ORIGINAL ARTICLE
Role of Chest Computed Tomography
in Head and Neck Cancer
Yen-Bin Hsu, MD; Pen-Yuan Chu, MD; Juhn-Cherng Liu, MD; Ming-Chin Lan, MD; Shyue-Yih Chang, MD; Tung-Lung Tsai, MD; Jui-Lin Huang, MD; Yi-Feng Wang, MD; Shyh-Kuan Tai, MD
Objectives:To evaluate the role of chest computed tomography (CT) in patients with head and neck squa-mous cell carcinoma (HNSCC) and to determine the optimal timing and predictive factors for positive findings.
Design:Retrospective analysis. Setting:Tertiary referral center.
Patients:Two hundred seventy screening chest CT scans performed in 192 patients with HNSCC during a 42-month period were reviewed.
Main Outcome Measures: The scans were
catego-rized as new cases, follow-up cases, or recurrent cases. The results were classified as abnormal or normal. Scans of patients having a radiologic diagnosis of a malignant neoplasm of the lung or an indeterminate lesion were con-sidered abnormal. Factors correlating with an abnormal chest CT scan or development of malignant neoplasm of
the lung were analyzed, including the timing of imaging and the patients’ clinicopathologic data.
Results: Seventy-nine scans (29.3%) were considered abnormal. The rate of an abnormal scan was signifi-cantly higher in the follow-up case group (44.2%) than in the new case group (14.2%) (P⬍.001). Ten of 15 in-determinate scans (66.7%) with small (⬍1 cm) solitary pulmonary nodules showed disease progression on sub-sequent follow-up scans, changing the patients’ diag-noses to a malignant neoplasm of the lung. The predic-tive factors for development of a malignant neoplasm of the lung were initial N2 or N3 disease, stage IV disease, recurrent disease, and distant metastasis to another site. Conclusions:Chest CT is recommended for high-risk patients, especially during the follow-up period. Inten-sified evaluation and management are mandatory for in-determinate small solitary pulmonary nodules because of the high rate of malignant neoplasms.
Arch Otolaryngol Head Neck Surg. 2008;134(10):1050-1054
T
HE DEVELOPMENT OF A MA-lignant neoplasm of the lung, including distant me-tastasis and second pri-mary cancer, is an impor-tant factor that limits the survival of patients with head and neck squamous cell carcinoma (HNSCC). The most common site of distant metastasis is the lungs,1,2with an incidence of 8% to 15% in clinical stud-ies.1-3Primary lung cancers account for 23% of second primary tumors in pa-tients with HNSCC.4Because the pres-ence of a malignant neoplasm of the lung may alter the case management, evalua-tion of the chest condievalua-tion is important for patients with HNSCC at the initial diag-nosis and during the follow-up period.
Chest radiography is the most com-mon screening tool for many patients with HNSCC, but its sensitivity for early chest lesions is far from satisfactory.2,5-7Chest computed tomography (CT) is a sensi-tive tool for the detection of pulmonary lesions.5However, routine screening by chest CT in patients with HNSCC is
con-troversial, and the cost-effectiveness and optimal timing for this imaging are not clearly defined.6,8-10The objective of this study was to review the results of a screen-ing chest CT in patients with HNSCC at Taipei Veterans General Hospital during a 42-month period. The rates of an abnor-mal chest CT scan at different times of imaging were analyzed. Possible predic-tive factors for the development of a ma-lignant neoplasm of the lung were also ex-plored to guide appropriate use of chest CT in the future.
METHODS
STUDY DESIGN
The computer database of Taipei Veterans Gen-eral Hospital, Taipei, Taiwan, between Febru-ary 1, 2002, and July 31, 2005, was searched for all chest CTs performed in patients with HNSCC. Patients with primary tumors origi-nating at the nose, paranasal sinuses, or naso-pharynx and patients with carcinoma of un-known primary site were excluded from this study. To explore the role of chest CT for Author Affiliations:
Department of Otolaryngology, Taipei Veterans General Hospital (Drs Hsu, Chu, Lan, Chang, Tsai, Huang, Wang, and Tai), and Department of Otolaryngology (Drs Hsu, Chu, Lan, Chang, Tsai, and Tai) and Institute of Clinical Medicine National Yang-Ming University, (Drs Hsu, Lan, Tsai, Wang, and Tai), Department of
Otolaryngology, Taipei Medical University Wan Fang Hospital (Dr Hsu), and Department of Radiology, China Medical University Hospital, Taichung (Dr Liu), Taiwan.
screening purposes, 1 or multiple scans of the same patient were included until any abnormal finding was found. Subsequent fol-low-up chest CT scans after an abnormal finding were ex-cluded from statistical analyses in this study.
