行政院國家科學委員會專題研究計畫 期中進度報告
(子計畫六)膀胱癌易罹癌基因之多發家族遺傳連鎖分析
(2/3)
計畫類別: 整合型計畫
計畫編號: NSC92-3112-B-038-002-
執行期間: 92 年 05 月 01 日至 93 年 04 月 30 日 執行單位: 臺北醫學大學公共衛生學系
計畫主持人: 邱弘毅
計畫參與人員: 陳建仁,薛玉梅,蒲永孝,沈正煌,王淵宏
報告類型: 完整報告
報告附件: 出席國際會議研究心得報告及發表論文 處理方式: 本計畫可公開查詢
中 華 民 國 93 年 3 月 12 日
基因體醫學國家型科技計畫
National Research Program for Genomic Medicine National Science Council, the Executive Yuan, ROC.
砷與移行細胞癌之毒理基因體研究─(子計畫六)
膀胱癌易罹癌基因之多發家族遺傳連鎖分析(2/3)
Linkage Analysis of Susceptibility Genes for Bladder Cancer in Multiplex Families (2/3)
報告類別:
□ 新進研究計畫 □ 修正後計畫書 ; 年度成果報告 (New Proposal) (Revised Proposal) (Progress Report) 計畫類別:□ 個別型計畫 ; 整合型計畫
(Individual Project) (Program Project) 計畫編號: 91GMP012-6
計畫主持人 (Principle Investigator):邱弘毅 ( Hung-Yi Chiou ) 執行單位 (Institution): 台北醫學大學公共衛生學系
( School of Public Health, Taipei Medical University )
中華民國 92 年 12 月 24 日
National Research Program for Genomic Medicine National Science Council, the Executive Yuan, ROC.
Progress Report—Research Project
基因體醫學國家型科技計畫
國科會延續性計畫進度報告
Program Classification:
; Genomic Medicine Bioinformatics
Proteomics & Structural Genomics ELSI Project Number
:91GMP012-6
(計畫編號)NSC Funding Number
NSC93-3112-B038-002
(93年度國科會預核編號)(in Chinese) 中文
膀胱癌易罹癌基因之多發家族遺傳連鎖分析
Title of Project 計畫名稱
(in English) 英文
Linkage Analysis of Susceptibility Genes for Bladder Cancer in Multiplex Families
(in Chinese) 中文
台北醫學大學 公共衛生學系
Institution
研究(執行)單位
(in English) 英文
School of Public Health, Taipei Medical University
(in Chinese) 中文
邱弘毅
Principle Investigator 計畫主持人
(in English) 英文
Hung-Yi Chiou
FY 2002 2003 2004 Total Budget
(in NT dollars: 1USD = 34 NTD) Signature of the PI:_______________Date:__12/24/2003____
Part B. Progress Report of
Component Projects
TABLE OF CONTENTS
Project Number
:91GMP012-6
Part B. Progress Report
B1. Response to previous reviewer’s critiques B2. Progress Report
Abstract (in Chinese and English) Background and Significance B2a. Specific Aims
B2b. Studies & Results B2c. Personnel
B2d. Projected Timeline B2e. Publications (Optional) B2f. Patents (Optional)
B3. Request for Modifications of the Project (Optional)
You do not have to finish this section except your budgets or items of requests are modified.
(請求經費或項目變動者才須加填此一部份,否則直接附上去年全程計畫書當附件 即可)
B3a. Background & Statement (including literature cited) B3b. Summary Budget Requested
B3c. Postdoctoral Fellows Requested B3d. Detailed Budget for Personnel
B3e. Detailed Budget Requested for Equipments B3f. Detailed Budget Requested for Travel to Overseas B3g. Detailed Budget Requested for Attending Conferences B3h. Detailed Budget Requested for Other Categories B3i. Use of Core Facilities Requested
B3j. Biographical Sketches of New Personnel
Progress Report
B1. Response to previous reviewers’ critiques
Please describe the previous reviewers’ critiques and how based on the critiques, you made modifications to specific aims, experimental design, or resource
allocation etc.
