義 守 大 學 醫 務 管 理 學 系 碩 士 班
Department of Healthcare Administration I-Shou University
碩 士 論 文
不同居住型態老人生活品質之比較研究
A Comparison of the Quality of Life of Community Elderly People with Different Living Arrangements
指導教授:顏永杰 研 究 生:釋妙尊
中 華 民 國 一百 年 七 月
- iii -
Acknowledgments
Improvement of the health, longevity and low fertility have driven the world to the aging population. The aging population certainly affects the economic expansion, politics of the country. The societal problems could arise from these impacts. The findings of the study should have made it possible to contrast the level of quality of life of the elderly people in different living places, providing a basis for making clinical and governmental policy changes.
With the compassionate of Master Hsing Yun and aim of the Fo Guang Shan, which is benefiting the society through charity activities, the religious organization concerns and take care of the sentient beings including the elderly people. Hopefully, the research findings could help to alleviate the quality of life for the elderly people.
Special thanks to Professor Yen for his patience on supervising the research. Both of us were having a stress on time constraint and always had to catch up thing within limited times.
But I did enjoy doing the research with him. Secondly, I would like to dedicate the gratitude
to the donations of Fo Guang Shan Compassion Foundation for the souvenirs; Professor Peter
Harasym for supporting the research; Hui-Fen, Su for collecting the data, and the Songhe
volunteers for interviewing the elderly people. There were heaps of challenges such as the
elderly’s hearing impairment, language barriers and etc especially interviewing the elderly
people. Though we still finally able to accomplish the research as in we believe in “where
there is dharma there is a way”.
- iv -
Abstract
Background: The building of senior housing becomes a priority issue for the country as the world is facing a dramatic transition to an aging society in the coming 10 to 20 years. The aim of this study was to compare the quality of life (QOL), physical illness, health status, depressive symptoms for the elderly in Taiwan with different living settings at apartment, home or the institution-based home and the contribution of these determinants to the quality of life. This was a cross-sectional comparative study.
Methods: One hundred fifty-one participants in Kaohsiung, Taiwan from three settings and fulfilling inclusion criteria were recruited in this study. The questionnaires administered included Quality of Life (WHOQOL-BREF, Taiwan version); Taiwan Depression Questionnaire (TDQ); level of dependence (Barthel Index of Activities of Daily Living, ADL;
Instrumental Activities of Daily Living Scale, IADL), sociodemographic characteristics.
Results: The health status (beta coefficient= -0.77, p<.01, =.04) showed significant effect to the association of different living places and quality of life for physical (p<.000), psychological (p<.05), social relationship (p<.05) and environment (p<.05) domains. The age and gender also showed the significant effects to the physical domain (beta coefficient= -0.05, SD 0.02, p= .04) and social relationship domain (beta coefficient= 0.85, SD 0.36, p= .02) respectively. The significant effects were found in the association of different living places and quality of life (p<.05). However, after controlling the age, gender, health status, life conditions of the three different living places the main effects of the association did not differ significantly (p>.05).
Conclusion: The good perceptions on the health status and mental health are the major determinant of the quality of life for the elderly people regardless the different living places.
These comparisons make it possible to contrast the level of quality of life of the elderly
people in different living places, providing a basis for making clinical and governmental
policy changes. However, selection bias or non-response bias could occur therefore the results
should be interpreted carefully.
- v -
Keywords: Senior Housing, Quality Of Life, Elderly
- vi -
摘要
研究背景:未來10到20年間全球面臨高齡社會的來臨,因此,老人居住處所成為各 國的重要議題。本研究的主要目的是在探討並比較居住在老人公寓、住家及機構的老人 間之生活品質、身體疾病、健康狀況和憂鬱症狀,及上述這些因子對生活品質的影響。
本研究採用橫斷、比較性的研究。
研究方法:共151位來自3種不同居住型態且符合條件的老人參與本研究。研究工具 包括世界衛生組織生活品質量表(台灣簡明版)、台灣憂鬱量表、工具性日常生活活動量 表以及個人基本資料問卷。
研究結果:健康狀態對不同居住處所和生活品質有顯著性的影響(β係數= -0.77,
p<.01, =.04),包括生理 (p<.000), 心理 (p<.05),社會關係 (p<.05) 及 環境 (p<.05) 的層面皆有顯著性影響。年齡和性別各別對生理(β係數= -0.05, SD 0.02, p= .04)和社會關 係(β係數= 0.85, SD 0.36, p= .02)層面也有顯著性的影響。不同居住處所和老人生活品質 有顯著性的影響(p<.05)。然而,將三種不同居住處所老人的年齡、性別、健康狀態和生 活條件等因子加以控制之後,不同居住處所與老人的生活品質變得沒有顯著性的影響 (p>.05)。
結論:健康狀態暨良好的生理和心理健康是決定老人生活品質的主要因素而非不同 的居住型態。透過此項研究比較這些居住在不同地方的老人其生活品質的對照可提供政 府政策制定和實際層面之參考準則。然而在本研究中可能發生選擇偏差及受試者拒絕回 答的偏差,因此在研究結果必需更為謹慎分析。
關鍵字: 老人居住型態,生活品質,老人
- vii -
Contents
Chapter 1 Introduction
1.1 Definition of old age ………
1.2 Normal a ging………
1.3 Definition of Quality of Life ………
1.4 Societal impact of aging ………
1.5 Aims of the study ………
Chapter 2 Literature Review
2.1 Quality of Life of elderly people………
2.2 Living arrangements and care of elderly people………
2.3 Hypothesis questions ………
Chapter 3 Materials and Methodology
3.1 Design………
3.2 Participants………
3.3 Instrumental tools ………
3.4 Statistical analysis ………
3.5 Ethical approval ………
Chapter 4 Results
4.1 Sample characteristic ………
4.2 Objective health conditions………
4.3 Quality of life assessed by the WHOQOL -BREF…………
1 2 4 9 16
17 20 26
30 30 34 36 38
39
47
49
- viii -
4.4 Contribution of the four QOL domains ………
4.5 Analysis of covariance ………
Chapter 5 Discussion
5.1 Important aspects of Quality of Life ………
5.2 Health status and Quality of Life ………
5.3 Depression and Quality of Life ………
5.4 Other weighting factors of Quality of Life ………
5.5 Limitation ………
Chapter 6 Conclusion
6.1 Important items and core items ………
6.2 Future Implications………
Bibliography ………
Appendices
Appendix A Short Portable Mental Status Questionnaire ……
Appendix B The World Health Organization Quality of Life (WHOQOL)-BREF-Taiwan Version ………
Appendix C Participant characteristics………
Appendix D Barthel index of activities of daily living (ADL) activity score ………
Appendix E Instrumental activities of daily living scale (IADL) Appendix F Taiwan depression questionnaire (TDQ) …………
56 60
66 67 68 69 71
73 74 76
83
85
91
94
96
100
- ix -
Table
Table 1-1▓Conceptual Quality of Life framework………
Table 1-2▓WHOQOL-BREF domains ………
Table 1-3▓Percentage of people >65 years living at home and in institutions (prevalence data; different years in the early1990s) ………
Table 1-4▓Elderly social welfare in Taiwan ………
Table 2-1▓Quality of life profile: seniors version ………
Table 2-2▓Number of the people >65 years living in different types of senior housing, Taiwan ………
Table 2-3▓The difference between the home, senior apartment and institution-based home………
Table 2-4▓Theoretical model of the study………
Table 3-1 Equations for computing the scores of each domain……
Table 4-1▓Demographic characteristics of participants………
Table 4-2▓Scores of objective health: mental health and level of dependence measures ………
Table 4-3▓Mean scores (SD) of Quality of Life by domains………
Table 4-4▓Scores of predictors for contributions of the four QOL domains………
Table 4-5▓Effect of living arrangements on QOL outcomes,
Kaohsiung, Taiwan (N=151)………
6 8
14 15 18
21
25 28 37 41
48 51
58
62
- x -
Figure
Figure 2-1▓Structure model of the study………
Figure 3-1▓Participants flow chart………
Figure 4-1 95%CI means of physical domain of QOL by different
living arrangements ………
Figure 4-1 95%CI means of psychological domain of QOL by
different living arrangements (continued)………
Figure 4-1 95%CI means of social relationship domain of QOL
by different living arrangements (continued)………
Figure 4-1 95%CI means of environment domain of QOL by
different living arrangements (continued)………
29 33
52
53
54
55
- 1 -
Chapter 1 ▓ Introduction
1.1▓Definition of old age
Old age or elderly is defined as 60 or 65 years of age or older (Encyclopedia Britannica, 2010). The chronological or “official” definitions of ageing can differ widely from traditional or community definitions of when a person is older. For an example, in Africa, definition of an elder should be either 50 or 55 years of age whereas many individuals in Africa do not have an official record of their birthdates (WHO, 2010). According to Senior Citizen Welfare Act of Taiwan- Chapter 1: General Regulations (Article 2): In this Act, elders are people who are aged above 65 years old. The United Nation (UN) has not adopted a standard criterion, but generally uses 60 years old and above to refer to the older population (United Nation, 2010).