Two hundred seventy chest CT scans that were performed as part of tumor surveillance in 192 patients with biopsy-proven HNSCC were obtained during the 42-month period. Ac-cording to the timing of the CT, the scans were divided into the following 3 groups: new cases (n = 134), follow-up cases (n = 52), and recurrent cases (n = 84). Chest CT in the new case group was performed within 2 weeks before the initial treat-ment of HNSCC. The follow-up case group included scans per-formed in patients without evidence of relapse during the fol-low-up period. The median intervals between the diagnosis of the primary tumor and the chest CT were 8 months (range, 1-50 months) for the follow-up case group and 10 months (range, 2-70 months) for the recurrent case group. All chest CTs were performed using contiguous axial 5- to 8-mm section thick-ness through the lungs (LightSpeed and HiSpeed; GE Medical Systems, Milwaukee, Wisconsin) after intravenous adminis-tration of contrast medium. Conventional lung and mediasti-nal thoracic views were surveyed. Chest radiographs within 1 month before chest CT were available in 266 of 270 studies.
IMAGE INTERPRETATION
Radiology reports of all imaging studies were collected and fur-ther reviewed togefur-ther by radiologists, oncologists, and head and neck surgeons (some of whom included the following au-thors, J.-C.L., Y.-B.H., P.-Y.C., T.-L.T., J.-L.H., Y.-F.W., and S.-K.T.). The initial results of the chest CT were classified as ab-normal or ab-normal. Abab-normal results included a malignant neoplasm of the lung and an indeterminate lesion, as both find-ings contribute to possible modifications of case manage-ment. The radiologic criteria2,6,11and the patient distribution of abnormal chest CT scans are listed inTable 1. Scans dem-onstrating a radiologic diagnosis of lung metastasis or second-ary primsecond-ary lung cancer were included in the category of ma-lignant neoplasm. Indeterminate lesions were considered benign if they were stable or decreased in follow-up scans. If indi-cated, the neoplastic nature of the CT results was confirmed by follow-up scan 3 to 6 months later or by pathologic find-ings on endoscopic or CT-guided needle biopsy. Images with-out any of the listed findings were considered normal.
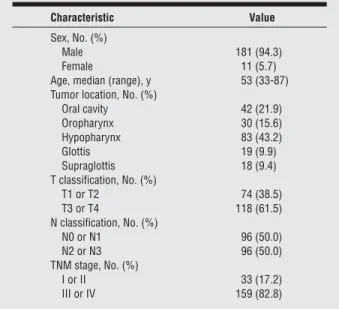
During the study, the use of chest CT mainly depended on physician choice. Among 192 patients with HNSCC, 159 (82.8%) were advanced cases (stage III or IV) according to the 2002
American Joint Committee on Cancer staging system.12All pa-tients underwent detailed history taking, physical examina-tion, and comprehensive tumor surveys, including chest radi-ography, abdominal ultrasonradi-ography, and bone scintigraphy. Further investigation and consultation were arranged as nec-essary to ensure that patients had no other primary malignant neoplasms that had metastasized to the lungs. Medical rec-ords and radiology and pathology reports were reviewed, and the characteristics of 192 patients with HNSCC are summa-rized inTable 2.
DATA ANALYSIS
Statistical analyses were performed to determine the associa-tion between variables and an abnormal chest CT scan or de-velopment of malignant neoplasm of the lung.2Test or Fisher exact test was used for univariate analysis. Variables analyzed included timing of imaging, history of cigarette smoking, pri-mary tumor location, T and N classifications, locoregional re-currence, and distant metastasis to another site. For patients with primary tumor treated by surgery, pathologic variables of the primary tumor or neck metastasis were analyzed where ap-propriate, including perineural invasion, lymphovascular per-meation, surgical margin, and extracapsular spread (ECS) of neck metastasis. Multivariate analysis was performed using a logistic regression model and inclusion of the significant fac-tors on univariate analysis. All analyses were performed using commercially available statistical software (SPSS version 12.0; SPSS, Inc, Chicago, Illinois).