中文摘要
關鍵詞:移形上皮細胞癌、砷、家族聚集研究
無機砷是確認之人體肺癌與皮膚癌致癌物,包括台灣、美國、日本、阿根廷、智利及 芬蘭等國家,均有研究指出砷暴露與泌尿道癌症的產生具有統計顯著相關存在。我們最近 於台灣東北角的蘭陽盆地亦發現砷暴露與泌尿道癌,特別是移形上皮細胞癌(TCC)具 有明顯的劑量效應關係存在。不過,引起膀胱癌之主要易感受基因及其功能目前並不清 楚。因此本計畫的研究目的包括(1)透過癌症登記系統及各合作醫院確認的膀胱癌病例,
以家族疾病史問卷作電話或家戶訪視,以尋找膀胱癌多發家庭。(2)以問卷訪視蒐集指標
個案及其家庭成員之研究資訊並收集其血液、尿液等生物檢體。(3)分離、純化及分裝研
究對象 DNA 並儲存在超低溫冷凍庫以供各子計畫使用。(4)針對過去 CGH 及 LOH 研 究所獲得在染色體上與膀胱癌發生相關之 DNA 增加與缺失的部位,進行易感受基因多型
性分析。(5)針對砷引起與非砷引起之膀胱癌,利用多發家庭連鎖分析,對相關易感受性
基因進行定位。(6)分析可能的易感受基因與環境因子對膀胱癌發生危險性之交互作用。
(7)建立遺傳流行病學與生物統計支援中心,協助各子計畫進行資料分析工作。本研究 共分為兩個部分,第一部分預備以三年時間在台南、嘉義、宜蘭三縣各合作醫院收集 150 位多發性家族之膀胱癌指標個案,及每一指標個案的十位一等親成員,合計 1500 位多發 家庭成員。第二部分針對 150 個多發家庭(每一家庭除指標個案外,至少一名成員罹患膀 胱癌)以問卷蒐集環境暴露等危險因子及生活史資料,以判定為砷暴露及非砷暴露組。每 一位研究對象亦將蒐集 35c.c.血液及 50c.c.尿液,以獲得研究所需的 DNA,DNA 將被分 離、純化、儲存在超低溫冷凍庫中,以供各子計畫使用。本計畫亦將針對過去 CGH 及 LOH 研究所獲得在染色體上與膀胱癌發生相關之 DNA 增加與缺失的部位,進行易感受 基因定位之連鎖分析,比較砷引起及非砷引起膀胱癌的易感受基因的部位之異同,供日後 做預防與治療的基礎資料。
Abstract
Keywords: Transitional Cell Carcinoma; Inorganic arsenic; multiplex family study
Inorganic arsenic has been well documented as a human carcinogen of skin and lung. A significant association between arsenic exposure and risk of urinary cancer has also been reported in many epidemiological studies carried out in many countries of the world. Our recent study had also found a significant dose-response relationship between risk of cancers of urinary organs, especially for transitional cell carcinoma (TCC), and arsenic exposure through drinking well water in Lanyang Basin. However, the major susceptible gene(s) of bladder cancer from arseniasis-endemic and non-endemic areas and their functional changes that make a person to be a victim of arsenic-induced bladder cancer is still unclear. The objective of this subproject is to identify and differentiate the major susceptibility gene(s) for arsenic-induced and non-arsenic-induced bladder cancers through the linkage analysis of genetic markers in members of multiplex families. It will include following specific aims: 1) the ascertainment of multiplex families through the telephone or home-visit interview, based on a family history questionnaire, of bladder cancer cases reported to the national cancer registry and cases diagnosed and treated in collaborative medical centers; 2) the recruitment of probands and families members through home-visit personal questionnaire interview and biospecimen collection; 3) the purification, depository and inventory of DNA samples in central biospecimen bank; 4) the typing of genetic markers on chromosomes in which loss or gain have been observed through previous comparative genomic hybridization and loss of heterozygosity studies; 5) the mapping of susceptibility gene(s) through linkage analysis of multiplex family data for bladder cancer cases in arseniasis -endemic and non-endemic areas; 6) the examination of the effects of possible candidate genetic marker(s) and their synergistic interactions with environmental factors on bladder cancer; and 7) the establishment of Genetic Epidemiology and Biostatistics Supporting Core to provide methodological support to other subprojects. A total of 150 multiplex families of bladder cancer including 150 probands and 1500 first-degree relatives from arseniasis -endemic and non-endemic area will be recruited by the end of three year grant period. An informed consent will be obtained from each participant for the collection of risk factor information through questionnaire interview. A 35 mL blood and buccal cell specimen will be obtained from each consenting participant. DNA samples will be extracted from peripheral lymphocytes and buccal cells, aliquoted and frozen at -70℃. Polymorphisms of genetics markers closely linked to the major susceptible gene(s) of bladder cancer will be typed.
Analysis of Lod score, and transmission disequilibrium test will be carried out to map susceptible gene(s) of arsenic-induced and non-arsenic-induced bladder cancer based on multiplex family study.
Background and Significance
Our previous studies have shown that capability of arsenic methylation is associated with the risk of arsenic-induced skin cancer (12). Null genotypes of glutathione S-transferase (GST) M and T1 and variant genotype of GST P1 have been found to increase the risk of arsenic-induced skin cancer (13). Whether the genotypic and phenotypic polymorphisms of GSTs and other enzymes related to arsenic methylation may modify the risk of arsenic-induced TCC remain to be elucidated. Furthermore, genetic polymorphisms of some DNA repair enzymes have been observed to be associated with the risk of arsenic-induced skin cancer (14). It is also important to assess whether the DNA repair enzymes, either their genotypes or gene expression profiles, are related to the risk of arsenic-induced bladder cancer. The existence of genetic susceptibility to arsenic-induced bladder cancer may be explored through the microarray analysis of differential expression profiles and single nucleotide polymorphisms of related genes. It may also be investigated by the genetic epidemiological study on familial TCC through linkage analysis.
Tobacco smoke is another important etiological agent of urinary bladder cancer in Taiwan. It plays an important role in the induction of urinary bladder cancer in non-arseniasis-endemic areas. The tobacco-related bladder cancer risk is modified by the genetic polymorphisms of N-acetyltransferase 1 and 2 (15). The comparison of toxicological genomic characteristics of TCC induced by tobacco and arsenic may help the elucidation of the arsenic-induced carcinogenicity. This program project is organized to study the difference in toxicological genomic characteristics between TCC induced by arsenic and tobacco smoke.