For research, statistic, and policy purposes, it is useful to distinguish between the old and the oldest old. National Institute on Aging, United State defined oldest old as people age 85 and over, while people of extreme old age—that is, centenarians (persons 100 years of age and older) (NIH, 2007).
As reviewed and suggested by Orimo, et al. (2006), the definition of elderly should be based on comprehensive evidence in all aspects of social, cultural and medical sciences. In his study, he found out that“over the past 10 years (1992-2002) the physical activity of healthy elderly (over 65) has been more youthful by 7.5 years in men and 10 years in women.
Pathological examination revealed that the cerebral arteries have been more youthful by 20 years in men and 10 years in women during the past 14 years (1986-2000)” (Orimo, 2006).
Thus, he suggested the current definition of elderly (65 year olds and above) should be
changed to those 75 years old and above. However, elderly people recruited in this research is
65 years old and above.
- 2 -
1.2▓Normal aging
Aging is a biological, complex natural process potentially involving every molecule, cell, and organ in the body. It may include some changes that are not necessarily problematic or harmful. Gray hair and wrinkles, for instance, certainly are manifestations of aging.
Individuals age at extremely different rates. In fact even within one person, organs and organ systems could show different rates of decline. According to the data from Baltimore Longitudinal Study of Aging, normal aging or some generalities can be made as below (NIH, 2006 & WebMED, 2008 ):
1. Heart muscle: Heart muscles thicken with age. Maximal oxygen consumption during exercise declines in men by about 10 percent with each decade of adult life and in women by about 7.5 percent.
2. Arteries: Arteries tend to stiffen with age. The older heart, in turn, needs to supply more force to propel the blood forward through the less elastic arteries.>
3. Lung: Maximum breathing (vital) capacity may decline by about 40 percent between the ages of 20 and 70.
4. Brain: With age, the brain loses some of the structures (axons) that connect nerve cells (neurons) to each other. The ability of individual neurons to function may diminish with age.
5. Kidneys: Kidneys gradually become less efficient at extracting wastes from the blood.
6. Bladder: Bladder capacity declines. Urinary incontinence, which may occur after tissues atrophy, particularly in women, can often be managed through exercise and behavioral techniques. BODY FA
7. Metabolism and body fat: Over time, the body typically needs less energy, and the
metabolism slows. Hormone changes in the aging body result in a shift to more body fat
and less muscle mass. With age, fat is redistributed in the body, shifting from just beneath
the skin to deeper organs. Women typically have a higher percentage of body fat than
men.
- 3 -
8. Muscles: Without exercise, estimated muscle mass declines 22 percent for women and 23 percent for men between the ages of 30 and 70.
9. Bones: Bone mineral is lost and replaced throughout life; loss begins to outstrip replacement around age 35. This loss accelerates in women at menopause.
10. Sight: Difficulty focusing close up may begin in the 40s; the ability to distinguish fine details may begin to decline in the 70s. Most people in their 40s develop a need for reading glasses as the lens becomes less flexible. It's also normal for night vision and visual sharpness to decline, while from 50 years on glare increasingly interferes with clear vision, greater difficulty in seeing at low levels of illumination, and more difficulty in detecting moving objects in the later years.
11. Hearing: Over time, changes in the ear make high-frequency sounds harder to hear and changes in tone and speech less clear. Hearing declines more quickly in men than in women. These changes tend to accelerate after age 55.
12. Skin: With age, the skin becomes less elastic and more lined and wrinkled. Fingernail growth also slows. The oil glands gradually produce less oil, making the skin drier than before.
13. Hair: It is normal for hair to gradually thin on the scalp, pubic area, and armpits. As hair pigment cells decline in number, gray hair growth increases.
14. Height: By age 80, it's common to have lost as much as 2 inch in height. This is often related to normal changes in posture and compression of joints, spinal bones, and spinal discs.
15. Sexual function: Men and women produce lower levels of hormones starting in their 50s.
Men produce less sperm, and their sexual response time slows, though the male sex drive does not decrease. Women stop ovulating and have a number of menopausal changes linked to lower estrogen production.
These are the normal signs of aging. Everyone has their own pace of changing gradually
as they aged. However, aging is not synonymous with the disease. As we aging the superficial
changes could also increase the risk of disease, disability or death. The progressive
deterioration of many bodily functions over time is accompanied by decreased fertility and
increased risk of mortality as an individual gets older (NIH, 2006). Birth, old age, sickness
and death are a natural process in our life span. These processes are inevitable and the old age
- 4 -
is the final stage of the normal life span. Thus, a healthy aging or a good quality of elderly life is what we are seeking for in the world of aging population. There probably is no single
“secret” of aging. More than likely, all of these elements—heredity, environment, and lifestyle—have complex roles in determining whether an individual will have a long and healthy life, according to scientists who study aging (NIH, 2006).
1.3▓Definition of Quality of Life
The definition of Quality of Life (QOL) involves broad concept and individual perception. McCall (1975) suggested that the best way of approaching quality of life measurement is to measure the extent to which people’s “happiness requirements” is met, that is those requirements which are a necessary (although not sufficient) condition of anyone’s happiness; those “without which no member of the human race can be happy.”
Individual’s quality of life could be very different, varied, subjective or objective. The concepts and models of quality of life vary potentially from country to country, and even from area to area within countries (Schalock et al., 2002). The objective axis incorporates norm-referenced measures of well-being which reflects the culturally normative values and determined by the assessment of external condition while the subjective axis incorporates measures of perceived well-being (Cummins, 1997). The subjective questions such as “How do you feel about your life as a whole” with respondent using a Likert scale with satisfaction/
dissatisfaction were incorporate into the one of the popular WHO-Quality of Life-BREF measurement instruments. Nevertheless, researchers have developed and incorporate domains such as housing, environment, jobs, neighborhood, and health, aspects of culture, values, and spirituality into the measurement. The useful techniques that have helped to conceptualize and measure these multiple domains have been developed. This broad multidimensional concept includes subjective evaluations of both positive and negative aspects of life (WHO, 1998).
The final scores of the quality of life reflect the degree of satisfaction with personally relevant
domains (Cummins, 1997).
- 5 -
World Health Organizations defines Quality of Life (QOL) as “an individual’s perception of his or her position in life in the context of the culture and value system where they live, and in relation to their goals, expectations, standards and concerns” (WHO, 1994).