RESULTS
CHEST CT
According to the radiologic criteria, 79 of 270 chest CT scans (29.3%) were initially considered abnormal, in-cluding 54 manifesting a malignant neoplasm of the lung (20.0%) and 25 manifesting indeterminate lesions (9.3%). All malignant neoplasms occurred within the lungs, and no isolated mediastinal lymph node metastasis was found. Table 1. Radiologic Criteria and Distribution of Abnormal
Chest Computed Tomographic (CT) Scans
Radiologic Finding
No. of Scans Malignant neoplasm of the lung
Multiple mostly smooth and peripheral nodules (without clinical symptoms of infection)
49 Lesions with bony destruction 1 Mediastinal lymph nodesⱖ1 cm 0 Solitary, spiculated, and centrally located
lesionsⱖ1 cm 4
Indeterminate lesiona
Small (⬍1 cm) solitary pulmonary nodules 15 Multiple air-space opacities with difficulty in distinguishing
infectious processes from metastases radiologically
10
aAll patients with indeterminate lesions had a follow-up CT scan 3 to 6
months later.
Table 2. Characteristics of 192 Patients With Head and Neck Squamous Cell Carcinoma
Characteristic Value Sex, No. (%)
Male 181 (94.3)
Female 11 (5.7)
Age, median (range), y 53 (33-87) Tumor location, No. (%)
Oral cavity 42 (21.9) Oropharynx 30 (15.6) Hypopharynx 83 (43.2) Glottis 19 (9.9) Supraglottis 18 (9.4) T classification, No. (%) T1 or T2 74 (38.5) T3 or T4 118 (61.5) N classification, No. (%) N0 or N1 96 (50.0) N2 or N3 96 (50.0) TNM stage, No. (%) I or II 33 (17.2) III or IV 159 (82.8)
Besides chest lesions, additional findings were noted on 7 chest CT scans, including 4 liver, 2 adrenal gland, and 1 peripancreatic lymph node metastases. Seventy-five ab-normal chest CT scans had antecedent chest radiogra-phy, but only 21 (28.0%) identified the lung lesions.
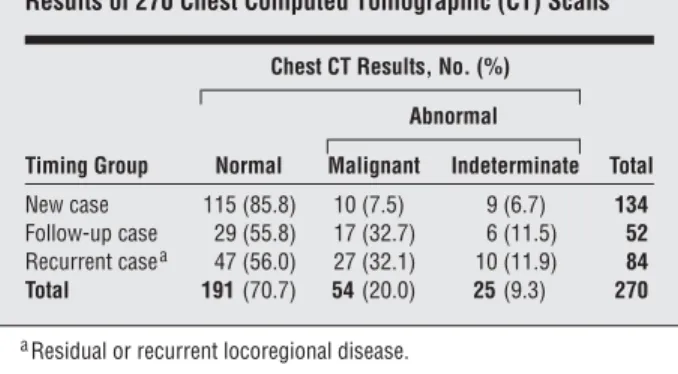
The correlations between the timing of CT and the re-sults are summarized inTable 3. The rate of an abnor-mal scan was significantly higher in the follow-up case group (44.2%) than in the new case group (14.2%) (P⬍.001) and was comparable in the follow-up case group and in the recurrent case group (44.0%). Of 54 scans dem-onstrating a malignant neoplasm of the lung, histologic confirmation by endoscopic or CT-guided needle bi-opsy was obtained in 4 patients with a solitary lesion larger than 1 cm. Most of the scans in 49 patients with mul-tiple pulmonary nodules on chest CT were considered radiologically unequivocal, and only 8 (16.3%) under-went biopsy for tissue confirmation. On subsequent clini-cal and radiologic follow-up, 2 CT scans were consid-ered false-positive results because lesion regression was found without any systemic treatment.
CASE MANAGEMENT ALTERATIONS Among 54 patients with the diagnosis of malignant neo-plasm of the lung by initial chest CT, 45 patients (83.3%) had major alterations in their case management. Instead of curative treatment, 34 patients received chemotherapy alone, and 7 patients underwent chemoradiotherapy for pal-liation. Only 4 patients received aggressive wedge resec-tion of malignant neoplasms of the lung followed by post-operative chemotherapy. The remaining 9 patients refused any treatment, although palliative chemotherapy was sug-gested. Excluding 2 cases with false-positive results, only
1 patient who received wedge resection and postoperative chemotherapy achieved ultimate disease control.
