Open Access
Research
Relation between air pollution and allergic rhinitis in Taiwanese
schoolchildren
Bing-Fang Hwang
1,2,3, Jouni JK Jaakkola
4, Yung-Ling Lee
2,5, Ying-Chu Lin
6and Yue-liang Leon Guo*
7Address: 1School and Graduate Institute of Occupational Safety and Health, College of Public Health, China Medical University, 91, Hsueh-Shih Road, Taichung, 40402, Taiwan, 2Department of Environmental and Occupational Health, College of Medicine, National Cheng Kung University, 138 Sheng-Li Road, Tainan 704, Tainan, Taiwan, 3Department of Health Care Administration, Diwan College of Management, 87-1, Nansh Li, Madou Jen, Tainan 721, Taiwan, 4Institute of Occupational and Environmental Medicine, The University of Birmingham, Edgbaston, Birmingham B15 2TT, UK, 5Department of Internal Medicine, National Cheng Kung University Hospital, 138 Sheng-Li Road, Tainan 704, Taiwan, 6College of Dental Medicine, Kaohsiung Medical University, 100 Shi-Chuan 1st Road, San Ming District, Kaohsiung City, Taiwan and 7Department of Environmental and Occupational Medicine, National Taiwan University, Taipei 100, Taiwan
Email: Bing-Fang Hwang - [email protected]; Jouni JK Jaakkola - [email protected]; Yung-Ling Lee - [email protected]; Ying-Chu Lin - [email protected]; Yue-liang Leon Guo* - [email protected]
* Corresponding author
Abstract
Background: Recent findings suggest that exposure to outdoor air pollutants may increase the
risk of allergic rhinitis. The results of these studies are inconsistent, but warrant further attention. The objective of the study was to assess the effect of relation between exposure to urban air pollution and the prevalence allergic rhinitis among school children.
Methods: We conducted a nationwide cross-sectional study of 32,143 Taiwanese school children.
We obtained routine air-pollution monitoring data for sulphur dioxide (SO2), nitrogen oxides (NOx), ozone (O3), carbon monoxide (CO), and particles with an aerodynamic diameter of 10 µm or less (PM10). A parent-administered questionnaire provided information on individual
characteristics and indoor environments (response rate 92%). Municipal-level exposure was calculated using the mean of the 2000 monthly averages. The effect estimates were presented as odds ratios (ORs) per 10 ppb change for SO2, NOx, and O3, 100 ppb change for CO, and 10 µg/
m3 change for PM 10.
Results: In two-stage hierarchical model adjusting for confounding, the prevalence of allergic
rhinitis was significantly associated with SO2 (adjusted odds ratio (OR) = 1.43, 95% confidence interval (CI): 1.25, 1.64), CO (aOR = 1.05, 95% CI: 1.04, 1.07), and NOx (aOR = 1.11, 95% CI: 1.08, 1.15). Contrary to our hypothesis, the prevalence of allergic rhinitis was weakly or not related to O3 (aOR = 1.05, 95% CI: 0.98, 1.12) and PM10 (aOR = 1.00, 95% CI: 0.99, 1.02).
Conclusion: Persistent exposure to NOx, CO, and SO2 may increase the prevalence of allergic rhinitis in children.
Published: 09 February 2006
Respiratory Research2006, 7:23 doi:10.1186/1465-9921-7-23
Received: 02 September 2005 Accepted: 09 February 2006 This article is available from: http://respiratory-research.com/content/7/1/23
© 2006Hwang et al; licensee BioMed Central Ltd.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background
The prevalence of allergic rhinitis is increasing among children in many countries [1]. There is accumulating evi-dence that both genetic and environmental factors play important roles in the aetiology of allergic rhinitis. It is likely that there is a multilevel interaction between genetic and environmental factors [2]. Changes in genetic pool are an unlikely to explain changes in the occurrence of allergic rhinitis on short time interval. Therefore, attempts to identify environmental factors are useful for prevention [3]. Identification of indicators for genetic susceptibility to environmental exposures could also be useful from pre-ventive point of view. Recent findings suggest that expo-sure to outdoor air pollutants may increase the risk of allergic rhinitis in children [4-9]. The results of these stud-ies are inconsistent, but warrant further attention. In 1995–1996, Lee et al. studied the association between air pollution and allergic rhinitis in Taiwan. This study of 331,686 children showed a relation between the risk of allergic rhinitis and a score of traffic-related air pollutants derived from municipal concentrations of carbon monox-ide (CO) and nitrogen oxmonox-ides (NOx) [10]. Relations between the prevalence of allergic rhinitis and the concen-trations of individual pollutants were not studied. This study was not able to adjust for parental atopy or indoor exposures, which are potential sources of confounding and effect modification.
