Aerosol and Air Quality Research, 12: 275–282, 2012 Copyright © Taiwan Association for Aerosol Research ISSN: 1680-8584 print / 2071-1409 online
doi: 10.4209/aaqr.2011.09.0155
Traffic Air Pollution and Risk of Death from Breast Cancer in Taiwan: Fine Particulate Matter (PM 2.5 ) as a Proxy Marker
Li-Ju Hung
1,2, Shang-Shyue Tsai
3, Pei-Shih Chen
4, Ya-Hui Yang
5, Saou-Hsing Liou
6, Trong-Neng Wu
6,7, Chun-Yuh Yang
4,6*1
Department of Public Health, Kaohsiung Medical University, Kaohsiung, Taiwan
2
Department of Family Medicine, Kaohsiung Veterans General Hospital, Ksohsiung, Taiwan
3
Department of Healthcare Administration, I-Shou University, Kaohsiung, Taiwan
4
Department of Public Health, Kaohsiung Medical University, Kaohsiung, Taiwan
5
Department of Occupational Safety and Hygiene, Fooyin University, Kaohsiung, Taiwan
6
Division of Environmental Health and Occupational Medicine, National Health Research Institute, Miaoli, Taiwan
7
Graduate Institute of Public Health, China Medical University, Taichung, Taiwan
ABSTRACT
The relationship between breast cancer mortality and air pollution was examined using an ecological design. The study areas consisted of 61 municipalities in Taiwan. Air quality data for recorded concentrations of fine particulate matter (PM
2.5) from study municipalities for 2006–2009 were obtained as a marker of traffic emissions and were used as a proxy for polycyclic aromatic hydrocarbons (PAHs) exposure. Age-standardized mortality rates for breast cancer mortality were calculated for the study municipalities for the years 1999–2008. A weighted multiple regression model was used to calculate the adjusted risk ratio in relation to PM
2.5levels. Results showed that individuals who resided in municipalities with the highest PM
2.5were at an increased risk of death from breast cancer. This study is the first to suggest that exposure to high levels of PM
2.5, a proxy measure of PAHs, may be associated with an increased risk of death from breast cancer.
The findings of this study warrant further investigation into the role of air pollutants in the risk of breast cancer.
Keywords: Traffic air pollution; Breast cancer; Fine particulate matter.
INTRODUCTION
The incidence of breast cancer varied widely internationally, with the highest rates observed in North America and Europe and the lowest rates in Asia (Schottenfeld and Frauimeni, 1996). In Taiwan, the incidence rates for breast cancer was 51.95 per 100,000 in 2008 (DOH, 2008). Breast cancer is the fourth leading cause of female cancer mortality (DOH/Taiwan, 2011). The age- adjusted mortality rate for breast cancer was 11 per 100,000 in 2010. There is substantial geographic variation in female breast cancer mortality within the country (NHRI/Taiwan, 2004), which suggests an environmental risk factor may be involved.
The known risk factors for breast cancer are primarily related to the reproductive life of women and inheritance (e.g., BRCA1 and BRCA2 gene mutations) (Coyle, 2004).
*
Corresponding author. Tel.: 886-7-3121101 ext. 2141;
Fax: 886-7-3110811
E-mail address: [email protected]
Only about one-third of new cases of breast cancer are attributable to known risk factors, and much of the etiology remains unexplained (Coyle, 2004; Crouse et al., 2010).
Therefore it has been hypothesized that environmental exposures may also contribute to breast cancer risk (Laden and Hunter, 1998; Coyle, 2004).
Ambient outdoor air pollution has been implicated as a cause of various health problems including cancer (Dominici et al., 2005; Boffetta, 2006; Curtis et al., 2006; Samet and Krewski, 2007). Air pollution is a complex mixture of different gaseous and particulate components; thus it is difficult to define an exposure measure of relevance when the biological mechanisms are largely unknown (Boffetta and Nyberg, 2003). Air pollution from motor vehicle exhaust has been one of the most studied environmental factors (Craig et al., 2008; Chen and Li, 2010; Chuang et al., 2010a;
Shen et al., 2010; Tsai et al., 2011). Exhaust from traffic is
a complex mixture of many chemical compounds, including
benzene, polycyclic aromatic hydrocarbons (PAHs) and
benzo[a]pyrene (B[a]P) (Chuang et al., 2010b; Wu et al.,
2010; Huang et al., 2011a, b; Kao et al., 2011). The
International Agency for Research on Cancer (IARC)
classified the emission of diesel exhaust engine compounds
Hung et al., Aerosol and Air Quality Research, 12: 275–282, 2012 276
as probably carcinogenic (Group 2A) and gas engine exhaust compounds as possibly (Group 2B) carcinogenic to humans (IARC, 1989).
