Original Article
Risk Factors Related to the Need for Endoscopic Retrograde Cholangiopancreatography Intervention in Cholelithiasis and Choledocholithiasis
Chi-Chih Wang
1,2,4, Tzu-Wei Yang
2,4,8, Hsuan-Yi Chen
2,4, Yao-Tung Wang
1,2,5, Wen-Wei
Sung
1,2,6, Chang-Cheng Su
4, Wei-Liang Chen
4, Chun-Che Lin
1,2,4, Ming-Hseng Tseng
3,7*,
Ming-Chang Tsai
1,2,4*Institute of Medicine1, School of Medicine2, Department of Medical Informatics3, Chung Shan Medical University and Division of Gastroenterology and Hepatology4, Division of Pulmonary Medicine5, Department of Internal Medicine, Department of Urology6, Information Technology Office7, Chung Shan Medical University Hospital, Taiwan
Institute and Department of Biological Science and Technology, National Chiao Tung University, Hsinchu8, Taiwan
Background and Aims: Cholelithiasis is associated with several risk factors. Moreover, cholelithiasis and choledocholithiasis share some risk factors. The risk stratification of pure gallbladder (GB) stones, as well as GB stones with common bile duct (CBD) stones and pure CBD stones requiring therapeutic endoscopic retrograde cholangiopancreatography (ERCP), has not been fully elucidated.
Methods: From Taiwan’s National Health Insurance Research Database (NHIRD), we identified 20671 cholelithiasis patients and 62013 control subjects (matched by sex and age in 1:3 ratio) during the period 2004-2011. We compared the risk factors for cholelithiasis patients and normal control group. Further evaluations were performed on patients with pure GB stones and patients with GB and CBD stones and patients with pure CBD stones who underwent therapeutic ERCP.
Results: Coronary artery disease, hyperlipidemia, chronic kidney disease, end stage renal disease on regular hemodialysis, hepatitis B infection, liver cirrhosis, diabetes mellitus, and hemolysis were risk factors for cholelithiasis. Risk factors for GB and CBD stone patients needing ERCP included male gender (odds ratio: 1.211, 95% CI: 1.039-1.436, p value = 0.015), age over 60 (odds ratio: 1.912, 95%
CI: 1.492-2.450, p value <0.001), and hemolysis (odds ratio: 1.719, 95% CI: 1.008-2.929, p value = 0.047). For pure CBD stone patients needing ERCP, risk factors were male gender (odds ratio: 1.496, 95% CI: 1.195-1.874, p value <0.001), age 41-60 (odds ratio: 2.344, 95% CI: 1.503-3.654, p value
<0.001), and age over 60 (odds ratio: 4.484, 95% CI: 2.896-6.943, p value <0.001). There was lower incidence of pure CBD stones requiring ERCP among those with hyperlipidemia (odds ratio: 0.613, 95% CI: 0.469-0.802, p value <0.001).
Conclusion: Male gender and advanced age play significant roles in the requirement for therapeutic ERCP among cholelithiasis patients.
Keywords: gallstones; choledocholithiasis; risk factors
* Corresponding Author: Ming-Chang Tsai
Ming-Hseng Tseng share correspondence with Ming-Chang Tsai.
Tel: +886-4-24739595 ext 38315 Fax: +886-4-24739220 E-mail: [email protected]
Introduction
Gallstone disease is a very common disorder that has led to significant economic burden on healthcare systems worldwide 1, 2. This disease often requires surgical intervention 3. The primary types of gallstones in the West are cholesterol stones 2. The epidemiology of gallstone disease in Asia differs somewhat from that in the West. Choledocholithiasis results from gallbladder (GB) stones passing through cystic duct into extra- and intrahepatic ducts or bile duct stones formed without GB stones. The former results in primarily cholesterol or black-pigment stones 4 and the latter brown pigment bile duct stones 5. In recent years, there have been changes in the types of gallstone disease observed clinically.
Moreover, in the past two decades, incidence rate of gallstone disease has increased in Taiwan 6.
Risk factors differ based on geographic distribution, ethnicity, and even socioeconomic status, according to a 2011 updated report from Taiwan 7. From the results of a previous study 8, overall prevalence of gallstone disease is around 5% in rural areas without significant gender differences. Fatty liver disease and age have been shown to be the most important risk factors. There are many population- based studies that have demonstrated that the risk factors of cholelithiasis in Taiwan are similar to those in Western countries 9-11.