In 2001, we conducted a new nationwide cross-sectional study, where we collected information also on those important potential determinants of allergic disease in children. Our primary objective was to assess the relation between exposure to urban air pollution and the preva-lence of allergic rhinitis in schoolchildren, focussing on predominantly traffic-related pollutants such as nitrogen oxides (NOx), ozone (O3), carbon monoxide (CO), pol-lutants from other fossil fuel combustion sources, such as sulphur dioxide (SO2), and particles with an aerodynamic
diameter of 10 µm or less (PM10). In addition, we hypoth-esised that the joint effect of parental atopy and exposure to outdoor air pollution on prevalence of the allergic rhin-itis is more than the expected on the basis of their inde-pendent effects. We assumed that parents with asthma, allergic rhinitis or allergic atopic eczema may give their children genes that increase the susceptibility to the effects of environmental factors on allergic rhinitis.
Methods
Data collection and study population
In 2001, we conducted a nationwide cross-sectional study in Taiwan using a modified Chinese version of The Inter-national Study of Asthma and Allergies in Childhood (ISAAC-C) questionnaire [11]. The questionnaire inquired details of children's health, environmental
expo-sures, and other relevant information. The study popula-tion was recruited from elementary and middle schools in 22 municipalities within one kilometre from a Taiwan Environmental Protection Agency (EPA) air-monitoring station. First, we randomly selected one monitoring sta-tion in each county. We then randomly selected one school next to each monitoring station. Finally, we con-ducted a stratified sampling of the students by selecting 5– 7 classes per grade from each school. The questionnaires were taken home by students and answered by parents. A total of 35,036 children aged 6–15 years were approached. The response rate was 91.7%. We excluded 2,893 children because of incomplete questionnaire and personal history of atopic ecezma. Therefore, the final study population included 32,143 school children. The study protocol was approved by the Respiratory Health Screening Steering Committee of the Taiwan Department of Health and the Institutional Review Board at the National Cheng Kung University Hospital, and it com-plied with the principles outlined in the Helsinki Declara-tion [12].
Health outcome
The outcome of interest was allergic rhinitis, which was defined on the basis of answers to the question: "Has a physician ever diagnosed your child as having allergic rhinitis?" (yes; no). The questionnaire also included a question on the symptoms of allergic rhinitis per se. After primary analyses, we decided to focus on physician-diag-nosed allergic rhinitis.
Physician-diagnosed allergic rhinitis reflects well the occurrence of allergic rhinitis, because Taiwanese children are almost all covered by health insurance (>99%) and there is a good access to health care. Thus children with allergic rhinitis are commonly diagnosed. A history of atopic eczema was defined as the presence of itching skin eruption at cubital, posterior popliteal, neck, periauricle, and eyebrow areas for 6 months or longer and a diagnosis of atopic eczema by physician.
Exposure assessment
Monitoring data for sulphur dioxide (SO2), nitrogen oxides (NOx), ozone (O3), carbon monoxide (CO),
parti-cles with an aerodynamic diameter of 10 µm or less (PM10), as well as for temperature and relative humidity, are available from Taiwan Environmental Protection Agency in 1994 and later years. Concentrations of each pollutant are measured continuously and reported hourly – CO by non-dispersive infrared absorption, NOx by chemiluminescence, O3 by ultraviolet absorption, SO2 by ultraviolet fluorescence, and PM10 by beta-gauge.