Among 25 patients with indeterminate lesions on ini-tial chest CT, 2 underwent CT-guided biopsy, and both had histologically negative results. A follow-up chest CT was performed 3 to 6 months later in all 25 patients, and pro-gression of the pulmonary finding was shown in 11 pa-tients (44.0%), changing the diagnosis to a malignant neo-plasm of the lung (Table 4). Initial indeterminate lesions manifesting as small solitary nodules had a significantly higher chance of developing into malignant neoplasm of the lung (66.7%) than indeterminate lesions manifesting as multiple air-space opacities (10.0%) (P=.01).
PREDICTORS OF A MALIGNANT NEOPLASM OF THE LUNG
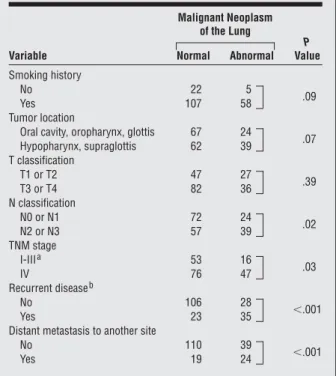
Sixty-three of 192 patients with HNSCC (32.8%) even-tually developed a malignant neoplasm of the lung. The median interval between the diagnosis of primary HNSCC and the development of a malignant neoplasm of the lung was 9.9 months (range, 1.7-59.7 months). Eighty-four percent of the malignant neoplasms of the lung devel-oped within 2 years. Univariate analysis results for the development of a malignant neoplasm of the lung rela-tive to clinicopathologic factors are summarized in Table 5. N2 or N3 disease (P =.02) and stage IV disease (P =.03) were significantly correlated with the develop-ment of a malignant neoplasm of the lung. Recurrent lo-coregional disease (P⬍.001) and distant metastasis to an-other site (P⬍.001) were also significant predictors for the development of a malignant neoplasm of the lung. Patients with a smoking history (P =.09) or with pri-mary sites at the hypopharynx and supraglottis (P =.07) had a trend to development of a malignant neoplasm of the lung that was statistically nonsignificant. In multi-variate analysis, recurrent locoregional disease, N2 or N3 disease, and distant metastasis to another site remained independent predictors for the development of a malig-nant neoplasm of the lung (Table 6).
Histopathologic results were available in 85 patients who underwent surgery as the primary treatment of HNSCC. Pathologic factors of the primary tumor, in-cluding perineural invasion (P=.64), lymphovascular per-meation (P =.40), and positive surgical margin (P =.74), were not predictive for the development of a malignant neoplasm of the lung. Fifty-two patients underwent neck dissection as part of their initial treatment, and patho-logic cervical metastasis was found in 40 patients (19 with-out ECS and 21 with ECS). The incidence of a malig-nant neoplasm of the lung was significantly higher in patients with ECS (57.1%) than in those without ECS (26.3%) (P =.04). However, ECS remained a borderline predictor for the development of a malignant neoplasm of the lung (P =.07) by multivariate analysis in this sub-group of patients.
COMMENT
For patients with HNSCC, chest diagnosis is crucial and may influence their treatment plan. However, routine Table 3. Correlation Between Timing of Imaging and Initial
Results of 270 Chest Computed Tomographic (CT) Scans
Timing Group
Chest CT Results, No. (%)
Total Normal Abnormal Malignant Indeterminate New case 115 (85.8) 10 (7.5) 9 (6.7) 134 Follow-up case 29 (55.8) 17 (32.7) 6 (11.5) 52 Recurrent casea 47 (56.0) 27 (32.1) 10 (11.9) 84 Total 191 (70.7) 54 (20.0) 25 (9.3) 270
aResidual or recurrent locoregional disease.
Table 4. Final Results of 25 Indeterminate Lesions on Follow-up Chest Computed Tomographic Scans
Original Finding No. (%) P Value Progression Resolution or No Change Small solitary nodule 10 (66.7)a 5 (33.3)
.01 Multiple air-space opacity 1 (10.0)b 9 (90.0)
Total 11 (44.0) 14 (56.0)
aMultiple nodules had developed in the follow-up scans. bMalignant pleural effusion was proved in this case.
yearly chest radiography has been shown by Shah and Applebaum7to contribute little to the overall survival in patients with HNSCC. In the initial 2 to 3 years of follow-up, intensive chest screening has been suggested at 4- to 6-month intervals rather than annually.4Chest CT is su-perior to radiography in sensitivity and adds little extra time and radiation dose (3-6 msv) when performed with neck CT.10,13However, chest CT is more expensive, and its indications vary widely as a screening tool for HNSCC. In the present study without strict guidelines, 70.7% of 270 chest CT scans showed normal findings. It is impor-tant to understand when and under which conditions chest CT will be cost-effective.