Besides, the definition Quality of Life by Quality of Life Research Unit, University of
Toronto (1994) is consistent with the definition by WHO which is “the degree to which a
person enjoys the important possibilities of his or her life.” The extent of a person's QOL in
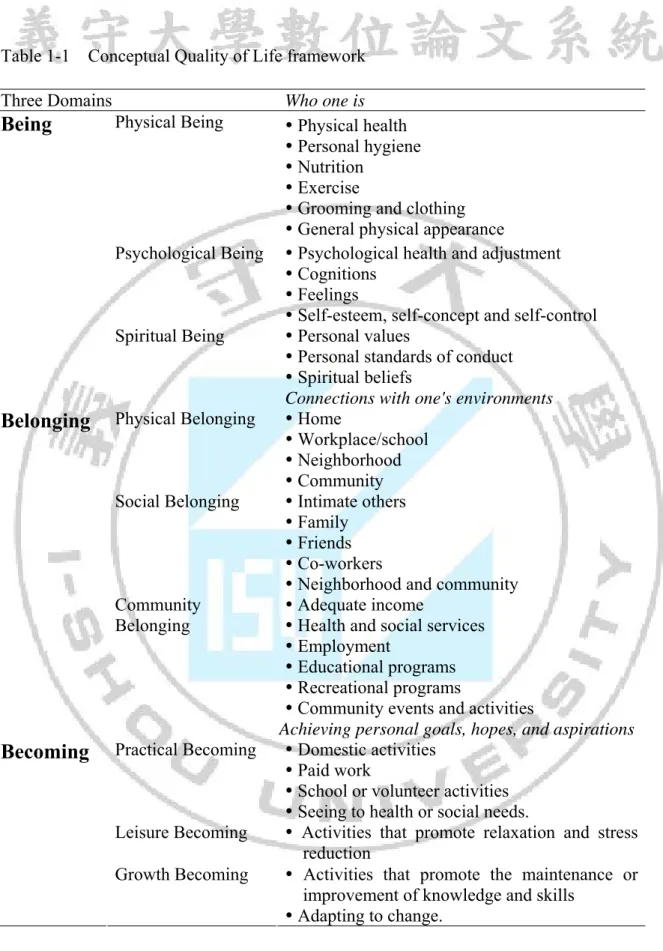
the areas of Being, Belonging, and Becoming and their sub-domains is determined by two
factors: importance and enjoyment (refer to Table 1-1). Thus, QOL consists of the relative
importance or meaning attached to each particular dimension and the extent of the person's
enjoyment with respect to each dimension. Farquhar (1995) suggested beside the general
health and functional status, valued components family relationship including marriage,
family and home life, social contacts and activities should be taken into consideration. In this
way, quality of life is adapted to the lives of all humans, at any time, and from their individual
perspectives. It is a complex perception and concept.
- 6 -
Table 1-1▓Conceptual Quality of Life framework
Three Domains Who one is
Physical Being Physical health
Personal hygiene
Nutrition
Exercise
Grooming and clothing
General physical appearance
Psychological Being Psychological health and adjustment
Cognitions
Feelings
Self-esteem, self-concept and self-control Being
Spiritual Being Personal values
Personal standards of conduct
Spiritual beliefs
Connections with one's environments Physical Belonging Home
Workplace/school
Neighborhood
Community Social Belonging Intimate others
Family
Friends
Co-workers
Neighborhood and community Belonging
Community Belonging
Adequate income
Health and social services
Employment
Educational programs
Recreational programs
Community events and activities
Achieving personal goals, hopes, and aspirations Practical Becoming Domestic activities
Paid work
School or volunteer activities
Seeing to health or social needs.
Leisure Becoming Activities that promote relaxation and stress reduction
Becoming
Growth Becoming Activities that promote the maintenance or improvement of knowledge and skills
Adapting to change.
Source: The Quality of Life Research Unit, University of Toronto (2011),
http://www.utoronto.ca/qol/concepts.html
- 7 -
There are few definitions or models that could draw the researcher attention or interest.
Overall, the quality of life is about the enjoyment, goodness and meaning of life.
The World Health Organization Quality of Life (WHOQOL-100) project was initiated in 1991 and WHOQOL-BREF since 1996 in order to develop an international cross-culturally comparable quality of life assessment instrument. There are two reasons to develop a quality of life assessment, which including a need for a genuinely international measure, and restates its commitment to the continued promotion of an holistic approach to health and health care.
Basically there are two instruments WHOQOL-100 and WHOQOL-BREF for the assessment of quality of life. Both instruments have many uses, including use in medical practice, research, audit, policy making and in assessing the effectiveness and relative merits of different treatments. The instruments use five-point Likert scales for all items. A visual analogue scaling methodology was used which specified the anchor points for the different types of response scales to be used in the instrument (that is, using English anchor points scales identified by “Very satisfied – Very dissatisfied”, “Not at all - Extremely”, “Not at all - Completely”, and “Never - Always”. The scales with anchor points “Very poor – Very good”
and “Very unhappy – Very happy” were also included by some centers).
The WHOQOL-BREF Field Trial Version has been developed to look at domain level profiles which assess quality of life since the WHOQOL-100 may be too lengthy for some uses. The WHOQOL-BREF is a shorter version of the original instrument that may be more convenient for use in large research studies or clinical trials (WHO, 1993). In these instances, assessments will be more willingly incorporated into studies if they are brief, convenient and accurate (Berwick et al, 1991). The most general question from each facet (i.e. the item that correlated most highly with the total score, calculated as the mean of all facets) was chosen for inclusion in the WHOQOL-BREF (WHO, 1998). The panel examined the individual items and established whether the selected to represent each domain, with good construct validity.
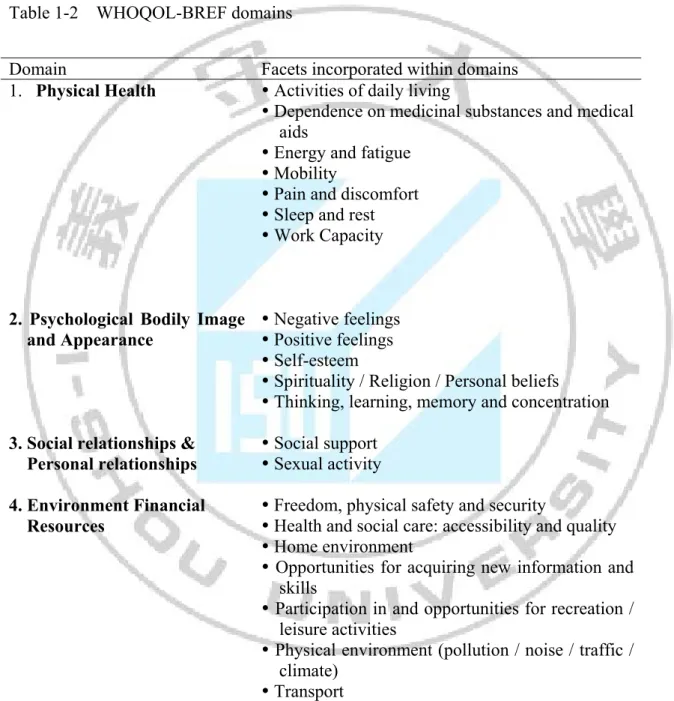
There are four domains with physical domain, psychological domain, social relationship
domain and environment domain. The details were shown in Table 1-2 (WHO, 1996). Of the
twenty six items were selected, and with the Taiwan version, two more questions were added.
- 8 -
Three items from the environment domain were substituted because they were highly correlated with the psychological domain. The WHOQOL-BREF proves useful in health policy research and make up an important aspect of the routine auditing of health and social services (WHO, 1998).
Table 1-2▓WHOQOL-BREF domains
Domain Facets incorporated within domains 1. Physical Health Activities of daily living
Dependence on medicinal substances and medical aids
Energy and fatigue
Mobility
Pain and discomfort
Sleep and rest
Work Capacity
2. Psychological Bodily Image and Appearance
Negative feelings
Positive feelings
Self-esteem
Spirituality / Religion / Personal beliefs
Thinking, learning, memory and concentration 3. Social relationships &
Personal relationships
Social support
Sexual activity 4. Environment Financial
Resources
Freedom, physical safety and security
Health and social care: accessibility and quality
Home environment
Opportunities for acquiring new information and skills
Participation in and opportunities for recreation / leisure activities
Physical environment (pollution / noise / traffic / climate)
Transport
Source: WHO (1997), http://www.who.int/mental_health/media/68.pdf
- 9 -
1.4▓Societal impact of aging
Nowadays, population aging is driven by declines in fertility and improvements in health and longevity. The proportion of the elderly in the total population increases significantly.