Exposure parameters in the present study were annual averages of air pollutants, calculated from the monthly
averages of the year 2000. Exposure assessment was per-formed for children attending schools located within one km of 22 of these monitoring stations.
Covariates
Information on potential confounders was obtained from the questionnaire. The covariates in the present analyses included age, gender, parental atopy, parental education, maternal smoking during pregnancy, and environmental tobacco smoke (ETS), cockroaches noted monthly, water damage and visible mould in the home (Table 1). Paren-tal atopy was a measure of genetic predisposition and was defined as the father or the mother of the index child ever
having been diagnosed as having asthma, allergic rhinitis, or atopic eczema.
Statistical methods
We applied two-stage hierarchical models, which allowed an appropriate adjustment for confounding and effect modification on individual-level and assessment of the effects of air pollution on municipal-level [13,14]. We used odds ratio as a measure of the relation between expo-sure to air pollution and the prevalence of allergic rhinitis. We estimated adjusted odds ratios in a two-stage hierar-chical model using logistic and linear regression analyses. The detail was described elsewhere [15]. The results from
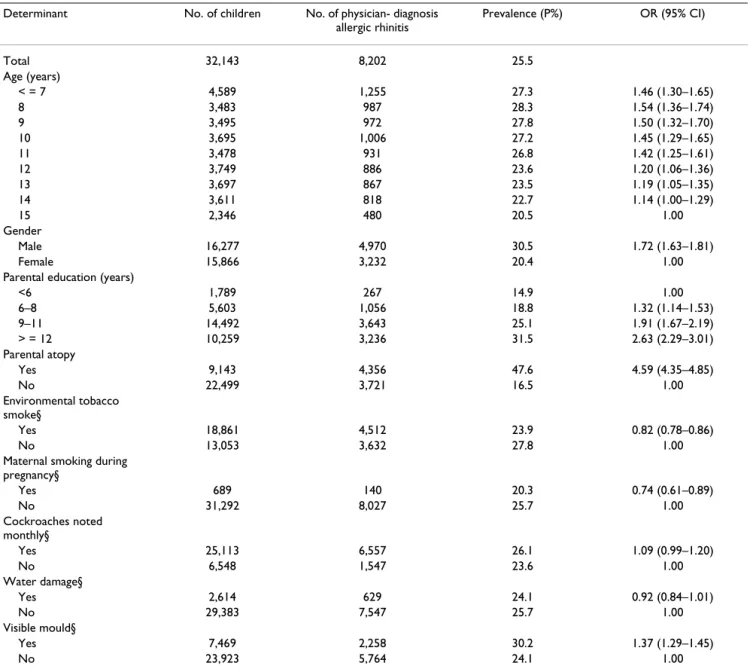
Table 1: Number of children with allergic rhinitis, and prevalence of allergic rhinitis with 95% confidence interval (95% CI) by selected covariates in Taiwan 2001.