Due to the lack of animal models for arsenic carcinogenicity, arsenic is a unique carcinogen in humans. Therefore, the high prevalence of urinary TCC in arseniasis-endemic area in Taiwan is a unique chance to investigate the carcinogenicity of arsenic. Since cancer development is mainly attributable to environmental factors and genes, it is of fundamental importance to understand the interaction between environment and genes. In this PPG, epidemiological components will establish the association of environmental factors and incidences of urinary TCC. Molecular, cellular and genetic components will identify the genetic factors involved in formation of urinary TCC. The joint efforts of epidemiological and molecular genetic studies will successfully dissect the interactions between environmental factors and genes. Novel findings of this PPG will allow us designing new strategy for prevention, diagnosis, and treatment of urinary TCC.
Though arsenic is a human carcinogen, there is no good animal model for the carcinogenicity of inorganic arsenic. Arsenic is inactive or extremely weak to induce gene mutations at specific loci (1,16). The modes of action for arsenic-induced carcinogenicity might include the induction of chromosome abnormality, inhibition of DNA repair, induction of oxidative stress, and increase of cell proliferation (17). Inorganic arsenic has several genotoxic effects including the induction of changes in chromosome structure and number, increases in sister chromatid exchanges and micronuclei, gene amplification, cell
transformation, aneuploidy, and chromosome-type chromosome aberration (1,17-22). The role of inorganic arsenic in the carcinogenesis has also been hypothesized as a co-carcinogen such as promoter or progressor rather than an initiator (23,24). However, the evidence is far from adequate to draw a definite conclusion on the exact mechanism of inorganic arsenic to induce various cancers in humans.
Most of the genetic variants which have been studied using the design of case-control study were only associated with a modest increased genetic risk for developing cancer, although the magnitude of their attributable risk is large because there are quite frequent in the population. Many rare cancer syndromes due to a mutated gene which confer very high risk of cancer have been well-documented, including the rare Li Fraumeni symdrom in which persons inhriting a gerlime mutation in the p53 gene are at almost 100 % risk of breast caner and other cancers by the age of 60 years (25,26), the familial adenomatous polyposis symdrome associated with mutation in the APC gene (27), and the breast-ovary cancer syndrome associated with an inherited mutation in BRCA1 (28).
Human genome sequence have been cloned successfully by “Human Genome Project”. A total of 3 x 105 of an estimated 3-10 x 106 single nucleotide polymorphisms which distinguish individuals and their disease traits and risk will be identified by 2002 (29).
Classical family, twin and adoptee studies have shown substantial heritabilities for many disease traits, but except in rare instances the pattern is polygenic rather than monogenic.
Knowledge and technology have become sufficient to enable molecular geneticists to study megaphenic disorders in single families, with the exceptation of isolating ‘the genes’
understanding the pathology and deriving clinically applicable test of status (30,31).
For polygenic traits, knowledge is sufficient to initiate tests of hypotheses, but the technology is yet insufficient to measure the contribution of genetic diversity to disease liabilities. Linkage analysis of multiplex family has an important role in genetic epidemiology because it identifies a biologic mechanism for transmission of a trait or disease (31). A large family displaying a clear-cut segregation pattern for a disease is examined at polymorphic sites representing each part of each chromosome (30). Recently, most sites of cancer has been recognized as multigene disorders. It means that many regions of each chromosome have been examined intensively to identify susceptible genes and then to differentia their functions on risk of various cancers. With a availability of a fairly complete human genome sequence, this approach is reducing to searching the sequence for the possible culprit gene on criteria such as its tissue expression pattern, apparent function predicted from sequence, etc. For example, haemochromatosis was shown by positional cloning to be attributable to an HLA-related genes and it has immediately been possible to examine the relationship between genetic and iron status diagnostics, population prevalence of mutations, and prevalence of HFE mutations in haemochromatosis-associated disease groups such as diabetics (32). In addition, given the widespread roles of iron, for various phenotypes and investigation of HFE interactions in other disorders such as porphyries, haemoglobinopathies and coronary disease and
environmental variables such as diet, lead poisoning and infections, is now proceeding to explore gene-environment and gene-gene interactions through epidemiological design (33-35).
The transformation of a normal cell into a malignant cell is a multistep mechanism, which involves various alterations on the molecular and genetic level. These molecular alterations occur spontaneously or are induced by carcinogens. As in most other malignancies the development of bladder cancer is caused by the accumulation of various molecular changes. The expression of oncogenes (ras, erbB-2 and EGF receptor), tumor-suppressor genes (Rb, p53),
cell-cycle genes (p15, p16) and DNA-repair genes is altered mostly by mutation or chromosomal aberration. Loss of heterozygosity of chromosome 9p and 9q has been shown to be a crucial event in the transition of normal urothelium to papillary transitional cell carcinoma while p53 is primarily involved in the development of carcinoma in situ (36). A study based on 44788 pairs of twin from Sweden, Denmark, and Finland showed that heritability was estimated to account 31 percent of the variation in susceptibility to the risk of bladder cancer. It was implied that genetic component might not be ignored in the carcinogeneicity of bladder cancer (37).
In this study, by the aid of linkage analysis, we plan to map the susceptibility gene(s) through multiplex family data of bladder cancer cases from arseniasis-endemic and non-endemic areas, to differentiate the difference between gene profiles of residents from arseniasis-endemic and non-endemic areas and to clarify the genetic and functional changes that make a person affected with arsenic-induced bladder cancer.