Chest CT performed at the initial diagnosis of primary tumors theoretically has the greatest effect on treatment planning. However, Keski-Säntti et al8and Tan et al9 dem-onstrated limited usefulness of routine chest CT screen-ing in patients newly diagnosed as havscreen-ing HNSCC. Our study also showed a low rate of an abnormal chest CT scan at the initial diagnosis. In contrast, a significantly higher rate of an abnormal chest CT scan was found in the low-up period. Among 23 abnormal scans in the fol-low-up case group, 12 had antecedent normal CT scans at the initial diagnosis of their primary tumor. For more ef-fective case management, chest CT during the follow-up period in high-risk patients should be emphasized.
Confirmation of the diagnosis of a malignant neoplasm of the lung theoretically should be supported by endoscopic or CT-guided biopsy. However, it is not always feasible in clinical practice. Brouwer et al11reported that pulmonary lesions were considered malignant if unequivocal radiologic findings were identified on chest CT or if progression of the lesions was demonstrated on a follow-up scan. In our study, lung biopsy was performed in only 8 of 49 patients (16.3%) with multiple and peripheral pulmonary nodules, as Mesur-olle et al14and Ginsberg et al15demonstrated more than 90% malignant results in such lesions. However, 2 false-positive CT scans were encountered in the present study. Therefore, follow-up CT scans should be mandatory, although false-positive findings are rare. Lung metastasis and second pri-mary lung cancer were categorized as a malignant neoplasm of the lung in this study. Differentiating between them in clinical practice is sometimes difficult for HNSCC, especially when the histologic diagnosis of pulmonary lesions is squa-mous cell carcinoma.16Advances in molecular genetic ap-proaches may become efficient tools for the differential di-agnosis in the future.16
Indeterminate lesions were common on chest CT in our study, and special attention should be paid to them. Based on the progressive change in follow-up scans, 44.0% of indeterminate lesions were eventually considered a ma-lignant neoplasm of the lung. We also found that small (⬍1 cm) solitary nodules, which were usually resect-able, carried significantly higher chances (66.7%) of being a malignant neoplasm. For patients with HNSCC, du-rable disease control has been reported in 34% of resect-able pulmonary metastases after undergoing surgery.17 However, under a close imaging follow-up policy, all pa-tients with progression from small solitary nodules de-veloped multiple pulmonary nodules, and their disease could only be managed with chemotherapy for pallia-tion in the present study.
The evaluation and management of potentially con-trollable small solitary pulmonary nodules remain great challenges. Computed tomography–guided biopsy has been reported by Quint et al18to be a valuable tool for larger (5-30 mm) pulmonary nodules. However, biopsy of small indeterminate nodules is associated with low ac-curacy, and pneumothorax may occur.19Positron emis-sion tomography with fludeoxyglucose F 18 (FDG-PET) has been advocated for high sensitivity.20,21However, it is not widely available and has been reported to be no more accurate in detecting a malignant neoplasm of the lung than chest CT.20,22Confirmation of abnormal find-ings on FDG-PET is necessary because false-positive re-sults occur in 20% to 67% of cases.20,21When appropri-ate, aggressive surgical excision is another choice for definitive diagnosis and management.
Because the chance of disease control is low in pa-tients with a malignant neoplasm of the lung at the ini-tial diagnosis of HNSCC or after locoregional treatment failure, an abnormal chest CT scan can affect the
treat-Table 5. Univariate Analysis for Predictors of a Malignant Neoplasm of the Lung Among 192 Patients
Variable Malignant Neoplasm of the Lung P Value Normal Abnormal Smoking history No 22 5 .09 Yes 107 58 Tumor location
Oral cavity, oropharynx, glottis 67 24
.07 Hypopharynx, supraglottis 62 39 T classification T1 or T2 47 27 .39 T3 or T4 82 36 N classification N0 or N1 72 24 .02 N2 or N3 57 39 TNM stage I-IIIa 53 16 .03 IV 76 47 Recurrent diseaseb No 106 28 ⬍.001 Yes 23 35
Distant metastasis to another site
No 110 39
⬍.001
Yes 19 24
aFor grouping early and advanced diseases, we used stages I through II in
this table, vs stages III through IV (as in Table 2).
bResidual or recurrent locoregional disease.