Determinant No. of children No. of physician- diagnosis allergic rhinitis Prevalence (P%) OR (95% CI) Total 32,143 8,202 25.5 Age (years) < = 7 4,589 1,255 27.3 1.46 (1.30–1.65) 8 3,483 987 28.3 1.54 (1.36–1.74) 9 3,495 972 27.8 1.50 (1.32–1.70) 10 3,695 1,006 27.2 1.45 (1.29–1.65) 11 3,478 931 26.8 1.42 (1.25–1.61) 12 3,749 886 23.6 1.20 (1.06–1.36) 13 3,697 867 23.5 1.19 (1.05–1.35) 14 3,611 818 22.7 1.14 (1.00–1.29) 15 2,346 480 20.5 1.00 Gender Male 16,277 4,970 30.5 1.72 (1.63–1.81) Female 15,866 3,232 20.4 1.00
Parental education (years)
<6 1,789 267 14.9 1.00 6–8 5,603 1,056 18.8 1.32 (1.14–1.53) 9–11 14,492 3,643 25.1 1.91 (1.67–2.19) > = 12 10,259 3,236 31.5 2.63 (2.29–3.01) Parental atopy Yes 9,143 4,356 47.6 4.59 (4.35–4.85) No 22,499 3,721 16.5 1.00 Environmental tobacco smoke§ Yes 18,861 4,512 23.9 0.82 (0.78–0.86) No 13,053 3,632 27.8 1.00
Maternal smoking during pregnancy§ Yes 689 140 20.3 0.74 (0.61–0.89) No 31,292 8,027 25.7 1.00 Cockroaches noted monthly§ Yes 25,113 6,557 26.1 1.09 (0.99–1.20) No 6,548 1,547 23.6 1.00 Water damage§ Yes 2,614 629 24.1 0.92 (0.84–1.01) No 29,383 7,547 25.7 1.00 Visible mould§ Yes 7,469 2,258 30.2 1.37 (1.29–1.45) No 23,923 5,764 24.1 1.00
the models are presented as odds ratios (ORs), along with their 95% confidence intervals (CIs). First, we fitted sin-gle-pollutant models estimating the increase in adjusted log odds per increase in air pollutant level (Table 4). We then considered two-pollutant models by fitting one traf-fic-related and one stationary fossil fuel combustion-related pollutant. Finally, we also fitted two-pollution models with O3 and another pollutant. The two-pollutant models provide estimates of the independent effects of CO, NOx, SO2, PM10, and O3 on allergic rhinitis control-ling for the other pollutant in the model. The effect of each pollutant on the prevalence of allergic rhinitis was presented as odds ratios (ORs) per 10 ppb change for SO2, NOx, and O3, 100 ppb change for CO, and 10 µg/m3
change for PM10, along with their 95% confidence
inter-vals (CIs). The goodness of fit was assessed with likeli-hood ratio tests (LR) to determine whether a variable contributed significantly to the model.
Results
Study population and occurrence of allergic rhinitis Table 1 displays the characteristics of the study popula-tion and the prevalence of allergic rhinitis according to the covariates. The overall prevalence of allergic rhinitis was estimated as 25.5% (95% CI: 25.0%, 26.0%). The preva-lence of allergic rhinitis was positively associated with age, higher parental education level, male gender, and paren-tal atopy. The prevalence was also related to the presence of cockroaches, although not statistically significantly. There was an association with visible mould in home but not with water damage. In contrast, a negative association was found for environmental tobacco smoke (ETS) and maternal smoking during pregnancy.
Air pollution
Table 2 'see additional file 1' summarizes the distributions of the annual mean air pollutant concentrations, temper-ature and relative humidity in the 22 monitoring stations in the year 2000. The correlations between different pol-lutants are shown in Table 3 'see additional file 2'. The correlation structure is generally consistent with the com-mon sources of the traffic-related pollutants (CO, and NOx) and stationary fossil fuel combustion-related pol-lutants (SO2, and PM10). The correlation between NOx
and CO concentrations was high (0.88), which reflects motor vehicles as the common source. The high correla-tion also implied that only one of the two pollutants could be used as an indicator of traffic-related pollution in the models estimating effects on the prevalence of allergic rhinitis. The correlation of PM10 and SO2 concentrations was also relatively high (0.58) indicating stationary fuel combustion as the common source, although SO2 concen-trations were also correlated with both traffic-related pol-lutants. The concentrations of O3 were negatively correlated with the mainly traffic-related pollutants, but
positively with PM10 and SO2, and it was only weakly cor-related with those of traffic-cor-related and stationary fossil fuel combustion-related air pollutants.