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2. Progress ReportB2a. Specific Aims
Please state the overall goals of the project, and specific aims, as reviewed and approved by the Study Section and actually awarded. If these specific aims as actually funded did not differ in scope from those actually pursued during the grant period, and if the aims have not been modified, state this. If they have been modified, give the revised aims and the reasons for the modifications.
The overall goals of this subproject are to identify and differentiate the major susceptibility gene(s) for arsenic-induced and non-arsenic-induced bladder cancers through the linkage analysis of genetic markers in members of multiplex families. This subproject will also set up a Genetic Epidemiology and Biostatistics Supporting Core for this program project. It will include following specific aims: 1) the ascertainment of multiplex families through the telephone or home-visit interview, based on a family history questionnaire, of bladder cancer cases reported to the national cancer registry and cases diagnosed and treated in collaborative medical centers; 2) the recruitment of probands and families members through home-visit personal questionnaire interview and biospecimen collection; 3) the purification, depository and inventory of DNA samples in central biospecimen bank; 4) the typing of genetic markers on chromosomes in which loss or gain have been observed through previous comparative genomic hybridization and loss of heterozygosity studies; 5) the mapping of susceptibility gene(s) through linkage analysis of multiplex family data for bladder cancer cases in arseniasis-endemic and non-endemic areas; 6) the examination of the effects of possible candidate genetic marker(s) and their synergistic interactions with environmental factors on bladder cancer; and 7) the establishment of Genetic Epidemiology and Biostatistics Supporting Core to provide methodological support to other subprojects. We do not modified any specific aims of this component project. Base on experience of the first year, we have confidence of accomplishing these specific aims. However, the total number of multiplex families will be less than the proposed number because the modified budgets raised in the initial time of the second grant year was not proved. We expect a total of 60 multiplex families will be recruited during three year grant period.
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2b. Studies and ResultsDescribe the studies directed toward the specific aims during the current grant period and the results obtained. Indicate the extent to which the work accomplished has successfully met the specific aims. Include negative results. If technical problems were encountered in carrying out this project, describe how your approach was modified.
Ⅰ. Multiplex families ascertainment
A total of 730 urothelial carcinoma (UC) consenting participants have been recruited.
Among them, 131 consenting participants from Taiwan University Hospital, 469 consenting participants from Chi-Mei Hospital and 130 consenting participants from Chia-Yi Christian Hospital. An informed consent will be obtained from each participant for the collection related study information. through personal interview in centers for outpatient and inpatient by well trained interviewer. Risk factor questionnaire (RFQ) was used to collect risk factors of UC including cigarette smoking, alcohol drinking, well water consumption, nutrition status, and usage of dye and drug. Family history questionnaire (FHQ) was used to obtain disease history of various cancers especially for UC and chronic diseases including diabetes mellitus (DM) and hypertension. Flow chart for multiplex families recruitment was shown in Figure 1.
Ⅱ. Recruitment of proband and families members
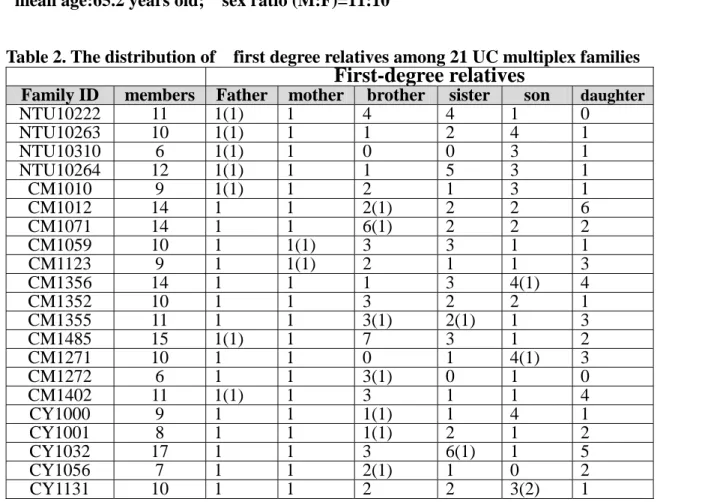
A total of 21 probands whose first degree relatives with UC have been ascertained through FHQ. Now we have mailed invited letters to family members of probands to invite them to participate this study. Among consenting family members, we decided to recruit ten members of each multiplex family including parents, spouse, sibling, and offspring. Questionnaire interview and biospecimen (blood, buccal cell, urine) collection will be executed either in outpatient center of collaborative medical center or household of consenting family members. The flow chart of multiplex families recruitment was shown in figure 2. Socio-demographic characteristics of probands and their first -degree relatives were shown in Table 1 and 2. Pedigrees of eight additive multiplex families newly recruited were illustrated in Figure 3-1 to Figure 3-8.
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2b. Studies and Results (Continue)Initially, among consenting family members, we decided to recruit ten members of each multiplex family including parents, spouse, sibling, and offspring. However, after trying to invite these relatives to participate in this study , about half of them can not be completely interviewed or even refused to be recruited. Reasons for not recruiting or not completing the questionnaire and biospecimen collection were: “no contact with relatives,” “too much effort,” “too emotional,” “too complicated to retrieve all data on relatives” ,“no permission from relatives to give information.”,
”expired address and telephone number” and “too far or no one can take them to the hospital” (44).