Table 6. Multivariate Analysis for Predictors of a Malignant Neoplasm of the Lung Among 192 Patients
Variable Hazard Ratio (95% Confidence Interval) P Value N classification (N2 or N3 vs N0 or N1) 2.73 (1.31-5.68) .01 Recurrent diseasea 8.43 (3.89-18.26) ⬍.001
Distant metastasis to another site 4.35 (1.93-9.78) ⬍.001
ment plan and prognosis. For patients with HNSCC who develop unresectable malignant neoplasm of the lung, the treatment policy should mostly be palliative. Only for pa-tients with potentially resectable malignant neoplasm of the lung should aggressive curative treatment at the pri-mary site and the lung be considered for possible long-term disease control.17,23
Several limitations should be noted in this study. Al-though ECS had been reported as a predictor of distant metastasis,24we show its predictive value in only a small subgroup of patients with pathologic N disease or greater by univariate analysis. Further analysis in a larger study population whose initial treatment includes neck dis-section is needed to clarify the relation between ECS and the development of a malignant neoplasm of the lung. Other limitations included selection bias in performing chest CT, the retrospective study design, and the lim-ited follow-up period in some patients. Therefore, our results should be interpreted with caution. In the pres-ent study, CT was performed based on physician choice in patients with multiple unfavorable factors and with high likelihood of distant metastasis. A prospective study in consecutive patients with longer follow-up time is needed for more substantial results.
In conclusion, chest CT is recommended for high-risk patients, especially every 6 months for the first 2 years during the follow-up period, although its role is contro-versial for patients newly diagnosed as having HNSCC. High-risk patients include those with N2 or N3 disease, stage IV disease, or locoregional recurrence. For pa-tients with indeterminate small (⬍1 cm) solitary pul-monary nodules, aggressive evaluation and manage-ment are imperative because of the high rate of a malignant neoplasm of the lung.
Submitted for Publication: June 26, 2007; final revi-sion received September 5, 2007; accepted December 19, 2007.
Correspondence: Shyh-Kuan Tai, MD, Department of Otolaryngology, Taipei Veterans General Hospital, 201 Shih-Pai Rd, Section 2, Taipei, Taiwan 11217 (sktai @vghtpe.gov.tw).
Author Contributions: Drs Hsu and Tai had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analy-sis. Study concept and design: Hsu and Tai. Acquisition of data: Chu, Lan, Chang, Tsai, Huang, and Wang. Analy-sis and interpretation of data: Hsu, Liu, and Tai. Drafting of the manuscript: Hsu. Critical revision of the manuscript for important intellectual content: Chu, Liu, Lan, Chang, Tsai, Huang, Wang, and Tai. Statistical analysis: Hsu and Tai. Administrative, technical, and material support: Liu, Lan, Chang, Tsai, Huang, and Wang. Study supervision: Chu and Tai.
Financial Disclosure: None reported.
Previous Presentation: This study was presented at the Eighth Taiwan-Japan Conference in Otolaryngology– Head and Neck Surgery; December 17, 2005; Taipei, Taiwan.
REFERENCES
1. Leo´n X, Quer M, Orus C, del Prado Venegas M, Lopez M. Distant metastases in head and neck cancer patients who achieved loco-regional control. Head Neck. 2000;22(7):680-686.
2. de Bree R, Deurloo EE, Snow GB, Leemans CR. Screening for distant metasta-ses in patients with head and neck cancer. Laryngoscope. 2000;110(3, pt 1): 397-401.
3. Alvi A, Johnson JT. Development of distant metastasis after treatment of advanced-stage head and neck cancer. Head Neck. 1997;19(6):500-505.
4. Leo´n X, Ferlito A, Myer CM III, et al. Second primary tumors in head and neck cancer patients. Acta Otolaryngol. 2002;122(7):765-778.
5. Ong TK, Kerawala CJ, Martin IC, Stafford FW. The role of thorax imaging in stag-ing head and neck squamous cell carcinoma. J Craniomaxillofac Surg. 1999; 27(6):339-344.
