INTERESTING IMAGE
Title: Parotid Gland Metastasis From Squamous Cell Carcinoma of Esophagus Detected by FDG PET/CT
Authors: Te-Chun Hsieh, MD,*† Yu-Chin Wu, MD,‡ Shung-Shung Sun, MD,*† Chun-Fan Yang, MD,§|| and Chia-Hung Kao, MD*¶
Abstract: A 55-year-old man was diagnosed with squamous cell carcinoma in the middle thoracic esophagus. The FDG PET/CT revealed an incidental strong FDG-avid finding (SUVmax, 11) in the right parotid gland, which was subsequently confirmed as
metastasis from the squamous cell carcinoma of esophagus via surgery. The current case adds another differential diagnosis of parotid FDG-avid lesion to the existing literature. Key Words: metastasis, parotid gland, squamous cell carcinoma, esophagus, FDG PET/CT.
ACKNOWLEDGMENTS
The authors thank Mr Kuo-Yang Yen for assisting with the editing of figures.
From the *Department of Nuclear Medicine and PET Center, China Medical University Hospital, Taichung; †Department of Biomedical Imaging and Radiological Science, China Medical University, Taichung; ‡Department of Nuclear Medicine, National Taiwan University Hospital Hsin-Chu Branch, Hsinchu City; §Department of Pathology,
China Medical University Hospital; ||China Medical University; and ¶School of Medicine, China Medical University, Taichung, Taiwan.
Conflicts of interest and sources of funding: none declared.
Drs. Wu and Kao contributed equally to this work.
Reprints: Chia-Hung Kao, MD, Department of Nuclear Medicine and PET Center, China Medical University Hospital, No. 2 Yuh-Der Rd, Taichung 404, Taiwan. E-mail:
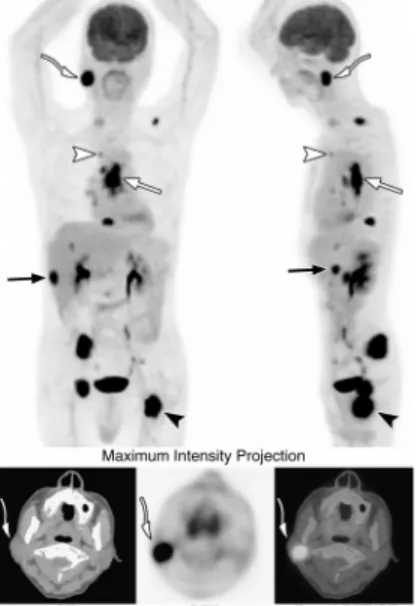
FIGURE 1. A 55-year-old man had middle thoracic esophageal squamous cell carcinoma. FDG PET/CT revealed FDG-avid malignancies in the esophagus (white straight arrows), lymph nodes (white arrowheads), bones (black arrowheads) and liver (black arrows). An unexpected FDG-avid lesion (white curved arrows; SUVmax, 11) was noticed in the right parotid gland. Differential diagnoses included Sjőgren sialoadenitis,1 compensated
hyperlasia,2 benign tumors,3 primary malignancies,3,4 and metastases.4,5 Because there was
significant overlap of FDG avidity between malignant and benign lesions,3,4 pathological
confirmation of the parotid lesion was necessary before treatment.
FIGURE 2. Biopsy of the right parotid gland demonstrated squamous cell carcinoma without apparent metaplasia of ductal or glandular epithelium in the parotid gland. Thus,
metastatic rather than primary squamous cell carcinoma was suggested.The incidence of salivary gland neoplasm is relatively uncommon. Most salivary gland tumors occur in the parotid gland. Eighty percent of parotid gland tumors are benign, and most are
pleomorphic adenomas or Warthin tumors.6 Metastasis occurs less than 10% of all parotid
gland malignancies.7 About 70% of metastases are from cutaneous squamous cell
carcinoma or melanoma of the head and neck.8 The other 15% are from noncutaneous
lesions of the head and neck. Metastases are seldom from infraclavicular primaries but have been reported from cancers of the lung,4 breast,8 gastroesophageal junction,9 colon,10
kidney,3 ovary,4 and prostate11 as well as liposarcoma,12 rhabdomyosarcoma,8 and
neuroblastoma.13 Primary squamous cell carcinoma of parotid gland is rare and must be
distinguished from other primary tumors of the parotid gland or metastases from
extraparotid origins. The development of primary squamous cell carcinoma is thought to be due to sequential changes of chronic inflammation, metaplasia, and transformation of invasive carcinoma of ductal epithelium. Hence, the coincidence of squamous metaplasia may provide a supplementary evidence to diagnose primary squamous cell carcinoma of the parotid gland.14In conclusion, our current case adds another differential diagnosis of
REFERENCES
1. Jadvar H, Bonyadlou S, Iagaru A, et al. FDG PET-CT demonstration of Sjo¨gren’s sialoadenitis. Clin Nucl Med. 2005;30:698-699.
2. Chen YK, Kuo CJ, Yeh CL. Unilateral agenesis of the parotid gland with
contralateral compensation hypermetabolism of FDG. Clin Nucl Med. 2011; 36:710-711. 3. Uchida Y, Minoshima S, Kawata T, et al. Diagnostic value of FDG PET and
salivary gland scintigraphy for parotid tumors. Clin Nucl Med. 2005;30: 170-176.
4. Wang HC, Zuo CT, Hua FC, et al. Efficacy of conventional whole-body (18)F-FDG PET/CT in the incidental findings of parotid masses. Ann Nucl Med. 2010;24:571-577. 5. Malhotra G, Nair N, Awasare S, et al. Metastatic parotid tumor: a rare presentation for papillary carcinoma of thyroid. Clin Nucl Med. 2007;32:488-490.
6. McCormick M, Keller T, Butler N. A case of synchronous unilateral parotid tumors of different histologic types. WMJ. 2009;108:200-202.
7. Ying YL, Johnson JT, Myers EN. Squamous cell carcinoma of the parotid gland. Head Neck. 2006;28:626-632.
8. Nuyens M, Schupbach J, Stauffer E, et al. Metastatic disease to the parotid gland. Otolaryngol Head Neck Surg. 2006;135:844-848.
9. Mohyuddin H, Mahrous A, Sharma V, et al. Parotid mass: an unusual presentation of gastroesophageal malignancy. J Laryngol Otol. 2011;125:546-548.
10. Mason AC, Azari KK, Farkas LM, et al. Metastatic adenocarcinoma of the colon presenting as a mass in the mandible. Head Neck. 2005;27:729-732.
11. Kirkali Z, Koyuncuoglu M, Pabuccuoglu U, et al. Prostatic carcinoma presenting with painless parotid mass. Urology. 1995;46:406-407.
12. Trabelsi A, Ben Abdelkrim S, Jemni H, et al. Metastatic liposarcoma to the parotid. J Oncol. 2008;2008:715153.
13. Boyd DT, Hayeri MR, Kadom N. Parotid metastasis from adrenal neuroblastoma. Pediatr Radiol. 2010;40(suppl 1):S113-S115.
14. Flynn MB, Maguire S, Martinez S, et al. Primary squamous cell carcinoma of the parotid gland: the importance of correct histological diagnosis. Ann Surg Oncol. 1999;6:768-770.