Especially, some probands already died for several years ago. In order to overcome these difficulties, we devoted to several strategies and did more intensive efforts to contact them for interview to achieve the goal as followed: [1] outreach to interview those unable to be the hospital
; [2] recheck their medical records and get the correct address and telephone number; [3] instead of face-to-face interview, we try to get the information by postal questionnaire. [4] give some kinds of presents or additional information and a reply card to encourage them to participate in this study.
[5] recruit more collaborated hospitals to increase the number of multiplex families and first-degree relatives; [6] subsequent telephone calls were made for additional information of uncompleted questionnaires; [7] refer the first-degree relatives living in the catchment area of our collaborated hospital to receive the face-to face interview; [8] link medical records and cancer registry database to identify new UC cases and update associated mortality information.
Table 1. The distribution of age and sex 21 UC probands
Family ID Sex Age (year)
NTU10222 M 61 NTU10263 F 67 NTU10310 M 61 NTU10264 M 66
CM1010 M 71
CM1012 M 85
CM1071 M 57
CM1059 F 62
CM1123 M 73
CM1356 F 96
CM1352 M 64
CM1355 F 65
CM1485 M 58
CM1271 M 73
CM1272 F 48
CM1402 M 60
CY1001 F 50
CY1032 F 85
CY1000 F 64
CY1056 F 45
CY1131 F 58
mean age:65.2 years old; sex ratio (M:F)=11:10
Table 2. The distribution of first degree relatives among 21 UC multiplex families
First-degree relatives
Family ID members Father mother brother sister son daughter
NTU10222 11 1(1) 1 4 4 1 0
NTU10263 10 1(1) 1 1 2 4 1
NTU10310 6 1(1) 1 0 0 3 1
NTU10264 12 1(1) 1 1 5 3 1
CM1010 9 1(1) 1 2 1 3 1
CM1012 14 1 1 2(1) 2 2 6
CM1071 14 1 1 6(1) 2 2 2
CM1059 10 1 1(1) 3 3 1 1
CM1123 9 1 1(1) 2 1 1 3
CM1356 14 1 1 1 3 4(1) 4
CM1352 10 1 1 3 2 2 1
CM1355 11 1 1 3(1) 2(1) 1 3
CM1485 15 1(1) 1 7 3 1 2
CM1271 10 1 1 0 1 4(1) 3
CM1272 6 1 1 3(1) 0 1 0
CM1402 11 1(1) 1 3 1 1 4
CY1000 9 1 1 1(1) 1 4 1
CY1001 8 1 1 1(1) 2 1 2
CY1032 17 1 1 3 6(1) 1 5
CY1056 7 1 1 2(1) 1 0 2
CY1131 10 1 1 2 2 3(2) 1
* Number of first-degree relatives affected with UC are shown in parenthesis
7
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2b. Studies and Results (Continue)Figure-3.1
Figure-3.2
Figure-3.3
CY1032 85
551 85
401 45
402 80
501 86
502 UN
503 UN
504 62
505 61
506 60
507 59
508 58
509 57
601 56
602 53
603 49
604 47
605 44
606 42 UN
UN
CY1001 50
551 401
70
402 62
501 52
502 46
503 42
601 24
602 27
603 21 551
64
CY1000 64
401 67
402 UN
501 62
502 54
601 36
602 33
603 34
604 31
605 29
8
Figure-3.4
Figure-3.5
Figure-3.6
CM1271 73
551 59 401
UN
402 UN
501 78
601 59
602 49
603 48
604 46
605 44
606 42
607 40 604
CY1131 58
551
401 402
602
501 502 503 504
601 603
CY1056 45
551 46 401
69
402 76
501 53
502 48
503 41
601 19
602 16
8
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2b. Studies and Results (Cont.)Figure-3.7
Figure-3.8
503 55
504 53 CM1402
60
551 42 401
68
402 56
501 12
502 71
605 28 601
36
602 34
603 32
604 30 601
15 551
48 CM1272
48 401
UN
402 UN
501 52
502 51
503 34
9
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2b. Studies and Results (Cont.)Ⅲ.Risk Ratios for Relatives
In human genetics and genetic epidemiology, risk ratios can assume a number of different forms, including risk ratios for relatives, for candidate genes, and for genetic markers. The goal of many genetic studies is to quantify the risk of disease occurrence associated with particular genetic factors. Evidence for familial aggregation, which is the tendency of disease to cluster in families, provides a rationale for subsequent genetic studies intended to assess particular genetic factors or to search for disease susceptibility genes.A related measure is known as the recurrence risk for a type R relative of an affected individual. It occurs in the numerator of the ratio (40), for familial
aggregation in family case–control designs. For controls that are representative of the general population, the denominator of this ratio approximates the population risk.
In Risch’s (41) development of multilocus models of inheritance for complex traits that are useful in linkage analysis, he defines a risk ratio, λR, which compares the recurrence risk in relatives of type R of an affected individual with the population prevalence K. For example, when the relative type is a sibling, λs is defined as(42)
Pr( D in Relative who is a sibling|affected case) K
Risch(43) also establishes how the power of affected relative pair studies to detect linkage critically depends on the value of λR.
Table 4. The estimated Recurrence Risk Ratio(RRR) of 730 urothelial cell carcinoma (UC) consenting participants
Type of relatives number (affected) siblings only( λs) all relatives (λR) Parents 1460 ( 9 )
Sibling 3650 ( 9 ) 8.2 Offspring 2920 ( 5 )
All relatives 8030 (23) 9.5
* The population prevalence was estimated as 30/100,000.