Air pollution and allergic rhinitis
The prevalence of allergic rhinitis was consistently related to the levels of traffic-related pollutants. In the single-pol-lutant model, the adjusted odds ratio for 10 bbp change in NOx was 1.11 (95% CI 1.08–1.15), and the estimate changed little when a second pollutant was added (Table 4: Models 1–3). The adjusted odds ratio for 100 ppb change in CO was 1.05 (95% CI 1.04–1.07) and again addition of SO2 (1.04), PM10 (1.05), or O3 (1.07) had lit-tle influence (Table 4 'see additional file 3' : Models 4, 5 and 6). The adjusted odds ratio for 10 ppb change in SO2
alone was 1.43 (95% CI 1.25–1.64), but inclusion of either of the traffic-related pollutants reduced the effect estimate substantially (Table 4 'see additional file 3' : Models 1 and 4), whereas addition of O3 had little influ-ence (Table 4 'see additional file 3' : Model 7). The preva-lence of allergic rhinitis was not related to PM10 concentrations in any combination of air pollutants (Table 4 'see additional file 3' : Models 2, 5 and 8). In the single-pollutant model, there was no significant associa-tion between O3 and the prevalence of allergic rhinitis, but an addition of either NOx or CO resulted in elevated, sta-tistically significant effect estimates (Table 4 'see addi-tional file 3' : Models 3 and 6).
In summary, positive statistically significant associations were found for SO2, and traffic-related pollutants (CO
and NOx). In contrast, negative or weak associations were found for O3 and PM10.
In order to elaborate the residual confounding and poten-tial effect modification, we systematically conducted strat-ified analyses in different categories of gender, parental atopy, parental education, and presence of exposure to ETS and visible moulds in the home. The stratified analy-ses did not indicate any major residual confounding or effect modification (Table 5 'see additional file 4').
Discussion
In our nationwide cross-sectional study of Taiwanese school children, the prevalence of allergic rhinitis was sta-tistically significantly associated with annual levels of the two traffic-related pollutants, NOx and CO, as well as SO2. The prevalence of allergic rhinitis was inconsistently related to levels of O3 and consistently not related to levels of PM10.
Furthermore, the results did not provide evidence that the joint effect of hereditary atopy representing genetic predis-position and outdoor air pollutants exposure is stronger than expected on the basis of their independent effects.
Validity of results
The exposure assessment was based on routine air-pollu-tion monitoring data. The monitoring data represented reasonably well exposures both in the school and in the home for two reasons. The schools were chosen to be near the monitoring stations. Almost all the children attended schools within one kilometre of their homes, because the density of elementary and middle schools in Taiwan is very high. Finally, the two-stage hierarchical modelling took into account the fact that municipal-level exposure information was used.
The cross-sectional study design is susceptible to selection bias. Parents of children with respiratory problems linked to air pollution could move to residential areas with lower levels of air pollution, which would lead to underestima-tion of the exposure-outcome relaunderestima-tions. Any random migration was likely to result in underestimation of the air pollution effects rather than introducing a positive bias in the associations. Information on residential history in a cross-sectional study or a longitudinal study design is needed to minimise this potential bias.
We were able to adjust for a number of potential individ-ual-level confounders such as parental atopy and educa-tion and central indoor environmental exposures. We also elaborated the possibility of residual confounding by studying the relations of interest in different levels of cov-ariates. Parental education had a positive association with concentrations of traffic-related pollutants. Also the prev-alence of allergic rhinitis was positively associated with the level of parental education (Table 1). Thus parental education was a potential confounder of the relations between air pollution levels and the risk of allergic rhini-tis. To elaborate this, we assessed the relation between air pollution levels and the prevalence of allergic rhinitis on different levels of parental education, and showed that the stratum-specific relations were relatively consistent (Table 5 'see additional file 4'), which reassured that parental education did not act as a confounder.
Urban air pollution constitutes a complex mixture of sev-eral compounds and the assessment of the independent effects of different pollutants is a major challenge, which includes both the issues of confounding and effect modi-fication (joint effect of several compounds). The correla-tions between different compounds are consistent with our knowledge of the sources of air pollution. NOx and CO concentrations were highly correlated representing motor vehicle traffic, whereas SO2 and PM10 concentra-tions were more related to other combustion sources. In the modelling, it was feasible to control for stationary fos-sil fuel pollutants as a potential confounder when assess-ing the effects of traffic-related pollutants and vice versa.
However, due to collinearity problems, it was not possible to separate the effects of traffic-related pollutants from each other (NOx and CO).
