence plate reader using 480 nm for excitation and 520 nm for emission. *P<0.05 vs control group on post-1.
B: Peripheral blood neutrophils measured by flow cytometry. †P<0.05 vs the corresponding groups on post-operative days.
Table 1. Formulation of the TPN solution
GLN Control
50% glucose 420 420
20% Lipofudin 50 50
1Moriamine 10% 345 450
NaCl3 3% 35 35
K3PO4 8.7% 10 10
KCL 7% 10 10
Calcium gluconate 10% 10 10
MgSO4 10% 4 4
ZnSO4 0.6% 2 2
2Infuvita 8 8
Choline chloride (g) 1 1
GLN (g) 8.4 ---
H2O 105 ---
Total volume 998 998
Total kcal 986 994
1From Chinese Pharmaceuticals, Taipei, Taiwan. Each deciliter contains: Leu 1250 mg, Ile 560 mg, Lys acetate 1240 mg, Met 350 mg, Phe 935 mg, Thr 650 mg, Trp 130 mg, Val 450 mg, Ala 620 mg, Arg 790 mg, Asp 380 mg, Cys 100 mg, Glu 650 mg, His 600 mg, Pro 330 mg, Ser 220 mg, Tyr 35 mg, and aminoacetic acid (Gly) 1570 mg.
2From Yu-Liang Pharmaceuticals, Taoyuan, Taiwan. Each milliliter contains: vitamin A 660 IU, ascorbic acid 20 mg, vitamin A 660 IU, ergocalciferol 40 IU, thiamine HCl 0.6 mg, riboflavin 0.72 mg, niacinamide 8 mg, pyridoxine HCl 0.8 mg, d-panthenol 3 mg, and dl-alpha-tocopheryl acetate 2 mg.
Table 2. Peritoneal lavage fluid (PLF) interleukin (IL)-1β and IL-6 tumor necrosis factor (TNF)-α concentrations between the 2 groups before and after operation (mean
± SD)
Pre-op (n =10) Post-1 (n =10) pg/mL
Post-3 (n =10)
IL-1β
Control 10.1 ± 6.8 13.6 ± 13.6 17.9 ± 22.6
GLN 8.7 ± 9.3 13.2 ± 5.6 5.9 ± 6.1
IL-6
Control 88.9 ± 46.1 130.0 ± 21.7 131.5 ± 50.8
GLN 94.0 ± 10.4 144.5 ± 51.7 118.0 ± 64.3
TNF-α
Control 24.0 ± 16.6 10.2 ± 8.3 54.7 ± 28.5a
GLN 12.7 ± 5.3 22.1 ± 24.9 27.1 ± 21.5b
a P<0.05 vs pre-op and post-1 groups in the same line
b P<0.05 vs control group on post-3
Fig 1
Before TPN Before sacrifice
Fig 2
*
A)
-500 -400 -300 -200 -100 0 100 200 300 400
post-1 post-2 post-3
Nitrogen (mg/d)
Control GLN
B)
Fig 3
* *
*
*
A)
0 50 100 150 200 250
pre-op post-1 post-3
GH (ng/mL)
Control GLN
B)
Fig 4
* *
A)
B)
Fig 5
*
† †