A widely used measure of familial aggregation is the sibling recurrence-risk ratio, also referred to as λS , which is defined as the ratio of the risk of disease manifestation in siblings of cases
compared with the disease risk in the general population [4,5]. These values underestimate the population risk and therefore overestimate familial aggregation. A mathematical foundation for the choice of the general population risk as the reference value for calculating the sibling
recurrence-risk ratio as a tool for mapping genes for complex diseases was clarified by the work of Risch in the early 1990s [5,14]. As λS is used to design studies and to estimate the power to detect genes for complex human disease, it must be determined [15–18].
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2b. Studies and Results (Cont.)IV. DNA purification, depository and inventory in central biospecimen bank
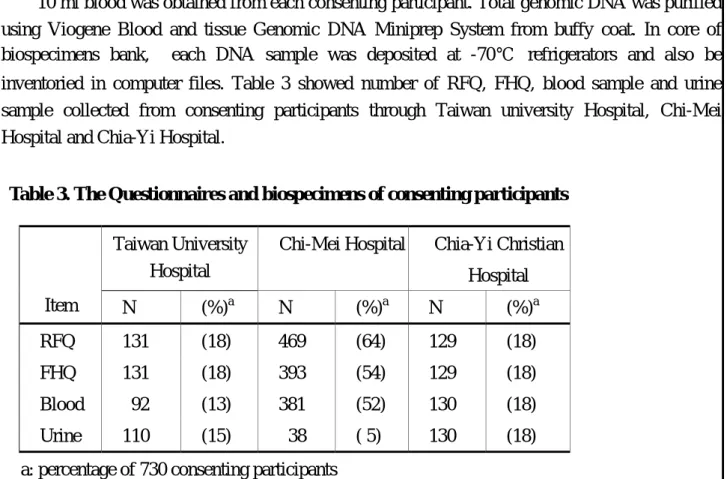
10 ml blood was obtained from each consenting participant. Total genomic DNA was purified using Viogene Blood and tissue Genomic DNA Miniprep System from buffy coat. In core of biospecimens bank, each DNA sample was deposited at -70 ℃ refrigerators and also be inventoried in computer files. Table 3 showed number of RFQ, FHQ, blood sample and urine sample collected from consenting participants through Taiwan university Hospital, Chi-Mei Hospital and Chia-Yi Hospital.
Table 3. The Questionnaires and biospecimens of consenting participants
Taiwan University Hospital
Chi-Mei Hospital Chia-Yi Christian Hospital
Item N (%)a N (%)a N (%)a
RFQ 131 (18) 469 (64) 129 (18) FHQ 131 (18) 393 (54) 129 (18) Blood 92 (13) 381 (52) 130 (18)
Urine 110 (15) 38 ( 5) 130 (18)
a: percentage of 730 consenting participants
Although, the collection of questionnaire and biospecimen was not comprehensive, we still try to do more efforts to increase the comprehensive rate. Some cases or their relatives are difficult to get appropriate volume of blood or urine, we use the buccal swab to collect buccal cells instead of blood samples. In another method, because patients will return to the hospital to have a routine examination, we mentioned interviewers and staffs of the Laboratory Science Department to collect un-recruited samples in this routine process.
At the same time, we extracted DNA from buffy coat or buccal cellls from biospecimen bank. If the patients died for several years ago, we try to check the tissue bank of the collaborated hospitals to get appropriate amounts of tissues for DNA extraction. Then we will performed PCR-RFLP to analyze the genotype of several UC associated susceptible genes such as NQO1, iNOS, EGFR.
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2c. PersonnelSummarize the personnel involved in the project during the grant period. List the personnel in accordance to the following categories: (1) senior investigators, including visitors; (2) postdoctoral fellows; (3) graduate students; (4) technicians; and (5) other research assistants.
Specify for each individual the period of involvement and the percentage commitment of effort.
Name
In Chinese In English Position Title Education
Degree % of effort Job Description or Responsibilities
邱弘毅
陳建仁
邱文祥
王淵宏
徐憶驊
蕭睿祺
謝宜蓁
Hung-Yi Chiou Chien-Jen Chen
Wen-Hsiang Chiou Iuang-Hung Wang Yi-Hwa Hsu
Jui-Chi Hsiao
Yi-Chen Hsieh
Professor
Professor
Associate Professor Doctor student Full-time research assistant Full-time research assistant Master student
Ph.D.
Sc.D.
MD, Ph.D.
MPH
MPH
BS
BS
30%
5%
10%
40%
100%
100%
40%
Director of the component project
Consultant of the component project
UC patients diagnosis and recruitment
Set-up of flow-chart of UC patient recruitment and data management
Questionnaire interview and biospecimens collection Questionnaire interview and biospecimens collection
DNA purification, depository and inventory
Component Project: 6
Data Analysis and Statistical Power:
Genetic linkage analysis will be carried out to identify major susceptible genes related to arsenic-induced bladder cancer based on the data of polymorphisms of microsatellite markers obtained from electrophoresis of ABI PRISM 377 sequencer. Nonparametric multipoint analysis using affected sib pairs, which is robust even when the mode of inheritance is not known, will be performed with program GENEHUNTER version 2.0 (38) to calculate normalized Z scores and associated P value. Traditional LOD score methods will be also performed by means of GENEHUNTER version 2.0 for two-point parametric analysis. Multipoint analysis has the advantage of increasing the power of detecting linkage by utilizing information from two flanking markers rather than a single marker (36). TDT will also be used to analyze linkage data when sufficient number of case-parental pairs is available. Gene markers will be identified as major susceptible gene(s) for arsenic-induced bladder cancer based on following criteria of P-value < 0.05 for Sibpal regression analysis and TDT, and LOD score >1.