Although gallstone disease has a long history worldwide and well-known risk factors, such as high body mass index (BMI), female gender 12, dietary habits 13, oral contraceptives 14, hyperlipidemia 13, 15,
16, rapid appetite loss, hepatitis C 17, cirrhosis, and high caloric intake 18, the relationship between and risk factors of cholelithiasis and choledocholithiasis remain to be elucidated. The aim of this study is to identify the differences in risk factors between cholelithiasis and choledocholithiasis using Taiwan’s National Health Insurance Research Database (NHIRD) for the period 2004-2011.
Our results may be helpful in understanding the high-risk groups requiring endoscopic retrograde cholangiopancreatography (ERCP).
Methods
This study was approved by the Institutional Review Board (IRB) of Chung Shan Medical University Hospital, Taiwan. The IRB waved the need for informed consent as this is a retrospective study based on the NHIRD. All authors declare no conflicts of interest.
Study design
This study is a population-based, retrospective, cohort study with data from Taiwan’s NHIRD, which covers more than 99% of the total population
19. Cholelithiasis cases were identified from one million random samples from 2004 to 2011 using Codes of International Statistical Classification of Diseases and Related Health Problems-9th Edition (ICD-9). Inpatient data and outpatient data were available and diagnoses were confirmed by at least 3 visits to OPD clinics to avoid classification errors.
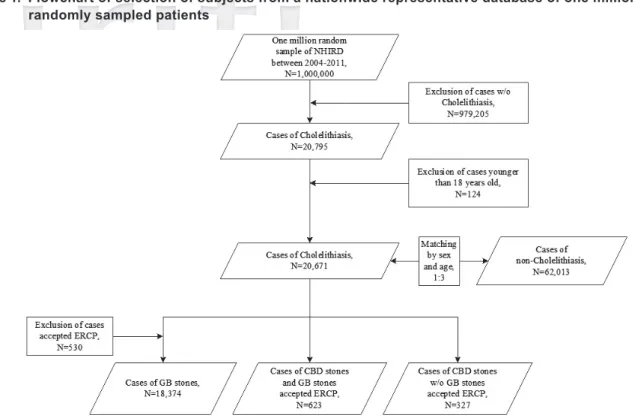
There were 20795 cholelithiasis cases included initially. However, 124 cases under the age of 18 were excluded. A total of 20671 patients were enrolled and 62013 control subjects were selected by sex and age matching in 1:3 ratio. Control subjects were defined as individuals who had not been diagnosed with cholelithiasis or had undergone a related medical procedure, such as cholecystectomy, common duct exploration for removal of calculus, or ERCP. Medical conditions that were considered possible risk factors for cholelithiasis included coronary artery disease (CAD), hyperlipidemia, chronic kidney disease (CKD), end stage renal disease (ESRD) on regular hemodialysis (HD), hepatitis B infection (CHB) without liver cirrhosis (LC), hepatitis C infection (CHC) without LC, LC, diabetes mellitus and hemolysis disease.
Risk factors and odds ratios were calculated for both cholelithiasis and control groups. ICD-9 and procedural codes are shown in the supplementary table.
Cholelithiasis cases were divided into three groups: (1) with pure GB stones, (2) with CBD and GB stones who underwent ERCP, and (3) with pure CBD (without GB) stones who underwent ERCP.
To avoid misclassification of patients with pure GB stones using only ICD-9, we excluded patients who had undergone therapeutic ERCP, which should only be performed for bile duct management. The
Wei-Liang Chen, Chun-Che Lin, Ming-Hseng Tseng, Ming-Chang Tsai
study concept is shown in Figure 1. All historical risk factors for cholelithiasis were compared among these three groups.
Data processing and statistical analysis Microsoft SQL Server 2008 R2 (Microsoft Corporation, Redmond, WA, USA) was employed to manage the study database and queries were performed with the SQL programming language.
Statistical analysis was conducted using SPSS 19.0 (SPSS, Inc., Chicago, IL).
Characteristics of the study subjects and their matched controls were compared using the Chi- Square χ2 test. Binary logistic regression model was also employed for comparisons of the risks of study subjects and their matched controls. A two- tailed P-value of 0.05 was considered statistically significant.