According to occupational epidemiologic studies, excess risks of breast cancer were reported to be associated with occupational exposure to PAHs among pre- and postmenopausal women (Petralia et al., 1999; Gammon et al., 2002; Labreche et al., 2010). Given that these same pollutants are present in the motor vehicle exhaust, it is plausible that traffic-related exposures may contribute to the risk of breast cancer (Crouse et al., 2010). Several studies reported an increased risk for breast cancer in association with surrogate measures of exposure to vehicle exhaust, including emissions associated with heavy traffic density (Lewis-Michl et al., 1996), total suspended particulates (TSP) (Bonner et al., 2005), estimated exposures to B[a]P derived from a traffic emissions model (Nie et al., 2007), and estimated nitrogen dioxide (NO
2) derived from a land- use regression model (Crouse et al., 2010).
In Taiwan, the major source of PAHs is traffic exhaust (Chang et al., 2003). PAHs can be present in particulate or gaseous phase. Gaseous PAHs usually contain more fractions of less carcinogenicity and lower molecular weights, while particulate PAHs contain more fractions of higher carcinogenicity and higher molecular weights (Chang et al., 2006). PAHs with high molecular weights are often more carcinogenic than those with low molecular weights (Ravindra et al., 2001). Therefore particulate phase PAHs are considered to be the most hazardous substances to human health. Most of the PAHs were in the particulate phase.
Ninety to 95% of particulate phase PAHs are physically associated with particular matter (PM) < 3.3 μm (Ravinndra et al., 2001; Bonner et al., 2005). These small particles are thought to have biological relevance because they can be inhaled and deposited in the lower respiratory tract (Bonner et al., 2005).
The study reported here was designed to explore further whether the risk of death from breast cancer is associated with exposure to PAHs, using fine particulate matter (PM
2.5), a marker of traffic-related air pollution, as a proxy for PAHs exposure in Taiwan.
METHODS Study Areas
Taiwan is divided into 359 administrative districts, which are referred to in this study as municipalities. In 1994, a network of 66 air pollution monitoring stations was established in 66 municipalities by the Environmental Protection Administration (EPA) in Taiwan. Among these, two stations were excluded because they were situated in the National Park areas and served as background monitoring sites. In addition, three stations were removed due to the reconstruction of the buildings where there were built during 2000–2007, and were excluded from analysis. This elimination left 61 monitoring stations situated in 61 municipalities for study (Fig. 1). These 61 municipalities provide an opportunity to investigate the impact of PM
2.5air pollution on the risk of death from breast cancer.
Fig. 1. Locations of the monitoring stations in this study.
PM
2.5Exposure Estimates
There is an extensive air pollution monitoring network in Taiwan, managed by Taiwan EPA as mentioned above, which routinely monitors five "criteria" pollutants (PM
10, O
3, CO, SO
2, NO
2). However, PM
2.5was not regularly monitored. The monitoring stations were fully automated and provided daily readings of polutant levels.
PM
2.5concentrations in Taiwan have been measured continuously since 2006. The monitoring stations provided data for PM
2.5in mean daily mass concentration (μg/m
3).
The availability of the monitoring network for PM
2.5provides an opportunity to investigate the impact of fine particle air pollution on female breast cancer mortality. We obtained PM
2.5data for study municipalities from the EPA's air quality monitoring stations for 2006–2009. The municipality of residence for all cases and controls was identified from death certificates. The municipality of residence formed the only basis for estimating their fine particulate air pollution exposure.