Synthesis with previous knowledge
The results of the present study and one previous study from Germany [5], are consistent with the hypothesis that long-term exposure to outdoor air pollutants increases the risk of allergic rhinitis in children. Both studies suggest an increased risk related to traffic-related air pollutants (NOx). In a British study the occurrence of general prac-tise consultations due to allergic rhinitis was related to short-term exposure to SO2 and O3. The strongest associa-tions were found for daily levels during 3 to 4 days prior to consultation [6].
Few air pollution studies have addressed allergic rhinitis as an outcome among children. A German study provided little evidence that exposure to high concentration of SO2, and moderate levels of NOx, and PM10 was related to the
occurrence of upper respiratory symptoms, including runny nose, cough and hoarseness [4]. Another German study indicated that the prevalence of symptoms of aller-gic rhinitis is related to traffic-related outdoor air pollut-ants (NO2) [5]. No association between prevalence of allergic rhinitis and mean SO2, NO2 and O3 was identified in French ISAAC study [7]. A cross-sectional study in Ger-many found no association between traffic-related air pol-lutants and prevalence of atopic symptoms [8]. Another survey conducted in French primary school children reported that the prevalence of atopy was not related to the levels of photochemical air pollutants [9].
Nitrogen dioxide has been shown to be an acute respira-tory irritant in controlled exposure studies [16]. There are no plausible mechanisms through which CO exposure would influence the airways and increase the risk of aller-gic rhinitis. Both NOx and CO represent the complex mix-ture of traffic exhaust, and NO2 is known to be the best
indicator of motor vehicle traffic emissions. In the present study, it was not possible to elaborate to what extent NOx would have direct effects on children airways. CO is unlikely to have any direct effects on the respiratory tract. Our finding of a lack of association between the risk of allergic rhinitis and PM10 levels is consistent with the results from the Harvard 24 Cities Study in North America [17]. Although the risk of allergic rhinitis was not related to the levels of PM10, it is likely that there is an association with fine particulate matter (PM 2.5) and ultrafine parti-cles typically present in motor vehicle exhausts and in par-ticular in diesel exhausts, which can enhance allergic inflammation and induce the development of allergic immune responses. Further studies should assess these relations.
A positive association between the risk of allergic rhinitis and SO2 levels was identified, compatible with a toxico-logical study [18]. SO2 may increase the permeability of the mucous membrane in airways, which may favour the penetration of allergens and the development of allergic reactions. High traffic density is inversely related to con-centrations of ozone (O3) [19], which is formed at some
distance from emission sources and scavenged in city cen-tres by nitrogen monoxide (NO) from vehicle exhaust. The concentrations of O3 were negatively correlated with the mainly traffic-related pollutants (Table 3 'see addi-tional file 2'). The prevalence of allergic rhinitis was asso-ciated with the levels of O3 only when adjusting for a traffic-related pollutant. This is consistent with the hypothesis that the direct emissions from motor vehicles, which scavenge O3 and therefore are negatively associated with O3, are more important determinants of prevalence of allergic rhinitis than the secondary pollutants, such as O3, that are formed downwind. O3 is a known respiratory irritant [20] and could also influence the permeability of the airways mucous membranes contributing to allergic rhinitis.
According to epidemiologic and toxicologic evidence, the World Health Organization (WHO) concluded that traffic related air pollution may increase the risk of allergic devel-opment and exacerbate symptoms in particular in suscep-tible subgroups [21]. Traffic related air pollutants may also increase the risk of non-allergic respiratory symptoms and disease due to their irritative properties [22]. The recent epidemiologic studies suggested that the evidence of the effect of persistent exposure to air pollution on allergic rhinitis still is weak and inconclusive [4-9].
Conclusion
The present study showed statistically significant relations between exposure to outdoor air pollutants and the prev-alence of allergic rhinitis in schoolchildren. The observed relations of the risk of allergic rhinitis to NOx and CO lev-els suggest that emissions from motor vehicles play an important role. In addition, the relation to SO2 levels indi-cates that also other combustion of fossil fuels contribute to adverse health effects.