Results
As age and sex were used to establish normal
population without cholelithiasis as the control group, these factors age and sex could not be included as the risk stratification in our study design.
Cholelithiasis cases and matched controls There were significant differences (p value less than 0.0001) in CAD, hyperlipidemia, CKD, ESRD on HD, CHB without LC, CHC without LC, LC, diabetes and hemolysis between the cholelithiasis cases and the control group. All these diseases were associated with higher risk of cholelithiasis, as shown in Table 1. We further compared the unadjusted odds ratios and the multi-variate adjusted odds ratios of these covariates. The highest unadjusted odds ratio was 5.68 (95% CI: 5.275-6.123, p <0.001) for LC patients, followed by 3.75 (95%
CI: 3.184-4.412, p <0.001) for hemolysis patients, 3.09 (95% CI: 2.382-4.013, p <0.001) for CHC patients, and 3.01 (95% CI: 2.787-3.253, p <0.001) for CHB patients. In terms of adjusted odds ratios, only CHC became non-significant with p value of 0.908 (Odds ratio: 1.02, 95% CI: 0.771-1.339). The NHIRD = National Health Insurance Research Database, GB = gallbladder, CBD = common bile duct, ERCP = endoscopic retrograde cholangiopancreatography
Figure 1. Flowchart of selection of subjects from a nationwide representative database of one million randomly sampled patients
highest adjusted odds ratio was 5.62 for LC patients (95% CI: 5.210-6.069, p value <0.001), followed by 3.25 for CHB patients (95% CI: 2.991-3.523, p value
<0.001), and 2.69 for hemolysis patients (95% CI:
2.259-3.200, p value <0.001). Chronic kidney disease and ESRD on HD were associated with higher risk for cholelithiasis (Odds ratio 1.33 and 1.18, p value
<0.001 and 0.007, respectively). Unadjusted odds ratios and adjusted odds ratios of these covariates are shown in Table 2.
Cholelithiasis and choledocholithiasis requiring intervention
Based on comparisons of patients with pure GB stones, patients with CBD and GB stones who underwent ERCP, and patients with pure CBD stones who underwent ERCP, we found
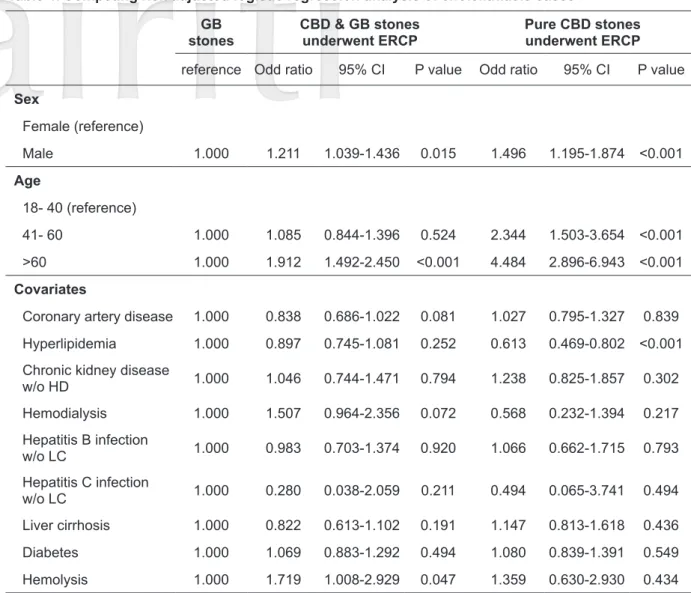
significant associations with gender, age, CAD, hyperlipidemia, CKD, ESRD and diabetes, but not with CHB, CHC, LC or hemolysis. From our results, CBD stones occurred more often in male, elderly, CAD, CKD, and diabetes patients, as shown in Table 3. Among the patients with pure CBD stones, 59.33 % were male, 60.86% were older than 60, 30.28% had CAD, 8.56% had CKD, and 31.5% had diabetes. Using pure GB stone group as a reference, competing risk adjusted logistic regression analysis of CBD and GB stone patients who underwent ERCP showed strong associations with male gender (odds ratio: 1.211, 95% CI: 1.039- 1.436, p value = 0.015), age over 60 (odds ratio:
1.912, 95% CI: 1.492-2.450, p value <0.001), and hemolysis (odds ratio: 1.719, 95% CI: 1.008-2.929, p value = 0.047). The risk analysis of pure CBD Table 1. Characteristics of cholelithiasis cases and matched controls
Characteristic Cholelithiasis
N=20,671 Control
N=62,013 p value
N SD; % N SD; %
Sex 1.000
Female 10667 51.6 32001 51.6 1.000
Male 10004 48.4 30012 48.4
Age
18 - 40 3820 18.48 11460 18.48
41 - 60 7936 38.39 23808 38.39
>60 8835 42.74 26505 42.74
Covariates <0.001
Coronary artery disease 5305 25.66 9747 15.72 <0.001
Hyperlipidemia 6553 31.70 13335 21.50 <0.001
Chronic kidney disease w/o HD 1124 5.44 1853 2.99 <0.001
H/D 458 2.22 844 1.36 <0.001
Hepatitis B infection w/o LC 1322 6.40 1376 2.22 <0.001
Hepatitis C infection w/o LC 115 0.56 112 0.18 <0.001
LC 1990 9.63 1141 1.84 <0.001
Diabetes 5868 28.39 11049 17.82 <0.001
Hemolysis 326 1.58 264 0.43 0.43
