Kaohsiung J Med Sci October 2010 • Vol 26 • No 10 567 © 2010 Elsevier. All rights reserved.
Croup, or laryngotracheobronchitis, is generally thought to be a common, short-term and self-limiting illness in children; respiratory distress requires hos-pitalization only in 1.3–2.6% of cases [1], and less than 1% develop severe croup [2]. Here, we describe a 5-year-old boy with recurrent croup and post-obstructive pulmonary edema (POPE). The rapid resolution of his illness, its differential diagnosis, and effective treatment are also discussed.
C
ASEP
RESENTATIONA previously healthy 5-year-old boy developed acute dyspnea in the middle of the night and was sent to our emergency room within a few minutes. He had no history of fever or other illness, but a 2-day history
of cough. In the emergency room, he was noted to be slightly drowsy, with a pulse rate of 120 beats/ min, respiratory rate of 40 breaths/min, blood pressure of 116/44 mmHg, temperature of 36.8°C, and pulse oximetry of 44% in room air. Physical examination revealed a child who was slowly responsive to verbal commands. Breath sound was coarse. He had the typi-cal symptoms of croup, including inspiratory stridor, barking cough, subcostal retractions, and a hoarse voice. He was given oxygen via a non-rebreathing mask immediately and treated with nebulized epinephrine, inhaled budesonide and intravenous methylpredni-solone (0.6 mg/kg). Intubation was not attempted by the doctor on duty because the boy’s pulse oximetry increased to 96% and consciousness recovered within several minutes.
Initial venous blood gas analysis revealed: pH 6.93; partial pressure of arterial carbon dioxide, 83.8 mmHg; partial pressure of arterial oxygen, 23.4 mmHg; HCO3–,
18.8 mmol/L; and base excess, −16.5mmol/L. Routine blood analysis showed leukocytosis (24.6× 109/L)
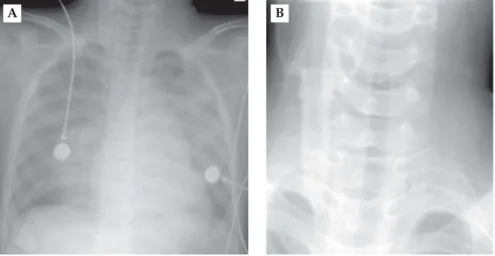
with 37.8% neutrophils and mildly elevated C-reactive protein (14 mg/L). Chest radiography showed bilat-eral alveolar infiltrates in both upper lung fields (Figure 1).
Received: Jan 18, 2010 Accepted: Apr 1, 2010 Address correspondence and reprint requests to: Dr Zen-Kong Dai, Department of Pediatrics, Kaohsiung Medical University Hospital, 100 Shih-Chuan 1stRoad, Kaohsiung 807, Taiwan. E-mail: [email protected]
C
ROUP
-
INDUCED
P
OSTOBSTRUCTIVE
P
ULMONARY
E
DEMA
I-Chen Chen,1Ko-Hsin Chen,1Chien-Ming Tseng,1Jong-Hau Hsu,1,2Jiunn-Ren Wu,1,2and
Zen-Kong Dai1,2,3
1Division of Pediatric Cardiology and Pulmonology, Department of Pediatrics, Kaohsiung Medical
University Hospital, 2Department of Pediatrics, Faculty of Medicine, and 3Department of
Pediatrics, Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung, Taiwan.
Postobstructive pulmonary edema is life-threatening, and results from a sudden episode of upper airway obstruction. Croup is generally thought to be a benign condition, but occasionally it can develop into postobstructive pulmonary edema. We present a case of a 5-year-old boy with recur-rent croup, who was diagnosed with postobstructive pulmonary edema. Our experience alerts pediatricians to this easily misdiagnosed disease.