While some countries such as Europe currently have four people of working age for every older person, it will have only two workers per older person by 2050 (NIH, 2007). In 1950, 1 in 15 persons (6.7%) aged 60 or older in the world. In 2000, approximately 10% of the world’s people were 60 years old or older. Population aging is the fastest in low-fertility countries. Today, 11 per cent of the population in low-fertility countries is 65 years or over. In 2050, the percentage is expected to be 26 per cent for this age group (United Nations, 2011).
A study from the Council for Economic Planning and Development, ROC (2010), showed the elderly population in Taiwan with more than 65 years old will increase to 13.6%
by 2015, the numbers of elderly people is expected to be 7 millions, which the elderly people in Taiwan will increase to 35.9% by 2050. According to the Ministry of Interior, the latest survey done by Department of Statistic, the registered elderly people in Taiwan by December of 2010, were 2,487,893 comprised of 10.74% of total population and the aging index was 68.64%.
The increase of the aging population in the society will definitely cause an impact on the economic, political and social conditions. For an example, economic expansion could be hampered as businesses or industrial struggle to attract new workers. This could be due to the working-age population, which contributes to economic growth and the pension system, is shrinking at the same time that the older, nonworking population is increasing. For instance, one of the great urgency to harmonize with the coming aging society is to change the social system such as retirement, pension, and medical care.
Four-generation families become more common as the life expectancy of the human
being rises. Some researchers estimate that, between year 2005 and 2030 the odds of living
from birth to age 100 may have risen from 1 in 20 million to 1 in 50 for females in
- 10 -
low-mortality nations such as Japan and Sweden (NIH, 2007). The working adults will definitely feel the financial pressures of supporting both their children and older parents and possibly grandparents simultaneously. Moreover, the oldest old always have the highest population levels of disability that might require a high cost long-term care. While much of this health care costs spending reflects the reality that incidence of illness is associated with aging. Besides, the cost of health care is staggering. The cost including spending on physician office visits, prescriptions and over the counter medication, as well as hospital visits. The health care costs continue to consume and increasing share of income and economic resources.
These costs including the long term care services cost, which could be the single greatest threat to the financial security of older people. There will be a great influence on the economics of a country as in these costs including Medicare will not only cause the burden to the family, but also the society and the country. The support of the older adults by the country is a concern, where life expectancy increases and the pensions and retirement income provided will need to be covered a longer period of life.
As the aging population increasing, the growing of the senior housing has become the
priority domestic issue for the country. Housing could play a unique role by providing a sense
of comfort and security as well as shelter. Indeed, older people’s living arrangements reflect
their need for family, community, or institutional support. Elderly people could spend their
lives with neighborhood. Besides, living arrangements also indicate sociocultural
preferences—for example, some choose to live in nuclear households while others prefer
extended families. Generally, the living arrangements (place of stay) for the elderly is divided
into home-dwelling (staying with family or alone), senior apartment, and institution-based
seniors’ home, and nursing home with specialized care in Taiwan. Research in many cultural
settings showed that older people prefer to be in their own homes and communities and this
was reinforced by an emphasis in many nations on community care (NIH, 2007). Besides, the
home care is much less expensive than institutional care. As suggested by United States and
their local government, 3 features installed in new houses to build accessible communities so
that people could live independently in their home as long as possible. These 3 features
include 1) no steps at entrance, outlet at wheelchair levels; 2) a bathroom with a grab bar on
the ground floor and; 3) wider doorway (Robinson & Reinhard, 2009). These housing trends
- 11 -
allow older adults to live independently rather than having move into an assisted-living facility or nursing home. Universal design is critical to aging with independence (AARP, 2005). Designing and building homes should have met new specifications capable of serving homeowners for a lifetime. It reduces the personal and social costs of having to relocate to institutional living by adding $200 to $1000 to the cost of building a home (Robinson &
Reinhard, 2009). However, nowadays the provision of the care at home is getting more difficult as in the family size decrease and the caregivers (son/daughter) are usually engaged in the employment outside the home. The quality of life and quality of care given could be affected. In some European countries, more than 40 percent of women age 65 and older live alone (NIH, 2007).
Senior apartment for the elderly to stay is gradually set up. However, the senior apartment will or will not provide three meals to the elderly people. Commonly, seniors’
apartment is the residences with limited assistance for individuals and sheltered housing are excluded from the nursing home category. These apartments may not provide nursing care to the residents. The country such as China, there is 1.5% of older people live in nursing homes and apartments (Chu et al., 2008). The policy of the country such as China (Chu et al., 2008) is encouraging the private sector to involve in the setting of the nursing homes or senior apartment and in Taiwan (Ministry of Interior–Social Affairs, 2011) also encouraging the private sector to provide caring services and to share various financial responsibilities.
Institution-based home is a residential home for elderly people (home for the aged) providing living conditions adjusted to the needs of residents usually requiring no more nursing care than can be given by a visiting nurse. In some homes, assistance can be provided for some basic activities of daily living, including assistance with dressing, assistance with mobility from a private room to a communal room for meals and limited assistance with appliances such as urinary catheters. Usually, most care in residential homes is provided by nursing aides and personnel with little or no training. In many countries, residential homes are building complexes (apartment buildings) where elders reside in private apartments or single rooms. Most residents are provided with three meals.
Nursing home is a private residential institution equipped to care for persons unable to
- 12 -
look after themselves, as they aged or chronically ill. Most nursing homes have nursing aides and skilled nurses on hand 24 hours a day where the medical care is provided. Some nursing homes have special care units for people with serious memory problems such as Alzheimer's disease. Nursing homes can be (NIH, 2009): 1) Hospital-like: It is often set up like a hospital.
Staffs give medical care, as well as physical, speech, and occupational therapy. There can be a nurses’ station on each floor. 2) Household-like: The facilities are designed to be more like homes, and the day-to-day routine isn’t fixed. Teams of staff and residents try to create a neighborhood feel. Kitchens are often opened to residents, decorations give a sense of home, and staffs are encouraged to develop relationships with residents. Some nursing homes have visiting doctors who see their patients on site. Between 2% and 5% of elderly people reside in nursing homes. Interestingly, Iceland, as the youngest country in this study, has the highest rate of institutionalization (living in residential or nursing homes), while the “oldest country”
(Sweden) has a low rate of institutionalization. In the early 1990s comparison of the people aged 65 years and above living at home and in institutions (refers to Table 1-3) (Ribbe et al., 1997).
Nowadays, the elderly people in Taiwan prefer to stay at home with their children.
According to the Ministry of the Interior- Department of Statistic, Taiwan, the ideal living arrangement for the elderly is living with children 68.5%, with couples or de facto partners 15.6%. The willingness of the elderly people to stay in institution based home, senior apartment were 42.4% and 19.5% respectively. They were only willing or agree to stay in nursing home, or long term care home, if they are disabled. However, there were trends of increasing the number of nursing home set up (refer table 1-4). Although there were 97.1% of the elderly people who is more than 65 years old and above had children. The main type family was 3 generations family 37.9%, 2 generations family 29.8%, staying alone 9.2%, and institution based home 2.8%. There were 16.8% of the elderly people who had difficulty in management of the daily living activities, had been mainly taking care by their children (including daughter-in-law, son-in-law) 48.5%, 20.2% taking care by couples, and 16.6% by the local carer or foreign carer.
Another statistic done by Ministry of Interior, Taiwan, by end of the year 2010, the long
term care facility comprised of 963 nursing homes, 90.25%, (provide 43,523 elderly people
- 13 -
staying), and the rate of utilization was 76.93%. 48 assisted living facilities provide 2,484 people staying, and rate of utilization was 70.93%. 42 of the residential care home also belong to the long term care facility, provide 9,059 people staying, and the rate of utilization was 69.24%. The rate of utilization of community based residential home and senior apartment was relatively low 13.37% and 43.50% respectively.