SD= standard deviation, w/o= without, H/D= hemodialysis, LC= liver cirrhosis
Wei-Liang Chen, Chun-Che Lin, Ming-Hseng Tseng, Ming-Chang Tsai
stone patients showed significant associations with male gender (odds ratio: 1.496, 95% CI: 1.195- 1.874, p value <0.001), age 41-60 (odds ratio:
2.344, 95% CI: 1.503-3.654, p value <0.001), and age over 60 (odds ratio: 4.484, 95% CI: 2.896- 6.943, p value <0.001). Meanwhile, hyperlipidemia was a protective factor for pure CBD stones (odds ratio: 0.613, 95% CI: 0.469-0.802, p value <0.001).
Odds ratios of comparisons among pure GB stone patients, CBD and GB stone patients who needed ERCP intervention, and pure CBD stone patients who needed ERCP intervention are shown in Table 4.
Discussion
In our study, we initially collected the risk factors of cholelithiasis observed in previous studies. In the comparisons of these risk factors between the cholelithiasis group and the control group, all covariates showed statistical significance. Therefore, cholelithiasis is more likely to occur in patients with CAD, hyperlipidemia, CKD, ESRD, CHB, CHC, LC, diabetes, or hemolysis. These results confirmed previous findings on the risk factors for cholelithiasis. On competing risk adjusted logistic
regression analysis for all risk factors, only CHC lost statistical significance in the association with cholelithiasis. CHC has been shown to be associated with lipid metabolism and steatohepatitis 20-22 and to overlap with hyperlipidemia. The true risk for cholelithiasis is due to hyperlipidemia or diabetes rather than CHC. The top 3 leading risk factors for cholelithiasis in Taiwan are LC, CHB, and hemolysis. People with these conditions have 2 to 5 times the risk compared with the normal population.
Comparisons were also performed among groups with pure GB stones, CBD and GB stones with ERCP, and pure CBD stones with ERCP to determine the risk factors for CBD stones requiring ERCP intervention. As gender and age were no longer controlling factors, we could include them in the evaluation. Based on gender and age stratification, there were significant differences in CAD, hyperlipidemia, CKD, ESRD and diabetes among the groups. The logistic regression model with pure GB stone patient group as a reference showed that only gender (male), age (over 60), and hemolysis contribute to the need for ERCP for both CBD and GB stones. Hemolysis increases the association of ERCP intervention with GB stones and CBD stones by increasing hemoglobin Table 2. Competing risk analysis for cholelithiasis
Variables Unadjusted odds ratio Adjusted odds ratio
Odd ratio 95% CI p value Odd ratio 95% CI p value Covariates
Coronary artery disease 1.851 1.782-1.923 <0.001 1.536 1.473-1.601 <0.001 Hyperlipidemia 1.694 1.636-1.755 <0.001 1.381 1.327-1.437 <0.001 Chronic kidney disease w/o HD
H/D 1.935 1.813-2.064 <0.001 1.331 1.228-1.443 <0.001
H/D 1.642 1.464-1.842 <0.001 1.182 1.046-1.335 0.007
Hepatitis B infection w/o LC 3.011 2.787-3.253 <0.001 3.246 2.991-3.523 <0.001 Hepatitis C infection w/o LC 3.092 2.382-4.013 <0.001 1.016 0.771-1.339 0.908
LC 5.683 5.275-6.123 <0.001 5.623 5.210-6.069 <0.001
Diabetes 1.828 1.763-1.897 <0.001 1.330 1.276-1.387 <0.001 Hemolysis 3.748 3.184-4.412 <0.001 2.689 2.259-3.200 <0.001 SD= standard deviation, w/o= without, H/D= hemodialysis, LC= liver cirrhosis
metabolism, causing increase in bilirubin production and secretion through the bile duct system 23, 24. Patients older than 60 have 1.912 times the risk for CBD stones needing ERCP intervention due to the cumulative time risk of allowing GB stones to pass through the cystic duct into bile ducts.