Mortality
Information concerning both the number of death and Taiwan's midyear population by sex, age, calendar year and municipality from 1999–2008 was obtained from the Department of Health which is in charge of the death registration system in Taiwan. In this study, female breast cancer deaths were those that were defined by the International Classification of Disease, Injury and Causes of Death (ICD-9 code 174). As the age distribution was not comparable among the 61 municipalities, the age standardized rates (ASR) were computed by the direct method, using the world population in 2000 as the standard population (Ahmad et al., 2000).
Fertility
Reproduction, particularly early full-term pregnancy,
seems to exert a protective effect against breast cancer
(Kelsey, 1979; Wigle, 1977; Rosenwaike, 1980; Remennick,
Hung et al., Aerosol and Air Quality Research, 12: 275–282, 2012 277 1989). One indicator of reproduction was available at the
municipality level in Taiwan where fertility rates were recorded for different time periods from 1971 till now. In this study the fertility rates from 1971 for females aged 20–24 years were used to study the possible beneficial effect that early pregnancy might have in the prevention of breast cancer mortality (MOI/Taiwan, 1973). Fertility rates for earlier than 1971 would have been preferable; however, data were not available. An assumption was thus made that a municipality with high average fertility rates in 1971 would also have higher than average rates prior to 1971.
Socioeconomic Factors
It was found that mortality attributed to cancer was associated with urbanization gradients (Yang and Hsieh, 1998; Reynolds et al., 2004a; Hall et al., 2005). In this study, an urbanization index (Tzeng and Wu, 1986) was used to adjust for possible confounding resulting from different urbanizational levels among the municipalities. The urbanization index used in this study serves as a proxy for a large number of explanatory variables such as population density, age composition, mobility, economic activity and family income, educational level, environmental factors, and health service-related facilities which are related to the etiology of mortality. Each municipality in Taiwan was given a degree of urbanization category, 1–8. A municipality with the highest urbanization score, such as the Taipei metropolitan area, was classified in category 1, while mountainous areas with the lowest score were assigned to category 8. This index was used previously (Chiu et al., 2006; Liu et al., 2008). For the analyses, the urban-rural classification was further subdivided into two categories: I, urban areas (categories 1–4); and II, rural areas (categories 5–8).
Statistics
In the analysis, the 61 municipalities were divided into tertiles according to the levels of PM
2.5and the fertility rates. The risk ratios were calculated in relation to the group with the lowest exposure level. A weighted multiple regression model was used to calculate the adjusted risk ratio. In addition to the levels of PM
2.5, both fertility rates and urbanization index were included in the multiple regression analysis to adjust for the possible influence on the increased risk of death from breast cancer and to obtain a better estimate of the impact of PM
2.5on the risk of death from breast cancer. Since Taiwan municipalities vary greatly in size, the regression model used took into account the size of the municipalities. For each municipality the weight used was the square root of person-years (Draper and Smith, 1998). A Wald chi-square test for linear trend was also performed by entering PM
2.5exposures as a 3- level ordinal variable (with the values 0–2) (Rothman and Greenland, 1998). Values of p < 0.05 were considered statistically significant.
RESULTS AND DISCUSSION
Average annual age-standardized breast cancer mortality
rates per 100,000 (ASR) for 1999–2008 by tertiles of PM
2.5levels and fertility rates are listed in Table 1.
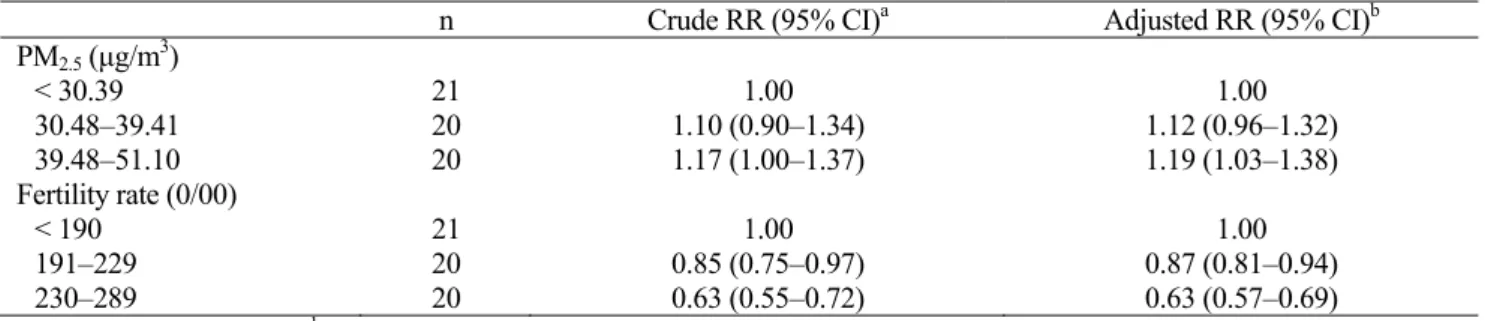
The crude risk ratios for death from breast cancer were significantly higher for the group with the highest levels of PM
2.5. Further, municipalities with high fertility rates have a statistically significant lower risk of death from breast cancer (Table 2).