As a person ages, the significance of home and its immediate vicinity increases along with the person’s growing sensitivity and response to environmental changes (Juvani, Isola, Kyngas, 2005). The physical environment includes concrete features, such as the climate, residential milieu and nature may have an influence on older people’s health. These attributes can be used to define the factors that contribute to the subjective environmental experiences of elderly people. The safety of the physical environment has been studied particularly from the viewpoint of anticipating and preventing falling accidents among elderly people, because, as people age, decrements in sensory, motor and cognitive functions often jeopardize their ability to manage, safely and comfortably, the activities of daily living in their own homes.
Noted by Grindley & Zizzi (2005) a safe environment is very important for the self-care of
elderly people living at home. The self-care of elderly people has a great influence on their
quality of life.
- 14 -
Table 1-3▓Percentage of people >65 years living at home and in institutions by countries (prevalence data; different years in the early 1990s) Place of residence USA Japan Iceland Sweden Denmark Netherlands UK France Italy
*Own home - 94.0 87.0 94.0 85.0 90.0 93.0 94.0 96.0
** Residential homes 1.5 0.5 5.0 3.0 10.5 6.5 3.5 4.0 1.0
***Nursing homes 5.0 1.5 8.0 2.0 4.0 2.5 2.0 - <2.0
****Hospitals - 4.0 - <1.0 <1.0 <1.0 1.5 - 1.0
*Own home: homes for the aged, old people's homes (low levels of care)
** Residential homes: independently or with informal and/or formal care (including domestic help and home nursing)
***Nursing homes: high levels of care
****Hospitals: intensive medical care
Source: Ribbe, Ljunggren, Steel, et al. (1997), p6
- 15 -
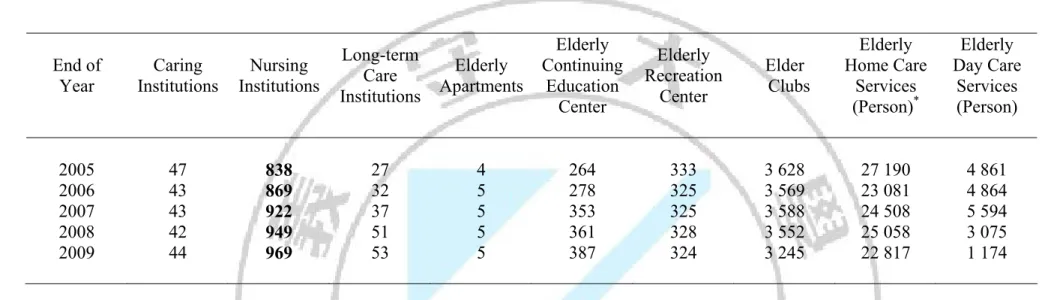
Table 1-4▓Elderly social welfare in Taiwan
End of Year
Caring Institutions
Nursing Institutions
Long-term Care Institutions
Elderly Apartments
Elderly Continuing
Education Center
Elderly Recreation
Center
Elder Clubs
Elderly Home Care
Services (Person)
*Elderly Day Care
Services (Person)
2005 47 838 27 4 264 333 3 628 27 190 4 861
2006 43 869 32 5 278 325 3 569 23 081 4 864
2007 43 922 37 5 353 325 3 588 24 508 5 594
2008 42 949 51 5 361 328 3 552 25 058 3 075
2009 44 969 53 5 387 324 3 245 22 817 1 174
*For entry Day Care Service, the serviced number of people from 2003 to 2007 included normal and disabled elders. To comply with the Ten-year Plan for Long-term Care in Taiwan, Ministry of Interior modified the home care serviced number of people in 2009 in order to focus on disabled elders only.
Source: Ministry of Interior-Social Affairs (2011), http://www.moi.gov.tw/outline/en/en-04.html
- 16 -
1.5▓Aims of the study
The placement of the elderly people could be an issue in facing a rapid aging of population. The development of safe housing and compassionate care for seniors in country such as United States has become a priority domestic issue despite the fastest growing of seniors’ home in nation (Spitzer, Neuman, Holden, 2005). The personal preferences, health care provided and financing support systems could affect the choice of the elderly people residing. Many countries are in the process of health and social care reforms nowadays. The growing of seniors home is fast and also it has to accommodate the changing needs or expectations of the residents and families. The quality of life and satisfy their needs should be emphasized.
To our knowledge, no comparison, cross-sectional or longitudinal study of the quality of life of elderly people with different living arrangements has been conducted in Taiwan.
Herein, the aim of this study is to investigate and to compare the quality of life of the elderly
living at senior apartment, home or the institution-based home. In order to maximize the
quality of life for the elderly people, the study was valuable to investigate how the different
placement settings of elderly people affect their lives. Further investigation involves the
association of the level of dependence, health status and depressive symptoms with the quality
of life in different setting of elderly placement. These comparisons make it possible to
contrast the level of quality of life of the elderly people in different living places arrangements,
providing a basis for making clinical and governmental policy changes.
- 17 -
Chapter▓2 Literature Review
2.1▓Quality of Life of elderly people
In view of aging population increasing projections, the world strives to improve the health and quality of life (QOL) of seniors. Though, it probably involves diverse factors such as the social, political and physical environment. Active aging is the process of optimizing opportunities for health. World Health Organization defined health as, “a state of complete physical, mental and social well-being, not just simply the absence of disease or injury.” Thus, in order to achieve good quality of life and good health, one of the key elements is health promotion. Promoting good health requires a system such as income, supportive neighbors and friends, remaining active, responsive community services, access to amenities, and public transportation that supports seniors in their ability to meet various age-related challenges with comparable resources (Bryant et al., 2002). The system refers to the broader political, social and economic context in which seniors live. These seniors identified issues were possibly important contributors to quality of life. The needs of the senior are complex. The care provided shall accommodate their needs and also focus on quality of life and their well-being.
Quality of Life Research Unit, University of Toronto (2011) suggested, QOL may be conceived as either a desired outcome of health promotion practice, or as a determinant of health among seniors, that is, differentiating between pathological, normal and optimal functioning among seniors. It appears to be a part of the public health planning and practice.
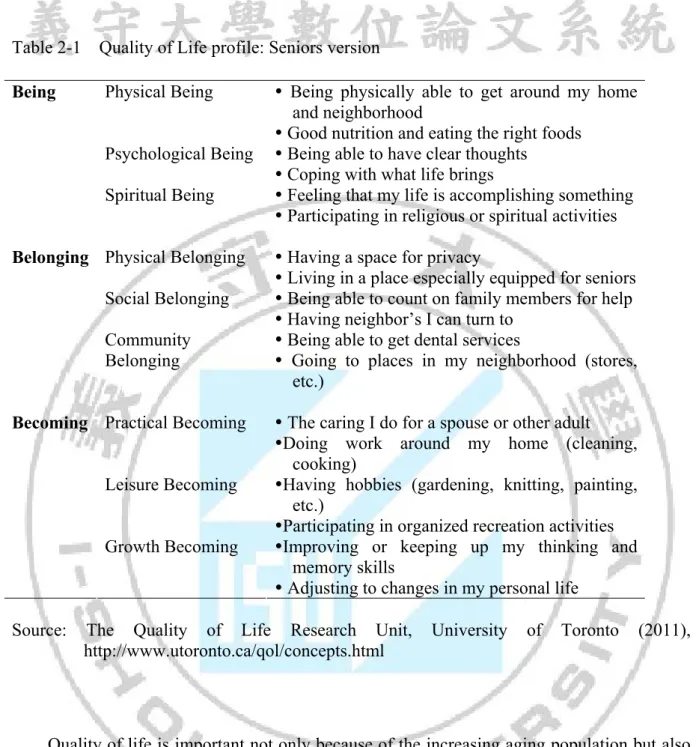
The Quality of Life profile: Seniors version had been developed (Refer to Table 2-1).