Previous studies have shown that pure CBD stone patients have different risk factors than GB stone patients 4, 5, 25. Male gender, age 41-60, and age over 60 increase the risk of pure CBD stones 1.50, 2.34, and 4.48 times, respectively. Hyperlipidemia reduces the risk of pure CBD stones by about 40%.
The majority of pure GB stones are cholesterol stones, which result from supersaturated cholesterol in bile content. Therefore, hyperlipidemia is an important risk factor for GB stones. In contrast, hyperlipidemia contributes less to the risk of pure
CBD stones.
CKD, CHB, LC, diabetes, and hemolysis only slightly increased the risk for pure CBD stones, while CHC slightly decreased the risk for pure CBD stones in this study, possibly due to the relationship with lipid metabolism. Although LC and hemolysis increased risks of CBD stones, the major risk factors for pure CBD stones compared with pure GB stones were still gender and age.
Although this is a reliable large-scale study, it has some limitations. First, this is a retrospective cohort study based on a national database. Therefore, we could only determine the relationships among diseases, not their consequences. Second, age and gender could not be compared between the cholelithiasis group and the normal population due to the study design. Some covariates with demonstrated Table 3. Demographic data of cholelithiasis cases
Characteristic Pure GB stones CBD & GB stones
underwent ERCP Pure CBD stones
underwent ERCP P value
N % N % N %
Sex <0.001
Female 9259 51.83 292 46.87 113 34.56
Male 8606 48.17 331 53.13 194 59.33
Age (years) <0.001
18-40 3727 20.86 98 15.73 25 7.65
41-60 7181 40.20 195 31.30 103 31.50
> 60 6957 38.94 330 52.97 199 60.86
Covariates
Coronary artery disease 4377 24.50 159 25.52 99 30.28 0.049
Hyperlipidemia 5743 32.15 191 30.66 81 24.77 0.014
Chronic kidney disease w/o HD 902 5.05 39 6.26 28 8.56 0.008
H/D 385 2.16 22 3.53 5 1.53 0.050
Hepatitis B infection w/o LC 1371 7.67 40 6.42 20 6.12 0.302
Hepatitis C infection w/o LC 103 0.58 1 0.16 1 0.31 0.323
LC 1575 8.82 53 8.51 40 12.23 0.093
Diabetes 4818 26.97 189 30.34 103 31.50 0.037
Hemolysis 251 1.40 15 2.41 7 2.14 0.069
SD= standard deviation, w/o= without, H/D= hemodialysis, LC= liver cirrhosis
Wei-Liang Chen, Chun-Che Lin, Ming-Hseng Tseng, Ming-Chang Tsai
effects on cholelithiasis, such as menopause and certain self-pay medications, could not be analyzed due to shortcomings in the registration of data.
In conclusion, male gender, age over 60, and concomitant hemolysis are associated with higher risk of biliary events requiring ERCP intervention in cholelithiasis patients. Meanwhile, age over 40 and male gender are the major risk factors for pure CBD stones needing ERCP intervention.
Funding
This work was supported by a grant from the Chung Shan Medical University Hospital research
program, Taichung, Taiwan (CSH- 2013-C-032).