Key Words:croup, obstructive sleep apnea syndrome, pulmonary edema, respiratory distress
Kaohsiung J Med Sci October 2010 • Vol 26 • No 10 568
I.C. Chen, K.H. Chen, C.M. Tseng, et al
Treatment was continued with nebulized epineph-rine (0.3 mL every 4 hours) and inhaled budesonide (0.25 mg every 12 hours), and antibiotic coverage with cefuroxime was initiated after he was admitted to the pediatric intensive care unit. Arterial blood gas analy-sis at 2 hours after the initial analyanaly-sis showed: pH 7.26; partial pressure of arterial carbon dioxide, 62 mmHg; partial pressure of arterial oxygen, 58 mmHg; HCO3–,
27.8 mmol/L; and base excess, − 0.2 mmol/L. Repeat chest radiography at 12 hours after the initial exami-nation showed dramatic resolution of alveolar infil-trates (Figure 2). Echocardiography revealed normal cardiac function without cardiac anatomical defects. The possibility of upper airway obstruction or for-eign body aspiration was considered, therefore, flexible tracheobronchoscopy was arranged and no foreign body was noted, but adenoid hyperplasia was present. Further history taking revealed that the patient had an episode of croup with respiratory distress 2 months previously. His parents also mentioned that the child had been snoring for 1 year, but they had never noted apnea. Subsequent polysomnography of the patient was normal. He was discharged in a stable condition.
D
ISCUSSIONThe hallmark of croup is subglottic edema that results in varying degrees of airway obstruction. POPE, also named negative pressure pulmonary edema, was first described in 1973 [3]. It is a life-threatening con-dition that results from a sudden, severe episode of
upper airway obstruction (type I), or after surgical relief of chronic upper airway obstruction (type II) [4,5]. The incidence of type I POPE in patients with upper airway obstruction is reported to be 7–12% [6]; the incidence of type II POPE in anesthetic patients is reported to be 0.05–0.1% [7]. The true frequency of type I POPE following croup is not known.
POPE develops when excessive negative intratho-racic pressure is generated by forced inspiration against a closed glottis or obstructed airway [8]. This leads to an increase in venous return to the right heart, which increases pulmonary venous pressure. The in-crease in pulmonary venous pressure creates a hydro-static transpulmonary gradient with fluid moving from the pulmonary veins to the interstitial space.
A B
Figure 1.Chest radiographs demonstrating (A) alveolar infiltrates in both upper lung fields and (B) steeple sign in a 5-year-old boy with acute dyspnea.
Figure 2. Chest radiograph taken 12 hours after initial exam-ination. The radiograph was normal, and there had been rapid resolution of the alveolar infiltrates.
At the same time, low cardiac output might increase afterload. The combination of increased preload and afterload results in a marked increase in hydrostatic pressure in the pulmonary vasculature [9]. The in-creased hydrostatic pressure changes Starling’s force and leads to pulmonary edema. Besides, an acute upper airway obstructive event can lead to severe hypoxia. Severe hypoxia can cause hypoxic pulmonary vasoconstriction, which can lead to hypoxic pulmonary hypertension and right heart failure [10]. Fortunately, the echocardiogram in our patient was normal.
The manifestations of POPE include: (1) signs of upper airway obstruction, such as drooling, hoarseness, stridor, and retractions; and (2) signs of pulmonary edema, such as hypoxemia, frothy sputum (not shown in our patient), and bilateral alveolar infiltrates in upper lung fields on chest radiography. POPE usually occurs within minutes and resolves rapidly within 12–24 hours [5,9,11,12]. Accordingly, our case described above had type I POPE. The common causes of type I POPE include epiglottitis, croup, foreign body aspi-ration and angioedema [7,9]. In our case, epiglottitis and foreign body aspiration could be excluded by the rapid resolution and flexible tracheobronchoscopy. Because of the history of prior respiratory tract infec-tion and the typical symptoms of croup, our patient was diagnosed with croup-induced type I POPE. How-ever, angioedema still cannot be ruled out, although no skin rash was noted on this patient.