Human subject
In this study, a total of 1650 study subjects will be recruited. Each study subject will sign an informed consent on a voluntary basis at recruitment. The consent form will follow the guidelines recommended by the Joint Working Group on Ethical, Legal, and Social Implications of Human Genome Research(39). Only the study subjects, themselves, will be permitted to give consent, not relatives or surrogates. The patients’ care will not be affected by whether they participate in the study or not.
The research procedures consist of the collection of 35 ml of venous blood, mucous cell, and 50 ml of urine sample for each study subject. All study information collected through various questionnaire including ARF, RFQ, and FHQ will be used for research purposes only. Disposable syringes with sterilized needles will be used for blood collection to prevent any blood-born transmission of infectious agents.
PROGRAM PROJECT: Component Project ___6__
((請填入子計畫編號) B2d. Projected TimelineProvide a reasonable timetable for the execution of the work outlined in the project. Highlight appropriate milestones that you might use to target the studies. Indicate technical hurdles that might slow down the execution of the work and discuss any contingencies that you have or might have built in the research plan in anticipation of these difficulties. Do not exceed one page.
Component projected timetable ( second year)
The second Year
Month Order
Item
1st Month 2nd Month 3rd Month 4th Month 5th Month 6th Month 7thMonth 8th Month 9th Month 10thMonth 11thMonth 12thMonth
Remark
Recruitment of more collaborative medical centers
Ascertainment of multiplex families (FHQ, RFQ) Biospecimens collection from consenting participants Set up biospecimens bank Recruitment first degree relatives of multiplex families
Data keying, checking, and analysis of FHQ and RFQ
During the second grant year of the component project, we worked very hard to recruit every UC patients we could found. Until now, we interview 730 consenting participants from Taiwan university Hospital ,Chi-Mei hospital. and Chia-Yi Christian Hospital. We also collected blood and urine from consenting participants if they agree us to do it. First degree relatives of twenty-one multiplex families have been recruitment (family history prevalence of UC =2.9%), which implied that we have good opportunities to examine the effects of possible candidate genetic marker(s) and their synergistic interactions with environmental factors on UC. However, based on our limited personnel, it would be very difficult to recruit 150 multiplex families during grant period. In order to speed recruitment of multiplex families, we need more research assistants to recruit at least 60 multiplex families each year in the following two grant year. The detail arrangement of personnel in this project and related modified budget will be further described in the section B3. I hope the modified budget could be funded. Then, we feel confident of accomplishing the component study.
Component Project: 6
Research Plan (continuation)- Literature Cited
1. International Agency for Research on Cancer. Arsenic and arsenic compounds.
Overall Evaluation of Carcinogenicity: An Updating of IARC Monographs Volumes 1 to 42, Suppl. 7, pp. 100-106. Lyon, France: International Agency for Reaserch on Cancer, 1987.
2. Chiou HY, Chiou ST, Hsu YH, et al. Incidence of transitional cell carcinoma and arsenic in drinking water: A Follow-up Study of 8102 Residents in an arseniasis-endemic area in northeastern Taiwan. Am J Epidemiol 2001;153(3):411-418.
3. Chen CJ, Chuang YC, Lin TM and Wu HY. Malignant neoplasms among residents of blackfoot disease endemic area in Taiwan:high arsenic artesian well water and cancers.Cancer Res 1985;45:5895-5899.
4. Chen CJ, Chuang YC, You SL and Wu HY. A retrospective study on malignant neoplasms of bladder, lung and liver in blackfoot disease endemic area in Taiwan. Br J Cancer 1986;53:399-405.
5. Chiou HY, Hsueh YM, Liaw KF, et al. Incidence of internal cancers and ingested inorganic arsenic: A seven-year follow-up study in Taiwan. Cancer Res 1995;55:1296-300.
6. Luchtrath H. The consequences of chronic arsenic poisoning among Moselle wine grower: pathoanatomical investigations of post-mortem examinations performed between 1960 and 1977. J Cancer Res Clin Oncol 1983;105:173-182.
7. Smith A, Goyeolea M, Haque R, et al. Marked increase in bladder and lung cancer mortality in a region of northern Chile due to arsenic in drinking water.Am J Epidemiol 1998;147:660-9
8. Hopenhayn-Rich C, Biggs ML, Fuchs A, et al.Bladder cancer mortality associated with arsenic in drinking water in Aargentina.Epidemiology 1996;7:117-24.
9. Ma L, Luo ZD, Zhang YM, et al. Current status of research on endemic arseniasis in Inner Mongolia. Chinese J Public Health 1997;15:S15-43.
10. Lee AM and Fraumeni JFJR. Arsenic and respiratory cancer in man: An occupational study. J Natl Camcer Inst 1969;42:1045-1052.
11. Yih LH, Ho IC, Lee TC. Sodium arsenite disturbs mitosis and induces chromosome loss in human fibroblasts. Cancer Res 1998;57:5051-9.
12. Hsueh YM, Chiou HY, Huang YL, et al. Serum beta-carotene level, arsenic methylation capability and incidence of arsenic-induced skin cancer. Cancer Epidemiol Biomark Prev 1997;6:589-96.