Author contribution statement
Conception and design: Chi-Chih Wang, Ming- Hseng Tseng, Ming-Chang Tsai
Acquisition of data: Ming-Hseng Tseng, Chi-Chih Wang, Chun-Che Lin
Analysis and interpretation of data: Ming-Chang Tsai, Chi-Chih Wang, Yao-Tung Wang
Drafting of the manuscript: Chi-Chih Wang, Tzu-Wei Yang, Hsuan-Yi Chen
Critical revision of the manuscript: Tzu-Wei Yang, Hsuan-Yi Chen, Chun-Che Lin
Table 4. Competing risk adjusted logistic regression analysis of cholelithiasis cases stonesGB CBD & GB stones
underwent ERCP Pure CBD stones underwent ERCP reference Odd ratio 95% CI P value Odd ratio 95% CI P value Sex
Female (reference)
Male 1.000 1.211 1.039-1.436 0.015 1.496 1.195-1.874 <0.001
Age
18- 40 (reference)
41- 60 1.000 1.085 0.844-1.396 0.524 2.344 1.503-3.654 <0.001
>60 1.000 1.912 1.492-2.450 <0.001 4.484 2.896-6.943 <0.001 Covariates
Coronary artery disease 1.000 0.838 0.686-1.022 0.081 1.027 0.795-1.327 0.839 Hyperlipidemia 1.000 0.897 0.745-1.081 0.252 0.613 0.469-0.802 <0.001 Chronic kidney disease
w/o HD 1.000 1.046 0.744-1.471 0.794 1.238 0.825-1.857 0.302
Hemodialysis 1.000 1.507 0.964-2.356 0.072 0.568 0.232-1.394 0.217 Hepatitis B infection
w/o LC 1.000 0.983 0.703-1.374 0.920 1.066 0.662-1.715 0.793
Hepatitis C infection
w/o LC 1.000 0.280 0.038-2.059 0.211 0.494 0.065-3.741 0.494
Liver cirrhosis 1.000 0.822 0.613-1.102 0.191 1.147 0.813-1.618 0.436
Diabetes 1.000 1.069 0.883-1.292 0.494 1.080 0.839-1.391 0.549
Hemolysis 1.000 1.719 1.008-2.929 0.047 1.359 0.630-2.930 0.434 GB= gallbladder, CBD= common bile duct, CI= Confidence interval, w/o= without, H/D= hemodialysis, LC= liver cirrhosis
Statistical analysis: Wen-Wei Sung, Chang-Cheng Su, Wei-Liang Chen
Supervision: Ming-Hseng Tseng, Ming-Chang Tsai
References
1. Nealon WH, Urrutia F, Fleming D, et al. The economic burden of gallstone lithotripsy. Will cost determine its fate? Ann Surg 1991;213:645-9; discussion 649-50.
2. Bodmer M, Brauchli YB, Krahenbuhl S, et al.
Statin use and risk of gallstone disease followed by cholecystectomy. JAMA 2009;302:2001-7.
3. Schirmer BD, Winters KL, Edlich RF. Cholelithiasis and cholecystitis. J Long Term Eff Med Implants 2005;15:329-38.
4. Mack E. Pathogenesis and Clinical Presentation of Bile Duct Calculi. Semin Laparosc Surg 1995;2:76- 84.
5. Sandstad O, Osnes T, Urdal P, et al. Brown pigment stones in the common bile duct: reduced bilirubinate diconjugate in bile. Scand J Gastroenterol 2000;35:198- 203.
6. Huang J, Chang CH, Wang JL, et al. Nationwide epidemiological study of severe gallstone disease in Taiwan. BMC Gastroenterol 2009;9:63.
7. Hung SC, Liao KF, Lai SW, et al. Risk factors associated with symptomatic cholelithiasis in Taiwan: a population-based study. BMC Gastroenterol 2011;11:111.
8. Chen CH, Huang MH, Yang JC, et al. Prevalence and risk factors of gallstone disease in an adult population of Taiwan: an epidemiological survey.
J Gastroenterol Hepatol 2006;21:1737-43.
9. Liu CM, Tung TH, Chou P, et al. Clinical correlation of gallstone disease in a Chinese population in Taiwan: experience at Cheng Hsin General Hospital.
World J Gastroenterol 2006;12:1281-6.
10. Nealon WH, Urrutia F, Fleming D, et al. The economic burden of gallstone lithotripsy. Will cost determine its fate? Ann Surg 1991;213:645-9; discussion 649-50.