- 18 -
Table 2-1▓Quality of Life profile: Seniors version
Physical Being Being physically able to get around my home and neighborhood
Good nutrition and eating the right foods Psychological Being Being able to have clear thoughts
Coping with what life brings Being
Spiritual Being Feeling that my life is accomplishing something
Participating in religious or spiritual activities Physical Belonging Having a space for privacy
Living in a place especially equipped for seniors Social Belonging Being able to count on family members for help
Having neighbor’s I can turn to Belonging
Community Belonging
Being able to get dental services
Going to places in my neighborhood (stores, etc.)
Practical Becoming The caring I do for a spouse or other adult
Doing work around my home (cleaning, cooking)
Leisure Becoming Having hobbies (gardening, knitting, painting, etc.)
Participating in organized recreation activities Becoming
Growth Becoming Improving or keeping up my thinking and memory skills
Adjusting to changes in my personal life
Source: The Quality of Life Research Unit, University of Toronto (2011), http://www.utoronto.ca/qol/concepts.html
Quality of life is important not only because of the increasing aging population but also the quality care of the elderly people; and as an indicator of well-being or satisfaction of life.
There were over 100 definitions and models of QOL (Cummins, 1997), and more than 1000 measures of various aspects of QOL (Hughes and Hwang, 1996). There were senior version of quality of life developed by The Quality of Life Research Unit, University of Toronto which mainly measures the functional status or their ability to participate (refer Table 2-1).
However, our study utilized the WHOQOL-BREF which was shorter and easier for the
elderly people to accomplish compare to the WHOQOL-100 questionnaire.
- 19 -
The quality of life divided into several domains and it is a multi-dimensional broad concepts. There are factors including age, gender, marital status, depression, physical illness, functional status determined to the quality of life. For instance, occurrence of disability and its effects on living conditions are two of the major factors that determine the quality of life of elderly people (Wenger & Burholt, 2003). However, there are other factors would affect the quality of life such as depressive symptoms, number of chronic conditions, military rank for the veterans, and social support (Chang, 2010). Social isolation and loneliness in old age are linked to a decline in both physical and mental well-being. Kondo et al. (2007) found that a higher level of engagement was associated with greater functional capacity, especially social role performance, which means that they have a higher quality of life.
The policymakers not only provide the shelter for the elderly people but also the community support. The elderly people commonly would still face the loneliness, helplessness and boredom no matter they are living with their loving family or in the nursing home. The degree of loneliness depends on the situation. The loneliness is the failure of the social systems. Therefore the social or family support systems are crucial for the well-being of the elderly.
Depression is common in the later life especially in the aged nursing home. Prevalence rates could be range from 2% to 61% (Jongenelis, et al., 2003). In Taiwan, older people who live in nursing homes suffer from more depressive symptoms than those in community dwellings (Chong, 2010). There was another study analyses indicated that men residing within an institution in Canada were significantly more depressed than those residing within detached homes and significantly more depressed than women in both situations (Vallain &
Furac, 1993). Lin, Wang & Huang (2007) study had discovered that the length of residency, number of chronic conditions, perceived health status and the amount of social support from their family and relatives could explain 38.8% of the total variances in depressive symptoms.
The coping strategies such as seeking support from family could help adapting to difficulty aroused from the disability (Hsu & Tung, 2011).
The knowledge such as the causes of health and illness remain relatively unknown to the
public including the senior groups and Bryant et al. (2002) suggested the seniors should be
- 20 -
increased the awareness of developing positive attitudes to life. These involved and increased their social activities (Schroll, Jonsson, Mor, Berg, Sherwood, 1997), and improved outreach efforts to older adults who live alone. Equally important was the need to provide information about aging and retirement. Besides, the filial piety is one of the factors affecting the willingness of children to take care of their elderly parents in the future. However, a decreasing birthrate, rising numbers of women pursuing careers, work pressures, tensions between parents and children, and a weakening in traditional filial piety mores have changed Taiwanese society in recent years (Liu & Huang, 2009). Moreover, there is less possible for the only child or employed children to take care of their parents especially disabled parents.
Such changes may result in poorer levels of family care. Thus, education with emphasis of filial piety should be implemented.
2.2▓Living arrangements and care of elderly people
Elderly people live in a wide range of housing settings-from single family homes, to
full-service retirement communities, to nursing facilities. There are several types of senior
housing or retirement home options for elderly people to choose including active adult
retirement communities, independent living retirement homes, and assisted living facilities,
long term care services in apartment, nursing home or hospital. The utilization rates of the
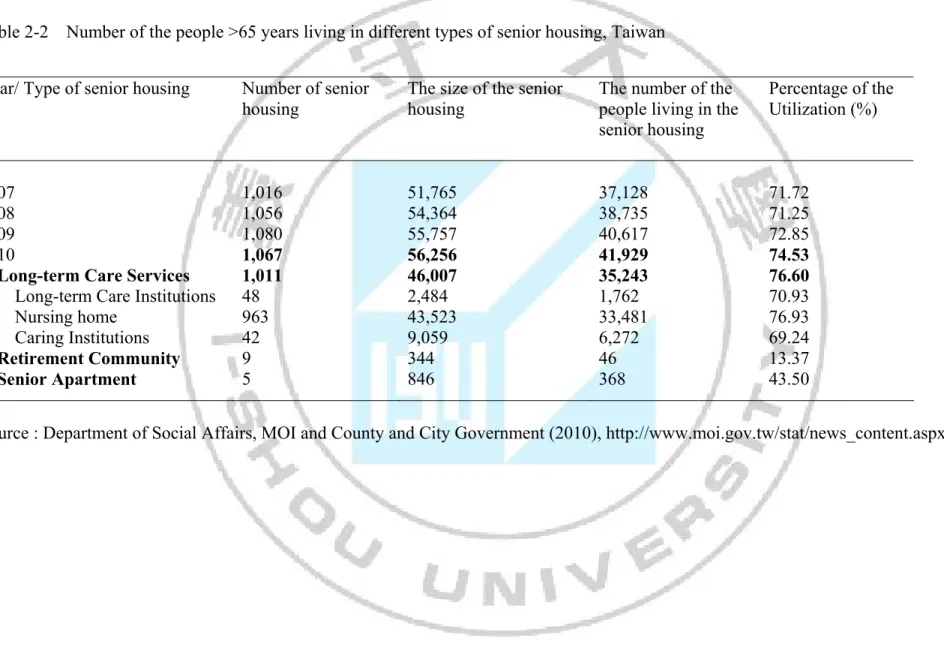
different type of the senior housing or institution in Taiwan were shown in table 2-2.
- 21 -
Table 2-2▓Number of the people >65 years living in different types of senior housing, Taiwan
Year/ Type of senior housing Number of senior housing
The size of the senior housing
The number of the people living in the senior housing
Percentage of the Utilization (%)
2007 1,016 51,765 37,128 71.72
2008 1,056 54,364 38,735 71.25
2009 1,080 55,757 40,617 72.85
2010
Long-term Care Services Long-term Care Institutions
Nursing home Caring Institutions Retirement Community Senior Apartment
1,067 1,011 48 963 42 9 5
56,256 46,007 2,484 43,523 9,059 344 846
41,929 35,243 1,762 33,481 6,272 46 368
74.53 76.60 70.93 76.93 69.24 13.37 43.50
Source : Department of Social Affairs, MOI and County and City Government (2010), http://www.moi.gov.tw/stat/news_content.aspx?sn=5209
- 22 -
As stated in table 2-2, the Department of Social Affairs, Minister of Interiors, Taiwan has divided the senior housing into three types with the low level of care to high level of care.