List of abbreviations used
NOx, nitrogen oxides
PM10, particles with aerodynamic diameter 10 µm or less SO2, sulphur dioxide
O3, ozone
CO, carbon monoxide
ppb, part per billion
Competing interests
The author(s) declare that have no competing interests.
Authors' contributions
Bing-Fang Hwang is responsible for obtained funding, study concept and design, integrity of the data, the accu-racy of the data analysis, and drafting of the manuscript; Jouni JK Jaakkola for planning of the statistical analyses and critical revision of the manuscript for important intel-lectual content; Yung-Ling Lee for data management, data collection, and manuscript comments; Ying-Chu Lin for data collection and manuscript comments; Yueliang Leo Guo for obtained funding, study concept and design, and study supervision. All authors read and approved the final manuscript.
Additional material
Acknowledgements
This study was partially supported by grant #NSC92-2302-B-006-028 from National Science Council and grand #DOH90-TD-1138 from Department of Health, and partially funded by Environmental Protection Administration in Taiwan. Prof. Jouni Jaakkola was partly supported by a grant from the Yrjö Jahnsson Foundation. The third author, Yung-Ling Lee, was also a recipient of the Taiwan National Health Research Institute MD-PhD Pre-doctoral Fellowship (DD9102N).
Additional File 1
Table 2. Annual air pollution and meteorological data from 22 monitor-ing stations in Taiwan, 2000.
Click here for file
[http://www.biomedcentral.com/content/supplementary/1465-9921-7-23-S1.pdf]
Additional File 2
Table 3. Correlations between air pollutants across 22 municipalities.
Click here for file
[http://www.biomedcentral.com/content/supplementary/1465-9921-7-23-S2.pdf]
Additional File 3
Table 4. Adjusted odds ratios (ORs), along with 95% confidence interval (CIs) of physician-diagnosis allergic rhinitis in single and two pollutant models.
Click here for file
[http://www.biomedcentral.com/content/supplementary/1465-9921-7-23-S3.pdf]
Additional File 4
Table 5. Adjusted odds ratios (ORs), along with 95% confidence interval (CIs) of physician-diagnosis allergic rhinitis stratified by different levels of covariates in the relation between allergic rhinitis and air pollutants.
Click here for file
[http://www.biomedcentral.com/content/supplementary/1465-9921-7-23-S4.pdf]
Publish with BioMed Central and every scientist can read your work free of charge "BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime."
Sir Paul Nurse, Cancer Research UK Your research papers will be:
available free of charge to the entire biomedical community peer reviewed and published immediately upon acceptance cited in PubMed and archived on PubMed Central yours — you keep the copyright
Submit your manuscript here:
http://www.biomedcentral.com/info/publishing_adv.asp
BioMedcentral
References
1. The international study of asthma and allergies in childhood (ISAAC) steering committee: Worldwide variation in prevalence of
symptoms of asthma, allergic rhinoconjunctivitis and atopy eczema: ISAAC. Lancet 1998, 351:1225-1232.
2. Kauffmann F, Dizier MH, Annesi-Maesano I, Bousquet J, Charpin D, Demenais F, Ecochard D, Feingold J, Gormand F, Grimfeld A, Lathrop M, Matran R, Neukirch F, Paty E, Pin I, Pison C, Scheinmann P, Verv-loet D, Lockhart A: EGEA (Epidemiological study on the
genet-ics and environment of asthma, bronchial hyperresponsiveness and atopy) – descriptive characteris-tics. Clin Exp Allergy 1999, 29(suppl 4):17-21.
3. D'Amato G: Outdoor air pollution, climate and allergic
respi-ratory disease: evidence of a link. Clin Exp Allergy 2000, 32:1391-1393.
4. von Mutius E, Sherrill DL, Fritzsch C, Martinez FD, Lebowitz MD: Air
pollution and upper respiratory symptom in children from East Germany. Eur Respir J 1995, 8:723-728.