2. Bodmer M, Brauchli YB, Krahenbuhl S, et al.
Statin use and risk of gallstone disease followed by cholecystectomy. JAMA 2009;302:2001-7.
3. Schirmer BD, Winters KL, Edlich RF. Cholelithiasis and cholecystitis. J Long Term Eff Med Implants 2005;15:329-38.
4. Mack E. Pathogenesis and Clinical Presentation of Bile Duct Calculi. Semin Laparosc Surg 1995;2:76-84.
5. Sandstad O, Osnes T, Urdal P, et al. Brown pigment stones in the common bile duct: reduced bilirubinate diconjugate in bile. Scand J Gastroenterol 2000;35:198- 203.
6. Huang J, Chang CH, Wang JL, et al. Nationwide epidemiological study of severe gallstone disease in Taiwan. BMC Gastroenterol 2009;9:63.
7. Hung SC, Liao KF, Lai SW, et al. Risk factors associated with symptomatic cholelithiasis in Taiwan: a population- based study. BMC Gastroenterol 2011;11:111.
8. Chen CH, Huang MH, Yang JC, et al. Prevalence and risk factors of gallstone disease in an adult population of Taiwan: an epidemiological survey.
J Gastroenterol Hepatol 2006;21:1737-43.
9. Liu CM, Tung TH, Chou P, et al. Clinical correlation of gallstone disease in a Chinese population in Taiwan: experience at Cheng Hsin General Hospital.
World J Gastroenterol 2006;12:1281-6.
10. Tung TH, Ho HM, Shih HC, et al. A population- based follow-up study on gallstone disease among type 2 diabetics in Kinmen, Taiwan. World J Gastroenterol 2006;12:4536-40.
11. Liew PL, Wang W, Lee YC, et al. Gallbladder disease among obese patients in Taiwan. Obes Surg 2007;17:383-90.
12. Wheeler M, Hills LL, Laby B. Cholelithiasis: a clinical and dietary survey. Gut 1970;11:430-7.
13. Cui Y, Li Z, Zhao E, et al. Risk factors in patients with hereditary gallstones in Chinese pedigrees.
Med Princ Pract 2012;21:467-71.
14. Howat JM, Jones CB, Schofield PF. Gall-stones and oral contraceptives. J Int Med Res 1975;3:59- 62.
15. Singh A. Familial hyperlipoproteinemia and gallstones.
Can Med Assoc J 1975;113:733-5.
16. Grigor'eva IN, Maliutina SK, Voevoda MI. [Role of hyperlipidemia in cholelithiasis]. Eksp Klin Gastroenterol 2010:64-8.
17. Acalovschi M, Buzas C, Radu C, et al. Hepatitis C virus infection is a risk factor for gallstone disease:
a prospective hospital-based study of patients with chronic viral C hepatitis. J Viral Hepat 2009;16:860-6.
18. Shaffer EA. Gallstone disease: Epidemiology of
Wei-Liang Chen, Chun-Che Lin, Ming-Hseng Tseng, Ming-Chang Tsai
gallbladder stone disease. Best Pract Res Clin Gastroenterol 2006;20:981-96.
19. Cheng TM. Taiwan's new national health insurance program: genesis and experience so far. Health Aff (Millwood) 2003;22:61-76.
20. Liu JL, Chen JY, Chen CT, et al. Community-based cross-sectional study: the association of lipids with hepatitis C seropositivity and diabetes mellitus. J Gastroenterol Hepatol 2012;27:1688-94.
21. Matos CA, Perez RM, Pacheco MS, et al. Steatosis in chronic hepatitis C: relationship to the virus and host risk factors. J Gastroenterol Hepatol 2006;21:1236-9.
22. Fierro NA, Gonzalez-Aldaco K, Torres-Valadez R, et al. Immunologic, metabolic and genetic factors in hepatitis C virus infection. World J Gastroenterol 2014;20:3443-56.
23. Iwanczak F, Prandota J. [Metabolism of bilirubin and its excretion with bile]. Pediatr Pol 1980;55:655- 60.
24. Schmid R. Bilirubin metabolism in man. N Engl J Med 1972;287:703-9.
25. Tazuma S. Gallstone disease: Epidemiology, pathogenesis, and classification of biliary stones (common bile duct and intrahepatic). Best Pract Res Clin Gastroenterol 2006;20:1075-83.