13. Tseng MP. Molecular epidemiological studies on associations with
arsenic-induced skin cancer for genetic polymorphisms of glutathione
S-transferases and p53. Master thesis, Graduate Institute of Epidemiology,
College of Public Health, National Taiwan University. Taipei: National Taiwan
Component Project: 6
Literature Cited
University, 1998.
14. Lin YC. Molecular epidemiological studies on association with arsenic-induced skin cancer for genetic polymorphisms of DNA repair enzymes. Master thesis, Graduate Institute of Epidemiology, College of Public Health, National Taiwan University. Taipei: National Taiwan University, 1999.
15. Hsieh FI, Pu YS, Chen HD, et al. Genetic polymorphisms of N-acetyltansferase 1 and 2 and risk of cigaratte smoking-related bladder cancer. Br J Cancer 1999;81:53
16. International Agency for Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans: overall evaluations of carcinogenicity (Suppl. 7). Lyon: IARC Publ, 1987:100-106.
17. US Environmental Protection Agency. Report on the expert panel on arsenic carcinogenicity: review and workshop. Washington, DC, 1997.
18. Wu MM, Kuo TL, Hwang YH, Chen CJ. Dose-response relation between arsenic concentration in well water and mortality from cancers and vascular diseases. Am J Epidemiol 1989;130:1123-1131.
19. Waner JK, Moore LE, Smith MT, et al. Increased micronuclei in exfoliated bladder cells of individuals who chronically ingest arsenic-contaminated water in Nevada. Cancer Epidemiol Biomarkers Prev 1994;3:583-590.
20. Larramendy ML, Popescu NC, DiPaolo JA. Induction by inorganic metal salts of sister-chromatid exchanges and chromosome aberrations in human and in Syrian hamster cell strains. Environ Mutagen 1981;3:597-606.
21. Hsu YH, Li SY, Chiou HY, et al. Spontaneous and induced sister chromatid exchanges and delayed cell proliferation in peripheral lymphocytes of Bowen’s disease patients and matched controls of arseniasis-hyperendemic villages.
Mutat Res 1997;336:241-251.
22. Liou SH, Lung JC, Chen YH, et al. Increased chromosome-type chromosome aberration frequency as biomarkers of cancer risk in a blackfoot endemic area.
Cancer Res 1999;59:1481-1484.
23. Gerhard S. Arsenic: opportunity for risk assessment. Arch Toxicol 1991;65:
525-531.
24. Jac A. Nicholoff and Merl F. Hoekstra. DNA damage and repair Volum II: DNA Repair in Higher Eukarytes. 1998.
25. Guengerich FP, Lim DH, Iwasaki M. Role of human cytochrome P-450 IIE1 in the oxidation of many low molecular weight cancer suspects. Chem Res Toxicol 1991;4:168-179.
26.
O’Neill IK, Chen J, Bartsch H. Relevance to human cancer of N-nitroso compounds, tobacco and mycotoxins. IARC Scientific Publications No. 105.
Lyon, France: International Agency for Research on Cancer, 1991.
Component Project: 6
27. Tsutsumi M, Matsuda Y, Takada A. Role of ethanol-inducible cytochrome P-450 2E1 in the nitrosodimethylamine. Hepatology 1993;18:1483-1489.
28. Yu MM, Gladek-Yarborough A, Chiamprasert S, Santella RM, et al. Cytochrome p450 2E1 and glutathione S-transferase M1 polymorphisms and susceptibility to hepatocellular carcinoma. Gastroenterology 1995;109:1266-1273.
29. The Human Genome. Science 2001;291.
Ian NMD, Dongfeng G, Rosalind H G, Emmanuel S, Shu Y. Epidemiology and the genetic basis of disease. Internal J Epidemiol 2001;30:661-667.
30.
Deborah AM. Genetic approach to familial aggregation: III. Linkage analysis.
In:Muin JK, Terri H, Bernice HC (eds) Fundamentals of Genetic Epidemiology,1993 pp.284-311.Oxford University Press, New York, USA.
31.
Kruglyak L, Paly MJ, Reeve-Daly MP, et al. Parametric and Nonparametric Linkage Analysis:A Unified Multipoint Approach. American J Human Genetics 1996;58:1347-1363.
32.
Sampson MJ, Williams T, Heyburn PJ et al. Prevalence of HFE (haemochromatosis gene) mutations in unselected male patients with type 2 diabetes. J Lab Clin Med 2000;135:170-173.
33.
Stuart KA, Busfield F, Jazwinska EC et al. The C282Y mutation in the haemochromatosis gene (HFE) and hepatitis C virus infection are independent cofactors for porphyria cutanea tarda in Australian patients. J Hepatol 1998;28:404-409.
34.
Piperno A, Mariani R, Arosio C et al. Haemochromatosis in patients with beta-thalassaemia trait. Br J Haematol 2000;111:908-914.
35.
Tuomainen TP, Kontula K, Nyyssonen K et al. Increased risk of acute myocardial infarction in carriers of the haemochromatosis gene Cys282Tyr mutation: a prospective cohort study in men in eastern Finland [see comments].
Circulation 1999;100:1274-1279.
36.
Brandau S, Bohle A Bladder cancer I. Molecular and genetic basis of carcinogenesis. European urology 2001;39(5):491-497.
37.