1. The long term care services (Ministry of Interior-Department of Social Affairs, 2011) includes caring institution, long term care institutions, nursing home or hospital. The designed not only to provide accommodation, but also meals, cleaning and laundry, assistance with showering and dressing, nursing care including medication management, social activities services. The caring institution are designed for the seniors who needs low level care or none of the family member are able to take care of these seniors. Then, they are eligible to apply for the caring institution in Taiwan (refer table 2-2). The long term care institutions are setting up for the chronic conditions elderly people with 24 hours nursing care needed. Nursing homes mainly serve frail elders with chronic diseases, urinary catheters appliances, tube feeding, disabilities, either physical or mental (mainly dementia) or both. These facilities usually provide health care, meals, which can be characterized as the highest level of care.
2. Active adult retirement communities: These communities could be closed off or gated.
They may also have on-site security and even health care. Typically, they are associated with amenities appealing to the newly retired. In Taiwan, the resources from the communities are utilized to set up the housing for the widow or senior who live alone.
There are only 9 retirement communities set up in Taiwan as shown in Table 2-2. However, in other country such as Canada, a country club, golf course, trails, swimming pool, tennis courts, spas, fitness centers and/or a variety of clubs features might be included in the community. Active adult community residences may be suites or condominiums in a tower, detached units, town houses, or bungalows. These are also known as resort communities, 55 plus or adult lifestyle communities (Senior Advisor Care-Comfort Life, 2011). These are ideal for seniors moving through the first phase of their retirement, also well-suited to those who want to leave their retirement options open.
3. Independent living retirement homes: Independent living comes in many different shapes
and forms. Housing arrangements can include suites or apartments in a tower, townhouse
complexes, mobile homes, standard subdivision complexes, bungalow style single
residences or “cluster housing” (Senior Advisor Care-Comfort Life, 2011). Five senior
- 23 -
apartments were set up in Taiwan (refer table 2-2). These homes are ideal for active, healthy, and low care requirement seniors. Usually, there will be a communal area but the size of this may vary greatly. Each unit will almost certainly include its own kitchen, even though the residence may offer communal meals. Independent living retirement homes are most often rentals but they can include subsidized housing. The cost of renting can vary widely depending on real estate costs in the region we are considering as well as services offered. In some cases, we may have the option of purchasing our home. While seniors in independent living homes take care of the majority of their own needs, they may also be provided with meals, laundry services, and linen delivery and planned activities. Many independent living communities provide some form of transportation service to community members.
Independent living communities do not necessarily exclude the option of medical assistance.
Residents may be allowed to hire in their own medical help. Many homes may include assistive technologies such as pull cords and handrails. In general, though, residents are in good health and as implied, they need no help from other people.
The assisted living retirement homes are ideal for seniors who need help with some daily activities such as meal preparation, laundry, shopping and medication but who are not in need of full time care. Other activities include bathing, dressing, toileting or diapering, grooming and other hygiene, meal preparation or cooking, eating, getting around the house, getting around town, housekeeping.
Board and care homes, supervised care facilities, personal care homes, residential care
facilities, domiciliary care, supervised care facilities are called assisted living retirement
homes (Senior Advisor Care-Comfort Life, 2011). Residents may have problems with
memory, incontinence or only mobility. Assisted living can be a more sensible alternative to
home health care. On a continuum of retirement care, assisted living offers more
independence than continued care or traditional nursing homes. It is also less costly than those
options. Assisted living care will cost in the range of $2000 CAD per month in most places
such as in Canada but costs can be much higher for people with high needs. Assisted living
attract residents with a perceived combination of security, personal care services, less
restrictive homelike environments and emphasis on independence, privacy and personal
dignity.
- 24 -
The senior apartment in Kaohsiung City comprises of 180 beds and the Ren-Ai institution-based home consists of 80 beds. Both offer single room or shared rooms only for couples. The current residents in apartment are 130 people and 78 in Ren-Ai home. The building is owned by government and managed by the Buddhist organization-Fo Guang Shan Compassion Foundation. Senior apartment is an independent retirement home. The home is mainly for the active and healthy elderly people. However, the residents are provided with meals, and planned activities. Three meals are provided and the nutritionist will give consultation once a weeks. A special diet could be prepared with the special ordered by the residents due to their conditions such as the vegetarian, soft food. The extra services include the laundry, showering, housekeeping, taking around the medical visit could be provided with the arrangement of the social workers. The assisted living will implied with the extra cost.
The activities including 27 courses to attend per week, the birthday celebration and outdoor activities every two month, is free for the residents to participate. They are encouraged involved with all these activities. A family doctor will come every Thursday. The nurse in the working hours will assist with the blood pressure, temperature measures and simple nursing care. To promote the ageing in place, when the higher level of care is needed, the carer could be employed for daily living assistance without any medical or nursing care.
The institution-based home, caring institution which mainly designed for healthy elderly people but they have no family member or their family members have no ability to take care of them. The setting of the Ren-Ai home is similar to the senior apartment in Kaohsiung City.
There is single or shared room available to be chosen. They have about four regular courses or activities organized per week. The nurse will be in working hours to assist with the elderly people. The family doctor and the doctor from the division of endocrinology and metabolism will come once a week. The hospital, nursing home and long term care institution is situated next door. The setting of the institution combines the personal care services, less restrictive homelike environments and emphasis on independence, and privacy.
The home-dwelling elderly people that participate in our study could stay with family
member, next of kin or live alone. They participate in the activities at least in a week
organized by the community.
- 25 -
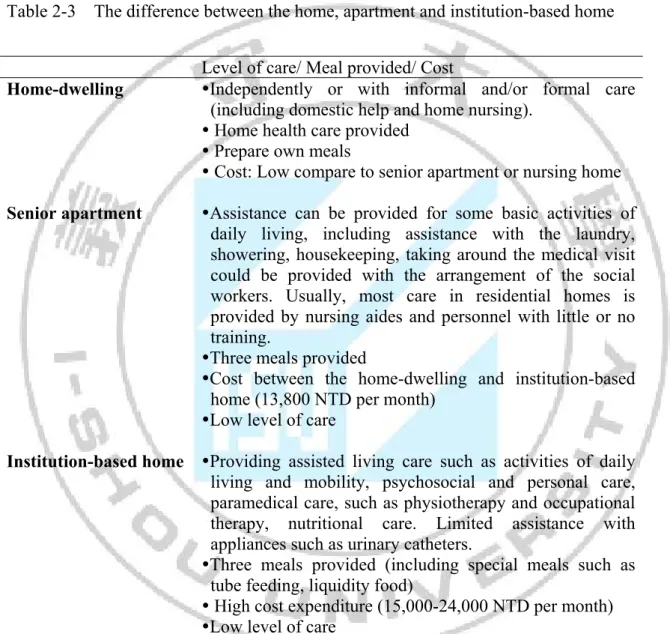
Table 2-3 summarized the difference between the home, apartment and institution-based home. With the right choice of the type of housing or type of care provided should help to reduce certain expenditure. Moreover, the most important is to stay with the enjoyment and freely.
Table 2-3▓The difference between the home, apartment and institution-based home
Level of care/ Meal provided/ Cost
Home-dwelling Independently or with informal and/or formal care (including domestic help and home nursing).
Home health care provided
Prepare own meals
Cost: Low compare to senior apartment or nursing home Senior apartment Assistance can be provided for some basic activities of
daily living, including assistance with the laundry, showering, housekeeping, taking around the medical visit could be provided with the arrangement of the social workers. Usually, most care in residential homes is provided by nursing aides and personnel with little or no training.
Three meals provided
Cost between the home-dwelling and institution-based home (13,800 NTD per month)
Low level of care
Institution-based home Providing assisted living care such as activities of daily living and mobility, psychosocial and personal care, paramedical care, such as physiotherapy and occupational therapy, nutritional care. Limited assistance with appliances such as urinary catheters.