On further consideration of this history of POPE and recurrent croup, we thought that obstructive sleep apnea syndrome (OSAS) might be a factor, given the occurrence of two episodes of respiratory distress at night, a 1-year history of snoring, and adenoid hyper-trophy. Our decision to include OSAS in the differential diagnosis was supported by a case report of a previ-ously healthy child with OSAS who developed POPE [13]. In addition, in a study of dogs, recurrent obstruc-tive apnea over an 8-hour period was noted to cause lung edema and deterioration in gas exchange [14]. Fortunately, our patient had normal polysomnography and there was no recurrence of nighttime respiratory distress thereafter. To the best of our knowledge, this is the first report that suggests the need to differentiate OSAS from recurrent croup, which might precipitate POPE, but further studies are warranted.
The treatment of POPE involves early recognition, supportive therapy such as oxygen supplementation by facemask or mechanical ventilation, and treatment
of the underlying disease [5,11]. The use of diuretics in POPE is controversial [11]. As for the treatment of croup, nebulized epinephrine and corticosteroids are the mainstay in relief of airway obstruction [2,15].
In summary, although croup is generally thought to be a benign condition, some cases might develop into POPE. Pediatricians should be alert to this life-threatening and easily misdiagnosed condition.
R
EFERENCES1. Peltola V, Heikkinen T, Ruuskanen O. Clinical courses of croup caused by influenza and parainfluenza viruses.
Pediatr Infect Dis J 2002;21:76–8.
2. Bjornson CL, Johnson DW. Croup. Lancet 2008;371:
329–39.
3. Oswalt CE, Gates GA, Holmstrom MG. Pulmonary
edema as a complication of acute airway obstruction.
JAMA 1977;238:1833–5.
4. Van Kooy MA, Gargiulo RF. Postobstructive pulmonary edema. Am Fam Physician 2000;62:401–4.
5. Mehta VM, Har-El G, Goldstein NA. Postobstructive pulmonary edema after laryngospasm in the otolaryn-gology patient. Laryngoscope 2006;116:1693–6.
6. Galvis AG. Pulmonary edema complicating relief of upper airway obstruction. Am J Emerg Med 1987;5:294–7.
7. McConkey PP. Postobstructive pulmonary oedema—a
case series and review. Anaesth Intensive Care 2000;28: 72–6.
8. Guffin TN, Har-el G, Sanders A, et al. Acute postob-structive pulmonary edema. Otolaryngol Head Neck Surg 1995;112:235–7.
9. Lang SA, Duncan PG, Shephard DA, et al. Pulmonary oedema associated with airway obstruction. Can J
Anaesth 1990;37:210–8.
10. E AM. Hypoxic pulmonary vasoconstriction. Essays
Biochem 2007;43:61–76.
11. Koh MS, Hsu AA, Eng P. Negative pressure pulmonary oedema in the medical intensive care unit. Intensive Care
Med 2003;29:1601–4.
12. Fremont RD, Kallet RH, Matthay MA, et al. Postob-structive pulmonary edema: a case for hydrostatic mechanisms. Chest 2007;131:1742–6.
13. Chowdary YC, Patel JP. Recurrent pulmonary edema: an uncommon presenting feature of childhood obstruc-tive sleep apnea hypoventilation syndrome in an oth-erwise healthy child. Clin Pediatr (Phila) 2001;40:287–90. 14. Fletcher EC, Proctor M, Yu J, et al. Pulmonary edema develops after recurrent obstructive apneas. Am J Respir
Crit Care Med 1999;160:1688–96.
15. Kristjansson S, Berg-Kelly K, Winso E. Inhalation of racemic adrenaline in the treatment of mild and moder-ately severe croup. Clinical symptom score and oxygen saturation measurements for evaluation of treatment effects. Acta Paediatr 1994;83:1156–60.
Croup-induced pulmonary edema
570 Kaohsiung J Med Sci October 2010 · Vol 26 · No 10