6. Houghton DJ, Hughes ML, Garvey C, et al. Role of chest CT scanning in the man-agement of patients presenting with head and neck cancer. Head Neck. 1998; 20(7):614-618.
7. Shah SI, Applebaum EL. Lung cancer after head and neck cancer: role of chest radiography. Laryngoscope. 2000;110(12):2033-2036.
8. Keski-Säntti HT, Markkola AT, Makitie AA, Back LJ, Atula TS. CT of the chest and abdomen in patients with newly diagnosed head and neck squamous cell carcinoma. Head Neck. 2005;27(10):909-915.
9. Tan L, Greener CC, Seikaly H, Rassekh CH, Calhoun KH. Role of screening chest computed tomography in patients with advanced head and neck cancer.
Oto-laryngol Head Neck Surg. 1999;120(5):689-692.
10. Houghton DJ, McGarry G, Stewart I, Wilson JA, MacKenzie K. Chest computer-ized tomography scanning in patients presenting with head and neck cancer. Clin
Otolaryngol Allied Sci. 1998;23(4):348-350.
11. Brouwer J, de Bree R, Hoekstra OS, et al. Screening for distant metastases in patients with head and neck cancer: is chest computed tomography sufficient?
Laryngoscope. 2005;115(10):1813-1817.
12. Greene FL, Page DL, Fleming ID, Balch CM, Haller DG, Morrow M. In: Fritz A, ed.
AJCC Cancer Staging Manual. 6th ed. New York, NY: Springer-Verlag; 2002.
13. Arunachalam PS, Putnam G, Jennings P, Messersmith R, Robson AK. Role of computerized tomography (CT) scan of the chest in patients with newly diag-nosed head and neck cancers. Clin Otolaryngol Allied Sci. 2002;27(5):409-411.
14. Mesurolle B, Mignon F, Meingan P, Domenge C, Vasile M, Sigal R. Head and neck cancer patients with pulmonary nodules: value and role of CT-guided trans-thoracic needle aspiration biopsies. Head Neck. 2003;25(11):889-894. 15. Ginsberg MS, Griff SK, Go BD, Yoo HH, Schwartz LH, Panicek DM. Pulmonary
nodules resected at video-assisted thoracoscopic surgery: etiology in 426 patients.
Radiology. 1999;213(1):277-282.
16. Geurts TW, Nederlof PM, van den Brekel MW, et al. Pulmonary squamous cell carcinoma following head and neck squamous cell carcinoma: metastasis or sec-ond primary? Clin Cancer Res. 2005;11(18):6608-6614.
17. Liu D, Labow DM, Dang N, et al. Pulmonary metastasectomy for head and neck cancers. Ann Surg Oncol. 1999;6(6):572-578.
18. Quint LE, Park CH, Iannettoni MD. Solitary pulmonary nodules in patients with extrapulmonary neoplasms. Radiology. 2000;217(1):257-261.
19. Wallace MJ, Krishnamurthy S, Broemeling LD, et al. CT-guided percutaneous fine-needle aspiration biopsy of small (ⱕ1-cm) pulmonary lesions. Radiology. 2002;225(3):823-828.
20. Wax MK, Myers LL, Gabalski EC, Husain S, Gona JM, Nabi H. Positron emission tomography in the evaluation of synchronous lung lesions in patients with un-treated head and neck cancer. Arch Otolaryngol Head Neck Surg. 2002;128 (6):703-707.
21. Keyes JW Jr, Chen MY, Watson NE Jr, Greven KM, McGuirt WF, Williams DW III. FDG PET evaluation of head and neck cancer: value of imaging the thorax. Head
Neck. 2000;22(2):105-110.
22. Hanasono MM, Kunda LD, Segall GM, Ku GH, Terris DJ. Uses and limitations of FDG positron emission tomography in patients with head and neck cancer.
Laryngoscope. 1999;109(6):880-885.
23. Kuriakose MA, Loree TR, Rubenfeld A, et al. Simultaneously presenting head and neck and lung cancer: a diagnostic and treatment dilemma. Laryngoscope. 2002; 112(1):120-123.
24. Puri SK, Fan CY, Hanna E. Significance of extracapsular lymph node metastases in patients with head and neck squamous cell carcinoma. Curr Opin Otolaryngol