Results of the weighted multiple regression analyses are shown in Table 2. Adjustments for possible confounders (the urbanization level and fertility rate) did not markedly alter the risk ratio. The adjusted RR (95% CI) were 1.12 (0.96–1.32) for the group with PM
2.5levels between 30.48 μg/m
3and 39.41 μg/m
3and 1.19 (1.03–1.38) for the group with PM
2.5levels between 39.48 μg/m
3and 51.10 μg/m
3, compared to the group with the lowest PM
2.5levels. Trend analyses showed statistically significant trend in risk of death attributed to breast cancer with increasing PM
2.5levels.
When we included PM
2.5levels as a continuous variable, similar trend in results were observed as those found when PM
2.5levels were examined as a categorical variable (a mortality rate of 0.065/10
5increase per 1 μg/m
3of PM
2.5increase). In contrast, there was a statistically significant decreasing trend in the risk of death from breast cancer with increasing fertility rates.
The results of the present study showed that individuals who resided in municipalities with the highest PM
2.5levels, a proxy measure of PAHs, were at a significantly increased risk of death from breast cancer. This finding is essentially consistent with previous epidemiologic studies which examined the hypothesis that breast cancer may be associated with exposure to traffic air pollution (Bonner et al., 2005;
Nie et al., 2007; Crouse et al., 2010) and industrial pollution (Pan et al., 2011).
There have been a number of epidemiological studies that assessed the increased risk of death from breast cancer development from living in an urban rather than a rural area.
In general, breast cancer mortality had been considerably higher in urban populations than non-urban ones (Blot et al., 1977; Goldsmith, 1980; Greenberg, 1983; Muir et al., 1987; Kelesy and Berkowitz, 1988; Yang and Hsieh, 1998).
The only "urban factor" consistently mentioned in the literature is air pollution, suggesting that residing in an urban area is a reliable surrogate for increased air pollution exposure (Greenberg, 1983).
The specific exposure chemicals responsible for the
Table 1. Mortality from breast cancer by PM
2.5levels and fertility rates in 61 Taiwan's municipalities, 1999–2008.
n ASR
aPM
2.5(μg/m
3)
< 30.39 21 10.83 ± 3.15
30.48–39.41 20 11.90 ± 4.21
39.48–51.10 20 12.69 ± 2.95
Fertility rate (0/00)
< 190 21 14.21 ± 2.11
191–229 20 12.11 ± 3.45
230–289 20 8.93 ± 2.66
a
ASR: age-standardized rate ± standard deviation.
Hung et al., Aerosol and Air Quality Research, 12: 275–282, 2012 278
Table 2. Risk ratio (RR) of mortality from breast cancer in relation to PM
2.5levels based on a weighted multiple regression model.
n Crude RR (95% CI)
aAdjusted RR (95% CI)
bPM
2.5(μg/m
3)
< 30.39 21 1.00 1.00
30.48–39.41 20 1.10 (0.90–1.34) 1.12 (0.96–1.32)
39.48–51.10 20 1.17 (1.00–1.37) 1.19 (1.03–1.38)
Fertility rate (0/00)
< 190 21 1.00 1.00
191–229 20 0.85 (0.75–0.97) 0.87 (0.81–0.94)
230–289 20 0.63 (0.55–0.72) 0.63 (0.57–0.69)
a