5. Kramer U, Koch T, Ranft U, Ring J, Behrendt H: Traffic-related air
pollution is associated with atopy in children living in urban areas. Epidemiology 2000, 11:64-70.
6. Hajat S, Haines A, Atkinson RW, Bremner SA, Anderson HR, Ember-lin J: Association between air pollution and daily
consulta-tions with general practitioners for allergic rhinitis in London, United Kingdom. Am J Epidemiol 2001, 153:704-714.
7. Ramadour M, Burel C, Lanteaume A, Vervloet D, Charpin D, Brisse F, Dutau H, Charpin D: Prevalence of asthma and rhinitis in
relation to long-term exposure to gaseous air pollutions. Allergy 2000, 55:1163-1169.
8. Hirsch T, Weiland SK, von Mutius E, Safeca AF, Grafe H, Csaplovics E, Duhme H, Keil U, Leupold W: Inner city air pollution and
res-piratory health and atopy in children. Eur Respir J 1999, 14:669-676.
9. Charpin D, Pascal L, Birnbaum J, Armengaud A, Sambuc R, Lanteaume A, Vervloet D: Gaseous air pollution and atopy. Clin Exp Allergy 1999, 29:1474-1480.
10. Lee YL, Shaw CK, Su HJ, Lai JS, Ko YC, Huang SL, Sung FC, Guo YL:
Climate, traffic-related air pollutants and allergic rhinitis prevalence in middle-school children in Taiwan. Eur Respir J
2003, 21:964-970.
11. Asher MI, Keil U, Anderson HR, Beasley R, Crane J, Martinez F, Mitch-ell EA, Pearce N, Sibbald B, Stewart AW, et al.: International study
of asthma and allergies in childhood (ISAAC): rationale and methods. Eur Respir J 1995, 8:483-491.
12. 41st World Medical Assembly: Declaration of Helsinki:
Recom-mendations guiding physicians in biomedical research involv-ing human subjects. Bulletin of the Pan American Health Organization
1990, 24:606-09.
13. Dominici F: Invited commentary: Air pollution and health –
what can we learn from a hierarchical approach? Am J Epi-demilo 2002, 155:11-15.
14. Witte JS, Greenland S, Kim LL, Arab L: Multilevel modelling in
Epidemiology with GLIMMIX. Epidemiology 2000, 11:684-88.
15. Hwang BF, Lee YL, Lin YC, Jaakkola JJK, Guo YL: Traffic related air
pollution as a determinant of asthma among Taiwanese school children. Thorax 2005, 60:467-473.
16. Wang JH, Devalia JL, Duddle JM, Hamilton SA, Davies RJ: Effect of
six-hour exposure to nitrogen dioxide on early-phase nasal response to allergen challenge in patients with a history of seasonal allergic rhinitis. J Allerg Clin Immunol 1995, 96:669-676.
17. Dockery DW, Cunningham J, Damokosh AI, Neas LM, Spengler JD, Koutrakis P, Ware JH, Raizenne M, Speizer FE: Health effects of
acid aerosols on North American children: respiratory symptoms. Environ Health Perspect 1996, 104:500-505.
18. Matsumura Y: The effect of ozone, nitrogen dioxide, and sulfur
dioxide on the experimentally induced allergic respiratory disorders in guinea pigs. Am Rev Respir Dis 1970, 102:430-447.
19. Wjst M, Reitmeir P, Dold S, Wulff A, Nicolai T, von Loeffelholz-Col-berg E, von Mutius E: Road traffic and adverse effects on
respi-ratory health in children. BMJ 1993, 307:596-600.
20. Brunekreef B, Holgate ST: Air pollution and health. Lancet 2002,
360:1233-1242.
21. WHO: Health aspects of air pollution with particulate
mat-ter, ozone and nitrogen dioxide. Report on a WHO working Group
2003 [http://www.euro.who.int/document/e79097.pdf]. Nonn: World Health Organization [Accessed November 2005]
22. Heinrich J, Wichmann HE: Traffic related pollutants in Europe
and their effect on allergic disease. Curr Opin Allergic Clin Immunol