Three meals provided (including special meals such as tube feeding, liquidity food)
High cost expenditure (15,000-24,000 NTD per month)
Low level of care
- 26 -
2.3▓Hypothesis questions
As the aging population increasing dramatically, the higher expectation of the “good life” within societies, has led to the great interest of achievement healthy aging with enjoyment of life, seeking satisfaction or meanings of life for the elderly people. In exploring the importance of QOL domains, Evans et al. (2005) found that family, finances, social life, leisure, health and living arrangements were considered important to over 80% of the elderly people studied. In WHOQOL-BREF the environment domain include the conditions such as noise, pollution, attractiveness, traffic. The perceived quality of neighborhood, facilities such as social leisure, health services, rubbish/liter, cleanliness, transport, closeness to the shop and safety home environment (Beaumont & Kenealy, 2004) are also an important determinant to the quality of life (QOL). The fit between individual’s and their surroundings environment is relevant in planning future residential strategies for the promotion of good quality of later in life (Kalfoss & Halvorsrud, 2009).
H
1: The quality of life is different across institution-based home, senior apartment or staying at home with the different living arrangements.
The prevalence of the old age depression is high especially the residents staying in nursing home (Abrams, Teresi, Butin, 1992). Health events such as physical illness (53.9%) appeared to be the most common and the most widely experienced caused of depression. It then followed by the death of someone with close ties (13.5%), events connected with relationships with children and family members (9.2%), with matters related to money or possessions (6.2%) (Chong, 2001). Health events is highly correlated with the depression state and nursing home (low ADL) has the higher prevalent of depression compare to independent living retirement home (high ADL).
H
2: The disability (Barthel Index of ADL), emotional state (Taiwan Depression
Questionnare TDQ), are significant different in the home-dwelling, institution-based
home or in the senior apartment.
- 27 -
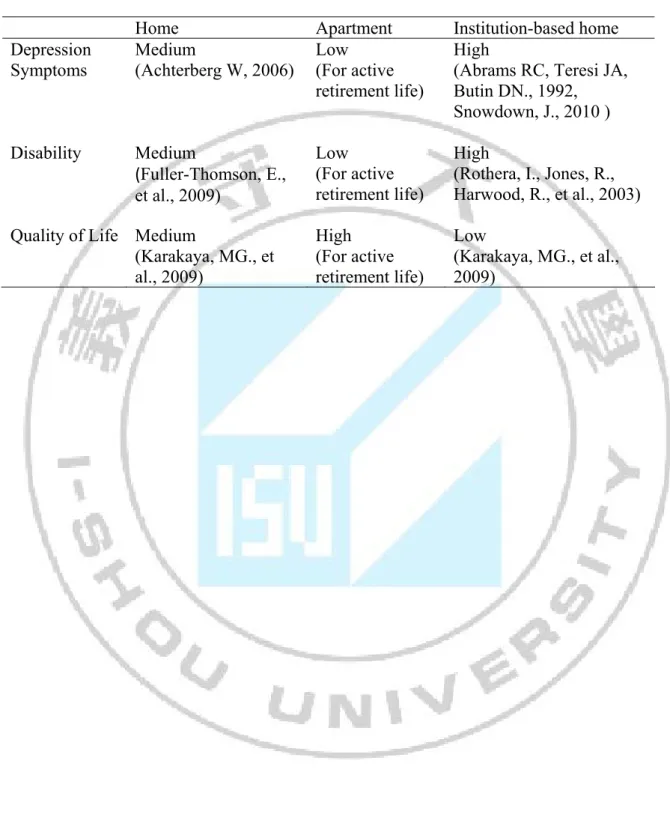
Improvements in assistive technology and environmental accomadation may be enabling persons with more severe disabilities to remain at home as there was a study showed the rates of basic disabilities among American community-dwelling adults aged 65 and older increased 9% between 2000 and 2005 (Fuller-Thomson et al., 2009). Disability is one of the good quality-of-life indicators as it captures both diseased and no diseased person. When institutionalized elders were included, basic Barthel Index of Activities of Daily Living (ADL) disability rates were stable among man but increased among women. In addition, functional mobility and independence level of the nursing home residents were higher than the home-dwelling elderly, but they had more depressive symptoms, and their level of QOL was lower (Karakaya, et al. 2009). Table 2-3 summarized the theoretical model of our study.
H
3: The disability (Barthel Index of ADL) and emotional state (depression scale)
contribute to the quality of life despite the different living arrangement?
- 28 -
Table 2-4▓Theoretical model of the study
Home Apartment Institution-based home
Depression Symptoms
Medium
(Achterberg W, 2006)
Low (For active retirement life)
High (Abrams RC, Teresi JA, Butin DN., 1992, Snowdown, J., 2010 ) Disability Medium
(Fuller-Thomson, E., et al., 2009)
Low (For active retirement life)
High (Rothera, I., Jones, R., Harwood, R., et al., 2003) Quality of Life Medium
(Karakaya, MG., et al., 2009)
High (For active retirement life)
Low
(Karakaya, MG., et al.,
2009)
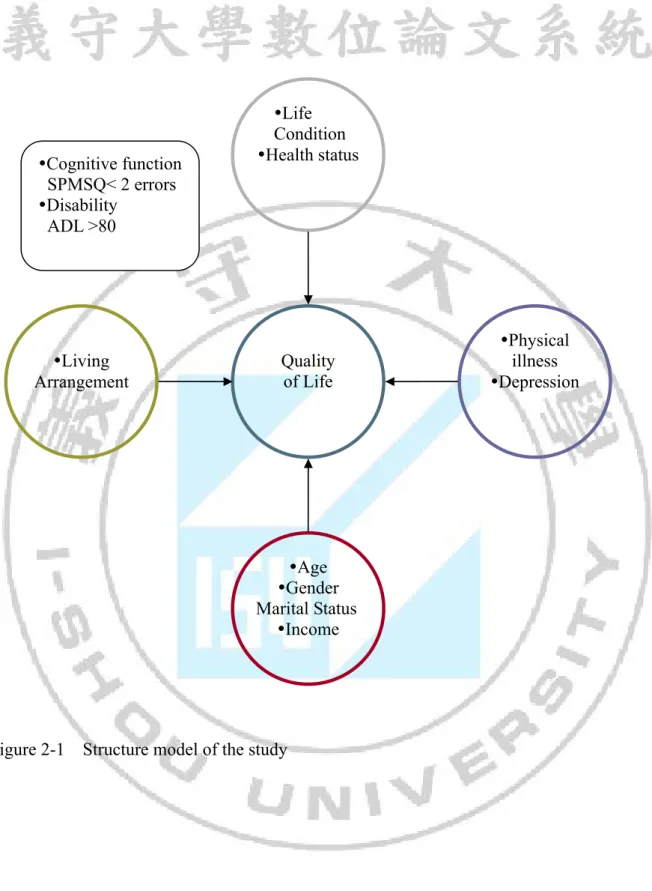
- 29 -
Living Arrangement
Age
Gender Marital Status
Income
Physical illness
Depression
Life Condition
Health status
Quality of Life
Cognitive function SPMSQ< 2 errors
Disability ADL >80
Figure 2-1▓Structure model of the study
- 30 -
Chapter 3▓Materials and Methodology
3.1▓Design
This research is a cross-sectional comparative study. In this study, elderly living in senior apartments, at home, or institution-based home, who fulfilled the inclusion criteria:
participants are more than 65 years old, and volunteered to participate, will be included. The bedridden and dementia elderly were excluded. The procedure of the study involved firstly the literature review, training interviewer, data collection, data analysis, and lastly writing up the conclusion.
The only senior apartment in the Kaohsiung City, institution-based home and home-dwelling elderly were selected for the survey. We recruit all the elderly people with those three different placements and those senior housing situated in Kaohsiung County with the same Medicare reimbursement or system, retirement system, for the elderly people, weather, and cultures. The three group elderly people participated the activity at least once a week. The home-dwelling people will either attend the course in the senior apartment or join the community activity at least once a week. They are either stay with their family member or live alone. They are active and independent. The elderly people in the senior apartment and institution-based may or may not have the assisted daily living care, or nurse care.
The interviewers were trained by the professional doctor for an hour in how to conduct the survey and skills of communicating with the elderly people. They were volunteering for this research. The consistencies of both interviewers are kept by having a discussion for any discrepancies encountered after each section of the survey questionnaires.
3.2▓Participants